
Verbal Short-Term Memory Disturbance in the Primary Progressive Aphasias: Challenges and Distinctions in a Clinical Setting

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Case Vignettes
3.1. lv-PPA Patient: NS
3.1.1. Neuropsychological Assessment
3.1.2. Clinical Opinion about the Patient’s Verbal and Visuospatial Short-Term and Working Memory Profile
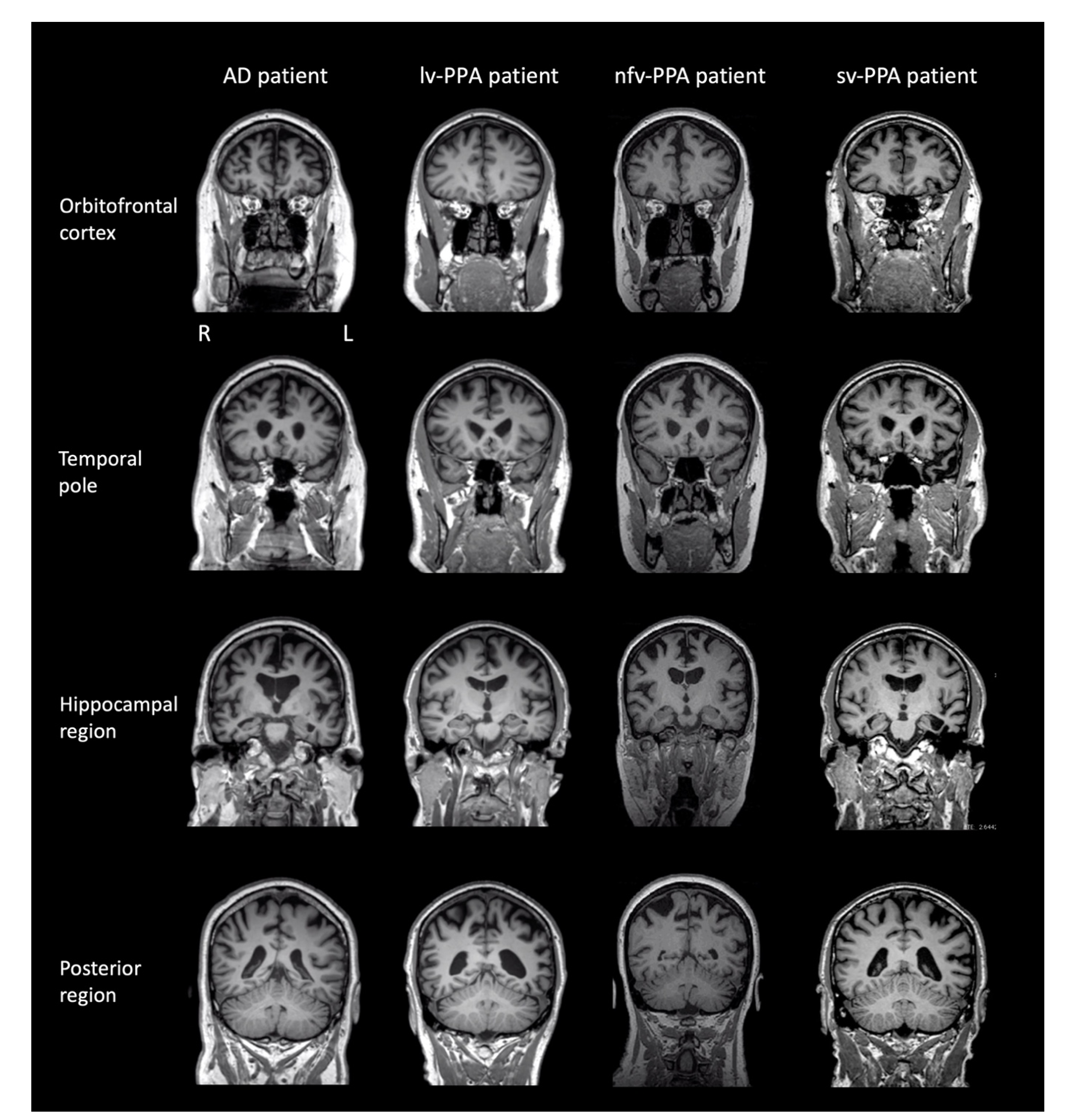
3.1.3. Brain MRI and Clinical Diagnosis
3.2. nfv-PPA Patient: ML
3.2.1. Neuropsychological Assessment
3.2.2. Clinical Opinion about the Patient’s Verbal and Visuospatial Short-Term and Working Memory Profile
3.2.3. Brain MRI and Clinical Diagnosis
3.3. sv-PPA Patient: JC
3.3.1. Neuropsychological Assessment
3.3.2. Clinical Opinion about the Patient’s Verbal and Visuospatial Short-Term and Working Memory Profile
3.3.3. Brain MRI and Clinical Diagnosis
3.4. Typical AD Patient: TN
3.4.1. Neuropsychological Assessment
3.4.2. Clinical Opinion about the Patient’s Verbal and Visuospatial Short-Term and Working Memory Profile
3.4.3. Brain MRI and Clinical Diagnosis
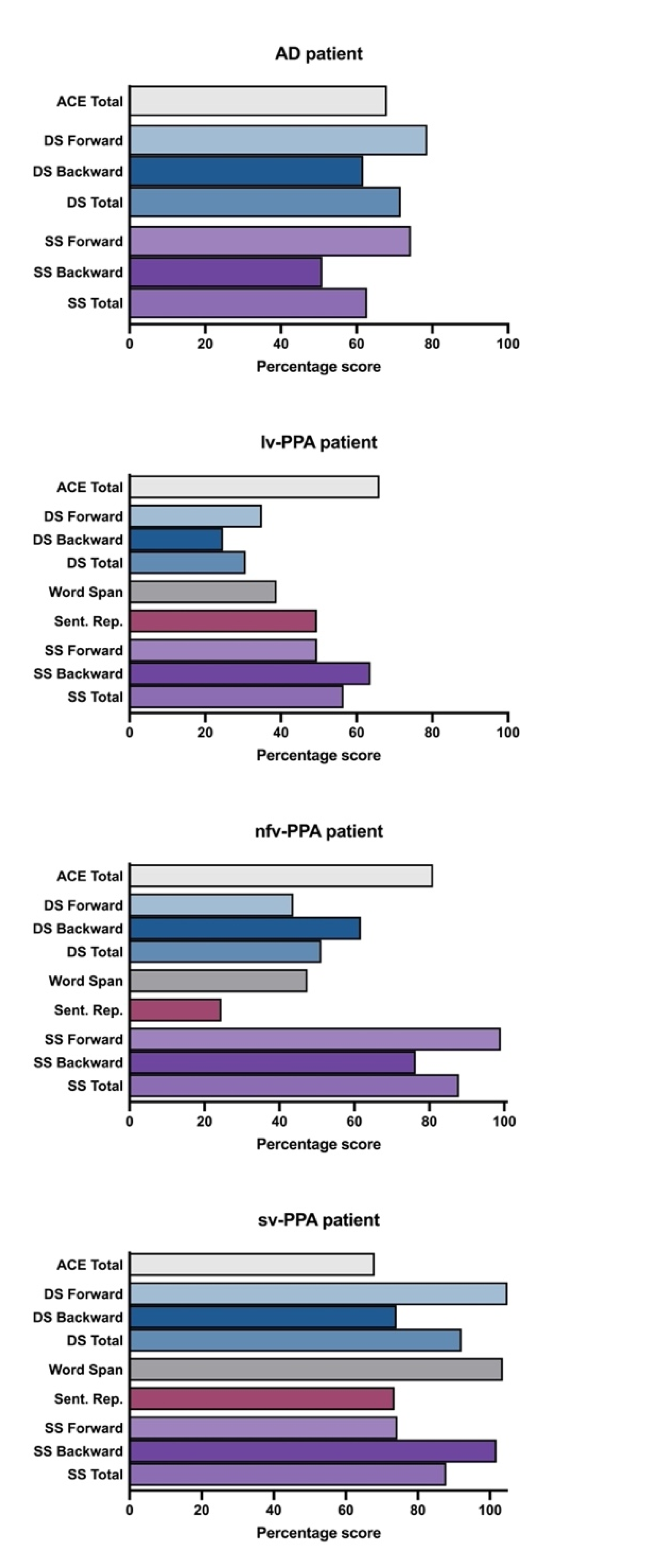
3.4.4. Summary of the Short-Term and Working Memory Profiles across Patients and Relative to a Matched Control Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Gorno-Tempini, M.L.; Hillis, A.E.; Weintraub, S.; Kertesz, A.; Mendez, M.; Cappa, S.F.; Ogar, J.M.; Rohrer, J.D.; Black, S.; Boeve, B.F.; et al. Classification of primary progressive aphasia and its variants. Neurology 2011, 76, 1006–1014. [Google Scholar] [CrossRef] [Green Version]
- Gorno-Tempini, M.L.; Brambati, S.M.; Ginex, V.; Ogar, J.; Dronkers, N.F.; Marcone, A.; Perani, D.; Garibotto, V.; Cappa, S.F.; Miller, B.L. The logopenic/phonological variant of primary progressive aphasia. Neurology 2008, 71, 1227–1234. [Google Scholar] [CrossRef] [Green Version]
- Leyton, C.E.; Savage, S.; Irish, M.; Schubert, S.; Piguet, O.; Ballard, K.J.; Hodges, J.R. Verbal repetition in primary progressive aphasia and Alzheimer’s disease. J. Alzheimer’s Dis. 2014, 41, 575–585. [Google Scholar] [CrossRef] [PubMed]
- Foxe, D.; Irish, M.; Roquet, D.; Scharfenberg, A.; Bradshaw, N.; Hodges, J.R.; Burrell, J.R.; Piguet, O. Visuospatial short-term and working memory disturbance in the primary progressive aphasias: Neuroanatomical and clinical implications. Cortex 2020, 132, 223–237. [Google Scholar] [CrossRef]
- Croot, K.; Ballard, K.; Leyton, C.E.; Hodges, J.R. Apraxia of speech and phonological errors in the diagnosis of nonfluent/agrammatic and logopenic variants of primary progressive aphasia. J. Speech Lang. Hear. Res. 2012, 55, s1562–s1572. [Google Scholar] [CrossRef]
- Owens, T.E.; Machulda, M.M.; Duffy, J.R.; Strand, E.A.; Clark, H.M.; Boland, S.; Martin, P.R.; Lowe, V.J.; Jack, C.R.; Whitwell, J.L.; et al. Patterns of neuropsychological dysfunction and cortical volume changes in logopenic aphasia. J. Alzheimer’s Dis. 2018, 66, 1015–1025. [Google Scholar] [CrossRef]
- Sajjadi, S.A.; Patterson, K.; Nestor, P.J. Logopenic, mixed, or Alzheimer-related aphasia? Neurology 2014, 82, 1127–1131. [Google Scholar] [CrossRef]
- Murley, A.G.; Coyle-Gilchrist, I.; Rouse, M.A.; Jones, P.S.; Li, W.; Wiggins, J.; Lansdall, C.; Rodriguez, P.V.; Wilcox, A.; Tsvetanov, K.A.; et al. Redefining the multidimensional clinical phenotypes of frontotemporal lobar degeneration syndromes. Brain 2020, 143, 1555–1571. [Google Scholar] [CrossRef]
