
Necessity and Content of Swing Phase Gait Coordination Training Post Stroke; A Case Report


Abstract
:1. Introduction
2. Methods
2.1. Case Characteristics
2.2. Measures
2.3. Interventions
2.3.1. Motor Learning Treatment Component
- “Percentage of the normal range of movement that could be executed, volitionally and independently.
- Percentage of the motor task that could be executed with the support of verbal or tactile facilitation.
- Percentage of the normal range of movement that could be executed along with an assistive movement device.
- Normality of effort level during the task (e.g., holding breath, abnormal co-contraction of muscles distant from the targeted task joints or antagonist muscle contractions).
- Compensatory strategies employed during execution of the motor task.
- Percentage of the task for which compensatory strategies were employed.
- Number of repetitions of the motor task that could be performed with only a “beat” between repetitions before the motor task was performed in an “abnormal fashion” (with permission [31]).
2.3.2. FES Assist in Motor Learning
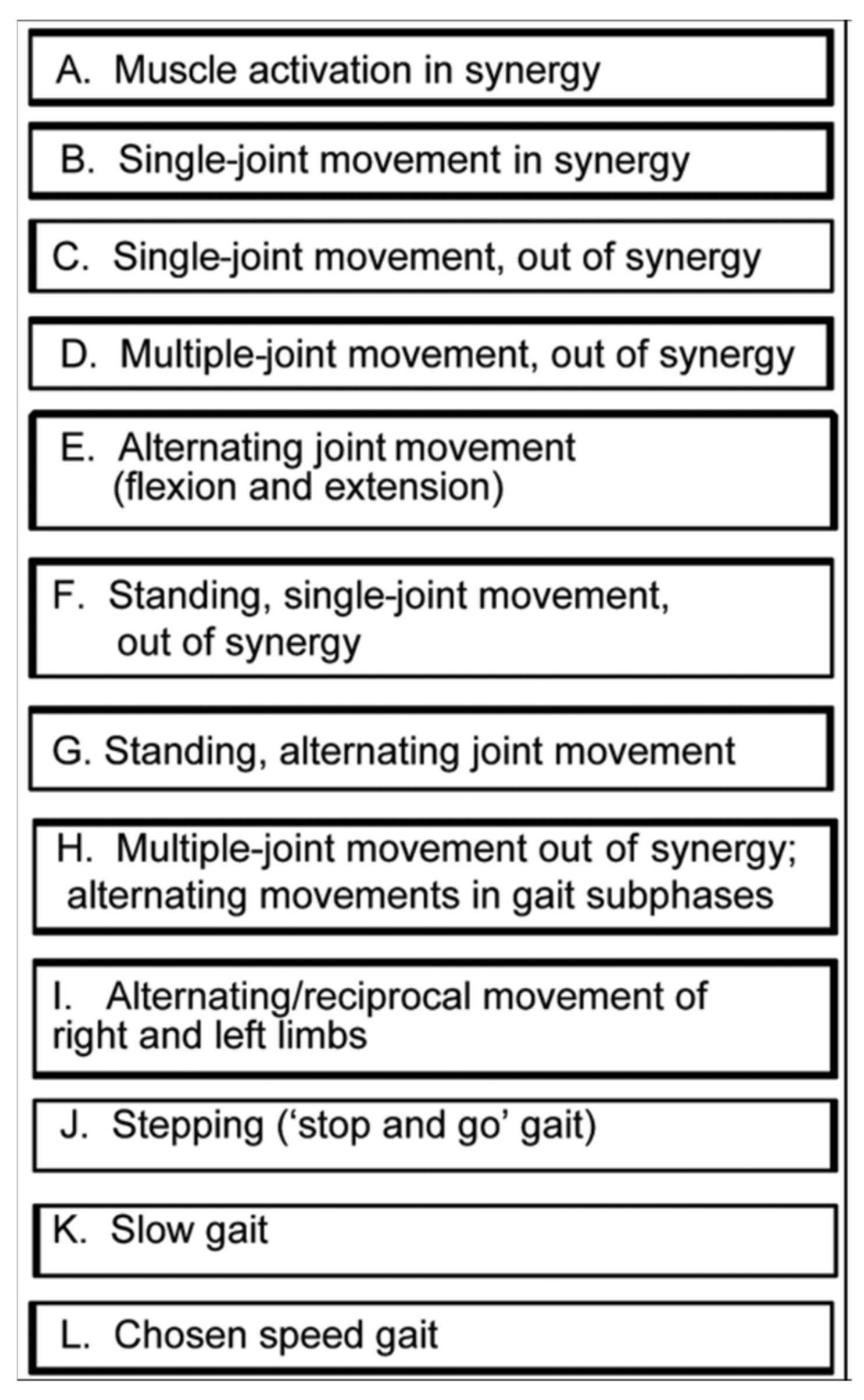
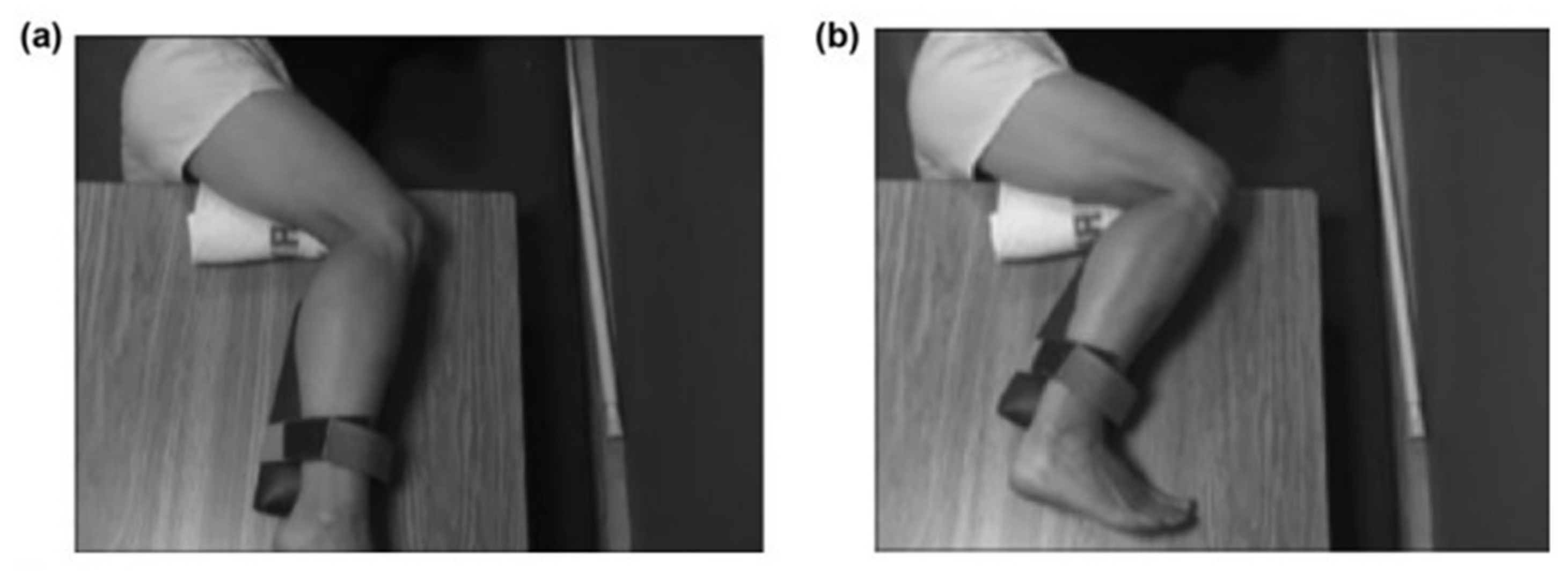
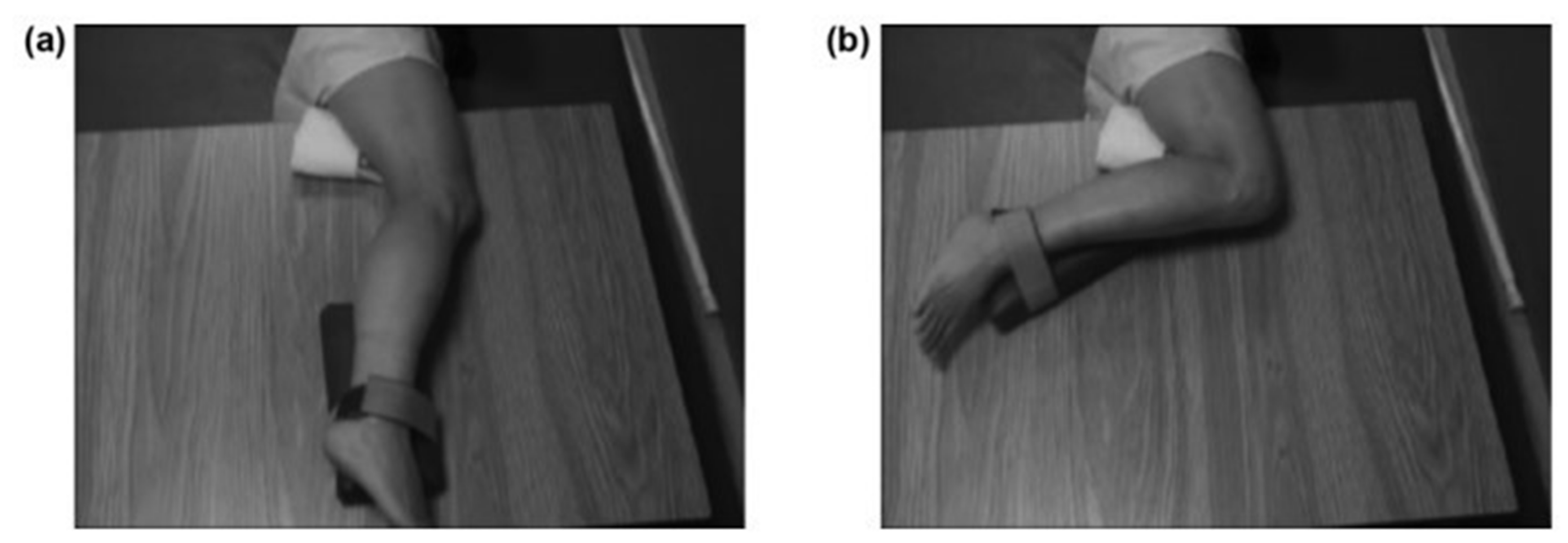
2.3.3. Progression from Side-Lying to Sitting Positions and Upright Standing
- Fifty percent of normal range of movement is executed, volitionally, independently; or 50 percent of motor task is executed with support of verbal or tactile facilitation; or 50 percent of normal range of movement is executed, along with motor assist device.
