
Effect of 6-Week Balance Exercise by Real-Time Postural Feedback System on Walking Ability for Patients with Chronic Stroke: A Pilot Single-Blind Randomized Controlled Trial

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
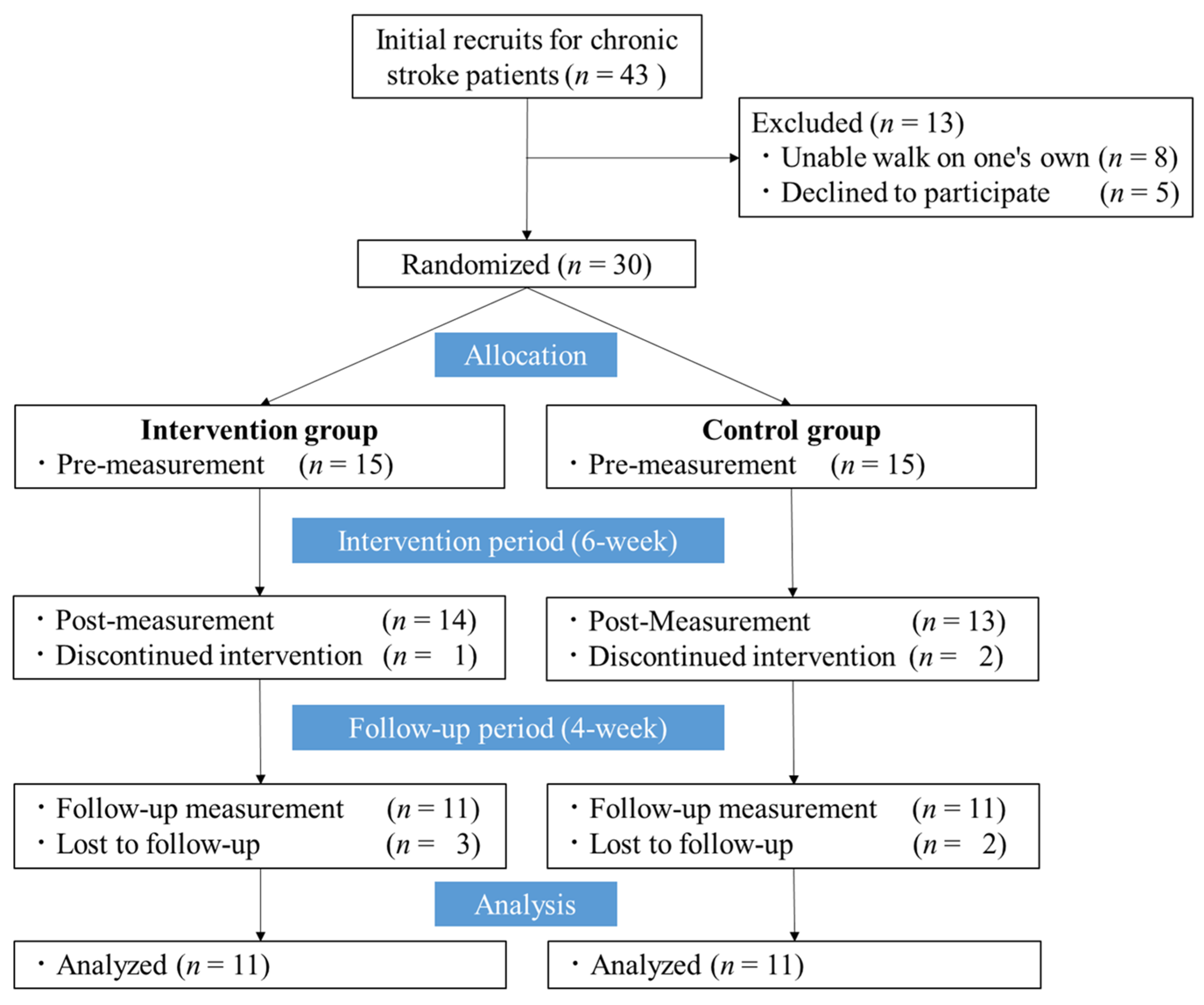
2.1. Study Design and Setting
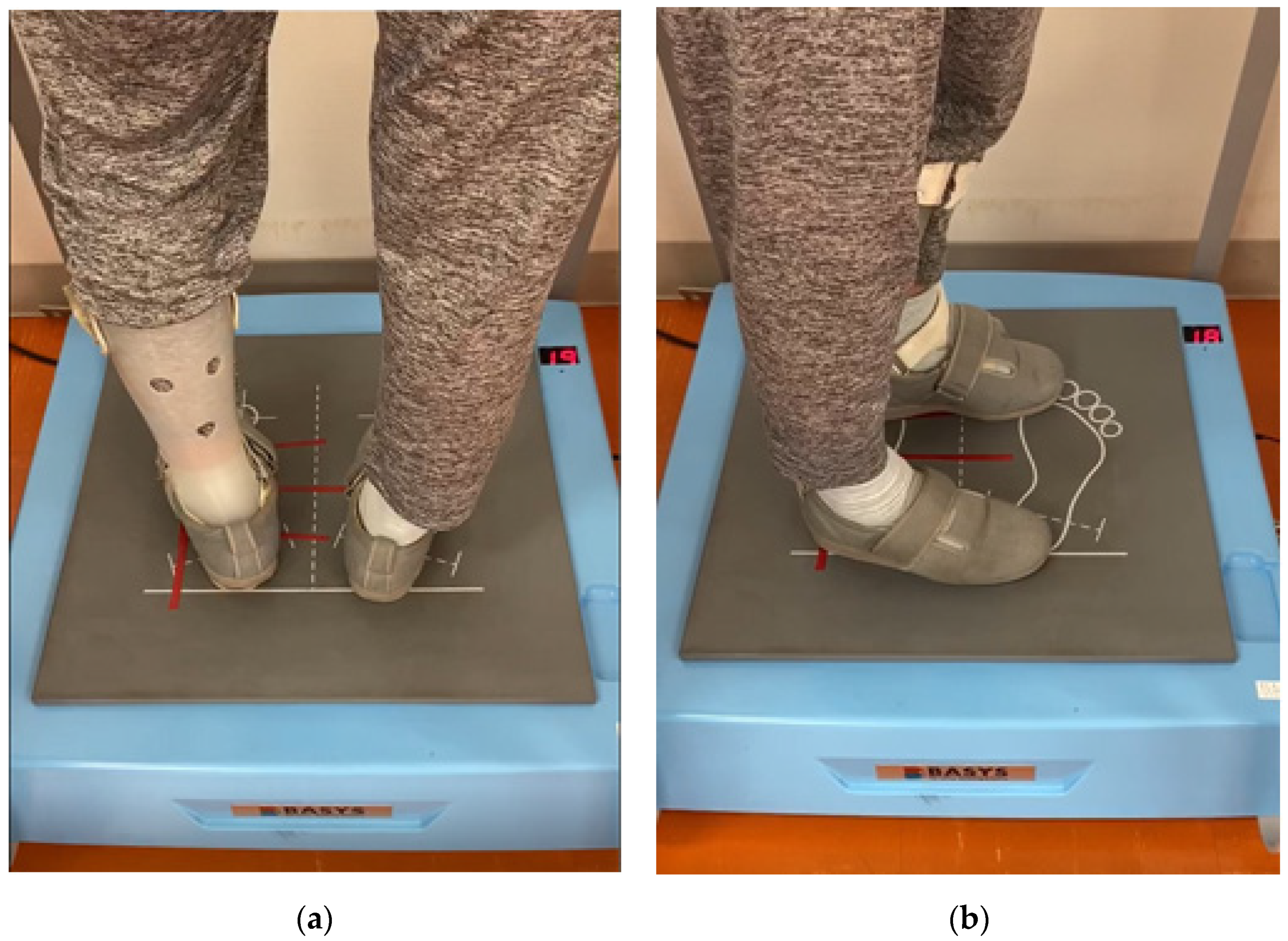
2.2. Intervention
2.3. Outcome Measures
2.3.1. Demographic and Baseline Data
2.3.2. Muscle Strength of Knee Extension
2.3.3. Physical Performance
2.3.4. Self-Reported Questionnaires for Fall and Gait Efficacy
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2015 Neurological Disorders Collaborator Group. Global, regional, and national burden of neurological disorders during 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Neurol. 2017, 16, 877–897. [Google Scholar] [CrossRef] [Green Version]
- Feigin, V.L.; Norrving, B.; Mensah, G.A. Global burden of stroke. Circ. Res. 2017, 120, 439–448. [Google Scholar] [CrossRef]
- Pollock, A.; Baer, G.; Campbell, P.; Choo, P.L.; Forster, A.; Morris, J.; Pomeroy, V.M.; Langhorne, P. Physical rehabilitation approaches for the recovery of function and mobility following stroke. Cochrane Database Syst. Rev. 2014, CD001920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent-Onabajo, G.; Musa, H.Y.; Joseph, E. Prevalence of balance impairment among stroke survivors undergoing neurorehabilitation in Nigeria. J. Stroke Cerebrovasc. Dis. 2018, 27, 3487–3492. [Google Scholar] [CrossRef]
- Sarah, F.T.; Marie, H.; Jay, C.; Andrea, S.; Raymond, C.T. Balance disability after stroke. Phys. Ther. 2006, 86, 30–38. [Google Scholar]
- Khan, F.; Chevidikunnan, M.F. Prevalence of balance impairment and factors associated with balance among patients with stroke. A cross sectional retrospective case control study. Healthcare 2021, 9, 320. [Google Scholar] [CrossRef]
- Michael, K.; Goldberg, A.P.; Treuth, M.S.; Beans, J.; Normandt, P.; Macko, R.F. Progressive adaptive physical activity in stroke improves balance, gait, and fitness: Preliminary results. Top. Stroke Rehabil. 