
A Case of Plasmodium malariae in Bangladesh: A Representation of the Suboptimal Performance of Rapid Diagnostic Approaches in Malaria Elimination Settings
 , and
, and 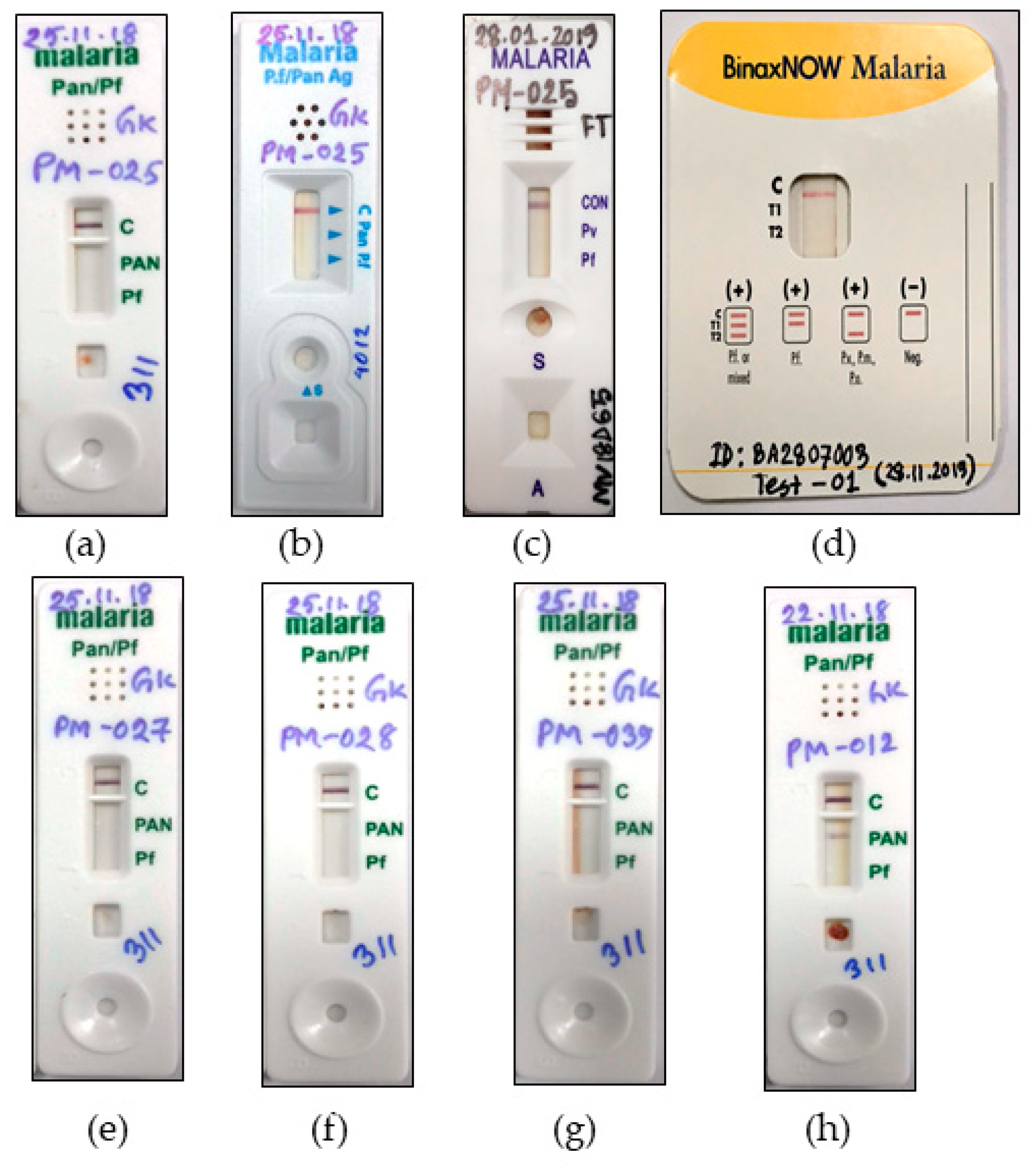{kind=link}
Abstract
:1. Introduction
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fuehrer, H.P.; Campino, S.; Sutherland, C.J. The primate malaria parasites Plasmodium malariae, Plasmodium brasilianum and Plasmodium ovale spp.: Genomic insights into distribution, dispersal and host transitions. Malar. J. 2022, 21, 138. [Google Scholar] [CrossRef] [PubMed]
- Rahman, W.; Chotivanich, K.; Silamut, K.; Tanomsing, N.; Hossain, A.; Faiz, M.A.; Dondorp, A.M.; Maude, R.J. Plasmodium malariae in Bangladesh. Trans. R. Soc. Trop. Med. Hyg. 2010, 104, 78–80. [Google Scholar] [CrossRef]
- Fuehrer, H.P.; Swoboda, P.; Harl, J.; Starzengruber, P.; Habler, V.E.; Bloeschl, I.; Haque, R.; Matt, J.; Khan, W.A.; Noedl, H. High prevalence and genetic diversity of Plasmodium malariae and no evidence of Plasmodium knowlesi in Bangladesh. Parasitol. Res. 2014, 113, 1537–1543. [Google Scholar] [CrossRef] [PubMed]
- Swoboda, P.; Fuehrer, H.P.; Ley, B.; Starzengruber, P.; Ley-Thriemer, K.; Jung, M.; Matt, J.; Fally, M.A.; Mueller, M.K.; Reismann, J.A.; et al. Evidence of a major reservoir of non-malarial febrile diseases in malaria-endemic regions of Bangladesh. Am. J. Trop. Med. Hyg. 2014, 90, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Starzengruber, P.; Fuehrer, H.P.; Ley, B.; Thriemer, K.; Swoboda, P.; Habler, V.E.; Jung, M.; Graninger, W.; Khan, W.A.; Haque, R.; et al. High prevalence of asymptomatic malaria in south-eastern Bangladesh. Malar. J. 2014, 13, 16. [Google Scholar] [CrossRef] [PubMed]