- Normal level of effort is expended during task (no holding breath or associative reactions in other limbs or trunk; relaxed uninvolved muscles).
- If motor compensatory strategies are employed, less than 10 degrees of movement is performed that is compensatory in nature.
- If motor compensatory strategies are employed, at least half of motor task is performed without compensatory strategies.
- Five or more repetitions of motor task can be performed in a row with only a “beat” between before motor task deteriorates into uncoordinated or incorrect.
Body Position and Limb Position Progression
- Side-lying position
- Sitting and standing positions
- Awareness training
2.3.4. Body Weight Support
2.3.5. Treadmill Use
2.4. Data Analysis
3. Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A. Measure | B. Pre | C. Post | D. Gain/Improvement |
|---|---|---|---|
| Impairment Measures | |||
| 1. FM Total Score (34, max); Items that changed: | 27 | 30 | 3 |
| Item: Ankle dorsiflexion, | 1 | 2 | 1 |
| Item: Knee Flx, sit, combined synergy | 3 | 4 | 1 |
| Item: KnFx, Stnd, out of synergy | 2 | 3 | 1 |
| 2. mAshworth (0, normal), item that changed: | |||
| Item: Knee extensors | 1 | 0 | 1 |
| 3. Muscle Strength | |||
| External hip rotators | 4+ | 5 | gain |
| Internal hip rotators | 3− | 3− | No change |
| Knee flexors | 4 | 4 | No change |
| Ankle evertors | 4+ | 4+ | No change |
| All other muscles | 5 | 5 | No change |
| 4. G.A.I.T. Overall Score (0 is normal; item scores, Table 2) | 25 | 13 | 12 |
| Functional Mobility Measure | |||
| 5. 6 MWT (feet) | 582 | 1114 | 532 * |
| meters | 77 | 339 | 162 |
| Speed (derived from 6MWT) | 0.49 m/s | 0.94 m/s | 0.45 m/s |
| * MCID > 233′ [29]. | |||
| Life Role Participation Measure | |||
| 6. SIS (Domain scores in separate Table below) | 293 | 305 | 12 * |
| * MCID = 10–15 points [30]. | |||
3.1. Impairment
- Swing phase Kinematics
- Muscle activation latencies
3.2. Functional Mobility
3.3. Life Role Participation
4. Discussion
4.1. Strength Is a Necessary Pre-Requisite, but Not Sufficient to Restore Normal Gait after Stroke, if Gait Dyscoordination Is Present
4.2. Relationship between Knee Flexion Coordination and Swing Phase Gait Coordination
4.3. Relationships among the Variables of Gait Coordination, Gait Speed, Function, and Life Role Participation
4.4. Advantages of the Combined Interventions
4.5. Limitations
5. Conclusions/Contribution to the Field
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kuptniratsaikul, V.; Kovindha, A.; Suethanapornkul, S.; Massakulpan, P.; Permsirivanich, W.; Kuptniratsaikul, P.S. Motor Recovery of Stroke Patients after Rehabilitation: One-Year Follow-up Study. Int. J. Neurosci. 2017, 127, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Krasovsky, T.; Levin, M.F. Review: Toward a Better Understanding of Coordination in Healthy and Poststroke Gait. Neurorehabil. Neural. Repair 2010, 24, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Sung, D.H.; Bang, H.J. Motor Branch Block of the Rectus Femoris: Its Effectiveness in Stiff-Legged Gait in Spastic Paresis. Arch. Phys. Med. Rehabil. 2000, 81, 910–915. [Google Scholar] [CrossRef]
- Li, S.; Francisco, G.E.; Zhou, P. Post-Stroke Hemiplegic Gait: New Perspective and Insights. Front. Physiol. 2018, 9, 1021. [Google Scholar] [CrossRef] [Green Version]
- Luckie, H.; Hollands, K.; Williamson, T.; Nester, C.; Williams, A. Comfortably Numb? Experiences of People with Stroke and Lower Limb Sensation Deficits: Impact and Solutions. Disabil. Rehabil. Assist. Technol. 2021, 16, 262–269. [Google Scholar] [CrossRef]
- Beyaert, C.; Vasa, R.; Frykberg, G.E. Gait Post-Stroke: Pathophysiology and Rehabilitation Strategies. Neurophysiol. Clin. Clin. Neurophysiol. 2015, 45, 335–355. [Google Scholar] [CrossRef] [PubMed]