- Sajjadi, S.A.; Patterson, K.; Arnold, R.J.; Watson, P.C.; Nestor, P.J. Primary progressive aphasia: A tale of two syndromes and the rest. Neurology 2012, 78, 1670–1677. [Google Scholar] [CrossRef] [Green Version]
- Vandenberghe, R. Classification of the primary progressive aphasias: Principles and review of progress since 2011. Alzheimer’s Res. Ther. 2016, 8, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Beales, A.; Whitworth, A.; Cartwright, J.; Panegyres, P.K.; Kane, R.T. Profiling sentence repetition deficits in primary progressive aphasia and Alzheimer’s disease: Error patterns and association with digit span. Brain Lang. 2019, 194, 1–11. [Google Scholar] [CrossRef]
- Hohlbaum, K.; Dressel, K.; Lange, I.; Wellner, B.; Saez, L.E.; Huber, W.; Grande, M.; Amunts, K.; Grodzinsky, Y.; Heim, S. Sentence repetition deficits in the logopenic variant of PPA: Linguistic analysis of longitudinal and cross-sectional data. Aphasiology 2018, 32, 1445–1467. [Google Scholar] [CrossRef]
- Hsieh, S.; Schubert, S.; Hoon, C.; Mioshi, E.; Hodges, J.R. Validation of the Addenbrooke’s Cognitive Examination III in frontotemporal dementia and Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2013, 36, 242–250. [Google Scholar] [CrossRef]
- Knopman, D.S.; Kramer, J.H.; Boeve, B.F.; Caselli, R.J.; Graff-Radford, N.R.; Mendez, M.F.; Miller, B.L.; Mercaldo, N. Development of methodology for conducting clinical trials in frontotemporal lobar degeneration. Brain 2008, 131, 2957–2968. [Google Scholar] [CrossRef] [Green Version]
- Ng, F.; Trauer, T.; Dodd, S.; Callaly, T.; Campbell, S.; Berk, M. The validity of the 21-item version of the depression anxiety stress scales as a routine clinical outcome measure. Acta Neuropsychiatr. 2007, 19, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states—comparison of the depression anxiety stress scales (dass) with the beck depression and anxiety inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Wechsler, D. Weschler Adult Intelligence Scale—Third Edition: Administration and Scoring Manual; Psychological Corporation: San Antonio, TX, USA, 1997. [Google Scholar]
- Mioshi, E.; Hsieh, S.; Savage, S.; Hornberger, M.; Hodges, J.R. Clinical staging and disease progression in frontotemporal dementia. Neurology 2010, 74, 1591–1597. [Google Scholar] [CrossRef] [PubMed]
- Strauss, E.; Sherman, E.M.S.; Spreen, O. A Compendium of Neuropsychological Tests: Administration, Norms, And Commentary, 3rd ed.; Oxford University Press: New York, NY, USA, 2006. [Google Scholar]
- Rey, A. L’examen psychologique dans les cas d’encéphalopathie traumatique. Arch. Psychol. 1941, 28, 286–340. [Google Scholar]
- Benton, A.L.; Hamsher, K.d.; Sivian, A.B. Multilingual Aphasia Examination, 3rd ed.; AJA Associates, Inc.: Iowa City, IA, USA, 1994. [Google Scholar]
- Wechsler, D. Weschler Memory Scale—Third Edition: Administration and Scoring Manual; Psychological Corporation: San Antonio, TX, USA, 1997. [Google Scholar]
- Savage, S.; Hsieh, S.; Leslie, F.; Foxe, D.; Piguet, O.; Hodges, J.R. Distinguishing subtypes in primary progressive aphasia: Application of the Sydney language battery. Dement. Geriatr. Cogn. Disord. 2013, 35, 208–218. [Google Scholar] [CrossRef] [PubMed]