- Vinetz, J.M.; Li, J.; McCutchan, T.F.; Kaslow, D.C. Plasmodium malariae infection in an asymptomatic 74-year-old Greek woman with splenomegaly. N. Engl. J. Med. 1998, 338, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Gilles, H.M.; Hendrickse, R.G. Nephrosis in Nigerian children. Role of Plasmodium malariae, and effect of antimalarial treatment. Br. Med. J. 1963, 2, 27–31. [Google Scholar] [CrossRef]
- Mueller, I.; Zimmerman, P.A.; Reeder, J.C. Plasmodium malariae and Plasmodium ovale—The “bashful” malaria parasites. Trends Parasitol. 2007, 23, 278–283. [Google Scholar] [CrossRef]
- Betson, M.; Sousa-Figueiredo, J.C.; Atuhaire, A.; Arinaitwe, M.; Adriko, M.; Mwesigwa, G.; Nabonge, J.; Kabatereine, N.B.; Sutherland, C.J.; Stothard, J.R. Detection of persistent Plasmodium spp. infections in Ugandan children after artemether-lumefantrine treatment. Parasitology 2014, 141, 1880–1890. [Google Scholar] [CrossRef]
- Dinko, B.; Oguike, M.C.; Larbi, J.A.; Bousema, T.; Sutherland, C.J. Persistent detection of Plasmodium falciparum, P. malariae, P. ovale curtisi and P. ovale wallikeri after ACT treatment of asymptomatic Ghanaian school-children. Int. J. Parasitol. Drugs Drug Resist. 2013, 3, 45–50. [Google Scholar] [CrossRef] [Green Version]
- Wongsrichanalai, C.; Barcus, M.J.; Muth, S.; Sutamihardja, A.; Wernsdorfer, W.H. A review of malaria diagnostic tools: Microscopy and rapid diagnostic test (RDT). Am. J. Trop. Med. Hyg. 2007, 77, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Mukkala, A.N.; Kwan, J.; Lau, R.; Harris, D.; Kain, D.; Boggild, A.K. An Update on Malaria Rapid Diagnostic Tests. Curr. Infect. Dis. Rep. 2018, 20, 49. [Google Scholar] [CrossRef] [PubMed]
- Ong, C.W.; Lee, S.Y.; Koh, W.H.; Ooi, E.E.; Tambyah, P.A. Monkey malaria in humans: A diagnostic dilemma with conflicting laboratory data. Am. J. Trop. Med. Hyg. 2009, 80, 927–928. [Google Scholar] [CrossRef] [PubMed]
- Directorate General of Health Services. Revised Malaria Treatment Regimen-2017; Directorate General of Health Services: Dhaka, Bangladesh, 2017.