- Sheffler, L.R.; Chae, J. Hemiparetic Gait. Phys. Med. Rehabil. Clin. North. Am. 2015, 26, 611–623. [Google Scholar] [CrossRef]
- Routson, R.L.; Clark, D.J.; Bowden, M.G.; Kautz, S.A.; Neptune, R.R. The Influence of Locomotor Rehabilitation on Module Quality and Post-Stroke Hemiparetic Walking Performance. Gait Posture 2013, 38, 511–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, W.; Li, K.; Yue, S.; Yin, C.; Wei, N. Associations between Lower-Limb Muscle Activation and Knee Flexion in Post-Stroke Individuals: A Study on the Stance-to-Swing Phases of Gait. PLoS ONE 2017, 12, e0183865. [Google Scholar] [CrossRef] [Green Version]
- Souissi, H.; Zory, R.; Bredin, J.; Roche, N.; Gerus, P. Co-Contraction around the Knee and the Ankle Joints during Post-Stroke Gait. Eur. J. Phys. Rehabil Med. 2018, 54, 380–387. [Google Scholar] [CrossRef]
- Kerrigan, D.C.; Karvosky, M.E.; Riley, P.O. Spastic Paretic Stiff-Legged Gait: Joint Kinetics. Am. J. Phys. Med. Rehabil. 2001, 80, 244–249. [Google Scholar] [CrossRef]
- Lewek, M.D.; Hornby, T.G.; Dhaher, Y.Y.; Schmit, B.D. Prolonged Quadriceps Activity Following Imposed Hip Extension: A Neurophysiological Mechanism for Stiff-Knee Gait? J. Neurophysiol. 2007, 98, 3153–3162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akbas, T.; Kim, K.; Doyle, K.; Manella, K.; Lee, R.; Spicer, P.; Knikou, M.; Sulzer, J. Rectus Femoris Hyperreflexia Contributes to Stiff-Knee Gait after Stroke. J. Neuroeng. Rehabil. 2020, 17, 117. [Google Scholar] [CrossRef]
- Kerrigan, D.C.; Frates, E.P.; Rogan, S.; Riley, P.O. Hip Hiking and Circumduction: Quantitative Definitions. Am. J. Phys. Med. Rehabil. 2000, 79, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Ivey, F.M.; Prior, S.J.; Hafer-Macko, C.E.; Katzel, L.I.; Macko, R.F.; Ryan, A.S. Strength Training for Skeletal Muscle Endurance after Stroke. J. Stroke Cereb. Dis. 2017, 26, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Lamberti, N.; Straudi, S.; Malagoni, A.M.; Argirò, M.; Felisatti, M.; Nardini, E.; Zambon, C.; Basaglia, N.; Manfredini, F. Effects of Low-Intensity Endurance and Resistance Training on Mobility in Chronic Stroke Survivors: A Pilot Randomized Controlled Study. Eur. J. Phys. Rehabil. Med. 2017, 53, 228–239. [Google Scholar] [CrossRef]
- Pontes, S.S.; de Carvalho, A.L.R.; de Almeida, K.O.; Neves, M.P.; Ribeiro Schindler, I.F.S.; Alves, I.G.N.; Arcanjo, F.L.; Gomes-Neto, M. Effects of Isokinetic Muscle Strengthening on Muscle Strength, Mobility, and Gait in Post-Stroke Patients: A Systematic Review and Meta-Analysis. Clin. Rehabil. 2019, 33, 381–394. [Google Scholar] [CrossRef]
- Lattouf, N.A.; Tomb, R.; Assi, A.; Maynard, L.; Mesure, S. Eccentric Training Effects for Patients with Post-Stroke Hemiparesis on Strength and Speed Gait: A Randomized Controlled Trial. NeuroRehabilitation 2021, 48, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Flansbjer, U.; Miller, M.; Downham, D.; Lexell, J. Progressive Resistance Training after Stroke: Effects on Muscle Strength, Muscle Tone, Gait Performance and Perceived Participation. Acta Derm. Venereol. 2008, 40, 42–48. [Google Scholar] [CrossRef] [Green Version]
- Hill, T.R.; Gjellesvik, T.I.; Moen, P.M.R.; Tørhaug, T.; Fimland, M.S.; Helgerud, J.; Hoff, J. Maximal Strength Training Enhances Strength and Functional Performance in Chronic Stroke Survivors. Am. J. Phys. Med. Rehabil. 2012, 91, 393–400. [Google Scholar] [CrossRef]
- Park, C.; Son, H.; Yeo, B. The Effects of Lower Extremity Cross-Training on Gait and Balance in Stroke Patients: A Double-Blinded Randomized Controlled Trial. Eur. J. Phys. Rehabil. Med. 2021, 57, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Gladstone, D.J.; Danells, C.J.; Black, S.E. The Fugl-Meyer Assessment of Motor Recovery after Stroke: A Critical Review of Its Measurement Properties. Neurorehabil. Neural. Repair 2002, 16, 232–240. [Google Scholar] [CrossRef]
