1. Introduction
Structure design codes worldwide specify ductile structure types which provide collapse avoidance, not functionality. Data from 13 earthquakes show that 90% of hospitals constructed as ductile structures lost functionality after severe earthquake shaking [
1,
2,
3,
4,
5]. The loss of hospital functionality resulted from earthquake structure force demands that were 3 to 20 times stronger than the minimal seismic design loads specified by structure codes for collapse avoidance. Laws, codes, and specifications on expected earthquake performance, require that all new hospitals be constructed to retain their maximum capacity to function after earthquakes [
6,
7,
8]. The Seismic Isolator Standard “SIS” is the only standard that specifies design criteria for retaining the functionality of hospitals after earthquakes [
1].
The first seismic isolators were implemented in New Zealand in 1981 with the intent to minimize earthquake damage and maintain functionality after earthquakes [
9]. Over 38 years of applications of isolators compliant with the American Seismic Isolator Standard have shown that SIS isolators effectively protect against earthquake damage, and result in cost effective construction for a broad range of important structures [
10]. Chapter 1 of the USA structure design code, ASCE 7, requires all new hospitals and essential facilities to be constructed to be functional after earthquakes. However, Chapter 12 of ASCE 7 specifies ductile structure types that were developed 5 decades ago only to provide minimum collapse resistance. The ASCE 7 seismic performance objective is that less than 10% of ductile structures will suffer collapse during earthquakes [
7].
Figure 1.
Adana Hospital Complex, Turkey, 100% Functional after 2023 Turkey Earthquakes.
Figure 1.
Adana Hospital Complex, Turkey, 100% Functional after 2023 Turkey Earthquakes.
Figure 2.
Elazig Hospital Complex, Turkey, 100% Functional after 2020 Earthquakes.
Figure 2.
Elazig Hospital Complex, Turkey, 100% Functional after 2020 Earthquakes.
Despite the laws and codes mandating functionality, and the fact that 90% of hospitals constructed as ductile structures have lost functionality, most new hospitals are still being constructed as ductile structures, which results in fatalities, and is against the law!
SIS isolators are the only earthquake proven means of avoiding damage and retaining the functionality of facilities after earthquakes. However, depending on which isolator product standard is specified, seismic isolators can either protect against earthquake damage, or cause structure collapse. Over 4000 seismic isolators not compliant with the SIS have failed during earthquakes, or under gravity loads only [
11]. During 2 earthquakes, the non-SIS isolators suffered structural collapse [
12,
13]. undreds of other isolators have resulted in more earthquake damage than structures built without isolators [
14,
15]. Learning from these isolator failures, all seismic isolators should comply with the American Seismic Isolator Standard, which is the only safe and effective product standard for seismic isolators.
Loss of Hospital Functionality: 667 of 740 hospitals lost functionality (90%), during 13 earthquakes that ranged from mild to very strong, that occurred from 1994 through 2023 [
2,
3,
16,
17,
18]. All 667 hospitals that lost functionality were designed as ductile structures according to the code. These 667 hospitals closed on the day of the earthquakes, the very day they were needed most [
17,
18]. The earthquake injured persons did not have hospitals available to provide them emergency medical care, and many died. The patients that were resident in the hospitals on the day of the earthquakes were moved out to the streets, and many died. 40 Years of earthquake data have consistently shown that 90% of hospitals constructed as ductile structures lose functionality during earthquakes. Current laws and codes worldwide require hospitals to be constructed to function at maximum capacity after earthquakes [
19]. It is the responsibility of all construction industry professionals to build all new hospitals and essential facilities to retain their maximum capacity to function after earthquakes. Yet, 95% of new hospitals are still being designed by structural engineers as ductile moment resisting frames.
It is the professional responsibility of health care architects and engineers to construct hospitals that reliably retain their maximum capacity to function after earthquakes. Functionality is a much higher performance standard than “Immediate Occupancy”. The ASCE standard for Immediate Occupancy implements ductile structures that are safe to occupy after an earthquake, such that the necessary earthquake damage repairs can be safely performed. Compliance with criteria for Immediate Occupancy does not comply with the laws and codes that require hospitals to be constructed to function at maximum capacity after earthquakes. To retain the functionality of hospitals after earthquakes, it is necessary to limit damage to less than 2% of replacement cost, the performance criteria which is implemented by the American Seismic Isolator Standard “SIS”.