- Snounou, G.; Viriyakosol, S.; Zhu, X.P.; Jarra, W.; Pinheiro, L.; do Rosario, V.E.; Thaithong, S.; Brown, K.N. High sensitivity of detection of human malaria parasites by the use of nested polymerase chain reaction. Mol. Biochem. Parasitol. 1993, 61, 315–320. [Google Scholar] [CrossRef]
- Talman, A.M.; Duval, L.; Legrand, E.; Hubert, V.; Yen, S.; Bell, D.; Le Bras, J.; Ariey, F.; Houze, S. Evaluation of the intra- and inter-specific genetic variability of Plasmodium lactate dehydrogenase. Malar. J. 2007, 6, 140. [Google Scholar] [CrossRef] [PubMed]
- Moody, A. Rapid diagnostic tests for malaria parasites. Clin. Microbiol. Rev. 2002, 15, 66–78. [Google Scholar] [CrossRef] [PubMed]
- Xia, J.; Fan, L.; Si, L.; Lu, Q.; Zhao, Y.; Zhang, M.; Xu, Y.; Wang, B. A Case Report of Serological Rapid Diagnostic Test-Negative Plasmodium malariae Malaria Imported from West Africa. Clin. Lab. 2021, 67, 10. [Google Scholar] [CrossRef]
- Yerlikaya, S.; Campillo, A.; Gonzalez, I.J. A Systematic Review: Performance of Rapid Diagnostic Tests for the Detection of Plasmodium knowlesi, Plasmodium malariae, and Plasmodium ovale Monoinfections in Human Blood. J. Infect. Dis. 2018, 218, 265–276. [Google Scholar] [CrossRef]
- Richter, J.; Göbels, K.; Müller-Stöver, I.; Hoppenheit, B.; Häussinger, D. Co-reactivity of plasmodial histidine-rich protein 2 and aldolase on a combined immuno-chromographic-malaria dipstick (ICT) as a potential semi-quantitative marker of high Plasmodium falciparum parasitaemia. Parasitol. Res. 2004, 94, 384–385. [Google Scholar] [CrossRef]
- Moody, A.H.; Chiodini, P.L. Non-microscopic method for malaria diagnosis using OptiMAL IT, a second-generation dipstick for malaria pLDH antigen detection. Br. J. Biomed. Sci. 2002, 59, 228–231. [Google Scholar] [CrossRef]
- Zhang, S.X.; Kronmann, K.C.; Kavanaugh, M.J. Plasmodium malariae-Repeat Light Microscopy when Molecular Testing is Not Available. Am. J. Trop. Med. Hyg. 2019, 100, 233–234. [Google Scholar] [CrossRef] [PubMed]
- Niño, C.H.; Cubides, J.R.; Camargo-Ayala, P.A.; Rodríguez-Celis, C.A.; Quiñones, T.; Cortés-Castillo, M.T.; Sánchez-Suárez, L.; Sánchez, R.; Patarroyo, M.E.; Patarroyo, M.A. Plasmodium malariae in the Colombian Amazon region: You don’t diagnose what you don’t suspect. Malar. J. 2016, 15, 576. [Google Scholar] [CrossRef] [PubMed]
- Dyer, M.E.; Tjitra, E.; Currie, B.J.; Anstey, N.M. Failure of the ‘pan-malarial’ antibody of the ICT Malaria P.f/P.v immunochromatographic test to detect symptomatic Plasmodium malariae infection. Trans. R. Soc. Trop. Med. Hyg. 2000, 94, 518. [Google Scholar] [CrossRef]
- Deng, Y.; Zhou, R.M.; Zhang, H.W.; Qian, D.; Liu, Y.; Chen, W.Q.; Zhao, X.D. Diagnosis and treatment for three imported Plasmodium malariae malaria cases in Henan Province. Zhongguo Ji Sheng Chong Xue Yu Ji Sheng Chong Bing Za Zhi 2014, 32, 61–63. [Google Scholar]
- Kosack, C.S.; Naing, W.T.; Piriou, E.; Shanks, L. Routine parallel diagnosis of malaria using microscopy and the malaria rapid diagnostic test SD 05FK60: The experience of Médecins Sans Frontières in Myanmar. Malar. J. 2013, 12, 167. [Google Scholar] [CrossRef]
