
Longitudinal Changes in Temporospatial Gait Characteristics during the First Year Post-Stroke


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Gait Evaluation
2.3. Data Reduction
2.4. Statistical Analysis
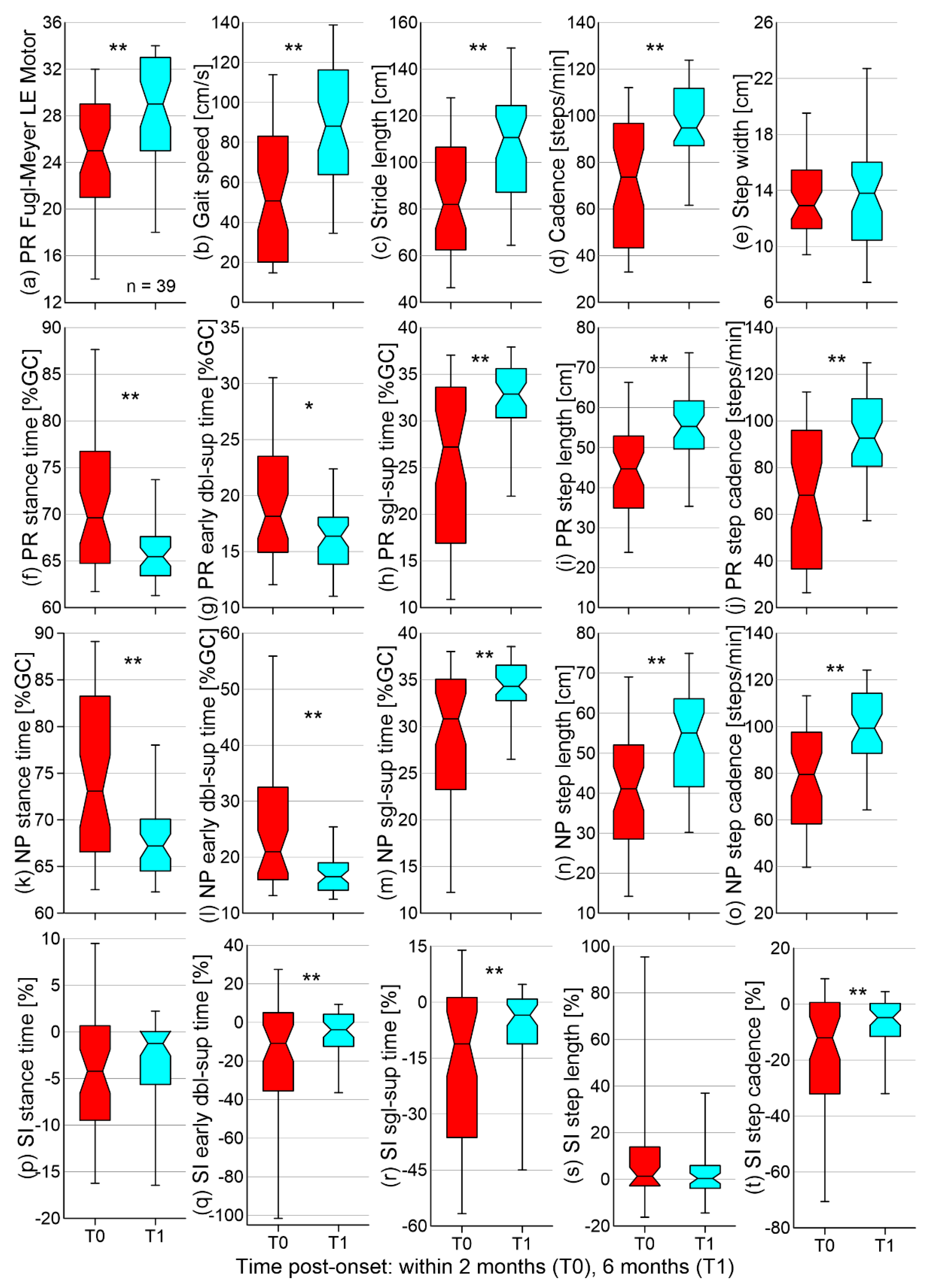
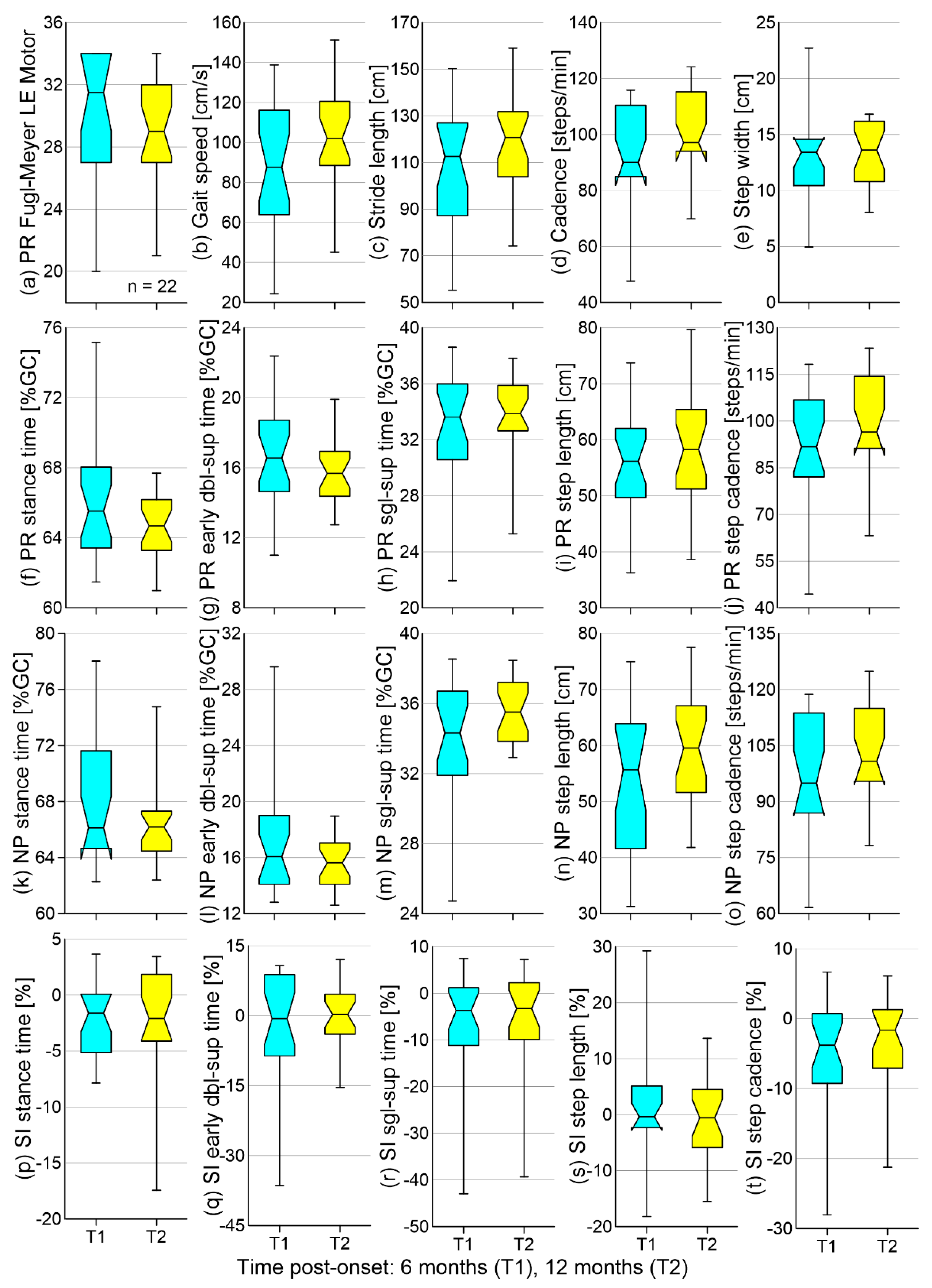
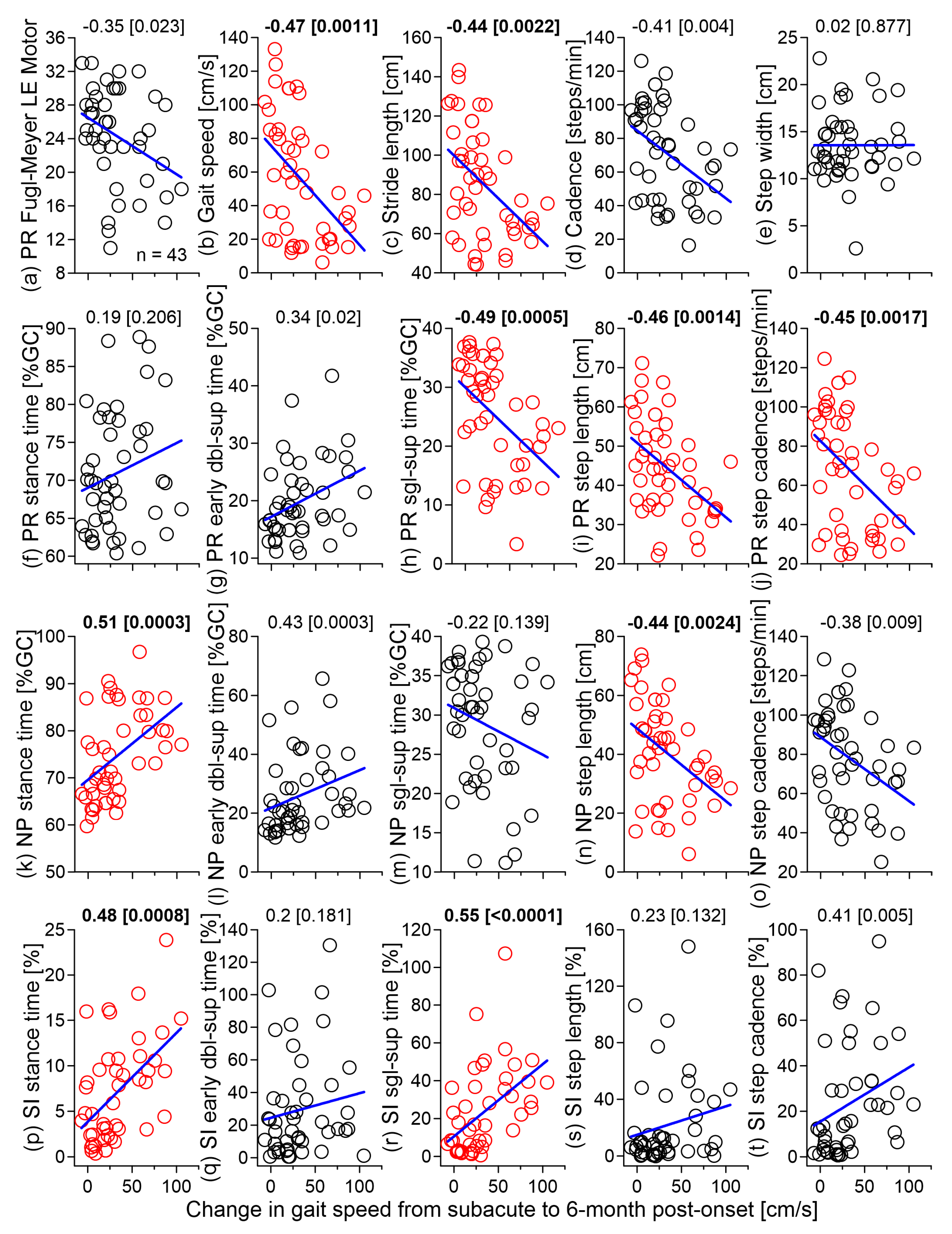
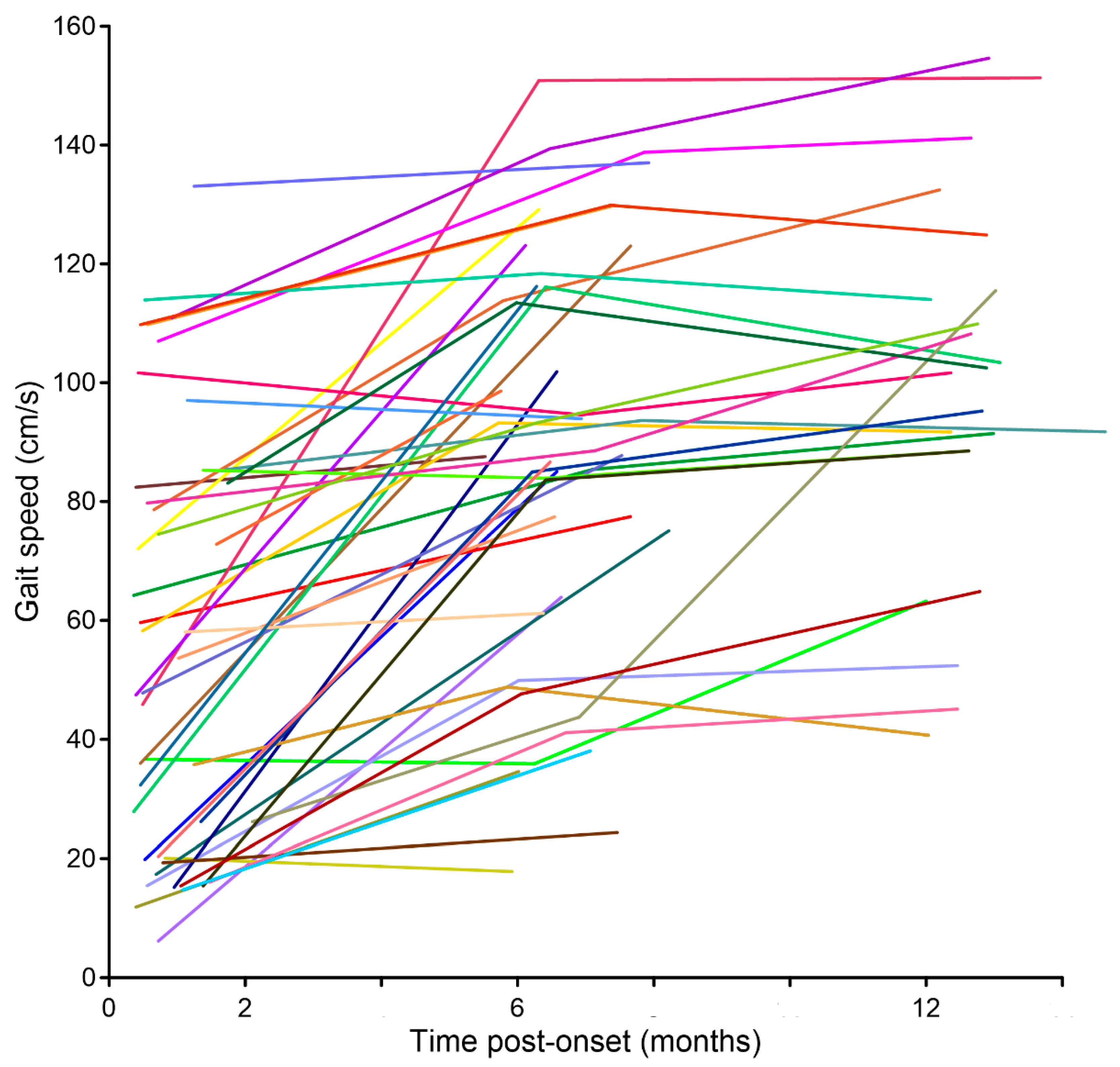
3. Results
4. Discussion
4.1. Longitudinal Changes
4.2. Relationship between Change in Gait Speed and Initial Gait Measures
4.3. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Determination of Speed Outcome

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stride # | Left | Right | Average |
|---|---|---|---|
| 1 | 0.653 | 0.656 | 0.655 |
| 2 | 0.737 | 0.745 | 0.741 |
| 3 | 0.719 | 0.694 | 0.706 |
| 4 | 0.646 * | - | - |
References
- Duncan, P.W.; Sullivan, K.J.; Behrman, A.L.; Azen, S.P.; Wu, S.S.; Nadeau, S.E.; Dobkin, B.H.; Rose, D.K.; Tilson, J.K.; Cen, S.; et al. Body-weight-supported treadmill rehabilitation after stroke. N. Engl. J. Med. 2011, 364, 2026–2036. [Google Scholar] [CrossRef] [PubMed]
- Katzan, I.; Schuster, A.; Kinzy, T. Physical activity monitoring using a Fitbit device in ischemic stroke patients: Prospective cohort feasibility study. JMIR Mhealth Uhealth 2021, 9, e14494. [Google Scholar] [CrossRef] [PubMed]
- Kollen, B.; van de Port, I.; Lindeman, E.; Twisk, J.; Kwakkel, G. Predicting improvement in gait after stroke: A longitudinal prospective study. Stroke 2005, 36, 2676–2680. [Google Scholar] [CrossRef] [PubMed]
- Mizukami, M.; Yoshikawa, K.; Kawamoto, H.; Sano, A.; Koseki, K.; Asakwa, Y.; Iwamoto, K.; Nagata, H.; Tsurushima, H.; Nakai, K.; et al. Gait training of subacute stroke patients using a hybrid assistive limb: A pilot study. Disabil. Rehabil. Assist. Technol. 2017, 12, 197–204. [Google Scholar] [CrossRef]
- Molteni, F.; Guanziroli, E.; Goffredo, M.; Calabrò, R.; Pournajaf, S.; Gaffuri, M.; Gasperini, G.; Filoni, S.; Baratta, S.; Galafate, D.; et al. Gait recovery with an overground powered exoskeleton: A randomized controlled trial on subacute stroke subjects. Brain Sci. 2021, 11, 104. [Google Scholar] [CrossRef]
- Yeung, L.-F.; Lau, C.C.Y.; Lai, C.W.K.; Soo, Y.O.Y.; Chan, M.-L.; Tong, R.K.Y. Effects of wearable ankle robotics for stair and over-ground training on sub-acute stroke: A randomized controlled trial. J. Neuroeng. Rehabil. 2021, 18, 19. [Google Scholar] [CrossRef]