Earthquake Proven Hospital Functionality: The SIS is the only construction standard that has been proven by earthquake performance to limit damage sufficiently to reliably retain facility functionality. For 34 years, all structures with SIS compliant seismic isolators have retained 100% functionality after earthquakes. The 2023 magnitude 7.8 Turkey earthquake, and 2016 magnitude 7.8 Ecuador earthquake, and over 100 other earthquakes worldwide, have resulted in seismic force demands 3 to 20 times stronger than the minimum seismic design loads specified by structure codes for collapse avoidance. These powerful earthquakes destroyed over 700,000 structures designed as ductile structures according to the code. Structures with SIS isolators have been the only essential structures to retain 100% functionality after such very strong earthquake shaking.
The Adana hospital Complex (
Figure 1) as in the disaster region of Turkey’s 2023 magnitude 7.8 earthquake and 49 aftershocks of magnitudes 5.0 to 7.5. The 8 g earthquake force demands were 20 times greater than the seismic design loads specified by the building code. There were: 55,000 fatalities; 236 inoperable health care facilities; 35,000 collapses; and 220,000 buildings demolished [
4].
Figure 3.
Acapulco Emergency Response Center, 100% Functional after 2021 Earthquakes.
Figure 3.
Acapulco Emergency Response Center, 100% Functional after 2021 Earthquakes.
Figure 4.
Texas Instruments, Medical Instruments Factory, Philippines, 100% Functional.
Figure 4.
Texas Instruments, Medical Instruments Factory, Philippines, 100% Functional.
Yet, Adana’s 550,000 square meters of hospital buildings retained 100% functionality, thereby saving many lives by caring for over 10,000 earthquake injured persons. This was the second time hospitals were 100% functional after such strong earthquake shaking.
The Elazig Hospital Complex (
Figure 2) were the closest hospital buildings to the epicenter of Turkey’s 2020 magnitude 6.7 Elazig earthquake. The Elazig hospitals maintained 100% functionality, saving many lives by caring for over 1000 earthquake injured persons. The Elazig earthquake caused 87 other multi-story buildings to collapse, and over 5000 buildings to lose functionality, of which 1287 were later demolished [
20]. The Elazig hospitals were the first to be completely functional after experiencing such strong earthquake shaking.
34 Years of Earthquake Proven Functionality in 18 Essential Structures: The Acapulco Emergency Response Center (
Figure 3) was 9 km from the epicenter of Acapulco’s 2021 magnitude 7.1 earthquake. It remained 100% functional during and after the earthquake. The soft bay muds resulted in ground accelerations of 0.54 g, and structure base shear demands of 1.1 g. The seismic force demands on the Acapulco Emergency Response Center were 10 times the seismic design loads specified by the building code for collapse avoidance. The emergency response center was able to respond to all calls for emergency assistance without interruption [
2]. This was the first time an emergency response center suffered no damage to architectural components and communications equipment after very strong earthquake shaking. The 100% functionality of Acapulco Emergency Response Center saved many lives.
Texas Instruments’ (
Figure 4) Philippines Plant has fragile manufacturing equipment that produce microprocessors used in medical devices. The facility’s manufacturing equipment remained completely functional after the 2019 magnitude 6.1 earthquake [
21]. The nearby airport and other buildings were forced to close because of earthquake shaking damage. Several older buildings in the area collapsed.
Ecuador’s 2016 magnitude 7.8 earthquake fault ruptured directly under the Bahia Bridge (
Figure 5). The 3 g seismic force demands were 20 times the seismic design loads specified by the code. Yet, this bridge remained 100% functional. In the 24 h after the earthquake, 15,000 vehicles crossed the Bahia Bridge to evacuate thousands of injured persons from the destroyed city [
22]. The SIS seismic isolators reduced the seismic design loads on the pile foundations by 80%, thereby reducing initial construction costs by 5%, and also avoiding damage from an extreme earthquake. Three other bridges with SIS pendulum isolators were within Ecuador’s 2016 fault rupture area, and also remained 100% functional.
Two large concrete Liquid Natural Gas tanks were completely functional after Chile’s 2010 Magnitude 8.8 Earthquake, and a Magnitude 7.1 aftershock with the epicenter 3 km from the tanks (
Figure 6). These tanks are critical for Chile to produce electric power. In Mexico, two large concrete Liquid Natural Gas tanks were completely functional after the 2022 magnitude 7.6 earthquake (
Figure 7). These concrete LNG tanks were protected by SIS isolators. The storage of hazardous materials is incompatible with the ductile structures specified by the building codes. The leaking of billions of liters of liquid natural gas from the concrete tanks would cause a fire, explosion, and major public catastrophe.