- Reitan, R.M. The relation of the trail making test to organic brain damage. J. Consult. Psychol. 1955, 19, 393–394. [Google Scholar] [CrossRef]
- So, M.; Foxe, D.; Kumfor, F.; Murray, C.; Hsieh, S.; Savage, G.; Ahmed, R.M.; Burrell, J.R.; Hodges, J.R.; Irish, M.; et al. Addenbrooke’s cognitive examination III: Psychometric characteristics and relations to functional ability in dementia. J. Int. Neuropsychol. Soc. 2018, 24, 854–863. [Google Scholar] [CrossRef] [PubMed]
- Klunk, W.E.; Engler, H.; Nordberg, A.; Wang, Y.; Blomqvist, G.; Holt, D.P.; Bergstrom, M.; Savitcheva, I.; Huang, G.F.; Estrada, S.; et al. Imaging brain amyloid in Alzheimer’s disease with Pittsburgh compound-B. Ann. Neurol. 2004, 55, 306–319. [Google Scholar] [CrossRef] [PubMed]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the national institute on aging-Alzheimer’s association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Jefferies, E.; Patterson, K.; Jones, R.W.; Bateman, D.; Lambon Ralph, M.A. A category-specific advantage for numbers in verbal short-term memory: Evidence from semantic dementia. Neuropsychologia 2004, 42, 639–660. [Google Scholar] [CrossRef] [PubMed]
- Eikelboom, W.S.; Janssen, N.; Jiskoot, L.C.; van den Berg, E.; Roelofs, A.; Kessels, R.P.C. Episodic and working memory function in primary progressive aphasia: A meta-analysis. Neurosci. Biobehav. Rev. 2018, 92, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Kamath, V.; Sutherland, E.R.; Chaney, G.A. A meta-analysis of neuropsychological functioning in the logopenic variant of primary progressive aphasia: Comparison with the semantic and non-fluent variants. J. Int. Neuropsychol. Soc. 2020, 26, 322–330. [Google Scholar] [CrossRef]
- Foxe, D.; Irish, M.; D’Mello, M.; Barhon, L.; Burrell, J.R.; Kessels, R.P.C.; Piguet, O. The box task: A novel tool to differentiate the primary progressive aphasias. Eur. J. Neurol. 2021. [Google Scholar] [CrossRef]
- Foxe, D.G.; Irish, M.; Hodges, J.R.; Piguet, O. Verbal and visuospatial span in logopenic progressive aphasia and Alzheimer’s disease. J. Int. Neuropsychol. Soc. 2013, 19, 247–253. [Google Scholar] [CrossRef]
- Foxe, D.; Leyton, C.E.; Hodges, J.R.; Burrell, J.R.; Irish, M.; Piguet, O. The neural correlates of auditory and visuospatial span in logopenic progressive aphasia and Alzheimer’s disease. Cortex 2016, 83, 39–50. [Google Scholar] [CrossRef]
- Wager, T.D.; Smith, E.E. Neuroimaging studies of working memory: A meta-analysis. Cogn. Affect. Behav. Neurosci. 2003, 3, 255–274. [Google Scholar] [CrossRef] [Green Version]
- Smith, E.E.; Jonides, J. Working memory: A view from neuroimaging. Cogn. Psychol. 1997, 33, 5–42. [Google Scholar] [CrossRef] [Green Version]
- Tippett, D.C.; Breining, B.; Goldberg, E.; Meier, E.; Sheppard, S.M.; Sherry, E.; Stockbridge, M.; Suarez, A.; Wright, A.E.; Hillis, A.E. Visuomotor figure construction and visual figure delayed recall and recognition in primary progressive aphasia. Aphasiology 2019, 34, 1456–1470. [Google Scholar] [CrossRef]