- Brandstater, M.E.; de Bruin, H.; Gowland, C.; Clark, B.M. Hemiplegic gait: Analysis of temporal variables. Arch. Phys. Med. Rehabil. 1983, 64, 583–587. [Google Scholar]
- Chow, J.W.; Stokic, D.S. Gait impairments in patients without lower limb hypertonia early poststroke are related to weakness of paretic knee flexors. Arch. Phys. Med. Rehabil. 2019, 100, 1091–1101. [Google Scholar] [CrossRef]
- De Quervain, I.A.; Simon, S.R.; Leurgans, S.; Pease, W.S.; McAllister, D. Gait pattern in the early recovery period after stroke. J. Bone Joint Surg. Am. 1996, 78, 1506–1514. [Google Scholar] [CrossRef]
- Alingh, J.F.; Fleerkotte, B.M.; Groen, B.E.; Rietman, J.S.; Weerdesteyn, V.; van Asseldonk, E.H.F.; Geurts, A.C.H.; Buurke, J.H. Effect of assist-as-needed robotic gait training on the gait pattern post stroke: A randomized controlled trial. J. Neuroeng. Rehabil. 2021, 18, 1–12. [Google Scholar] [CrossRef]
- Ji, S.G.; Kim, M.K. The effects of mirror therapy on the gait of subacute stroke patients: A randomized controlled trial. Clin. Rehabil. 2014, 29, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Noh, H.-J.; Lee, S.-H.; Bang, D.-H. Three-dimensional balance training using visual feedback on balance and walking ability in subacute stroke patients: A single-blinded randomized controlled pilot trial. J. Stroke Cerebrovasc. Dis. 2019, 28, 994–1000. [Google Scholar] [CrossRef] [PubMed]
- Van Bloemendaal, M.; Bus, S.A.; Nollet, F.; Geurts, A.C.H.; Beelen, A. Feasibility and preliminary efficacy of gait training assisted by multichannel functional electrical stimulation in early stroke rehabilitation: A pilot randomized controlled trial. Neurorehabil. Neural Repair 2021, 35, 131–144. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.R.; Yen, J.G.; Wang, R.Y.; Yen, L.L.; Lieu, F.K. Gait outcomes after additional backward walking training in patients with stroke: A randomized controlled trial. Clin. Rehabil. 2005, 19, 264–273. [Google Scholar] [CrossRef] [PubMed]
- Aaslund, M.K.; Moe-Nilssen, R.; Gjelsvik, B.B.; Bogen, B.; Næss, H.; Hofstad, H.; Skouen, J.S. A longitudinal study investigating how stroke severity, disability, and physical function the first week post-stroke are associated with walking speed six months post-stroke. Physiother. Theory Pract. 2017, 33, 932–942. [Google Scholar] [CrossRef] [PubMed]
