
Applicability of Clinical Decision Support in Management among Patients Undergoing Cardiac Surgery in Intensive Care Unit: A Systematic Review


 ,
, 
Abstract
:1. Introduction
1.1. Background of Decision Support Systems
1.2. Objectives
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
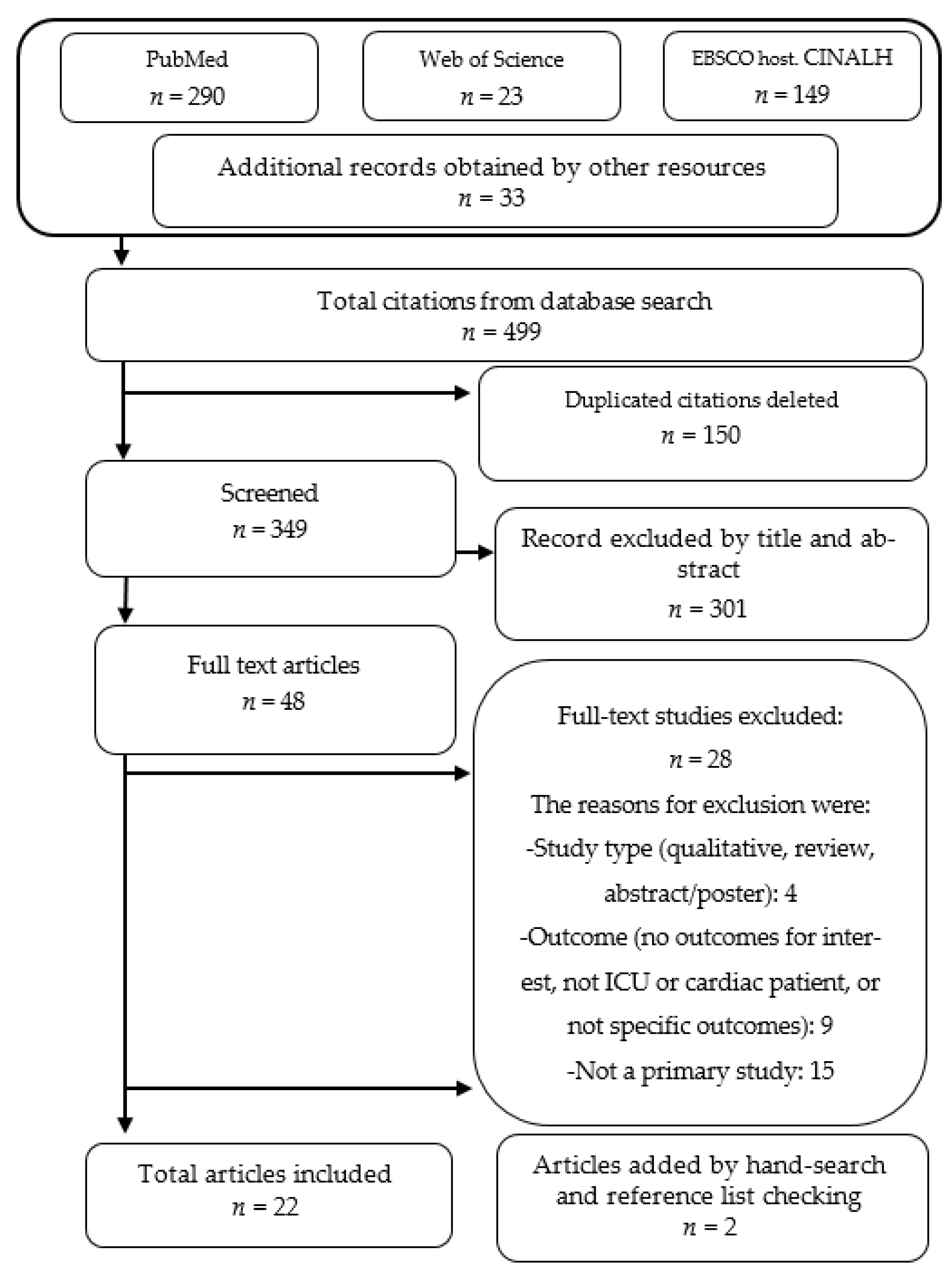
2.3. Study Selection
2.4. Data Extraction and Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Characteristics
3.2. Thematic Categories
3.2.1. Development Forecast
3.2.2. Medication Errors
3.2.3. Warning Systems: Early Detection and Early Action
3.2.4. Standardization and Compliance with Protocols
3.2.5. Precise Adjustment to Objectives
3.2.6. Cost Reduction
3.2.7. Acceptance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Terms
| Keywords | Mesh Terms |
| Intensive Care Units | Intensive Care Units (Coronary Care Units; Intensive Care Units, Pediatric; Intensive Care Units, Neonatal) |
| Critical Care | Critical Care (Early Goal-Directed Therapy; Intensive Care) |
| Artificial Intelligence | Artificial intelligence (Computer Heuristics; Expert Systems; Fuzzy Logic; Knowledge Bases; Machine Learning) |
| Big Data | Big Data |
| Electronic Medical Records | Electronic Health Records (Health Information Exchange) |
| Clinical Decision Support Systems | Decision Support Systems, Clinical |
| Computerized Physician Order Entry | Medical Order Entry Systems |
| Database | Database Management Systems |
| Cardiogenic Shock | Shock, Cardiogenic |
| Post-Cardiac | Post-Cardiac Arrest Syndrome |
References
- Elgharably, H.; Gamaleldin, M.; Ayyat, K.S.; Zaki, A.; Hodges, K.; Kindzelski, B.; Yongue, C.; de la Serna, S.; Perez, J.; Spencer, C.; et al. Serious Gastrointestinal Complications after Cardiac Surgery & Associated Mortality. Ann. Thorac. Surg. 2020. [Google Scholar] [CrossRef]
- Tanner, T.G.; Colvin, M.O. Pulmonary Complications of Cardiac Surgery. Lung 2020, 198, 889–896. [Google Scholar] [CrossRef]
- Ghannem, M.; Ahmaidi, S.; Ghannem, L.; Meimoun, P. Infectious and inflammatory complications occurring after cardiac surgery in cardiac rehabilitation centres. Ann. Cardiol. Angeiol. (Paris) 2020, 69, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Hassan, A.; Anderson, C.; Kypson, A.; Kindell, L.; Ferguson, T.B.; Chitwood, W.R.; Rodriguez, E. Clinical Outcomes in Patients With Prolonged Intensive Care Unit Length of Stay After Cardiac Surgical Procedures. Ann. Thorac. Surg. 2012, 93, 565–569. [Google Scholar] [CrossRef]
- Silberman, S.; Bitran, D.; Fink, D.; Tauber, R.; Merin, O. Very Prolonged Stay in the Intensive Care Unit After Cardiac Operations: Early Results and Late Survival. Ann. Thorac. Surg. 2013, 96, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.J.; Nam, K.; Yoo, S.J.; Lee, S.; Bae, J.; Park, J.-Y.; Kim, H.-R.; Kim, T.K.; Jeon, Y. Effects of remote ischemic preconditioning on platelet activation and reactivity in patients undergoing cardiac surgery using cardiopulmonary bypass: A randomized controlled trial. Platelets 2020, 1–9. [Google Scholar] [CrossRef]
- Vedel, A.G.; Holmgaard, F.; Rasmussen, L.S.; Langkilde, A.; Paulson, O.B.; Lange, T.; Thomsen, C.; Olsen, P.S.; Ravn, H.B.; Nilsson, J.C. High-target versus low-target blood pressure management during cardiopulmonary bypass to prevent cerebral injury in cardiac surgery patients: A randomized controlled trial. Circulation 2018, 137, 1770–1780. [Google Scholar] [CrossRef]
- Abrard, S.; Fouquet, O.; Riou, J.; Rineau, E.; Abraham, P.; Sargentini, C.; Bigou, Y.; Baufreton, C.; Lasocki, S.; Henni, S. Preoperative endothelial dysfunction in cutaneous microcirculation is associated with postoperative organ injury after cardiac surgery using extracorporeal circulation: A prospective cohort study. Ann. Intensive Care 2021, 11, 4. [Google Scholar] [CrossRef]
- Rossaint, J.; Berger, C.; Van Aken, H.; Scheld, H.H.; Zahn, P.K.; Rukosujew, A.; Zarbock, A. Cardiopulmonary Bypass during Cardiac Surgery Modulates Systemic Inflammation by Affecting Different Steps of the Leukocyte Recruitment Cascade. PLoS ONE 2012, 7, e45738. [Google Scholar] [CrossRef] [Green Version]