- Watson, C.L.; Possin, K.; Allen, I.E.; Hubbard, H.I.; Meyer, M.; Welch, A.E.; Rabinovici, G.D.; Rosen, H.; Rankin, K.P.; Miller, Z.; et al. Visuospatial functioning in the primary progressive aphasias. J. Int. Neuropsychol. Soc. 2018, 24, 259–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Possin, K.L. Visual spatial cognition in neurodegenerative disease. Neurocase 2010, 16, 466–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bak, T.H.; Caine, D.; Hearn, V.C.; Hodges, J.R. Visuospatial functions in atypical parkinsonian syndromes. J. Neurol. Neurosurg. Psychiatry 2006, 77, 454–456. [Google Scholar] [CrossRef] [Green Version]
- Huntley, J.D.; Howard, R.J. Working memory in early Alzheimer’s disease: A neuropsychological review. Int. J. Geriatr. Psychiatry 2010, 25, 121–132. [Google Scholar] [CrossRef]
- Magnin, E.; Chopard, G.; Ferreira, S.; Sylvestre, G.; Dariel, E.; Ryff, I.; Mertz, C.; Lamidieu, C.; Hidalgo, J.; Tio, G.; et al. Initial neuropsychological profile of a series of 20 patients with logopenic variant of primary progressive aphasia. J. Alzheimer’s Dis. 2013, 36, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; de Jager, C.A.; Haigh, A.M.; Garrard, P. Logopenic aphasia in Alzheimer’s disease: Clinical variant or clinical feature? J. Neurol. Neurosurg. Psychiatry 2012, 83, 1056–1062. [Google Scholar] [CrossRef] [PubMed]
- Taylor-Rubin, C.; Croot, K.; Nickels, L. Speech and language therapy in primary progressive aphasia: A critical review of current practice. Expert Rev. Neurother. 2021, 21, 419–430. [Google Scholar] [CrossRef] [PubMed]
- Ramanan, S.; Roquet, D.; Goldberg, Z.L.; Hodges, J.R.; Piguet, O.; Irish, M.; Lambon Ralph, M.A. Establishing two principal dimensions of cognitive variation in logopenic progressive aphasia. Brain Commun. 2020, 2, fcaa125. [Google Scholar] [CrossRef]
- Foxe, D.; Irish, M.; Hu, A.N.; Carrick, J.; Hodges, J.R.; Ahmed, R.M.; Burrell, J.R.; Piguet, O. Longitudinal cognitive and functional changes in primary progressive aphasia. J. Neurol. 2021, 268, 1951–1961. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, C.M.; Clemson, L.; Flanagan, E.; Kaizik, C.; Brodaty, H.; Hodges, J.R.; Piguet, O.; Mioshi, E. The relationship between behavioural changes, cognitive symptoms, and functional disability in primary progressive aphasia: A longitudinal study. Dement. Geriatr. Cogn. Disord. 2016, 42, 215–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, J.; Cushing, N.; Clemson, L.; Hodges, J.R.; Mioshi, E. Activities of daily living in progressive non-fluent aphasia, logopenic progressive aphasia and Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2012, 33, 354–360. [Google Scholar] [CrossRef]
- Chare, L.; Hodges, J.R.; Leyton, C.E.; McGinley, C.; Tan, R.H.; Kril, J.J.; Halliday, G.M. New criteria for frontotemporal dementia syndromes: Clinical and pathological diagnostic implications. J. Neurol. Neurosurg. Psychiatry 2014, 85, 865–870. [Google Scholar] [CrossRef]
- Harris, J.M.; Gall, C.; Thompson, J.C.; Richardson, A.M.; Neary, D.; du Plessis, D.; Pal, P.; Mann, D.M.; Snowden, J.S.; Jones, M. Classification and pathology of primary progressive aphasia. Neurology 2013, 81, 1832–1839. [Google Scholar] [CrossRef]
- Mesulam, M.; Wicklund, A.; Johnson, N.; Rogalski, E.; Leger, G.C.; Rademaker, A.; Weintraub, S.; Bigio, E.H. Alzheimer and frontotemporal pathology in subsets of primary progressive aphasia. Ann. Neurol. 2008, 63, 709–719. [Google Scholar] [CrossRef]
- Rowe, J.B. Parkinsonism in frontotemporal dementias. Int. Rev. Neurobiol. 2019, 149, 249–275. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Domain | Cognitive Test | Subtest (Max Score) | TN: AD Patient | NS: lv-PPA Patient | ML: nfv-PPA Patient | JC: sv-PPA Patient |