2009, 16, 133–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onigbinde, A.T.; Awotidebe, T.; Awosika, H. Effect of 6 weeks wobble board exercises on static and dynamic balance of stroke survivors. Technol. Health Care 2009, 17, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Llorens, R.; Gil-Gomez, J.-A.; Alcaniz, M.; Colomer, C.; Noe, E. Improvement in balance using a virtual reality-based stepping exercise: A randomized controlled trial involving individuals with chronic stroke. Clin. Rehabil. 2015, 29, 261–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghayour, N.M.; Shariat, A.; Dommerholt, J.; Hakakzadeh, A.; Nakhostin-Ansari, A.; Selk-Ghaffari, M.; Ingle, L.; Cleland, J.A. Aquatic therapy for improving lower limbs function in post-stroke survivors: A systematic review with meta-analysis. Top. Stroke Rehabil. 2021, 19, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, C.B.; Medeiros, R.T.; Frota, N.A.F.; Greters, M.E.; Conforto, A.B. Balance control in hemiparetic stroke patients: Main tools for evaluation. J. Rehabil. Res. Dev. 2008, 45, 1215–1226. [Google Scholar] [CrossRef] [PubMed]
- Peterka, J.R. Sensorimotor integration in human postural control. J. Neurophysiol. 2002, 88, 1097–1118. [Google Scholar] [CrossRef] [Green Version]
- Karasu, A.U.; Batur, E.B.; Karataş, G.K. Effectiveness of Wii-based rehabilitation in stroke: A randomized controlled study. J. Rehabil. Med. 2018, 50, 406–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zijlstra, A.; Mancini, M.; Chiari, L.; Zijlstra, W. Biofeedback for training balance and mobility tasks in older populations: A systematic review. J. Neuroeng. Rehabil. 2010, 7, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ju, S.K.; Yoo, W.G. The effect of somatosensory and cognitive-motor tasks on the paretic leg of chronic stroke patients in the standing posture. J. Phys. Ther. Sci. 2014, 26, 1869–1870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K. Balance training with electromyogram-triggered functional electrical stimulation in the rehabilitation of stroke patients. Brain Sci. 2020, 10, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawashima, N. Implicit adjustment of the postural control strategy accomplished by real-time feedback-driven movable platform. J. Med. Biol. Eng. 2016, 54, 2T5–4. (In Japanese) [Google Scholar]
