
Histopathological Investigation of Dura-like Membrane in Vestibular Schwannomas


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Study Population
2.3. Immunohistochemical Analysis
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
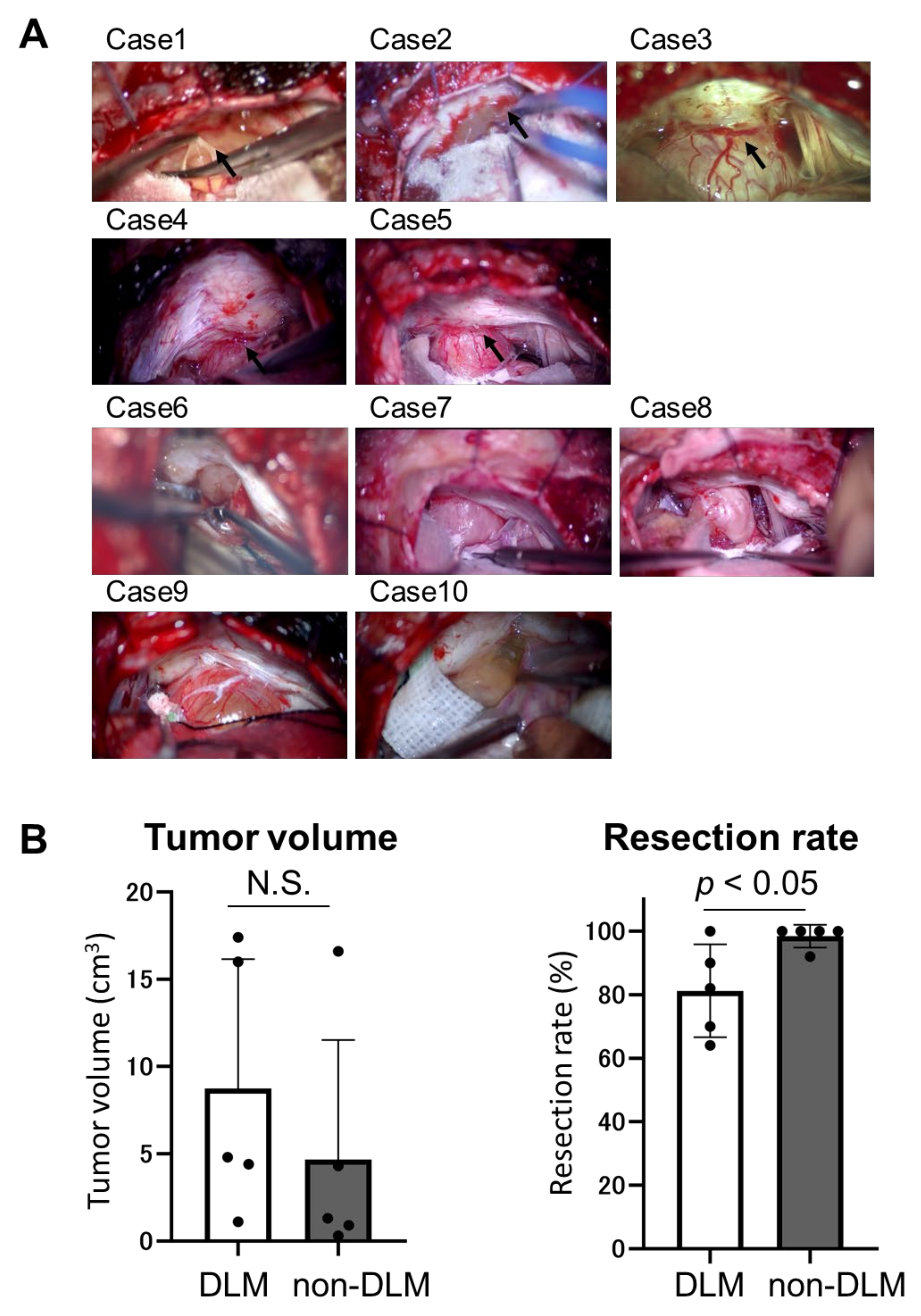
3.2. Intraoperative Findings and Surgical Outcome
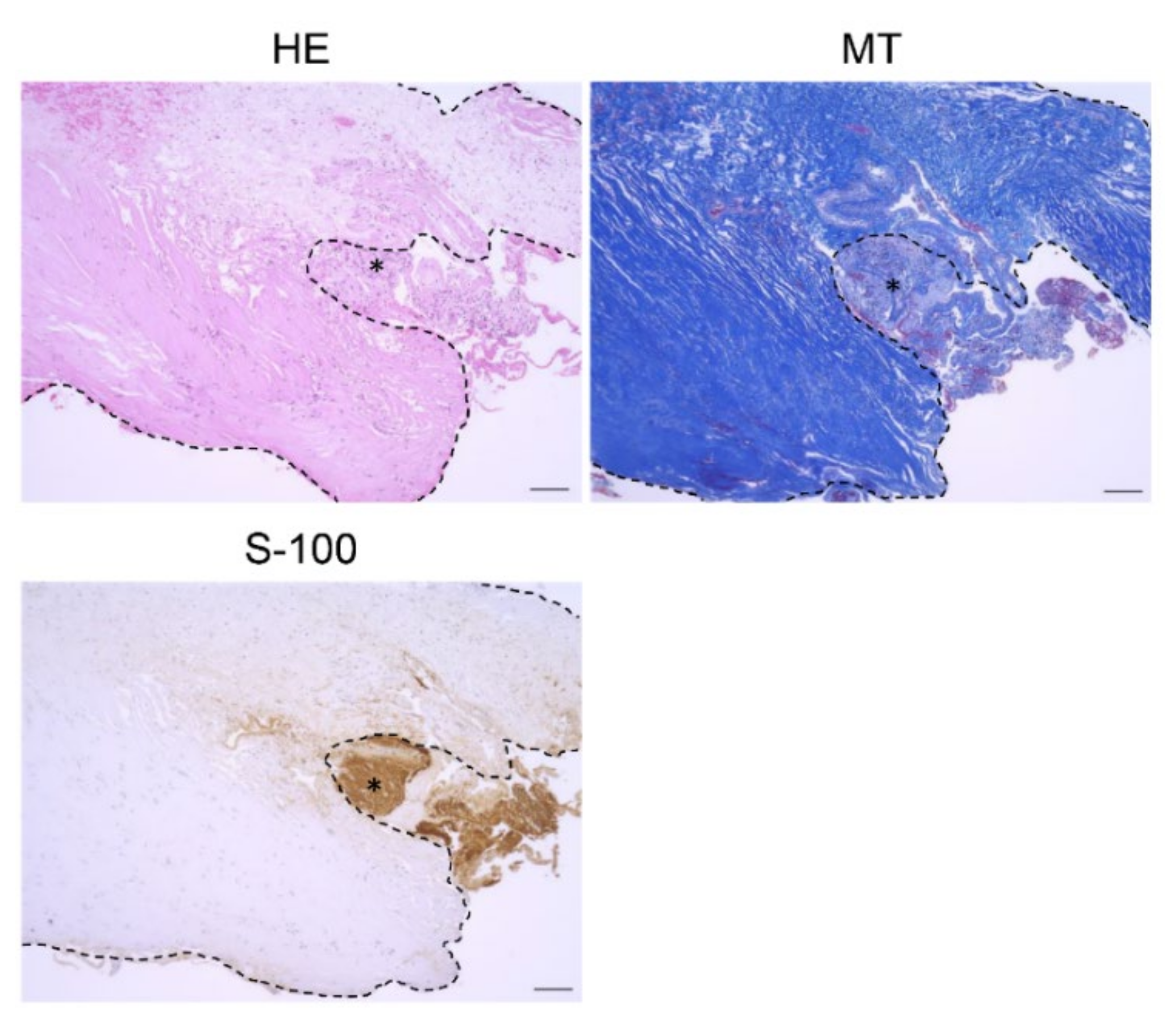
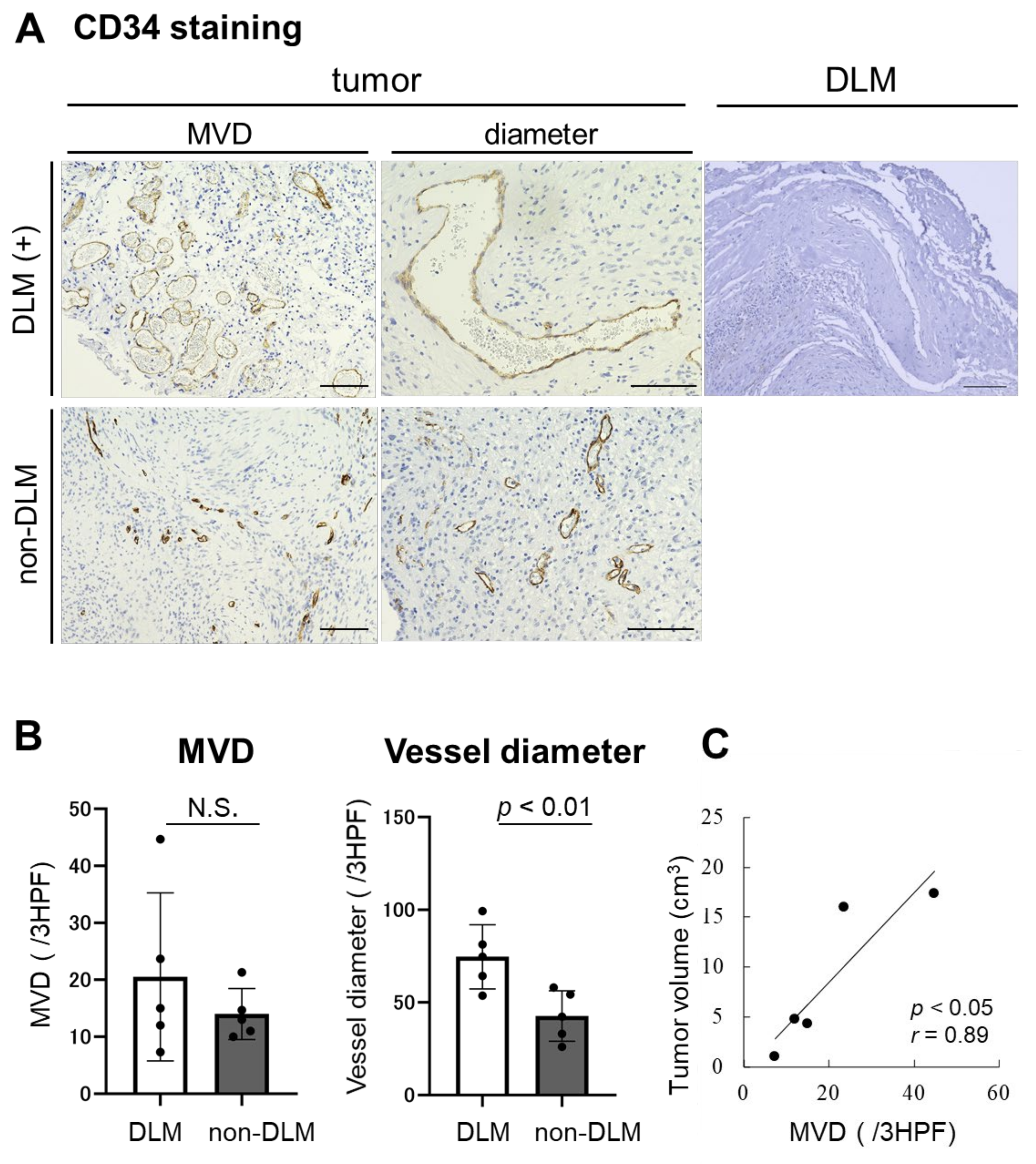
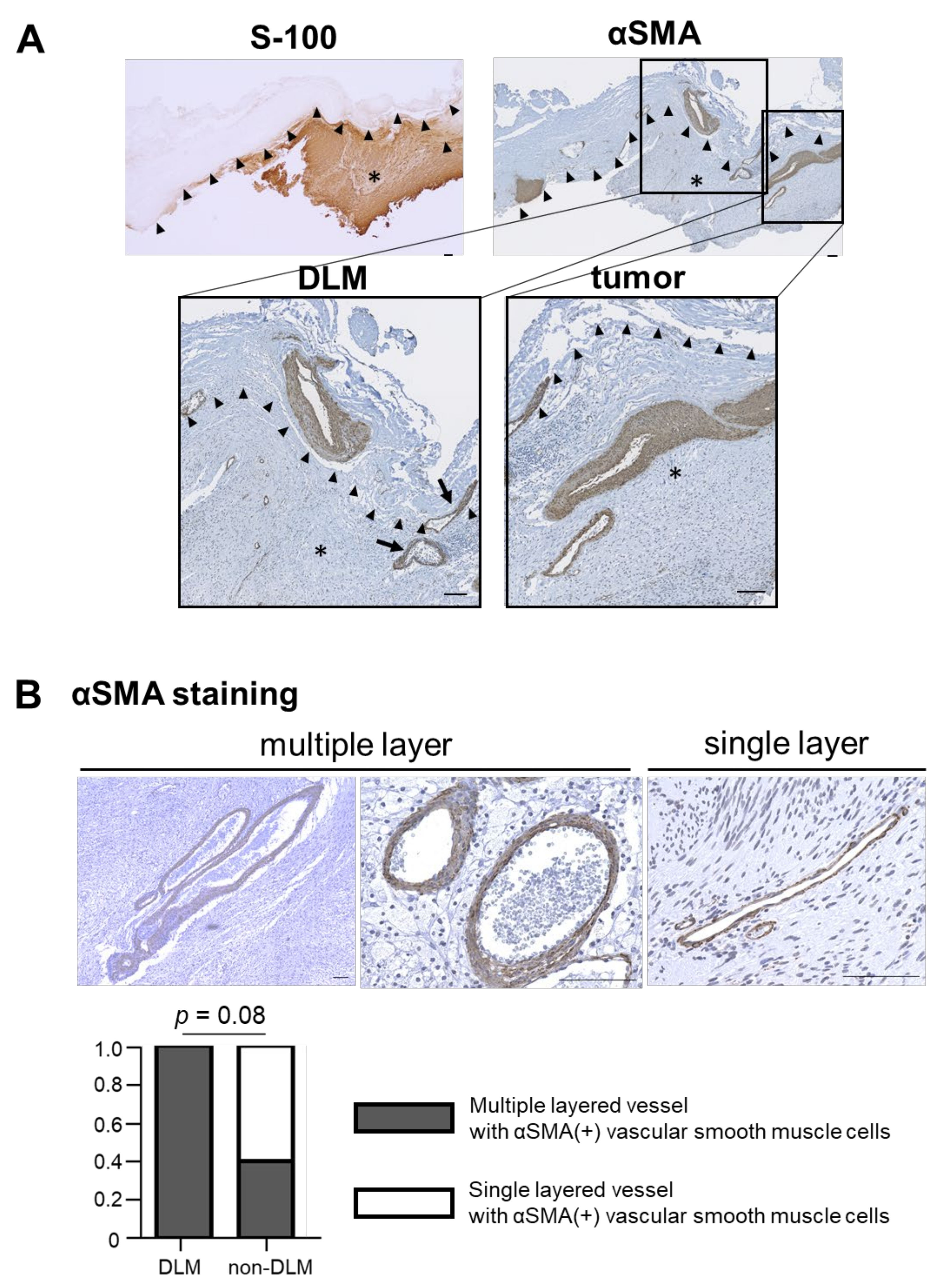
3.3. Histological Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rachinger, J.; Rampp, S.; Prell, J.; Scheller, C.; Alfieri, A.; Strauss, C. Tumor origin and hearing preservation in vestibular schwannoma surgery. J Neurosurg. 2011, 115, 900–905. [Google Scholar] [CrossRef] [PubMed]
- Troude, L.; Boucekine, M.; Montava, M.; Lavieille, J.-P.; Régis, J.-M.; Roche, P.-H. Predictive Factors of Early Postoperative and Long-Term Facial Nerve Function After Large Vestibular Schwannoma Surgery. World Neurosurg. 2019, 127, e599–e608. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, T.; Shono, T.; Hashiguchi, K.; Yoshida, F.; Suzuki, S.O. Histological considerations of the cleavage plane for preservation of facial and cochlear nerve functions in vestibular schwannoma surgery. J Neurosurg. 2009, 110, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Tomio, R.; Yoshida, K.; Kohno, M.; Kamamoto, D.; Mikami, S. The outermost "dura-like membrane" of vestibular schwannoma. Surg. Neurol. Int. 2016, 7, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sitohy, B.; Nagy, J.A.; Dvorak, H.F. Anti-VEGF/VEGFR Therapy for Cancer: Reassessing the Target: Figure 1. Cancer Res. 2012, 72, 1909–1914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagy, J.A.; Dvorak, H.F. Heterogeneity of the tumor vasculature: The need for new tumor blood vessel type-specific targets. Clin. Exp. Metastasis 2012, 29, 657–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stegmann, T.J. FGF-1: A human growth factor in the induction of neoangiogenesis. Expert Opin. Investig. Drugs 1998, 7, 2011–2015. [Google Scholar] [CrossRef] [PubMed]
- Tamura, R.; Fujioka, M.; Morimoto, Y.; Ohara, K.; Kosugi, K.; Oishi, Y.; Sato, M.; Ueda, R.; Fujiwara, H.; Hikichi, T.; et al. A VEGF receptor vaccine demonstrates preliminary efficacy in neurofibromatosis type 2. Nat. Commun. 2019, 10, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamura, R.; Tanaka, T.; Ohara, K.; Miyake, K.; Morimoto, Y.; Yamamoto, Y.; Kanai, R.; Akasaki, Y.; Murayama, Y.; Tamiya, T.; et al. Persistent restoration to the immunosupportive tumor microenvironment in glioblastoma by bevacizumab. Cancer Sci. 2019, 110, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Morera, P.; Castaño-González, I.; Travieso-González, C.; Mompeó-Corredera, B.; Ortega-Santana, F. Quantification and statistical analysis methods for vessel wall components from stained images with Masson’s trichrome. PLoS ONE 2016, 11, e0146954. [Google Scholar] [CrossRef] [PubMed]
- Stone, J.J.; Boland, J.M.; Spinner, R.J. Analysis of Peripheral Nerve Schwannoma Pseudocapsule. World Neurosurg. 2018, 119, e986–e990. [Google Scholar] [CrossRef] [PubMed]
- Cleaver, O.; A Melton, D. Endothelial signaling during development. Nat. Med. 2003, 9, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Carmeliet, P. Mechanisms of angiogenesis and arteriogenesis. Nat. Med. 