|---|---|---|---|---|---|---|
| Demographics | ||||||
| Sex (m:f) | Male | Male | Female | Male | ||
| Age (y) | 67 | 66 | 64 | 62 | ||
| Handedness | Right | Right | Right | Right | ||
| Education (y) | 9 | 12.25 | 12 | 16 | ||
| Disease duration (y) | 7.4 | 3.5 | 6.6 | 5.4 | ||
| General cognition Attention and executive functioning | ACE-III | Total (100) | 68 ** | 66 ** | 81 * | 67 ** |
| Trails | A time (errors) | 48 (0) | 56 (0) * | 65 (0) ** | 43 (0) | |
| B time (errors) | 365 (3) ** | 460 (2) ** | 344 (0) ** | 99 (0) | ||
| B-A time difference | 317 ** | 404 ** | 279 ** | 56 | ||
| Letter fluency | F, A, S | 36 | 14 ** | 12 ** | 36 | |
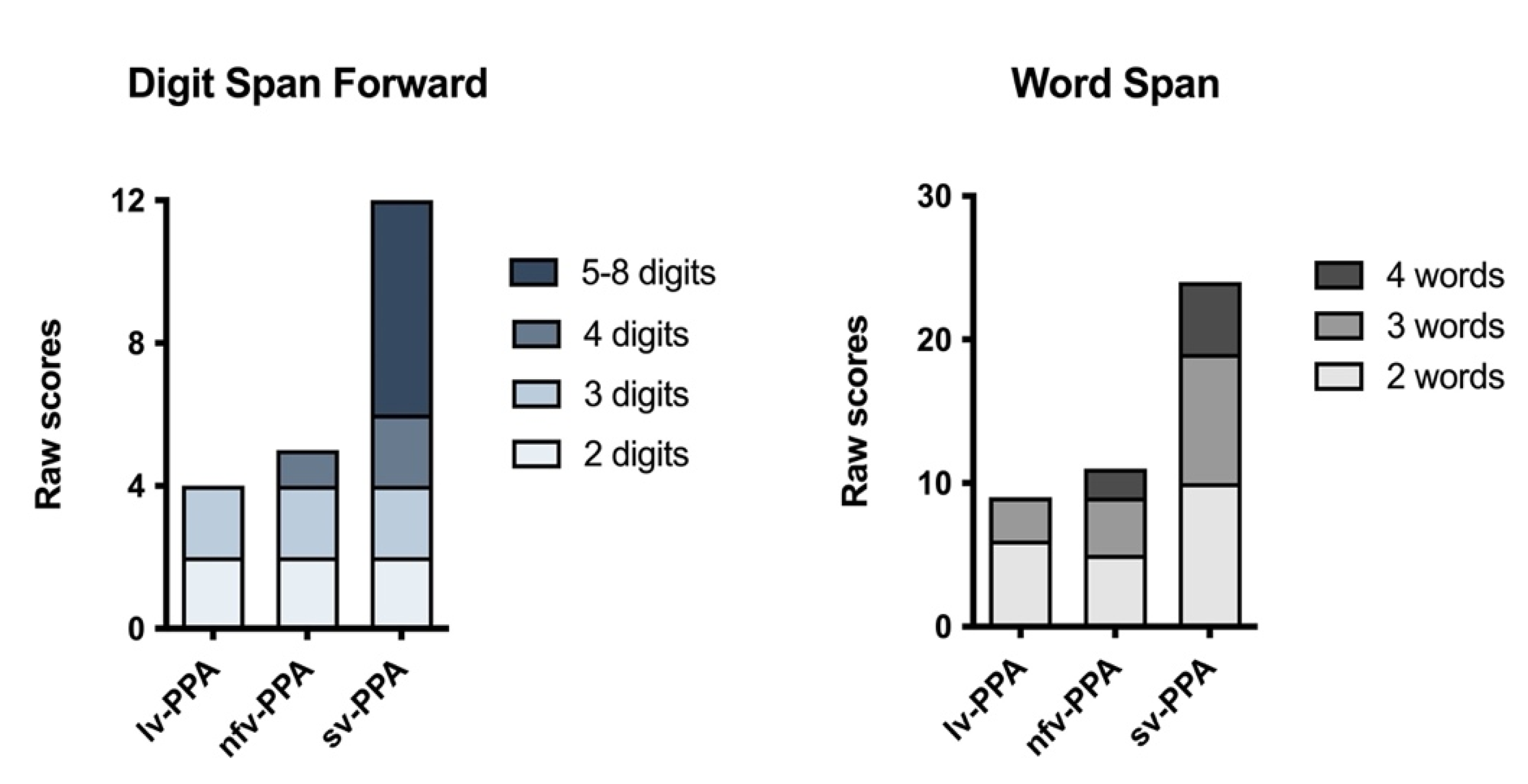
| Short-term and working memory | Digit Span | Raw Forward (longest) | 9 (6) | 4 (3) ** | 5 (4) * | 12 (8) |
| Raw Backward (longest) | 5 (4) | 2 (3) ** | 5 (4) * | 6 (4) | ||
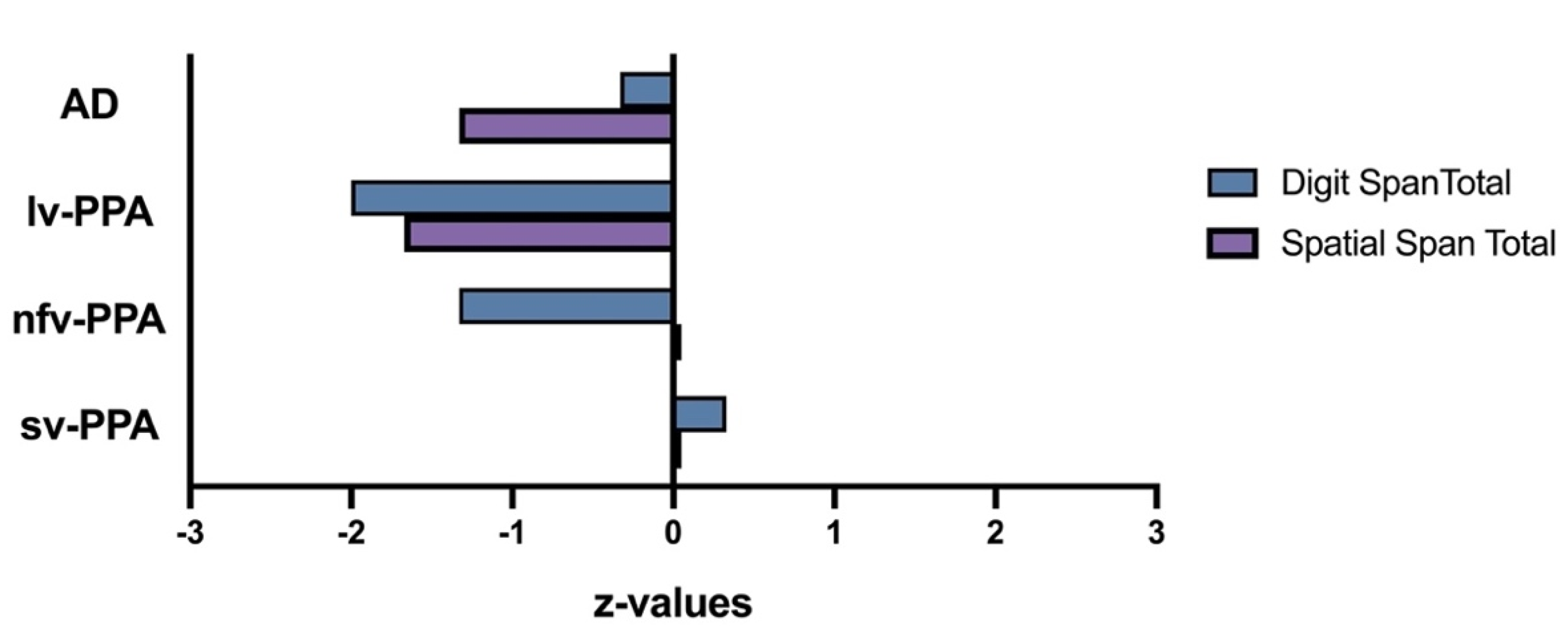
| Raw Total (SS) | 14 (9) | 6 (4) ** | 10 (6) * | 18 (11) | ||
| Spatial Span | Raw Forward (longest) | 6 (4) | 4 (3) * | 8 (6) | 6 (6) | |
| Raw Backward (longest) | 4 (4) * | 5 (4) | 6 (4) | 8 (6) | ||
| Raw Total (SS) | 10 (6) * | 9 (5) * | 14 (10) | 14 (10) | ||
| Sentence Rep | Raw Total (14) | Nil | 6 ** | 3 ** | 9 ** | |
| Word Span | Raw Total (30) | Nil | 9 ** | 11 ** | 24 | |
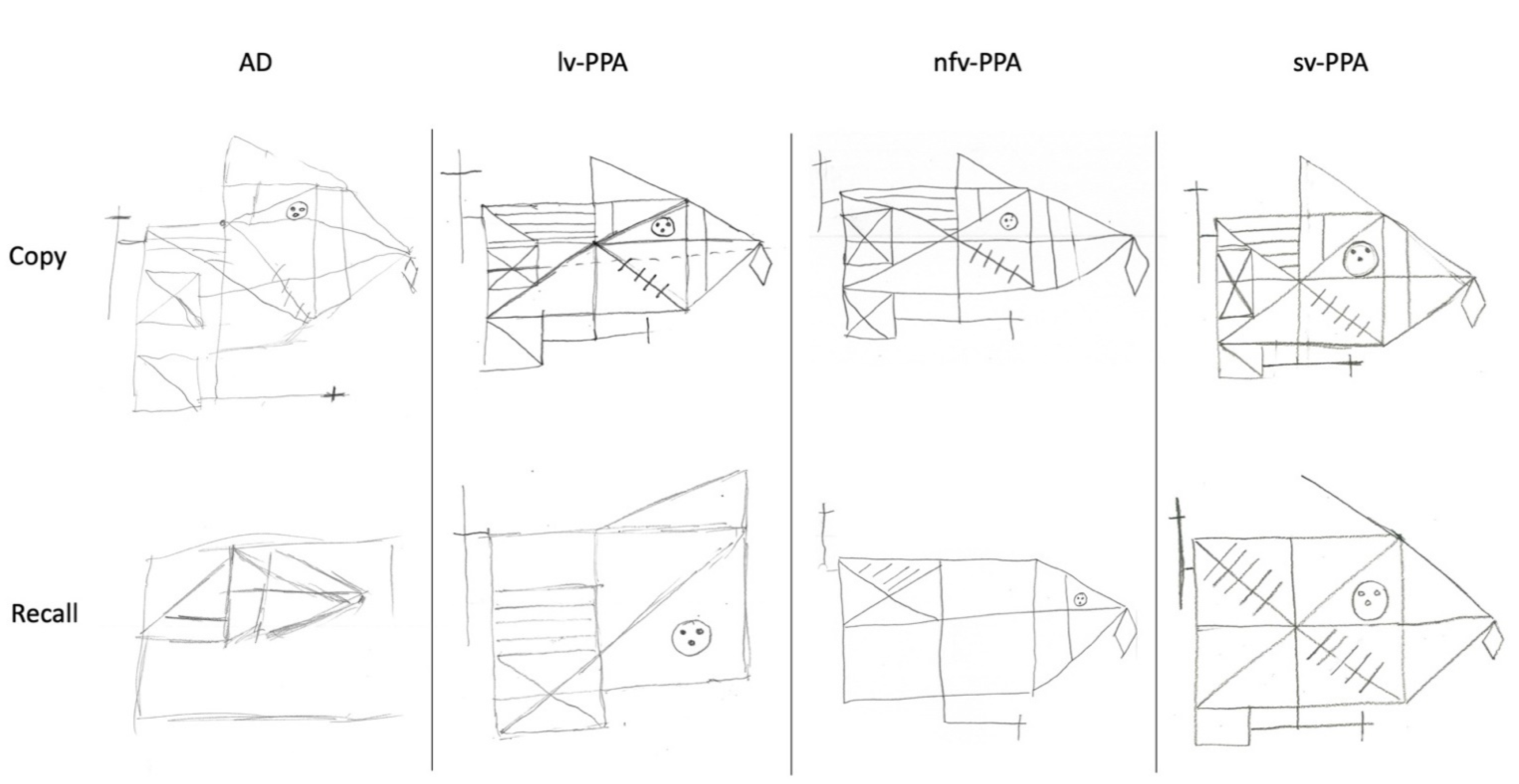
| Memory | RCFT | Copy (36) | 12.5 ** | 29 * | 30 * | 36 |
| 3-min recall (36) | 1 ** | 7.5 * | 18.5 | 22.5 | ||
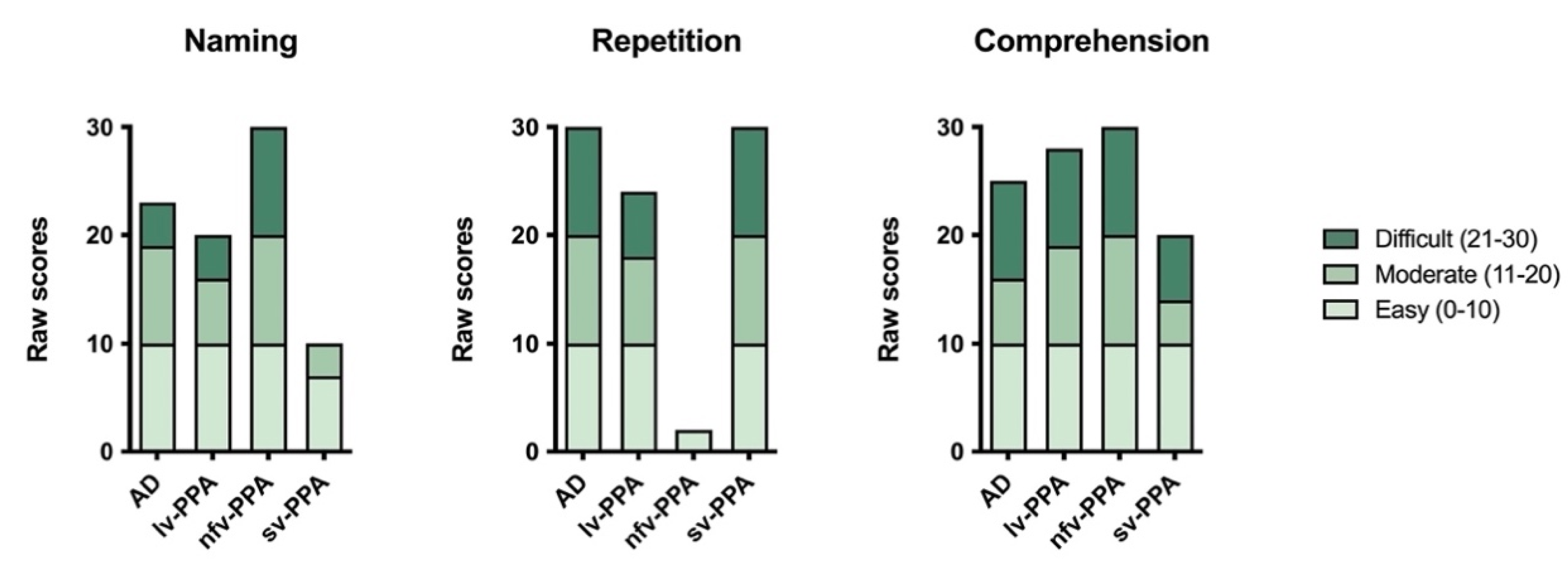
| Language | SYDBAT | Naming (30) | 23 * | 20 ** | 30 | 10 ** |
| Repetition (30) | 30 | 24** | 2 ** | 30 | ||
| Comprehension (30) | 25 * | 28 | 30 | 20 ** | ||
| Semantic Assoc. (30) | 27 | 29 | 29 | 19 ** | ||
| Visuospatial | Clock drawing | (5) | 5 | 5 | 5 | 5 |
| ACE Visuospatial | (16) | 15 | 15 | 14 | 16 | |
| RCFT | Copy time (secs) | 594 ** | 513 ** | 229 | 290 | |
| Mood | DASS-21 | Depression | 4 (Normal) | 0 (Normal) | 3 (Normal) | 0 (Normal) |
| Anxiety | 2 (Normal) | 1 (Normal) | 3 (Normal) | 0 (Normal) | ||
| Stress | 4 (Normal) | 4 (Normal) | 4 (Normal) | 3 (Normal) | ||
| Functional capacity | FRS | Total Rasch | 0.16 (Mod.) | 2.86 (Mild) | 5.39 (V. Mild) | 2.19 (Mild) |
| CDR-FTLD | Sums of boxes (SoB) | 5 (Mild) | 1.5 (Quest.) | 4 (V. Mild) | 2 (Quest.) |
| Analysis on Sentence-Level | Analysis on Word-Level | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 = No; 1 = Yes | Frequency | ||||||||||||||
| Item | Produced Sentence | Correct 0/1 | Erroneous Correct 0/1 | Uncertain/Repaired Correct 0/1 | Required Stimulus Repetition Correct 0/1 | Misordered Words Correct 0/1 | Violation of Syntactic Rules Correct 0/1 | Omission | Semantic Substitution | Formal Errors | Phonological Errors | Phonological Errors Affecting Morphemes | Grammatical Errors | Sound Deviations | Not Classified Errors |
| NS: lv-PPA patient | |||||||||||||||
| 1 | Take this home | 1 | 0 | 0 | 0 | 0 | 0 | ||||||||
| 2 | Where is the child? | 1 | 0 | 0 | 0 | 0 | 0 | ||||||||
| 3 | The car will not run | 1 | 0 | 0 | 0 | 0 | 0 | ||||||||
| 4 | Why are they not living here? | 1 | 0 | 0 | 0 | 0 | 0 | ||||||||
| 5 | The band (.) played and the /kraʊnd/ (5) cheered | 0 | 1 | 0 | 0 | 0 | 0 | 1 | |||||||