- Muscles: Testing and Function with Posture and Pain, 5th ed.; Kendall, F.P.; Kendall, F.P. (Eds.) Lippincott Williams & Wilkins: Baltimore, MD, USA, 2005; ISBN 978-0-7817-4780-6. [Google Scholar]
- Ghotbi, N.; Nakhostin Ansari, N.; Naghdi, S.; Hasson, S. Measurement of Lower-Limb Muscle Spasticity: Intrarater Reliability of Modified Modified Ashworth Scale. J. Rehabil. Res. Dev. 2011, 48, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Daly, J.J.; Nethery, J.; McCabe, J.P.; Brenner, I.; Rogers, J.; Gansen, J.; Butler, K.; Burdsall, R.; Roenigk, K.; Holcomb, J. Development and Testing of the Gait Assessment and Intervention Tool (G.A.I.T.): A Measure of Coordinated Gait Components. J. Neurosci. Methods 2009, 178, 334–339. [Google Scholar] [CrossRef] [Green Version]
- Gor-García-Fogeda, M.D.; Cano de la Cuerda, R.; Carratalá Tejada, M.; Alguacil-Diego, I.M.; Molina-Rueda, F. Observational Gait Assessments in People With Neurological Disorders: A Systematic Review. Arch. Phys. Med. Rehabil. 2016, 97, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Ferrarello, F.; Bianchi, V.A.M.; Baccini, M.; Rubbieri, G.; Mossello, E.; Cavallini, M.C.; Marchionni, N.; Di Bari, M. Tools for Observational Gait Analysis in Patients With Stroke: A Systematic Review. Phys. Ther. 2013, 93, 1673–1685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daly, J.J.; Roenigk, K.; Cheng, R.; Ruff, R.L. Abnormal Leg Muscle Latencies and Relationship to Dyscoordination and Walking Disability after Stroke. Rehabil. Res. Pract. 2011, 2011, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Fulk, G.D.; He, Y. Minimal Clinically Important Difference of the 6-Minute Walk Test in People With Stroke. J. Neurol. Phys. 2018, 42, 235–240. [Google Scholar] [CrossRef]
- Duncan, P.W.; Wallace, D.; Lai, S.M.; Johnson, D.; Embretson, S.; Laster, L.J. The Stroke Impact Scale Version 2.0: Evaluation of Reliability, Validity, and Sensitivity to Change. Stroke 1999, 30, 2131–2140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daly, J.J.; McCabe, J.P.; Gansen, J.; Rogers, J.; Butler, K.; Brenner, I.; Burdsall, R.; Nethery, J. Guest Editorial: Gait Coordination Protocol for Recovery of Coordinated Gait, Function, and Quality of Life Following Stroke. JRRD 2012, 49, xix. [Google Scholar] [CrossRef]
- Biernaskie, J.; Corbett, D. Enriched Rehabilitative Training Promotes Improved Forelimb Motor Function and Enhanced Dendritic Growth after Focal Ischemic Injury. J. Neurosci. 2001, 21, 5272–5280. [Google Scholar] [CrossRef] [PubMed]
- Jones, T.A.; Chu, C.J.; Grande, L.A.; Gregory, A.D. Motor Skills Training Enhances Lesion-Induced Structural Plasticity in the Motor Cortex of Adult Rats. J. Neurosci. 1999, 19, 10153–10163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nudo, R.J.; Wise, B.M.; SiFuentes, F.; Milliken, G.W. Neural Substrates for the Effects of Rehabilitative Training on Motor Recovery After Ischemic Infarct. Science 1996, 272, 1791–1794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nudo, R.; Milliken, G.; Jenkins, W.; Merzenich, M. Use-Dependent Alterations of Movement Representations in Primary Motor Cortex of Adult Squirrel Monkeys. J. Neurosci. 1996, 16, 785–807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butefisch, C.; Hummelsheim, H.; Denzler, P.; Mauritz, K.-H. Repetitive Training of Isolated Movements Improves the Outcome of Motor Rehabilitation of the Centrally Paretic Hand. J. Neurol. Sci. 1995, 130, 59–68. [Google Scholar] [CrossRef]