- Moody, A.; Hunt-Cooke, A.; Gabbett, E.; Chiodini, P. Performance of the OptiMAL malaria antigen capture dipstick for malaria diagnosis and treatment monitoring at the Hospital for Tropical Diseases, London. Br. J. Haematol. 2000, 109, 891–894. [Google Scholar] [CrossRef]
- Piper, R.C.; Buchanan, I.; Choi, Y.H.; Makler, M.T. Opportunities for improving pLDH-based malaria diagnostic tests. Malar J. 2011, 10, 213. [Google Scholar] [CrossRef]
- Elizardez, Y.B.; Fotoran, W.L.; Junior, A.J.G.; Curado, I.; Junior, N.K.; Monteiro, E.F.; Romero Neto, I.; Wunderlich, G.; Kirchgatter, K. Recombinant proteins of Plasmodium malariae merozoite surface protein 1 (PmMSP1): Testing immunogenicity in the BALB/c model and potential use as diagnostic tool. PLoS ONE 2019, 14, e0219629. [Google Scholar] [CrossRef] [PubMed]
- Woodford, J.; Collins, K.A.; Odedra, A.; Wang, C.; Jang, I.K.; Domingo, G.J.; Watts, R.; Marquart, L.; Berriman, M.; Otto, T.D.; et al. An Experimental Human Blood-Stage Model for Studying Plasmodium malariae Infection. J. Infect. Dis. 2020, 221, 948–955. [Google Scholar] [CrossRef]
- Paul, R.; Sinha, P.K.; Bhattacharya, R.; Banerjee, A.K.; Raychaudhuri, P.; Mondal, J. Study of C reactive protein as a prognostic marker in malaria from Eastern India. Adv. Biomed. Res. 2012, 1, 41. [Google Scholar] [CrossRef]
- Ho, M.-F.; Baker, J.; Lee, N.; Luchavez, J.; Ariey, F.; Nhem, S.; Oyibo, W.; Bell, D.; González, I.; Chiodini, P.; et al. Circulating antibodies against Plasmodium falciparum histidine-rich proteins 2 interfere with antigen detection by rapid diagnostic tests. Malar. J. 2014, 13, 480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, W.E.; Jeffery, G.M. Plasmodium malariae: Parasite and disease. Clin. Microbiol. Rev. 2007, 20, 579–592. [Google Scholar] [CrossRef] [PubMed]
- Lover, A.A.; Baird, J.K.; Gosling, R.; Price, R.N. Malaria Elimination: Time to Target All Species. Am. J. Trop. Med. Hyg. 2018, 99, 17–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Johora, F.T.; Kibria, M.G.; Fuehrer, H.-P.; Alam, M.S. A Case of Plasmodium malariae in Bangladesh: A Representation of the Suboptimal Performance of Rapid Diagnostic Approaches in Malaria Elimination Settings. Pathogens 2022, 11, 1072. https://doi.org/10.3390/pathogens11101072
Johora FT, Kibria MG, Fuehrer H-P, Alam MS. A Case of Plasmodium malariae in Bangladesh: A Representation of the Suboptimal Performance of Rapid Diagnostic Approaches in Malaria Elimination Settings. Pathogens. 2022; 11(10):1072. https://doi.org/10.3390/pathogens11101072
Chicago/Turabian StyleJohora, Fatema Tuj, Mohammad Golam Kibria, Hans-Peter Fuehrer, and Mohammad Shafiul Alam. 2022. "A Case of Plasmodium malariae in Bangladesh: A Representation of the Suboptimal Performance of Rapid Diagnostic Approaches in Malaria Elimination Settings" Pathogens 11, no. 10: 1072. https://doi.org/10.3390/pathogens11101072