| 6 | Where are you going to work next summer? | 1 | 0 | 0 | 0 | 0 | 0 | ||||||||
| 7 | He sold his house /ən/ moved to the farm | 0 | 1 | 0 | 0 | 0 | 0 | 1 | |||||||
| 8 | Work in the garden until you’ve picked all the beans | 1 | 0 | 0 | 0 | 0 | 0 | ||||||||
| 9 | The artist /peɪtəd / painted (3) many pictures of the /fɑ: / no sorry | 0 | 1 | 0 | 0 | 0 | 0 | 4 | 1 | 2 | |||||
| 10 | This doctor doesn’t go to all of the towns | 0 | 1 | 0 | 0 | 0 | 0 | 3 | 1 * | ||||||
| 11 | She should be able to tell us when /ʃɜ: / (2) when she (.) is (.) performing | 0 | 1 | 0 | 0 | 0 | 0 | 4 | 1 | ||||||
| 12 | Why /dɒn / (.) that group (1) why doesn’t that group apply (.) for (.) money | 0 | 1 | 0 | 0 | 0 | 0 | 8 | 1 * | 1 | |||||
| 13 | Many /pi:pəl / (5) they were not able to get work because of the (.) weather | 0 | 1 | 0 | 0 | 0 | 0 | 6 | 2 * | 1 | |||||
| 14 | Did not attempt | ||||||||||||||
| Total | 6 | 7 | 0 | 0 | 0 | 0 | 26 | 5 | 1 | 4 | 0 | 1 | 0 | 0 | |
| ML: nfv-PPA patient | |||||||||||||||
| 1 | /teɪki ðə/ | 0 | 1 | 0 | 0 | 0 | 0 | 1 | |||||||
| 2 | /wɜ:ʳɪz ðə/ child | 1 | 0 | 0 | 0 | 0 | 0 | ||||||||
| 3 | /kɑ (2) ðə kɑ wɪl wuz nɒʔ rʌn/ | 0 | 1 | 0 | 0 | 0 | 0 | 2 ** | |||||||
| 4 | why /ɑ neɪ nɒʔ/ living here | 1 | 0 | 0 | 0 | 0 | 0 | ||||||||
| 5 | /ðɜ:ʳ beɪn peɪʔ ə ən tʃi (4) tʃeəʳz/ | 0 | 1 | 0 | 0 | 0 | 0 | 1 | |||||||
| 6 | /wɜ ə ju: goʊɪŋ tu: wɜ:ʳʔ nəʔ zə nə nətʃə (3) zʌmə/ | 1 | 0 | 0 | 0 | 0 | 0 | ||||||||
| 7 | / i: (.) sʊld ɪz haʊs əndə ðə wi: (4) fɑm/ | 0 | 1 | 0 | 0 | 0 | 0 | 3 | |||||||
| 8 | /wɜ:ʳk ən ðə gɑ:dən æn (4) bɪk tʃɒ gɒ ðə bi:nz/ | 0 | 1 | 0 | 0 | 0 | 0 | 4 | |||||||
| 9 | /ðɜ:ʳ ɑ:dɜ:ʳzd peɪʔ (3) / um / peɪndəd/… no | 0 | 1 | 0 | 0 | 0 | 0 | 8 | |||||||
| 10 | / ɪz (3) ɒl ðɜ:ʳ kʊntri: (1) ɒl ðɜ:ʳ (1) dɒz ɪn ðə kʊntri:/ | 0 | 1 | 0 | 0 | 0 | 0 | 7 | |||||||
| 11 | /i: wɒz/ no | 0 | 1 | 0 | 0 | 0 | 0 | 13 | |||||||
| 12 | /waɪz du ðə gruf (3) waɪʔs (4) wəz/ | 0 | 1 | 0 | 0 | 0 | 0 | 10 | |||||||
| 13 | Did not attempt | ||||||||||||||
| 14 | Did not attempt | ||||||||||||||
| Total | 3 | 9 | 0 | 0 | 0 | 0 | 47 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | |
| JC: sv-PPA patient | |||||||||||||||
| 1 | Take this home | 1 | 0 | 0 | 0 | 0 | 0 | ||||||||
| 2 | Where is the child? | 1 | 0 | 0 | 0 | 0 | 0 | ||||||||
| 3 | The car will not run | 1 | 0 | 0 | 0 | 0 | 0 | ||||||||
| 4 | Why are they not living here? | 1 | 0 | 0 | 0 | 0 | 0 | ||||||||
| 5 | The band played and the crowd cheered | 1 | 0 | 0 | 0 | 0 | 0 | ||||||||
| 6 | Where are you going to work next summer? | 1 | 0 | 0 | 0 | 0 | 0 | ||||||||
| 7 | He sold his house and they moved to the farm. | 1 | 0 | 0 | 0 | 0 | 0 | ||||||||
| 8 | Work in the garden until you have picked all the beans | 1 | 0 | 0 | 0 | 0 | 0 | ||||||||
| 9 | The artist painted many of the beautiful scenes in this valley | 1 | 0 | 0 | 0 | 0 | 0 | ||||||||
| 10 | This doctor does not travel to all the towns in this country | 0 | 1 | 0 | 0 | 0 | 0 | 1 | |||||||
| 11 | He should actually be able to tell us when she will actually be performing here | 0 | 1 | 0 | 0 | 0 | 0 | 2 ** | |||||||
| 12 | Why do members of that group never write to their representatives of their group for aid? | 0 | 1 | 0 | 0 | 0 | 0 | 3 ** | |||||||