- Dean, C.M.; Shepherd, R.B. Task-Related Training Improves Performance of Seated Reaching Tasks After Stroke: A Randomized Controlled Trial. Stroke 1997, 28, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Waddell, K.J.; Birkenmeier, R.L.; Moore, J.L.; Hornby, T.G.; Lang, C.E. Feasibility of High-Repetition, Task-Specific Training for Individuals With Upper-Extremity Paresis. Am. J. Occup. Ther. 2014, 68, 444–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, R.N.; Lidor, R.; Cauraugh, J.H. To Be Aware or Not Aware? What to Think about While Learning and Performing a Motor Skill. Sport Psychol. 1993, 7, 19–30. [Google Scholar] [CrossRef]
- Pascual-Leone, A.; Torres, F. Plasticity of the Sensorimotor Cortex Representation of the Reading Finger in Braille Readers. Brain 1993, 116, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Elbert, T.; Pantev, C.; Wienbruch, C.; Rockstroh, B.; Taub, E. Increased Cortical Representation of the Fingers of the Left Hand in String Players. Science 1995, 270, 305–307. [Google Scholar] [CrossRef] [Green Version]
- Plautz, E.J.; Milliken, G.W.; Nudo, R.J. Effects of Repetitive Motor Training on Movement Representations in Adult Squirrel Monkeys: Role of Use versus Learning. Neurobiol. Learn. Mem. 2000, 74, 27–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winstein, C.J. Knowledge of Results and Motor Learning—Implications for Physical Therapy. Phys. Ther. 1991, 71, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Daly, J.J.; Ruff, R.L. Construction of Efficacious Gait and Upper Limb Functional Interventions Based on Brain Plasticity Evidence and Model-Based Measures For Stroke Patients. Sci. World J. 2007, 7, 2031–2045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daly, J.J.; Ruff, R.L. Electrically Induced Recovery of Gait Components for Older Patients with Chronic Stroke. Am. J. Phys. Med. Rehabil. 2000, 79, 349–360. [Google Scholar] [CrossRef]
- Daly, J.J.; Zimbelman, J.; Roenigk, K.L.; McCabe, J.P.; Rogers, J.M.; Butler, K.; Burdsall, R.; Holcomb, J.P.; Marsolais, E.B.; Ruff, R.L. Recovery of Coordinated Gait: Randomized Controlled Stroke Trial of Functional Electrical Stimulation (FES) Versus No FES, With Weight-Supported Treadmill and Over-Ground Training. Neurorehabil. Neural. Repair 2011, 25, 588–596. [Google Scholar] [CrossRef] [PubMed]
- Daly, J.J.; Roenigk, K.; Holcomb, J.; Rogers, J.M.; Butler, K.; Gansen, J.; McCabe, J.; Fredrickson, E.; Marsolais, E.B.; Ruff, R.L. A Randomized Controlled Trial of Functional Neuromuscular Stimulation in Chronic Stroke Subjects. Stroke 2006, 37, 172–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumann, D.A. Kinesiology of the Musculoskeletal System—E-Book: Foundations for Rehabilitation; Elsevier Health Sciences: Amsterdam, The Netherlands, 2013; ISBN 978-0-323-26632-1. [Google Scholar]
- Perry, J.; Garrett, M.; Gronley, J.K.; Mulroy, S.J. Classification of Walking Handicap in the Stroke Population. Stroke 1995, 26, 982–989. [Google Scholar] [CrossRef]
- Dorsch, S.; Ada, L.; Alloggia, D. Progressive Resistance Training Increases Strength after Stroke but This May Not Carry over to Activity: A Systematic Review. J. Physiother. 2018, 64, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Mudge, S.; Barber, P.A.; Stott, N.S. Circuit-Based Rehabilitation Improves Gait Endurance but Not Usual Walking Activity in Chronic Stroke: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2009, 90, 1989–1996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, J.-E.; Lee, W.-H.; Shin, J.-H.; Kim, H. Effects of Bi-Axial Ankle Strengthening on Muscle Co-Contraction during Gait in Chronic Stroke Patients: A Randomized Controlled Pilot Study. Gait Posture 2021, 87, 177–183. [Google Scholar] [CrossRef]