- Itagaki, S.; Chikwe, J.P.; Chiang, Y.P.; Egorova, N.N.; Adams, D.H. Long-Term Risk for Aortic Complications After Aortic Valve Replacement in Patients With Bicuspid Aortic Valve Versus Marfan Syndrome. J. Am. Coll. Cardiol. 2015, 65, 2363–2369. [Google Scholar] [CrossRef] [Green Version]
- Arora, R.C.; Chatterjee, S.; Shake, J.G.; Hirose, H.; Engelman, D.T.; Rabin, J.; Firstenberg, M.; Moosdorf, R.G.H.; Geller, C.M.; Hiebert, B.; et al. Survey of Contemporary Cardiac Surgery Intensive Care Unit Models in the United States. Ann. Thorac. Surg. 2020, 109, 702–710. [Google Scholar] [CrossRef] [PubMed]
- Benoit, M.A.; Bagshaw, S.M.; Norris, C.M.; Zibdawi, M.; Chin, W.D.; Ross, D.B.; Van Diepen, S. Postoperative complications and outcomes associated with a transition to 24/7 intensivist management of cardiac surgery patients. Crit. Care Med. 2017, 45, 993–1000. [Google Scholar] [CrossRef] [PubMed]
- Kumar, K.; Zarychanski, R.; Bell, D.D.; Manji, R.; Zivot, J.; Menkis, A.H.; Arora, R.C. Impact of 24-Hour In-House Intensivists on a Dedicated Cardiac Surgery Intensive Care Unit. Ann. Thorac. Surg. 2009, 88, 1153–1161. [Google Scholar] [CrossRef]
- Rahmanian, P.B.; Kröner, A.; Langebartels, G.; Özel, O.; Wippermann, J.; Wahlers, T. Impact of major non-cardiac complications on outcome following cardiac surgery procedures: Logistic regression analysis in a very recent patient cohort. Interact. Cardiovasc. Thorac. Surg. 2013, 17, 319–327. [Google Scholar] [CrossRef] [Green Version]
- Pimentel, M.F.; Soares, M.J.F.; Junior, J.A.M.; de Oliveira, M.A.B.; Faria, F.L.; Faveri, V.Z.; Iano, Y.; Guido, R.C. Predictive Factors of Long-Term Stay in the ICU after Cardiac Surgery: Logistic CASUS Score, Serum Bilirubin Dosage and Extracorporeal Circulation Time. Braz. J. Cardiovasc. Surg. 2017, 32, 367–371. [Google Scholar] [CrossRef] [Green Version]
- Albanesi, B.; Nania, T.; Barello, S.; Villa, G.; Rosa, D.; Caruso, R.; Udugampolage, N.S.; Casole, L.; Dellafiore, F. Lived experience of patients in after cardiac surgery: A phenomenological study. Nurs. Crit. Care 2020. [Google Scholar] [CrossRef]
- Kolat, P.; Guttenberger, P.; Ried, M.; Kapahnke, J.; Haneya, A.; Schmid, C.; Diez, C. ICU Readmission after Cardiac Surgery—Still a Matter of Concern? Thorac. Cardiovasc. Surg. 2020, 68, 384–388. [Google Scholar] [CrossRef]
- Latif, A.; Kruer, R.; Jarrell, A. Reducing medication errors in critical care: A multimodal approach. Clin. Pharmacol. Adv. Appl. 2014, 6, 117–126. [Google Scholar] [CrossRef] [Green Version]
- Martinez, E.A.; Shore, A.; Colantuoni, E.; Herzer, K.; Thompson, D.A.; Gurses, A.P.; Marsteller, J.A.; Bauer, L.; Goeschel, C.A.; Cleary, K.; et al. Cardiac surgery errors: Results from the UK National Reporting and Learning System. Int. J. Qual. Heal. Care 2011, 23, 151–158. [Google Scholar] [CrossRef] [Green Version]
- Farzi, S.; Irajpour, A.; Saghaei, M.; Ravaghi, H. Causes of medication errors in intensive care units from the perspective of healthcare professionals. J. Res. Pharm. Pract. 2017, 6, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Romero, M.; Vázquez-Naya, J.M.; Pereira, J.; Pereira, M.; Pazos, A.; Baños, G. The iOSC3 System: Using Ontologies and SWRL Rules for Intelligent Supervision and Care of Patients with Acute Cardiac Disorders. Comput. Math. Methods Med. 2013, 2013, 650671. [Google Scholar] [CrossRef] [Green Version]
- Chi, C.-L.; Street, W.N.; Katz, D.A. A decision support system for cost-effective diagnosis. Artif. Intell. Med. 2010, 50, 149–161. [Google Scholar] [CrossRef]
- Kindle, R.D.; Badawi, O.; Celi, L.A.; Sturland, S. Intensive Care Unit Telemedicine in the Era of Big Data, Artificial Intelligence, and Computer Clinical Decision Support Systems. Crit. Care Clin. 2019, 35, 483–495. [Google Scholar] [CrossRef] [PubMed]
- Schuh, C.; de Bruin, J.S.; Seeling, W. Clinical decision support systems at the Vienna General Hospital using Arden Syntax: Design, implementation, and integration. Artif. Intell. Med. 2018, 92, 24–33. [Google Scholar] [CrossRef]