- Nakashima, Y.; Hirofumi, G. Effect of a balance adjustment system on gait disturbance in patients with neurodegenerative disease. Neurotherapeutics 2020, 37, 47–50. (In Japanese) [Google Scholar]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomized trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [Green Version]
- Arnold, C.M.; Warkentin, K.D.; Chilibeck, P.D.; Magnus, C.R. The reliability and validity of handheld dynamometry for the measurement of lower-extremity muscle strength in older adults. J. Strength Cond. Res. 2010, 24, 815–824. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [PubMed]
- Tilson, J.K.; Sullivan, K.J.; Cen, S.Y.; Rose, D.K.; Koradia, C.H.; Azen, S.P.; Duncan, P.W.; for the Locomotor Experience Applied Post Stroke (LEAPS) Investigative Team. Meaningful gait speed improvement during the first 60 days post stroke minimal clinically important difference. Phys. Ther. 2010, 90, 196–208. [Google Scholar] [CrossRef]
- Bischoff, H.A.; Stähelin, H.B.; Monsch, A.U.; Iversen, M.D.; Weyh, A.; von Dechend, M.; Akos, R.; Conzelmann, M.; Dick, W.; Theiler, R. Identifying a cut-off point for normal mobility: A comparison of the timed ‘up and go’ test in community-dwelling and institutionalised elderly women. Age Ageing 2003, 32, 315–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newell, A.M.; VanSwearingen, J.M.; Hile, E.; Brach, J.S. The modified gait efficacy scale: Establishing the psychometric properties in older adults. Phys. Ther. 2012, 92, 318–328. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Richman, D.; Powell, L. Falls efficacy as a measure of fear of falling. J. Gerontol. 1990, 45, P239–P243. [Google Scholar] [CrossRef] [PubMed]
- Winstein, C.J.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.R.; Cramer, S.C.; Deruyter, F.; Eng, J.J.; Fisher, B.; Harvey, R.L.; et al. Guidelines for Adult Stroke Rehabilitation and Recovery. A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2016, 47, e98–e169. [Google Scholar] [CrossRef] [PubMed]
- Shima, J.; Nahid, T.; Alireza, A.B.; Maryam, Z. Stroke patients showed improvements in balance in response to visual restriction exercise. Phys. Ther. 2021, E10081. [Google Scholar] [CrossRef]