- Berges, I.-M.; Kuo, Y.-F.; Ottenbacher, K.J.; Seale, G.S.; Ostir, G.V. Recovery of functional status after stroke in a tri-ethnic population. PM&R 2012, 4, 290–295. [Google Scholar] [CrossRef]
- Kollen, B.; Kwakkel, G.; Lindeman, E. Hemiplegic gait after stroke: Is measurement of maximum speed required? Arch. Phys. Med. Rehabil. 2006, 87, 358–363. [Google Scholar] [CrossRef]
- O’Dell, M.W.; Jaywant, A.; Frantz, M.; Patel, R.; Kwong, E.; Wen, K.; Taub, M.; Campo, M.; Toglia, J. Changes in the activity measure for post-acute care domains in persons with stroke during the first year after discharge from inpatient rehabilitation. Arch. Phys. Med. Rehabil. 2021, 102, 645–655. [Google Scholar] [CrossRef]
- Ullberg, T.; Zia, E.; Petersson, J.; Norrving, B. Changes in functional outcome over the first year after stroke: An observational study from the Swedish stroke register. Stroke 2015, 46, 389–394. [Google Scholar] [CrossRef]
- Rozanski, G.M.; Wong, J.S.; Inness, E.L.; Patterson, K.K.; Mansfield, A. Longitudinal change in spatiotemporal gait symmetry after discharge from inpatient stroke rehabilitation. Disabil. Rehabil. 2020, 42, 705–711. [Google Scholar] [CrossRef]
- Shin, S.Y.; Lee, R.K.; Spicer, P.; Sulzer, J. Does kinematic gait quality improve with functional gait recovery? A longitudinal pilot study on early post-stroke individuals. J. Biomech. 2020, 105, 109761. [Google Scholar] [CrossRef] [PubMed]
- Kwakkel, G.; Kollen, B.J.; Wagenaar, R.C. Long term effects of intensity of upper and lower limb training after stroke: A randomised trial. J. Neurol. Neurosurg. Psychiatry 2002, 72, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar] [PubMed]
- Sanford, J.; Moreland, J.; Swanson, L.R.; Stratford, P.W.; Gowland, C. Reliability of the Fugl-Meyer assessment for testing motor performance in patients following stroke. Phys. Ther. 1993, 73, 447–454. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Smith, M.B. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys. Ther. 1987, 67, 206–207. [Google Scholar] [CrossRef]
- Kadaba, M.P.; Ramakrishnan, H.K.; Wootten, M.E. Measurement of lower extremity kinematics during level walking. J. Orthop. Res. 1990, 8, 383–392. [Google Scholar] [CrossRef]
- Stokic, D.S.; Horn, T.S.; Ramshur, J.M.; Chow, J.W. Agreement between temporospatial gait parameters of an electronic walkway and a motion capture system in healthy and chronic stroke populations. Am. J. Phys. Med. Rehabil. 2009, 88, 437–444. [Google Scholar] [CrossRef]