- Fernandes, M.; Vieira, S.M.; Leite, F.; Palos, C.; Finkelstein, S.; Sousa, J.M.C. Clinical Decision Support Systems for Triage in the Emergency Department using Intelligent Systems: A Review. Artif. Intell. Med. 2020, 102, 101762. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.E.W.; Ghassemi, M.M.; Nemati, S.; Niehaus, K.E.; Clifton, D.; Clifford, G.D. Machine Learning and Decision Support in Critical Care. Proc. IEEE 2016, 104, 444–466. [Google Scholar] [CrossRef] [Green Version]
- Sidey-Gibbons, J.A.M.; Sidey-Gibbons, C.J. Machine learning in medicine: A practical introduction. BMC Med. Res. Methodol. 2019, 19, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osheroff, J. Improving Outcomes with Clinical Decision Support; HIMSS Publishing: Boca Ratón, FL, USA, 2012; ISBN 9781498757461. [Google Scholar]
- Tygesen, H.; Eriksson, H.; Herlitz, J. Clinical decision support system (CDSS)—Effects on care quality. Int. J. Health Care Qual. Assur. 2014, 27, 707–718. [Google Scholar] [CrossRef] [Green Version]
- Fan, Y.; Zhao, Y.; Li, P.; Liu, X.; Jia, L.; Li, K.; Feng, C.; Pan, F.; Li, T.; Zhang, Z.; et al. Analysis of diseases distribution in Medical Information Mart for Intensive Care III database. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2018, 30, 531–537. [Google Scholar] [CrossRef]
- Celi, L.; Hinske, L.C.; Alterovitz, G.; Szolovits, P. An artificial intelligence tool to predict fluid requirement in the intensive care unit: A proof-of-concept study. Crit. Care 2008, 12, R151. [Google Scholar] [CrossRef] [Green Version]
- Bashar, S.K.; Hossain, M.B.; Ding, E.; Walkey, A.J.; McManus, D.D.; Chon, K.H. Atrial Fibrillation Detection During Sepsis: Study on MIMIC III ICU Data. IEEE J. Biomed. Heal. Inform. 2020, 24, 3124–3135. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-P.; Payne, T.H.; Nichol, W.P.; Hoey, P.J.; Anderson, C.L.; Gennari, J.H. Evaluating Clinical Decision Support Systems: Monitoring CPOE Order Check Override Rates in the Department of Veterans Affairs’ Computerized Patient Record System. J. Am. Med. Inform. Assoc. 2008, 15, 620–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, A.; Amato, M.G.; Seger, D.L.; Rehr, C.; Wright, A.; Slight, S.P.; Beeler, P.E.; Orav, E.J.; Bates, D.W. Prospective evaluation of medication-related clinical decision support over-rides in the intensive care unit. BMJ Qual. Saf. 2018, 27, 718–724. [Google Scholar] [CrossRef] [Green Version]
- Cresswell, K.; Mozaffar, H.; Shah, S.; Sheikh, A. Approaches to promoting the appropriate use of antibiotics through hospital electronic prescribing systems: A scoping review. Int. J. Pharm. Pract. 2017, 25, 5–17. [Google Scholar] [CrossRef] [Green Version]
- Stultz, J.S.; Nahata, M.C. Computerized clinical decision support for medication prescribing and utilization in pediatrics. J. Am. Med. Inform. Assoc. 2012, 19, 942–953. [Google Scholar] [CrossRef] [Green Version]
- Jin, B.; Che, C.; Liu, Z.; Zhang, S.; Yin, X.; Wei, X. Predicting the Risk of Heart Failure With EHR Sequential Data Modeling. IEEE Access 2018, 6, 9256–9261. [Google Scholar] [CrossRef]
- Dias, D.; Paulo Silva Cunha, J. Wearable Health Devices—Vital Sign Monitoring, Systems and Technologies. Sensors 2018, 18, 2414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downing, N.L.; Rolnick, J.; Poole, S.F.; Hall, E.; Wessels, A.J.; Heidenreich, P.; Shieh, L. Electronic health record-based clinical decision support alert for severe sepsis: A randomised evaluation. BMJ Qual. Saf. 2019, 28, 762–768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prgomet, M.; Li, L.; Niazkhani, Z.; Georgiou, A.; Westbrook, J.I. Impact of commercial computerized provider order entry (CPOE) and clinical decision support systems (CDSSs) on medication errors, length of stay, and mortality in intensive care units: A systematic review and meta-analysis. J. Am. Med. Inform. Assoc. 2017, 24, 413–422. [Google Scholar] [CrossRef] [Green Version]
- Vermeulen, K.M.; van Doormaal, J.E.; Zaal, R.J.; Mol, P.G.M.; Lenderink, A.W.; Haaijer-Ruskamp, F.M.; Kosterink, J.G.W.; van den Bemt, P.M.L.A. Cost-effectiveness of an electronic medication ordering system (CPOE/CDSS) in hospitalized patients. Int. J. Med. Inform. 2014, 83, 572–580. [Google Scholar] [CrossRef]