- Horak, F.B. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age Ageing 2006, 35, 7–11. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y.; Park, J.; Lee, D.; Roh, H. The effects of exercising on unstable surfaces on the balance ability of stroke patients. J. Phys. Ther. Sci. 2011, 23, 789–792. [Google Scholar] [CrossRef] [Green Version]
- Dickstein, R.; Ocherman, S.; Dannenbaum, E.; Shina, N.; Pillar, T. Stance stability and EMG changes in the ankle musculature of hemiparetic patients trained on a moveable platform. Neurorehabil. Neural Repair 1991, 5, 201–209. [Google Scholar] [CrossRef] [Green Version]
- Flansbjer, U.B.; Holmbäck, A.M.; Downham, D.; Patten, C.; Lexell, J. Reliability of gait performance tests in men and women with hemiparesis after stroke. J. Rehabil. Med. 2005, 37, 75–82. [Google Scholar] [PubMed] [Green Version]
- Perez, M.A.; Lungholt, B.K.; Nyborg, K.; Nielsen, J.B. Motor skill training induces changes in the excitability of the leg cortical area in healthy humans. Exp. Brain Res. 2004, 159, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Di Fabio, R.P.; Badke, M.B.; Duncan, P. Adapting human postural reflexes following localized cerebrovascular lesion: Analysis of bilateral long latency responses. Brain Res. 1986, 363, 257–264. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Total (n = 22) | Intervention Group (n = 11) | Control Group (n = 11) | p-Value |
|---|---|---|---|---|
| Age (years) | 75.0 ± 11.5 | 73.6 ± 12.5 | 76.4 ± 10.9 | 0.591 |
| Height (cm) | 158.6 ± 9.9 | 158.6 ± 10.7 | 158.7 ± 9.4 | 0.983 |
| Weight (kg) | 61.4 ± 8.9 | 60.6 ± 8.8 | 62.2 ± 9.4 | 0.687 |
| BMI (kg/m2) | 24.5 ± 3.5 | 24.2 ± 3.2 | 24.8 ± 3.9 | 0.677 |
| Sex: Female (n, %) | 7 (31.8) | 3 (27.2) | 4 (36.4) | 0.901 |
| Use of walking equipment (n, %) | 16 (72.7) | 9 (81.8) | 7 (63.6) | 0.580 |
| Use of ankle foot orthosis (n, %) | 4 (18.2) | 3 (27.3) | 1 (9.1) | 0.228 |
| Duration after stroke (months) | 43.0 (24.0–85.5) | 42.0 (26.0–138.0) | 66.0 (20.0–72.0) | 0.656 |
| HDS-R (points) | 24.1 ± 5.4 | 24.9 ± 6.3 | 23.4 ± 4.7 | 0.520 |
| Brunnstrom Recovery Stage (Lower Limb) | III:3, IV:3, V:6, VI:10 | III:1, IV:2, V:4, VI:4 | III:2, IV:1, V:2, VI:6 | 0.630 |