- Zeni, J.A., Jr.; Richards, J.G.; Higginson, J.S. Two simple methods for determining gait events during treadmill and overground walking using kinematic data. Gait Posture 2008, 27, 710–714. [Google Scholar] [CrossRef]
- Wang, Y.; Mukaino, M.; Ohtsuka, K.; Otaka, Y.; Tanikawa, H.; Matsuda, F.; Tsuchiyama, K.; Yamada, J.; Saitoh, E. Gait characteristics of post-stroke hemiparetic patients with different walking speeds. Int. J. Rehabil. Res. 2020, 43, 69–75. [Google Scholar] [CrossRef]
- Fagerland, M.W.; Sandvik, L. Performance of five two-sample location tests for skewed distributions with unequal variances. Contemp. Clin. Trials 2009, 30, 490–496. [Google Scholar] [CrossRef]
- Ruxton, G.D. The unequal variance t-test is an underused alternative to Student’s t-test and the Mann-Whitney U test. Behav. Ecol. 2006, 17, 688–690. [Google Scholar] [CrossRef]
- Lewek, M.D.; Sykes, R. Minimal detectable change for gait speed depends on baseline speed in individuals with chronic stroke. J. Neurol. Phys. Ther. 2019, 43, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Akoglu, H. User’s guide to correlation coefficients. Turkish J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef] [PubMed]
- Schober, P.; Schwarte, L.A. Correlation coefficients: Appropriate use and interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef] [PubMed]
- Duncan, P.; Studenski, S.; Richards, L.; Gollub, S.; Lai, S.M.; Reker, D.; Perera, S.; Yates, J.; Koch, V.; Rigler, S.; et al. Randomized clinical trial of therapeutic exercise in subacute stroke. Stroke 2003, 34, 2173–2180. [Google Scholar] [CrossRef]
- Bonita, R.; Beaglehole, R. Recovery of motor function after stroke. Stroke 1988, 19, 1497–1500. [Google Scholar] [CrossRef]
- Branvo, J.P.; Oliveira, S.; Sargento-Freitas, J.; Laíns, J.; Pinheiro, J. Assessing functional recovery in the first six months after acute ischemic stroke: A prospective, observational study. Eur. J. Phys. Rehabil. Med. 2019, 55, 1–7. [Google Scholar] [CrossRef]
- De Wit, L.; Putman, K.; Schuback, B.; Komárek, A.; Angst, F.; Baert, I.; Berman, P.; Bogaerts, K.; Brinkmann, N.; Connell, L.; et al. Motor and functional recovery after stroke: A comparison of 4 European rehabilitation centers. Stroke 2007, 38, 2101–2107. [Google Scholar] [CrossRef]