- Jacob, V.; Thota, A.B.; Chattopadhyay, S.K.; Njie, G.J.; Proia, K.K.; Hopkins, D.P.; Ross, M.N.; Pronk, N.P.; Clymer, J.M. Cost and economic benefit of clinical decision support systems for cardiovascular disease prevention: A community guide systematic review. J. Am. Med. Inform. Assoc. 2017, 24, 669–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Njie, G.J.; Proia, K.K.; Thota, A.B.; Finnie, R.K.C.; Hopkins, D.P.; Banks, S.M.; Callahan, D.B.; Pronk, N.P.; Rask, K.J.; Lackland, D.T.; et al. Clinical Decision Support Systems and Prevention. Am. J. Prev. Med. 2015, 49, 784–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fillmore, C.L.; Bray, B.E.; Kawamoto, K. Systematic review of clinical decision support interventions with potential for inpatient cost reduction. BMC Med. Inform. Decis. Mak. 2013, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ann McKibbon, K.; Lokker, C.; Handler, S.M.; Dolovich, L.R.; Holbrook, A.M.; O’Reilly, D.; Tamblyn, R.; Hemens, B.J.; Basu, R.; Troyan, S.; et al. The effectiveness of integrated health information technologies across the phases of medication management: A systematic review of randomized controlled trials. J. Am. Med. Informatics Assoc. 2012, 19, 22–30. [Google Scholar] [CrossRef] [Green Version]
- Sutton, R.T.; Pincock, D.; Baumgart, D.C.; Sadowski, D.C.; Fedorak, R.N.; Kroeker, K.I. An overview of clinical decision support systems: Benefits, risks, and strategies for success. npj Digit. Med. 2020, 3, 17. [Google Scholar] [CrossRef] [Green Version]
- Chuo, J.; Hicks, R.W. Computer-Related Medication Errors in Neonatal Intensive Care Units. Clin. Perinatol. 2008, 35, 119–139. [Google Scholar] [CrossRef]
- MacK, E.H.; Wheeler, D.S.; Embi, P.J. Clinical decision support systems in the pediatric intensive care unit. Pediatr. Crit. Care Med. 2009, 10, 23–28. [Google Scholar] [CrossRef]
- York, J.B.; Cardoso, M.Z.; Azuma, D.S.; Beam, K.S.; Binney, G.G.; Weingart, S.N. Computerized Physician Order Entry in the Neonatal Intensive Care Unit: A Narrative Review. Appl. Clin. Inform. 2019, 10, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Banner, M.J.; Euliano, N.R.; MacIntyre, N.R.; Layon, A.J.; Bonett, S.; Gentile, M.A.; Bshouty, Z.; Peters, C.; Gabrielli, A. Ventilator Advisory System Employing Load and Tolerance Strategy Recommends Appropriate Pressure Support Ventilation Settings. Chest 2008, 133, 697–703. [Google Scholar] [CrossRef]
- Campion, T.R.; May, A.K.; Waitman, L.R.; Ozdas, A.; Lorenzi, N.M.; Gadd, C.S. Characteristics and effects of nurse dosing over-rides on computer-based intensive insulin therapy protocol performance. J. Am. Med. Inform. Assoc. 2011, 18, 251–258. [Google Scholar] [CrossRef] [Green Version]
- Denaï, M.A.; Mahfouf, M.; Ross, J.J. A hybrid hierarchical decision support system for cardiac surgical intensive care patients. Part I: Physiological modelling and decision support system design. Artif. Intell. Med. 2009, 45, 35–52. [Google Scholar] [CrossRef] [PubMed]
- Hsu, J.-C.; Chen, Y.-F.; Chung, W.-S.; Tan, T.-H.; Chen, T.; Chiang, J.Y. Clinical Verification of A Clinical Decision Support System for Ventilator Weaning. Biomed. Eng. Online 2013, 12, S4. [Google Scholar] [CrossRef] [Green Version]
- Jalali, A.; Bender, D.; Rehman, M.; Nadkanri, V.; Nataraj, C. Advanced analytics for outcome prediction in intensive care units. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 2520–2524. [Google Scholar]
- Jalali, A.; Simpao, A.F.; Gálvez, J.A.; Licht, D.J.; Nataraj, C. Prediction of Periventricular Leukomalacia in Neonates after Cardiac Surgery Using Machine Learning Algorithms. J. Med. Syst. 2018, 42, 177. [Google Scholar] [CrossRef]
- Kallet, R.H.; Branson, R.D. Respiratory controversies in the critical care setting. Do the NIH ARDS Clinical Trials Network PEEP/FIO2 tables provide the best evidence-based guide to balancing PEEP and FIO2 settings in adults? Respir. Care 2007, 52, 461–475; discussion 475–477. [Google Scholar]