| Variables | Intervention Group (n = 11) | Control Group (n = 11) | Main Effect | Interaction Effect | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Time | Group | Time * Group | |||||||||
| Mean ± SD | Mean ± SD | F | p Value | F | p Value | F | p Value | η2 | Effect Size | Observed Power | |
| Muscle strength of knee extension (Nm/kg) NPA | 0.525 | 0.547 | 0.015 | 0.905 | 0.153 | 0.800 | 0.008 | 0.090 | 0.132 | ||
| Pre | 1.52 ± 0.41 | 1.47 ± 0.35 | |||||||||
| Post | 1.54 ± 0.26 | 1.56 ± 0.46 | |||||||||
| Follow-up | 1.55 ± 0.18 | 1.52 ± 0.44 | |||||||||
| Muscle strength of knee extension (Nm/kg) PA | 0.147 | 0.862 | 0.011 | 0.919 | 0.351 | 0.705 | 0.017 | 0.132 | 0.237 | ||
| Pre | 1.24 ± 0.52 | 1.25 ± 0.50 | |||||||||
| Post | 1.25 ± 0.53 | 1.20 ± 0.51 | |||||||||
| Follow-up | 1.24 ± 0.48 | 1.22 ± 0.45 | |||||||||
| SPPB score (points) | 1.625 | 0.215 | 0.876 | 0.360 | 0.768 | 0.443 | 0.037 | 0.196 | 0.478 | ||
| Pre | 8.00 ± 3.46 | 9.45 ± 2.46 | |||||||||
| Post | 8.36 ± 3.47 | 9.18 ± 1.94 | |||||||||
| Follow-up | 8.73 ± 2.94 | 9.64 ± 1.80 | |||||||||
| TUG (s) | 5.004 | 0.015 ♀ | 1.944 | 0.178 | 6.078 | 0.007 ♀ | 0.233 | 0.551 | 0.999 | ||
| Pre | 16.95 ± 8.28 | 11.97 ± 4.66 | |||||||||
| Post | 15.01 ± 6.54 | 12.31 ± 4.80 | |||||||||
| Follow-up | 14.71 ± 6.29 | 11.93 ± 4.10 | |||||||||
| COP length (cm/s) | 0.263 | 0.770 | 0.682 | 0.419 | 0.068 | 0.934 | 0.003 | 0.054 | 0.079 | ||
| Pre | 2.33 ± 1.99 | 1.78 ± 0.96 | |||||||||
| Post | 2.24 ± 1.95 | 1.77 ± 0.81 | |||||||||
| Follow-up | 2.23 ± 1.75 | 1.71 ± 0.83 | |||||||||
| mGES (points) | 0.457 | 0.615 | 2.038 | 0.169 | 3.759 | 0.038 ♀ | 0.158 | 0.433 | 0.994 | ||
| Pre | 46.27 ± 19.74 | 63.36 ± 19.56 | |||||||||
| Post | 52.64 ± 14.19 | 63.36 ± 17.02 | |||||||||
| Follow-up | 56.82 ± 17.68 | 55.91 ± 14.65 | |||||||||
| FES (points) | 2.387 | 0.106 | 0.707 | 0.410 | 0.248 | 0.777 | 0.012 | 0.110 | 0.177 | ||
| Pre | 296.36 ± 50.45 | 317.27 ± 60.18 | |||||||||
| Post | 306.36 ± 62.17 | 327.27 ± 46.71 | |||||||||
| Follow-up | 290.00 ± 53.67 | 298.18 ± 51.54 | |||||||||
| Variables | Intervention Group (n = 11) | Control Group (n = 11) | ||||||