- Jorgensen, H.S.; Nakayama, H.; Raaschou, H.O.; Vive-Larsen, J.; Støier, M.; Olsen, T.S. Outcome and time course of recovery in stroke. Part I: Outcome. The Copenhagen stroke study. Arch. Phys. Med. Rehabil. 1995, 76, 399–405. [Google Scholar] [CrossRef]
- Kwakkel, G.; Kollen, B.; Twisk, J. Impact of time on improvement of outcome after stroke. Stroke 2006, 37, 2348–2353. [Google Scholar] [CrossRef]
- Verheyden, G.; Nieuwboer, A.; De, W.L.; Thijs, V.; Dobbelaere, J.; Devos, H.; Severijns, D.; Vanbeveren, S.; De, W.W. Time course of trunk, arm, leg, and functional recovery after ischemic stroke. Neurorehabil. Neural Repair 2008, 22, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W.; Andrews, A.W.; Glenney, S.S. Minimal clinically important difference for comfortable speed as a measure of gait performance in patients undergoing inpatient rehabilitation after stroke. J. Phys. Ther. Sci. 2013, 25, 1223–1225. [Google Scholar] [CrossRef] [PubMed]
- Fulk, G.D.; Ludwig, M.; Dunning, K.; Golden, S.; Boyne, P.; West, T. Estimating clinically important change in gait speed in people with stroke undergoing outpatient rehabilitation. J. Neurol. Phys. Ther. 2011, 35, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Geiger, M.; Supiot, A.; Pradon, D.; Do, M.C.; Zory, R.; Roche, N. Minimal detectable change of kinematic and spatiotemporal parameters in patients with chronic stroke across three sessions of gait analysis. Hum. Mov. Sci. 2019, 64, 101–107. [Google Scholar] [CrossRef]
- Lewek, M.D.; Randall, E.P. Reliability of spatiotemporal asymmetry during overground walking for individuals following chronic stroke. J. Neurol. Phys. Ther. 2011, 35, 116–121. [Google Scholar] [CrossRef]
- Tilson, J.K.; Sullivan, K.J.; Cen, S.Y.; Rose, D.K.; Koradia, C.H.; Azen, S.P.; Duncan, P.W. Locomotor Experience Applied Post Stroke (LEAPS) Investigative Team Meaningful gait speed improvement during the first 60 days poststroke: Minimal clinically important difference. Phys. Ther. 2010, 90, 196–208. [Google Scholar] [CrossRef]
- Beaton, D.E.; Boers, M.; Wells, G.A. Many faces of the minimal clinically important difference (MCID): A literature review and directions for future research. Curr. Opin. Rheumatol. 2002, 14, 109–114. [Google Scholar] [CrossRef]
- Copay, A.G.; Subach, B.R.; Glassman, S.D.; Polly, D.W.; Schuler, T.C. Understanding the minimum clinically important difference: A review of concepts and methods. Spine J. 2007, 7, 541–546. [Google Scholar] [CrossRef]