- May, L.J.; Longhurst, C.A.; Pageler, N.M.; Wood, M.S.; Sharek, P.J.; Zebrack, C.M. Optimizing Care of Adults With Congenital Heart Disease in a Pediatric Cardiovascular ICU Using Electronic Clinical Decision Support. Pediatr. Crit. Care Med. 2014, 15, 428–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, J.J.; Denaï, M.A.; Mahfouf, M. A hybrid hierarchical decision support system for cardiac surgical intensive care patients. Part II. Clinical implementation and evaluation. Artif. Intell. Med. 2009, 45, 53–62. [Google Scholar] [CrossRef]
- Sintchenko, V.; Coiera, E. Decision complexity affects the extent and type of decision support use. In AMIA Annual Symposium Proceedings; American Medical Informatics Association: Bethesda, MD, USA, 2006; pp. 724–728. [Google Scholar]
- Sondergaard, S.; Wall, P.; Cocks, K.; Parkin, W.G.; Leaning, M.S. High concordance between expert anaesthetists’ actions and advice of decision support system in achieving oxygen delivery targets in high-risk surgery patients. Br. J. Anaesth. 2012, 108, 966–972. [Google Scholar] [CrossRef] [Green Version]
- Thompson, B.T.; Orme, J.F.; Zheng, H.; Luckett, P.M.; Truwit, J.D.; Willson, D.F.; Hite, R.D.; Brower, R.G.; Bernard, G.R.; Curley, M.A.Q.; et al. Multicenter Validation of a Computer-Based Clinical Decision Support Tool for Glucose Control in Adult and Pediatric Intensive Care Units. J. Diabetes Sci. Technol. 2008, 2, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Warrick, C.; Naik, H.; Avis, S.; Fletcher, P.; Franklin, B.D.; Inwald, D. A clinical information system reduces medication errors in paediatric intensive care. Intensive Care Med. 2011, 37, 691–694. [Google Scholar] [CrossRef] [PubMed]
- Zaslansky, R.; Rothaug, J.; Chapman, R.C.; Backström, R.; Brill, S.; Engel, C.; Fletcher, D.; Fodor, L.; Funk, P.; Gordon, D.; et al. PAIN OUT: An international acute pain registry supporting clinicians in decision making and in quality improvement activities. J. Eval. Clin. Pract. 2014, 20, 1090–1098. [Google Scholar] [CrossRef]
- Aushev, A.; Ripoll, V.R.; Vellido, A.; Aletti, F.; Pinto, B.B.; Herpain, A.; Post, E.H.; Medina, E.R.; Ferrer, R.; Baselli, G.; et al. Feature selection for the accurate prediction of septic and cardiogenic shock ICU mortality in the acute phase. PLoS ONE 2018, 13, e0199089. [Google Scholar] [CrossRef] [Green Version]
- Johnson, A.E.W.; Pollard, T.J.; Shen, L.; Lehman, L.H.; Feng, M.; Ghassemi, M.; Moody, B.; Szolovits, P.; Anthony Celi, L.; Mark, R.G. MIMIC-III, a freely accessible critical care database. Sci. Data 2016, 3, 160035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeed, M.; Villarroel, M.; Reisner, A.T.; Clifford, G.; Lehman, L.-W.; Moody, G.; Heldt, T.; Kyaw, T.H.; Moody, B.; Mark, R.G. Multiparameter Intelligent Monitoring in Intensive Care II: A public-access intensive care unit database. Crit. Care Med. 2011, 39, 952–960. [Google Scholar] [CrossRef] [Green Version]
- Rojas, J.C.; Carey, K.A.; Edelson, D.P.; Venable, L.R.; Howell, M.D.; Churpek, M.M. Predicting Intensive Care Unit Readmission with Machine Learning Using Electronic Health Record Data. Ann. Am. Thorac. Soc. 2018, 15, 846–853. [Google Scholar] [CrossRef]
- Armada, E.R.; Villamañán, E.; López-de-Sá, E.; Rosillo, S.; Rey-Blas, J.R.; Testillano, M.L.; Álvarez-Sala, R.; López-Sendón, J. Computerized physician order entry in the cardiac intensive care unit: Effects on prescription errors and workflow conditions. J. Crit. Care 2014, 29, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Gouyon, B.; Iacobelli, S.; Saliba, E.; Quantin, C.; Pignolet, A.; Jacqz-Aigrain, E.; Gouyon, J.B. A Computer Prescribing Order Entry-Clinical Decision Support system designed for neonatal care: Results of the ‘preselected prescription’ concept at the bedside. J. Clin. Pharm. Ther. 2017, 42, 64–68. [Google Scholar] [CrossRef]
- Vardi, A.; Efrati, O.; Levin, I.; Matok, I.; Rubinstein, M.; Paret, G.; Barzilay, Z. Prevention of potential errors in resuscitation medications orders by means of a computerised physician order entry in paediatric critical care. Resuscitation 2007, 73, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Wulff, A.; Haarbrandt, B.; Tute, E.; Marschollek, M.; Beerbaum, P.; Jack, T. An interoperable clinical decision-support system for early detection of SIRS in pediatric intensive care using openEHR. Artif. Intell. Med. 2018, 89, 10–23. [Google Scholar] [CrossRef]