2000, 6, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Kimura, Y.; Morohashi, S.; Yoshizawa, T.; Suzuki, T.; Morohashi, H.; Sakamoto, Y.; Koyama, M.; Murata, A.; Kijima, H.; Hakamada, K. Clinicopathological significance of vascular endothelial growth factor, thymidine phosphorylase and microvessel density in colorectal cancer. Mol. Med. Rep. 2016, 13, 1551–1557. [Google Scholar] [CrossRef] [PubMed]
- Prior, B.M.; Yang, H.T.; Terjung, R.L. What makes vessels grow with exercise training? J Appl Physiol. 2004, 97, 1119–1128. [Google Scholar] [CrossRef] [PubMed]
- Koutsimpelas, D.; Stripf, T.; Heinrich, U.R.; Mann, W.J.; Brieger, J. Expression of Vascular Endothelial Growth Factor and Basic Fibroblast Growth Factor in Sporadic Vestibular Schwannomas Correlates to Growth Characteristics. Otol. Neurotol. 2007, 28, 1094–1099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- A Nagy, J.; Chang, S.-H.; Dvorak, A.M.; Dvorak, H.F. Why are tumour blood vessels abnormal and why is it important to know? Br. J. Cancer 2009, 100, 865–869. [Google Scholar] [CrossRef] [PubMed]