- Kwan, M.S.-M.; Hassett, L.M.; Ada, L.; Canning, C.G. Relationship between Lower Limb Coordination and Walking Speed after Stroke: An Observational Study. Braz. J. Phys. 2019, 23, 527–531. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, L.R.; de Menezes, K.K.P.; Scianni, A.A.; Faria-Fortini, I.; Teixeira-Salmela, L.F. Deficits in Motor Coordination of the Paretic Lower Limb Limit the Ability to Immediately Increase Walking Speed in Individuals with Chronic Stroke. Braz. J. Phys. 2020, 24, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Boissoneault, C.; Grimes, T.; Rose, D.K.; Waters, M.F.; Khanna, A.; Datta, S.; Daly, J.J. Innovative Long-Dose Neurorehabilitation for Balance and Mobility in Chronic Stroke: A Preliminary Case Series. Brain Sci. 2020, 10, 555. [Google Scholar] [CrossRef]
- Winter, D.A. Biomechanics and Motor Control. of Human Gait, 2nd ed.; University of Waterloo Press: Waterloo, ON, Canada, 1991; ISBN 978-0-88898-105-9. [Google Scholar]
- Faria-Fortini, I.; Basílio, M.L.; Scianni, A.A.; Faria, C.D.C.M.; Teixeira-Salmela, L.F. Performance and Capacity-Based Measures of Locomotion, Compared to Impairment-Based Measures, Best Predicted Participation in Individuals with Hemiparesis Due to Stroke. Disabil. Rehabil. 2018, 40, 1791–1798. [Google Scholar] [CrossRef] [PubMed]
- Faria-Fortini, I.; Polese, J.C.; Faria, C.D.C.M.; Teixeira-Salmela, L.F. Associations between Walking Speed and Participation, According to Walking Status in Individuals with Chronic Stroke. NeuroRehabilitation 2019, 45, 341–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Price, R.; Choy, N.L. Investigating the Relationship of the Functional Gait Assessment to Spatiotemporal Parameters of Gait and Quality of Life in Individuals With Stroke. J. Geriatr. Phys. Ther. 2019, 42, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Martino Cinnera, A.; Bonnì, S.; Pellicciari, M.C.; Giorgi, F.; Caltagirone, C.; Koch, G. Health-Related Quality of Life (HRQoL) after Stroke: Positive Relationship between Lower Extremity and Balance Recovery. Top. Stroke Rehabil. 2020, 27, 534–540. [Google Scholar] [CrossRef]
- Pundik, S.; Holcomb, J.; McCabe, J.; Daly, J.J. Enhanced Life-Role Participation in Response to Comprehensive Gait Training in Chronic-Stroke Survivors. Disabil. Rehabil. 2012, 34, 1535–1539. [Google Scholar] [CrossRef]
- Calvo-Lobo, C.; Useros-Olmo, A.I.; Almazán-Polo, J.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Palomo-López, P.; Rodríguez-Sanz, D.; López-López, D. Rehabilitative Ultrasound Imaging of the Bilateral Intrinsic Plantar Muscles and Fascia in Post-Stroke Survivors with Hemiparesis: A Case-Control Study. Int. J. Med. Sci. 2018, 15, 907–914. [Google Scholar] [CrossRef] [Green Version]
- Calvo-Lobo, C.; Useros-Olmo, A.; Almazán-Polo, J.; Martín-Sevilla, M.; Romero-Morales, C.; Sanz-Corbalán, I.; Rodríguez-Sanz, D.; López-López, D. Quantitative Ultrasound Imaging Pixel Analysis of the Intrinsic Plantar Muscle Tissue between Hemiparesis and Contralateral Feet in Post-Stroke Patients. Int. J. Environ. Res. Public Health 2018, 15, 2519. [Google Scholar] [CrossRef] [Green Version]
- Lang, C.E.; Lohse, K.R.; Birkenmeier, R.L. Dose and Timing in Neurorehabilitation: Prescribing Motor Therapy after Stroke. Curr. Opin. Neurol. 2015, 28, 549–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, Z.; Sui, M.; Zhuang, Z.; Liu, H.; Zheng, X.; Cai, C.; Jin, D. Effectiveness of Neuromuscular Electrical Stimulation on Lower Limbs of Patients With Hemiplegia After Chronic Stroke: A Systematic Review. Arch. Phys. Med. Rehabil. 2018, 99, 1011–1022.e1. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Lee, G. Effect of Afferent Electrical Stimulation with Mirror Therapy on Motor Function, Balance, and Gait in Chronic Stroke Survivors: A Randomized Controlled Trial. Eur. J. Phys. Rehabil. Med. 2019, 55, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.-R.; Mi, P.-L.; Huang, S.-F.; Chiu, S.-L.; Liu, Y.-C.; Wang, R.-Y. Effects of Neuromuscular Electrical Stimulation on Gait Performance in Chronic Stroke with Inadequate Ankle Control—A Randomized Controlled Trial. PLoS ONE 2018, 13, e0208609. [Google Scholar] [CrossRef] [Green Version]