- Khalifa, M.; Magrabi, F.; Gallego, B. Developing a framework for evidence-based grading and assessment of predictive tools for clinical decision support. BMC Med. Inform. Decis. Mak. 2019, 19, 207. [Google Scholar] [CrossRef] [Green Version]
- Myssiorek, D.; Ahmed, Y.; Parsikia, A.; Castaldi, M.; McNelis, J. Factors predictive of the development of surgical site infection in thyroidectomy—An analysis of NSQIP database. Int. J. Surg. 2018, 60, 273–278. [Google Scholar] [CrossRef]
- Wessler, B.S.; Lai YH, L.; Kramer, W.; Cangelosi, M.; Raman, G.; Lutz, J.S.; Kent, D.M. Clinical Prediction Models for Cardiovascular Disease. Circ. Cardiovasc. Qual. Outcomes 2015, 8, 368–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elshayib, M.; Pawola, L. Computerized provider order entry–related medication errors among hospitalized patients: An integrative review. Health Inform. J. 2020, 26, 2834–2859. [Google Scholar] [CrossRef] [PubMed]
- Manias, E.; Kusljic, S.; Wu, A. Interventions to reduce medication errors in adult medical and surgical settings: A systematic review. Ther. Adv. Drug Saf. 2020, 11, 204209862096830. [Google Scholar] [CrossRef]
- Kinlay, M.; Zheng, W.Y.; Burke, R.; Juraskova, I.; Moles, R.; Baysari, M. Medication errors related to computerized provider order entry systems in hospitals and how they change over time: A narrative review. Res. Soc. Adm. Pharm. 2020. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, A.; Canobbio, M.; Clarke, J.; Randall, M.; Skelland, T.; Weston, E. Incidence and prevalence of intravenous medication errors in the UK: A systematic review. Eur. J. Hosp. Pharm. 2020, 27, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Hosseini-Marznaki, Z.; Pouy, S.; Salisu, W.J.; Emami Zeydi, A. Medication errors among Iranian emergency nurses: A systematic review. Epidemiol. Health 2020, 42, e2020030. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Country | Sample | Event Identified | Associated to | Description | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Type | Number | CDSS | CPOE | Database | EHR | Purpose of the Study | Main Findings | |||
| Armada et al., 2014 [69] | Spain | Adult patients | 137 | Cardiogenic shock, acute coronary syndrome, and malignant arrhythmias | x | This study analyzed the effects of the Computerized Physician Order Entry (CPOE) system in cardiac patients by detecting medication errors and evaluating the use of electronic prescription by health professionals. | The results concluded that CPOE was safe in practice and was well received by health professionals, and its use reduced errors in the prescription. | |||
| Aushev et al., 2018 [65] | USA | Adult patients | 75 | Cardiogenic shock and septic shock | x | The aim of the study was to identify clinical features that can predict mortality associated with cardiogenic or septic shock. | This study determined that the application of different models for prediction can prognosticate the risk of death in the acute phase of cardiogenic and septic shock. | |||
| Banner et al., 2008 [51] | USA | Adult patients | 87 | Respiratory failure | x | This study aimed to validate the advisory system recommendation, compared to the experienced physician’s decision. | The results indicated that there were not significant differences in either system. The advisory system was well evaluated due to its forecasts in settings of pressure support ventilation (PSV). | |||
| Campion et al., 2011 [52] | USA | Adult patients | 179,452 | Emergency general surgery, vascular surgery, and cardiac/thoracic surgery | x | The objective of this study was to determine the effects and conditions resulting from nurses’ override of clinical decision support system (CDSS) recommendations in ICUs. | The study concluded that the nurses accepted among 95% of dosing recommendations. The evaluation of the frequency, direction, and resistance of the intensive insulin therapy (IIT) of the CDSS overrides may be interesting for the health professionals and researchers. | |||