- Stratford, P.W.; Riddle, D.L. When minimal detectable change exceeds a diagnostic test-based threshold change value for an outcome measure: Resolving the conflict. Phys. Ther. 2012, 92, 1338–1347. [Google Scholar] [CrossRef]
- Schmid, A.; Duncan, P.W.; Studenski, S.; Lai, S.M.; Richards, L.; Perera, S.; Wu, S.S. Improvements in speed-based gait classifications are meaningful. Stroke 2007, 38, 2096–2100. [Google Scholar] [CrossRef]
- Hsu, A.-L.; Tang, P.-F.; Jan, M.-H. Analysis of impairments influencing gait velocity and asymmetry of hemiplegic patients after mild to moderate stroke. Arch. Phys. Med. Rehabil. 2003, 84, 1185–1193. [Google Scholar] [CrossRef]
- Kim, W.-S.; Choi, H.; Jung, J.-W.; Yoon, J.S.; Jeoung, J.H. Asymmetry and variability should be included in the assessment of gait function in poststroke hemiplegia with independent ambulation during early rehabilitation. Arch. Phys. Med. Rehabil. 2021, 102, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Spaich, E.; Svaneborg, N.; Jørgensen, H.R.; Andersen, O. Rehabilitation of the hemiparetic gait by nociceptive withdrawal reflex-based functional electrical therapy: A randomized, single-blinded study. J. Neuroeng. Rehabil. 2014, 11, 81. [Google Scholar] [CrossRef] [PubMed]
- Duncan, P.W.; Goldstein, L.B.; Horner, R.D.; Landsman, P.B.; Samsa, G.P.; Matchar, D.B. Similar motor recovery of upper and lower extremities after stroke. Stroke 1994, 25, 1181–1188. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.-C.; Byblow, W.D.; Barber, P.A.; Stinear, C.M. Proportional recovery from lower limb motor impairment after stroke. Stroke 2017, 48, 1400–1403. [Google Scholar] [CrossRef]




| ID | Sex | Age | BMI | Onset to T0 | Paretic | Paretic<break/>FM-LE | Gait Speed [m/s] | Speed Change [m/s] | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [year] | [Days] | Side | T0 | T1 | T2 | T0 | T1 | T2 | T1-T0 * | T2-T1 # | |||
| 1 | M | 74 | 27 | 16 | L | na | 33 | – | 0.20 (0.03) W | 0.85 (0.05) C | – | 0.65 | – |
| 2 | M | 74 | 26 | 16 | L | na | 24 | 27 | 0.37 (0.03) W | 0.36 (0.05) W | 0.63 (0.05) C | −0.01 | 0.27 |
| 3 | M | 82 | 23 | 12 | L | 30 | 34 | – | 0.79 (0.05) | 0.87 (0.04) | – | 0.08 | – |
| 4 | M | 65 | 26 | 13 | L | 32 | 34 | – | 0.72 (0.06) | 1.28 (0.07) | – | 0.56 | – |
| 5 | F | 54 | 25 | 14 | L | 24 | 27 | – | 0.59 (0.07) C | 0.78 (0.06) C | – | 0.19 | – |