- Allen, J.L.; Ting, L.H.; Kesar, T.M. Gait Rehabilitation Using Functional Electrical Stimulation Induces Changes in Ankle Muscle Coordination in Stroke Survivors: A Preliminary Study. Front. Neurol. 2018, 9, 1127. [Google Scholar] [CrossRef] [PubMed]
- Shendkar, C.V.; Lenka, P.K.; Biswas, A.; Kumar, R.; Mahadevappa, M. Therapeutic Effects of Functional Electrical Stimulation on Gait, Motor Recovery, and Motor Cortex in Stroke Survivors. Hong Kong Physiother. J. 2015, 33, 10–20. [Google Scholar] [CrossRef]
- Gil-Castillo, J.; Alnajjar, F.; Koutsou, A.; Torricelli, D.; Moreno, J.C. Advances in Neuroprosthetic Management of Foot Drop: A Review. J. Neuroeng. Rehabil. 2020, 17, 46. [Google Scholar] [CrossRef]
- Alnajjar, F.; Zaier, R.; Khalid, S.; Gochoo, M. Trends and Technologies in Rehabilitation of Foot Drop: A Systematic Review. Expert Rev. Med. Devices 2021, 18, 31–46. [Google Scholar] [CrossRef]
- Mehrholz, J.; Thomas, S.; Elsner, B. Treadmill Training and Body Weight Support for Walking after Stroke. Cochrane Database Syst. Rev. 2017, 8, CD002840. [Google Scholar] [CrossRef] [PubMed]




| G.A.I.T. ITEMS Showing a Gain | Pre | Post | Gain Score |
|---|---|---|---|
| Stance phase, item number | |||
| 6, trunk lat flx | 1 | 0 | 1 |
| 7, trunk wgt shift | 3 | 0 | 3 |
| 12, knee loading | 1 | 0 | 1 |
| 13, knee flx midstance | 2 | 1 | 1 |
| 15, ankle plntarflx | 1 | 0 | 1 |
| 17, ankle plntarflx, term pre-swing | 2 | 0 | 2 |
| Swing Phase, Item number | |||
| 23, knee initial swing | 1 | 0 | 1 |
| 26, ankle sagtl | 1 | 0 | 1 |
| 27, ankle inversion | 1 | 0 | 1 |
| Gain score for items that changed | 12 |
| A. Joint Movement and Gait Event | B. Pre-Treatment | C. Post-Treatment | D. Gain | E. Normal * |
|---|---|---|---|---|
| 1. Mid-Swing Hip Flexion | 9 | 34 | 25 | 35 |
| (±3) | (±2) | (±3) | ||
| 2. Knee Flexion at Toe-Off | 23 | 35 | 12 | 35 |
| (±3) | (±3) | (±5) | ||
| 3. Mid Swing Knee Flexion | 12 | 44 | 32 | 60 |
| (±3) | (±2) | (±4) | ||
| 4. Mid Swing Ankle Dorsiflexion | −7 | 6 | 13 | 4 |
| (±3) | (±2) | (±4) |
| Domain | Pre-Treatment | Post-Treatment | Change Score |
|---|---|---|---|
| 1. Physical/mental problems due to stroke (x/20) | 15 | 17 | 2 |
| 2. Memory and thinking (x/40) | 40 | 40 | 0 |
| 3. Mood/emotions post stroke (x/45) | 40 | 39 | −1 |
| 4. Communication and understg. (x/35) | 35 | 35 | 0 |
| 5. Daily activities (x/60) | 55 | 59 | 4 |
| 6. Mobility (x/50) | 46 | 49 | 3 |
| 7. Hand function (x/25) | 20 | 23 | 3 |
| 8. Meaningful activities (x/45) | 42 | 43 | 1 |
| Total | 293 | 305 | 12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McCabe, J.P.; Roenigk, K.; Daly, J.J. Necessity and Content of Swing Phase Gait Coordination Training Post Stroke; A Case Report. Brain Sci. 2021, 11, 1498. https://doi.org/10.3390/brainsci11111498
McCabe JP, Roenigk K, Daly JJ. Necessity and Content of Swing Phase Gait Coordination Training Post Stroke; A Case Report. Brain Sciences. 2021; 11(11):1498. https://doi.org/10.3390/brainsci11111498
Chicago/Turabian StyleMcCabe, Jessica P., Kristen Roenigk, and Janis J. Daly. 2021. "Necessity and Content of Swing Phase Gait Coordination Training Post Stroke; A Case Report" Brain Sciences 11, no. 11: 1498. https://doi.org/10.3390/brainsci11111498