| Denaï et al., 2009 [53] | United Kingdom | Adult patients | 7 | Impaired cardiac function | x | The aim of the study was to develop a CDSS for clinicians’ decision making in post-cardiac surgery patients weaned from cardiopulmonary bypass. | The study showed good feasibility for applying CDSS to control the cardiovascular system in post-surgery patient. | |||
| Gouyon et al., 2017 [70] | France | Pediatric patients | 760 | Lower gestational age | x | x | This project evaluated the performance of the CDSS/CPOE combination, using the out-of-range dose rate. | The conclusion was that the CDSS/CPOE system was feasible for the prescription of all drugs in ICUs. This system allows for the evaluation and comparison of drugs. | ||
| Hsu et al., 2013 [54] | Japan | Adult patients | 380 | Respiratory failure | x | The objective was to verify the effectiveness of a CDSS to predict and reduce the use of ventilator weaning. | This CDSS was effective in the identification of the earliest time of ventilator weaning for a patient to resume and sustain spontaneous breathing. | |||
| Jalali et al., 2016 [55] | USA | Adult patients | 4000 | Cardiac surgery and infections | x | The study’s purpose was to develop a CDSS algorithm for predicting the prognostic of patients in ICUs. | The conclusions demonstrated that CDSSs can resolve complex situations in ICUs. | |||
| Jalali et al., 2018 [56] | USA | Pediatric patients | 71 | Periventricular leukomalacia | x | The aim was to design a classifier adaptable to the patient and incorporated into the experts’ opinion in the classification process. | This project collected data from a highly reliable digital instrument with greater frequency, expanding the set of features, pre-classifying patients according to the diagnosis. | |||
| Johnson et al., 2016 [66] | USA | Adult patients | 38597 | Coronary disease, cardiac surgery, trauma, and surgical procedure | x | This study wanted to determine the accessibility of the Medical Information Mart for Intensive Care III (MIMIC-III) database for the scientific community. | The study concluded that the MIMIC-III database allowed access to ICU data at an international level, improving the quality of academic and industrial research. | |||
| Kallet et al., 2007 [57] | Canada | Adult patients | NA | Pulmonary and cardiac surgery | x | This paper reviewed the use of the National Institutes of Health acute respiratory distress syndrome (ARDS) network positive end-expiratory pressure (PEEP)/ inspired oxygen fraction (FIO2) titration tables to the treatment of patients with ARDS. | The study determined that the PEEP/FIO2 tables were a good option for the treatment of ARDS. | |||
| May et al., 2014 [58] | USA | Adult patients | 114 | Cardiac surgery | x | This project’s purpose was to determine if CDSSs will facilitate better compliance with project measures and improve healthcare. | Through CDSSs, compliance with national surgical quality was improved. | |||
| Rojas et al., 2018 [68] | USA | Adult patients | 24885 | Medical, surgical, and coronary care | x | The aim was to use an automatic learning technique to derive an ICU readmission model with electronic medical record variables in real time. | The study developed and validated readmission prediction modeling of ICUs through a novel machine modeling technique. | |||
| Ross et al., 2009 [59] | United Kingdom | Adult patients | 3 | Cardiac surgery | x | The study determined whether the CDSS process provides clinical decision-making advice to anesthesiologists. | CDSSs developed proposed real-time diagnostic and therapeutic advice based on the continuous monitoring of cardiovascular hemodynamic patients. | |||
| Saeed et al., 2011 [67] | USA | Adult patients | 22,870 | Cardiac diseases and coronary problems | x | The study’s purpose was to develop an ICU research database through automated techniques to aggregate high-resolution diagnostic and therapeutic data in ICU adult patients. | The study concluded that the MIMIC-II database is a resource that supports decision making. | |||