| 6 | M | 59 | 28 | 22 | L | 16 | 22 | – | 0.7 (0.02) OW | 0.64 (0.03) OC | – | 0.57 | – |
| 7 | M | 72 | 36 | 11 | L | 31 | 32 | 32 | 0.63 (0.07) W | 0.85 (0.07) | 0.91 (0.04) | 0.22 | 0.06 |
| 8 | M | 73 | 35 | 20 | R | 32 | na | 34 | 0.78 (0.05) | 1.13 (0.06) | 1.32 (0.04) | 0.35 | 0.19 |
| 9 | F | 63 | 36 | 25 | R | 28 | 31 | – | 0.20 (0.02) C | 0.16 (0.02) W | – | −0.04 | – |
| 10 | M | 42 | 30 | 15 | L | 18 | 33 | 27 | 0.46 (0.04) C | 1.51 (0.03) | 1.51 (0.06) | 1.05 | 0.00 |
| 11 | M | 55 | 26 | 17 | R | 16 | 19 | 21 | 0.16 (0.02) C | 0.50 (0.02) C | 0.52 (0.02) C | 0.34 | 0.02 |
| 12 | F | 70 | 30 | 21 | R | 23 | 31 | – | 0.17 (0.02) | 0.76 (0.09) | – | 0.59 | – |
| 13 | F | 39 | 32 | 14 | L | 28 | 29 | – | 0.36 (0.02) | 1.24 (0.10) | – | 0.88 | – |
| 14 | M | 49 | 32 | 12 | R | 14 | 20 | – | 0.12 (0.01) OC | 0.37 (0.03) OC | – | 0.25 | – |
| 15 | F | 61 | 23 | 22 | L | 30 | 34 | 34 | 1.07 (0.05) | 1.40 (0.10) | 1.41 (0.09) | 0.33 | 0.01 |
| 16 | F | 48 | 38 | 29 | L | 14 | 24 | – | 0.16 (0.03) C | 1.02 (0.13) C | – | 0.86 | – |
| 17 | M | 49 | 33 | 11 | R | 17 | 33 | 30 | 0.28 (0.04) | 1.16 (0.09) | 1.04 (0.08) | 0.88 | −0.12 |
| 18 | M | 67 | 26 | 24 | R | 27 | na | – | 0.19 (0.02) C | 0.25 (0.04) C | – | 0.06 | – |
| 19 | F | 73 | 24 | 15 | L | 30 | 34 | 32 | 0.60 (0.07) C | 0.94 (0.12) C | 0.92 (0.06) | 0.34 | −0.02 |
| 20 | M | 65 | 29 | 12 | L | 33 | 34 | 30 | 1.02 (0.03) | 0.94 (0.07) | 1.02 (0.03) | −0.08 | 0.08 |
| 21 | M | 48 | 33 | 15 | L | 23 | 29 | – | 0.48 (0.03) | 0.87 (0.04) | – | 0.39 | – |
| 22 | M | 76 | 28 | 9 | L | 24 | 34 | 31 | 1.23 (0.03) | 1.29 (0.09) | 1.20 (0.10) | 0.06 | −0.09 |
| 23 | M | 56 | 25 | 38 | L | 23 | na | na | 0.36 (0.04) OC | 0.49 (0.04) OC | 0.41 (0.02) OC | 0.13 | −0.08 |
| 24 | M | 57 | 28 | 60 | L | 21 | 32 | 32 | 0.26 (0.02) | 0.44 (0.08) | 1.14 (0.08) | 0.18 | 0.70 |
| 25 | F | 75 | 21 | 12 | R | 29 | 32 | – | 0.48 (0.03) W | 1.23 (0.07) | – | 0.75 | – |
| 26 | F | 75 | 23 | 38 | L | 33 | 34 | – | 1.33 (0.09) | 1.37 (0.05) | – | 0.04 | – |
| 27 | F | 57 | 31 | 52 | R | 25 | 29 | 25 | 0.85 (0.04) | 0.94 (0.08) | 0.91 (0.06) O | 0.09 | −0.03 |
| 28 | F | 44 | 33 | 48 | R | 23 | 29 | – | 0.73 (0.05) | 0.99 (0.05) | – | 0.26 | – |
| 29 | F | 32 | 33 | 31 | L | 26 | 28 | – | 0.54 (0.03) | 0.77 (0.04) | – | 0.23 | – |
| 30 | M | 53 | 29 | 45 | R | 11 | 18 | 22 | 0.16 (0.01) W | 0.41 (0.03) C | 0.45 (0.02) C | 0.25 | 0.04 |