- Mishra, P.J.; Mishra, P.J.; Glod, J.W.; Banerjee, D. Mesenchymal stem cells: Flip side of the coin. In Cancer Res.; 2009; Volume 69, pp. 1255–1258. [Google Scholar] [CrossRef] [Green Version]
- Walocha, J.A.; Litwin, J.A.; Miodoński, A.J. Vascular system of intramural leiomyomata revealed by corrosion casting and scanning electron microscopy. Hum. Reprod. 2003, 18, 1088–1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age | Sex | DLM | Preoperative Symptom | Postoperative Symptom | Tumor Volume (cm3) | Resection Rate (%) | Rec |
|---|---|---|---|---|---|---|---|---|
| 1 | 35 | M | + | hearing disorder (G-R Gr.3) facial pain | facial n. palsy (H-B Gr.4, permanent) | 16 | 100 | - |
| 2 | 45 | M | + | hearing disorder (G-R Gr.2) gait disturbance hydrocephalus | no change | 17.4 | 70 | - |
| 3 | 21 | F | + | hearing disorder (deaf) | no change | 4.8 | 90 | - |
| 4 | 61 | F | + | hearing disorder (G-R Gr.2) | no change | 4.4 | 82 | - |
| 5 | 67 | F | + | hearing disorder (G-R Gr.3) | hearing disorder (deaf) | 1.1 | 64 | - |
| 6 | 66 | M | - | hearing disorder (G-R Gr.3) | facial n. palsy (H-B Gr.3, temporary) | 0.3 | 100 | - |