| Sintchenko et al., 2006 [60] | Australia | Specialists Intensive Care | 31 | None | x | The aim was to examine the impact of CDSSs for ICU antibiotic prescribing. | The study concluded that CDSSs are an important factor in the process of complex decisions; it supported decision making and the functionality of different tasks. | |||
| Sondergaard et al., 2012 [61] | Sweden | Adult patients | 24 | Pancreatic cancer, heart transplants, and intestinal carcinoid diseases | x | The study’s purpose was to research the performance of CDSSs in achieving some parameters in patients with major abdominal surgery. | The results demonstrated that there was a concordance between the recommend treatments of CDSSs and the treatments of anesthetists. | |||
| Thompson et al., 2008 [62] | USA | All adult and pediatric patients | 148 | Pulmonary, neurological, cardiovascular, gastrointestinal, and multisystem diseases | x | The aim was to determine the effectiveness, satisfaction, and acceptance of eProtocol-insulin in ICUs. | eProtocol-insulin was generally accepted in ICUs. This study demonstrated that it can be a decision-support tool and a method for use in practices and clinical research. | |||
| Vardi et al., 2007 [71] | Israel | Pediatric patients | 105 | Congenital heart diseases, metabolic diseases, multiple traumas, head traumas, respiratory diseases, and sepsis | x | x | The objective was to determine the impact of CDSS/CPOE in the preventions of medical errors in medication resuscitation orders. | The project considered that this warning system is a support tool in drug treatment, leading to medical error reductions. | ||
| Warrick et al., 2011 [63] | United Kingdom | Pediatric patients | NA | None | x | The study wanted to determine the effect of electronic prescribing (EP) on prescribing errors and doses in pediatric ICUs. | The study determined that EP increases medication safety in pediatric ICUs. | |||
| Wulff et al., 2018 [72] | Germany | Pediatric patients | 16 | None | x | x | The aim was to develop and evaluate an open electronic health record (EHR) for systemic inflammatory response syndrome (SIRS) detection in pediatric ICUs. | The study found that the inclusion of an open EHR in a CDSS can bridge the interoperability gap between local infrastructure in said CDSS. | ||
| Zaslansky et al., 2014 [64] | Germany | Adults patients | 40,898 | Pain | x | The aim was to develop and validate a medical registry to measure and identify some aspects regarding pain. | This pain-related CDSS provides health professionals with easy access to data on the clinical management of pain, supporting the decision-making process. | |||
| Patient | Application Area |
|---|---|
| Before admission | Forecast and evolutionary prediction |
| During admission | Reduction in medical errors |
| Alerts, fast detection of alterations, and treatment settings | |
| Achievement of objectives and maintenance in established ranges | |
| After admission | Reduction in health costs |
| Level of satisfaction in health personnel |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, M.; Concheiro-Moscoso, P.; López-Álvarez, A.; Baños, G.; Pazos, A.; Pereira, J. Applicability of Clinical Decision Support in Management among Patients Undergoing Cardiac Surgery in Intensive Care Unit: A Systematic Review. Appl. Sci. 2021, 11, 2880. https://doi.org/10.3390/app11062880
Pereira M, Concheiro-Moscoso P, López-Álvarez A, Baños G, Pazos A, Pereira J. Applicability of Clinical Decision Support in Management among Patients Undergoing Cardiac Surgery in Intensive Care Unit: A Systematic Review. Applied Sciences. 2021; 11(6):2880. https://doi.org/10.3390/app11062880
Chicago/Turabian StylePereira, Miguel, Patricia Concheiro-Moscoso, Alexo López-Álvarez, Gerardo Baños, Alejandro Pazos, and Javier Pereira. 2021. "Applicability of Clinical Decision Support in Management among Patients Undergoing Cardiac Surgery in Intensive Care Unit: A Systematic Review" Applied Sciences 11, no. 6: 2880. https://doi.org/10.3390/app11062880