| 13 | Many men and women were not able to get to their work because of the severe snowstorm | 0 | 1 | 0 | 0 | 0 | 0 | 1 ** | |||||||
| 14 | The members of the committee have agreed to hold their meeting on the first Tuesday of every month | 0 | 1 | 0 | 0 | 0 | 0 | 1 | |||||||
| Total | 9 | 5 | 0 | 0 | 0 | 0 | 0 | 8 | 0 | 0 | 0 | 0 | 0 | 0 | |
| (a) | Diagnostic Criteria for Logopenic Variant of PPA | Patient NS | (b) | Diagnostic Criteria for Non-Fluent Variant of PPA | Patient ML | (c) | Diagnostic Criteria for Semantic Variant of PPA | Patient JC |
|---|---|---|---|---|---|---|---|---|
| I. Clinical diagnosis of logopenic variant PPA | I. Clinical diagnosis of non-fluent/agrammatic variant PPA | I. Clinical diagnosis of semantic variant PPA | ||||||
| Both of the following core features must be present: | At least one of the following core features must be present: | Both of the following core features must be present: | ||||||
| 1. Impaired single-word retrieval in spontaneous speech and naming | ✓ | 1. Agrammatism in language production | ✓ | 1. Impaired confrontation naming | ✓ | |||
| 2. Impaired repetition of sentences and phrases | ✓ | 2. Effortful, halting speech with inconsistent speech sound errors and distortions (apraxia of speech) | ✓ | 2. Impaired single-word comprehension | ✓ | |||
| At least 3 of the following other features must be present: | At least 2 of 3 of the following other features must be present: | At least 3 of the following other features must be present: | ||||||
| 1. Speech (phonologic) errors in spontaneous speech and naming | ✓ | 1. Impaired comprehension of syntactically complex sentences | Unknown | 1. Impaired object knowledge, particularly for low-frequency or low-familiarity items | ✓ | |||
| 2. Spared single-word comprehension and object knowledge | ✓ | 2. Spared single-word comprehension | ✓ | 2. Surface dyslexia or dysgraphia | ✓ | |||
| 3. Spared motor speech | ✓ | 3. Spared object knowledge | ✓ | 3. Spared repetition | ✓ | |||
| 4. Absence of frank agrammatism | ✓ | II. Imaging-supported non-fluent/agrammatic variant diagnosis | 4. Spared speech production (grammar and motor speech) | ✓ | ||||
| II. Imaging-supported logopenic variant diagnosis | Both of the following criteria must be present: | II. Imaging-supported semantic variant diagnosis | ||||||
| Both of the following criteria must be present: | 1. Clinical diagnosis of non-fluent/agrammatic variant PPA | ✓ | Both of the following criteria must be present: | |||||
| 1. Clinical diagnosis of logopenic variant PPA | ✓ | 2. Imaging must show one or more of the following results: | 1. Clinical diagnosis of semantic variant PPA | ✓ | ||||
| 2. Imaging must show at least one of the following results: | a. Predominant left posterior fronto-insular atrophy on MRI or | ✓ | 2. Imaging must show one or more of the following results: | |||||
| a. Predominant left posterior perisylvian or parietal atrophy on MRI | ✓ | b. Predominant left posterior fronto-insular hypoperfusion or hypometabolism on SPECT or PET | Not available | a. Predominant anterior temporal lobe atrophy | ✓ | |||
| b. Predominant left posterior perisylvian or parietal hypoperfusion or hypometabolism on SPECT or PET | Not available | III. Non-fluent/agrammatic variant PPA with definite pathology | b. Predominant anterior temporal hypoperfusion or hypometabolism on SPECT or PET | Not available | ||||