| 7 | 54 | M | - | hearing disorder (G-R Gr.3) | no change | 1.3 | 92 | - |
| 8 | 35 | F | - | hearing disorder (G-R Gr.3) | no change | 0.9 | 100 | - |
| 9 | 50 | M | - | hearing disorder (G-R Gr.2) facial numbness | hearing disorder (deaf) facial n. palsy (H-B Gr.4, temporary) | 4.3 | 100 | - |
| 10 | 60 | F | - | hearing disorder (G-R Gr.4) facial n. palsy (H-B Gr.2) facial numbness | no change | 16.6 | 100 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oishi, Y.; Tamura, R.; Yoshida, K.; Toda, M. Histopathological Investigation of Dura-like Membrane in Vestibular Schwannomas. Brain Sci. 2021, 11, 1649. https://doi.org/10.3390/brainsci11121649
Oishi Y, Tamura R, Yoshida K, Toda M. Histopathological Investigation of Dura-like Membrane in Vestibular Schwannomas. Brain Sciences. 2021; 11(12):1649. https://doi.org/10.3390/brainsci11121649
Chicago/Turabian StyleOishi, Yumiko, Ryota Tamura, Kazunari Yoshida, and Masahiro Toda. 2021. "Histopathological Investigation of Dura-like Membrane in Vestibular Schwannomas" Brain Sciences 11, no. 12: 1649. https://doi.org/10.3390/brainsci11121649