|---|---|---|---|---|---|---|---|---|
| Difference [95% CI] | p Value | Effect Size | Observed Power | Difference [95% CI] | p Value | Effect Size | Observed Power | |
| TUG test (s) | ||||||||
| Post–Pre | −1.95 ± 0.660 (−3.42, −0.473) | 0.015 a | −0.888 | 0.977 | 0.34 ± 0.26 (−0.25, −0.92) | 0.227 | 0.388 | 0.411 |
| Follow-up–Pre | −2.24 ± 0.77 (−3.97, −0.52) | 0.016 b | −0.875 | 0.974 | −0.04 ± 0.39 (−0.92, 0.83) | 0.912 | −0.034 | 0.052 |
| Follow-up–Post | −0.30 ± 0.52 (−1.45, 0.86) | 0.855 | −0.173 | 0.121 | −0.38 ± 0.36 (−1.19, 0.42) | 0.313 | −0.320 | 0.299 |
| mGES (points) | ||||||||
| Post–Pre | 6.36 ± 6.25 (−7.57, 20.30) | 0.330 | 0.307 | 0.279 | 0.00 ± 3.85 (−8.57, 8.57) | 1.000 | −0.591 | 0.752 |
| Follow-up–Pre | 10.55 ± 4.36 (0.84, 20.26) | 0.036 b | 0.730 | 0.903 | −7.46 ± 3.16 (−14.48, −0.43) | 0.040 b | −1.365 | 0.999 |
| Follow-up–Post | 4.18 ± 6.35 (−9.96, 18.32) | 0.525 | 0.199 | 0.144 | −7.46 ± 3.14 (−14.45, −0.46) | 0.039 c | −1.369 | 0.999 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Komiya, M.; Maeda, N.; Narahara, T.; Suzuki, Y.; Fukui, K.; Tsutsumi, S.; Yoshimi, M.; Ishibashi, N.; Shirakawa, T.; Urabe, Y. Effect of 6-Week Balance Exercise by Real-Time Postural Feedback System on Walking Ability for Patients with Chronic Stroke: A Pilot Single-Blind Randomized Controlled Trial. Brain Sci. 2021, 11, 1493. https://doi.org/10.3390/brainsci11111493
Komiya M, Maeda N, Narahara T, Suzuki Y, Fukui K, Tsutsumi S, Yoshimi M, Ishibashi N, Shirakawa T, Urabe Y. Effect of 6-Week Balance Exercise by Real-Time Postural Feedback System on Walking Ability for Patients with Chronic Stroke: A Pilot Single-Blind Randomized Controlled Trial. Brain Sciences. 2021; 11(11):1493. https://doi.org/10.3390/brainsci11111493
Chicago/Turabian StyleKomiya, Makoto, Noriaki Maeda, Taku Narahara, Yuta Suzuki, Kazuki Fukui, Shogo Tsutsumi, Mistuhiro Yoshimi, Naoki Ishibashi, Taizan Shirakawa, and Yukio Urabe. 2021. "Effect of 6-Week Balance Exercise by Real-Time Postural Feedback System on Walking Ability for Patients with Chronic Stroke: A Pilot Single-Blind Randomized Controlled Trial" Brain Sciences 11, no. 11: 1493. https://doi.org/10.3390/brainsci11111493