| III. Logopenic variant PPA with definite pathology | Clinical diagnosis (criterion 1 below) and either criterion 2 or 3 must be present: | III. Semantic variant PPA with definite pathology | ||||||
| Clinical diagnosis (criterion 1 below) and either criterion 2 or 3 must be present: | 1. Clinical diagnosis of non-fluent/agrammatic variant PPA | ✓ | Clinical diagnosis (criterion 1 below) and either criterion 2 or 3 must be present: | |||||
| 1. Clinical diagnosis of logopenic variant PPA | ✓ | 2. Histopathologic evidence of a specific neurodegenerative pathology (e.g., FTLD-tau, FTLDTDP, AD, other) | Not available | 1. Clinical diagnosis of semantic variant PPA | ✓ | |||
| 2. Histopathologic evidence of a specific neurodegenerative pathology (e.g. AD, FTLD-tau, FTLD-TDP, other) | Not available | 3. Presence of a known pathogenic mutation | Not available | 2. Histopathologic evidence of a specific neurodegenerative pathology (e.g., FTLD-tau, FTLDTDP, AD, other) | Not available | |||
| 3. Presence of a known pathogenic mutation | Not available | 3. Presence of a known pathogenic mutation | Not available |
| ACE-III Total Score | <40 | 40–49 | 50–59 | 60–69 | 70–79 | 80–89 | 90–100 | ||
|---|---|---|---|---|---|---|---|---|---|
| AD | Spatial Span | Forward | 3.2 | 3.6 | 4.5 | 4.9 | 6.8 | 5.1 | - |
| Backward | 1.0 | 2.2 | 3.7 | 3.2 | 5.5 | 4.8 | - | ||
| Digit Span | Forward | 4.2 | 6.5 | 8.7 | 8.1 | 8.4 | 8.7 | - | |
| Backward | 1.6 | 2.9 | 3.7 | 3.7 | 5.1 | 5.3 | - | ||
| lv-PPA | Spatial Span | Forward | 4.8 | 4.3 | 4.0 | 5.6 | 6.8 | 8.0 | 9.0 |
| Backward | 3.0 | 4.5 | 2.7 | 5.4 | 6.4 | 7.7 | 8.0 | ||
| Digit Span | Forward | 4.0 | 5.0 | 5.7 | 5.9 | 8.4 | 9.3 | 9.0 | |
| Backward | 2.3 | 2.0 | 2.3 | 4.0 | 4.6 | 6.3 | 8.0 | ||
| nfv-PPA | Spatial Span | Forward | 5.0 | - | 5.0 | 6.0 | 8.5 | 7.6 | 7.0 |
| Backward | 4.0 | - | 2.5 | 3.5 | 6.0 | 6.7 | 8.0 | ||
| Digit Span | Forward | - | - | 5.0 | 6.0 | 6.3 | 7.5 | 10.0 | |
| Backward | 2.0 | - | 2.0 | 3.0 | 4.2 | 4.8 | 5.7 | ||
| sv-PPA | Spatial Span | Forward | 6.8 | 7.3 | 8.5 | 8.1 | 8.4 | 9.4 | 8.0 |
| Backward | 6.5 | 4.7 | 7.8 | 8.1 | 8.8 | 9.2 | 9.0 | ||
| Digit Span | Forward | 8.5 | 11.0 | 9.0 | 9.7 | 12.2 | 12.6 | 8.0 | |
| Backward | 5.8 | 5.7 | 5.3 | 5.8 | 8.0 | 8.2 | 8.0 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foxe, D.; Cheung, S.C.; Cordato, N.J.; Burrell, J.R.; Ahmed, R.M.; Taylor-Rubin, C.; Irish, M.; Piguet, O. Verbal Short-Term Memory Disturbance in the Primary Progressive Aphasias: Challenges and Distinctions in a Clinical Setting. Brain Sci. 2021, 11, 1060. https://doi.org/10.3390/brainsci11081060
Foxe D, Cheung SC, Cordato NJ, Burrell JR, Ahmed RM, Taylor-Rubin C, Irish M, Piguet O. Verbal Short-Term Memory Disturbance in the Primary Progressive Aphasias: Challenges and Distinctions in a Clinical Setting. Brain Sciences. 2021; 11(8):1060. https://doi.org/10.3390/brainsci11081060
Chicago/Turabian StyleFoxe, David, Sau Chi Cheung, Nicholas J. Cordato, James R. Burrell, Rebekah M. Ahmed, Cathleen Taylor-Rubin, Muireann Irish, and Olivier Piguet. 2021. "Verbal Short-Term Memory Disturbance in the Primary Progressive Aphasias: Challenges and Distinctions in a Clinical Setting" Brain Sciences 11, no. 8: 1060. https://doi.org/10.3390/brainsci11081060