| 31 | M | 63 | 27 | 35 | L | 24 | 28 | – | 0.96 (0.07) C | 0.93 (0.04) | – | −0.03 | – |
| 32 | F | 61 | 35 | 42 | L | 25 | 32 | 29 | 0.85 (0.03) | 0.83 (0.09) | 0.89 (0.08) | −0.02 | 0.06 |
| 33 | F | 51 | 22 | 17 | R | 26 | na | – | 1.09 (0.06) | 1.29 (0.012) | – | 0.20 | – |
| 34 | F | 54 | 33 | 34 | L | 27 | 27 | – | 0.56 (0.10) | 0.59 (0.012) C | – | 0.03 | – |
| 35 | F | 67 | 41 | 17 | L | 29 | 34 | 27 | 0.79 (0.07) | 0.87 (0.10) | 1.07 (0.09) | 0.08 | 0.20 |
| 36 | M | 48 | 32 | 41 | R | 24 | 25 | 29 | 0.26 (0.03) OC | 0.85 (0.03) | 0.96 (0.06) O | 0.59 | 0.11 |
| 37 | F | 61 | 24 | 42 | L | 25 | 32 | 29 | 0.15 (0.02) | 0.83 (0.08) | 0.89 (0.08) | 0.68 | 0.06 |
| 38 | M | 57 | 26 | 32 | R | 18 | 18 | 12 | 0.15 (0.02) OC | 0.48 (0.03) OC | 0.65 (0.05) O | 0.33 | 0.17 |
| 39 | M | 66 | 30 | 16 | L | 28 | 30 | 33 | 1.15 (0.17) | 1.19 (0.08) | 1.13 (0.10) | 0.04 | −0.06 |
| 40 | M | 57 | 25 | 28 | R | 30 | 30 | 30 | 1.11 (0.10) | 1.39 (0.03) | 1.54 (0.06) | 0.28 | 0.15 |
| 41 | F | 55 | 33 | 14 | R | 21 | 27 | – | 0.33 (0.01) | 1.18 (0.10) | – | 0.85 | – |
| 42 | F | 49 | 34 | 53 | R | na | 25 | 25 | 0.83 (0.06) | 1.12 (0.15) | 1.02 (0.09) | 0.29 | −0.10 |
| 43 | F | 51 | 22 | 14 | R | 26 | 29 | 29 | 1.09 (0.06) | 1.29 (0.12) | 1.23 (0.11) | 0.20 | −0.06 |
| 44 | M | 71 | 28 | 22 | L | 28 | 27 | 29 | 0.74 (0.06) | 0.93 (0.10) | 1.10 (0.04) | 0.19 | 0.17 |
| 45 | M | 64 | 27 | 22 | R | 19 | 22 | – | 0.20 (0.02) C | 0.86 (0.07) C | – | 0.66 | – |
| 46 | F | 65 | 27 | 33 | L | 13 | 13 | – | 0.15 (0.02) W | 0.38 (0.04) C | – | 0.23 | – |
| Mean | 59.7 | 29.0 | 25.0 | 24.3 | 28.4 | 28.2 | 0.56 | 0.89 | 1.00 | 0.33 | 0.07 | ||
| SD | 11.1 | 4.7 | 13.3 | 5.8 | 5.3 | 4.9 | 0.36 | 0.24 | 0.31 | 0.30 | 0.17 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chow, J.W.; Stokic, D.S. Longitudinal Changes in Temporospatial Gait Characteristics during the First Year Post-Stroke. Brain Sci. 2021, 11, 1648. https://doi.org/10.3390/brainsci11121648
Chow JW, Stokic DS. Longitudinal Changes in Temporospatial Gait Characteristics during the First Year Post-Stroke. Brain Sciences. 2021; 11(12):1648. https://doi.org/10.3390/brainsci11121648
Chicago/Turabian StyleChow, John W., and Dobrivoje S. Stokic. 2021. "Longitudinal Changes in Temporospatial Gait Characteristics during the First Year Post-Stroke" Brain Sciences 11, no. 12: 1648. https://doi.org/10.3390/brainsci11121648