It is more reliable and lower cost construction to absorb earthquake displacements in SIS isolators, than to absorb earthquake displacements through the yielding of special ductile structural members. Turkey’s Adana and Elazig hospital complexes, Acapulco’s Emergency Response Center; Texas Instrument’s Philippines Medical Instruments Factory; Ecuador’s 4 epi-central bridges, 2 Liquid Natural Gas Tanks in Chile; 2 Liquid Natural Gas Tanks in Mexico, and DOW Chemical Company’s Emergency Water Tank in California; all retained 100% functionality after experiencing major earthquakes that caused seismic force demands from 3 to 20 times the seismic design loads specified by structure codes for collapse avoidance.
Figure 5.
Bahia Bridge Ecuador, 100% Functional after 2016 Earthquakes.
Figure 5.
Bahia Bridge Ecuador, 100% Functional after 2016 Earthquakes.
Figure 6.
LNG Tanks, Chile, 100% Functional after 2010 M8.8 Earthquake.
Figure 6.
LNG Tanks, Chile, 100% Functional after 2010 M8.8 Earthquake.
Figure 7.
LNG Tanks, Mexico, 100% Functional after 2022 M7.6 Earthquake.
Figure 7.
LNG Tanks, Mexico, 100% Functional after 2022 M7.6 Earthquake.
These 18 essential structures, and hundreds of other structures, implemented pendulum isolators compliant with the Seismic Isolator Standard. The 100% functioning of these 18 essential structures after strong earthquakes confirms that seismic isolators compliant with the Seismic Isolator Standard reliably maintains a facility’s maximum capacity to function after earthquakes.
2. When Hospital Lose Functionality, Lives Are Lost!
The 2023 Turkey earthquakes caused 55,000 fatalities, and 236 inoperable health care facilities [
4]. Since 1994, earthquakes have caused over 800,000 deaths [
5]. Over 400,000 people died on the day of the earthquakes. Over 400,000 people died after the earthquakes because they could not receive adequate medical care. Since 1994, 13 earthquakes resulted in 667 of 740 hospitals losing functionality, 90% [
2,
3]. Interior Damage (
Figure 8) to architectural components is the primary cause of lost functionality. When hospitals lost functionality the earthquake injured persons did not receive the medical care they needed, and patients that were in the hospitals are put out onto the streets, increasing fatalities by hundreds of thousands (
Figure 9). In 2019, on the day of a mild magnitude 6.4 earthquake, California’s new Ridgecrest Hospital closed [
16]. The seismic load demands were 3 times stronger than the minimal seismic design loads specified by structure code. Damage to the hospital’s fragile architectural components and equipment forced it to close on the day it was needed most. The hospital appeared undamaged from the exterior. Most hospitals that lose functionality appear undamaged from the outside. The September 2022 magnitude 7.6 earthquake in Mexico caused 10 of 10 hospitals to lose functionality [
2]. The 2017 magnitude 7.1 earthquake in Mexico caused 26 of 31 hospitals to lose functionality [
2]. The magnitude 7.8 earthquake in Ecuador resulted in structure force demands 20 times stronger than the minimal seismic design loads specified by the code, causing 39 of 50 hospitals to suffer very severe damage and loss of functionality, of which 20 hospitals were later demolished [
18,
23].
The 2 hospitals that remained functional complied with the SIS acceleration and drift limits. 4 hospitals that lost functionality exceeded both the acceleration and drift limits. 3 hospitals that lost functionality exceeded the drift limit, but not the acceleration limit. For the 7 hospitals that lost functionality, the peak floor spectra accelerations exceeded 5 g, causing severe interior damage.
Figure 10 shows 7 hospitals that lost functionality after Mexico’s 2017 magnitude 7.1 earthquake, and 2 hospitals that retained functionality.
A magnitude 7.9 earthquake in Peru resulted in 6 of 10 hospitals being demolished [
3]. A magnitude 8.8 earthquake in Chile caused 60 of 80 hospitals to lose functionality [
24]. The 1995 magnitude 6.9 earthquake in Kobe Japan caused 176 out of 180 hospitals to lose functionality [
25]. The 1994 magnitude 6.7 California earthquake resulted in 38 hospitals suffering major architectural component damage, and 4 suffering severe structural damage [
19]. The Olive View Hospital had in-structure spectral accelerations over 4.0 g, and remained closed for 3 months [
26]. New Zealand’s Christchurch Women’s Hospital was constructed with rubber seismic isolators designed according to the structure code. Magnitude 6 earthquakes caused damage exceeding 30% of replacement costs [
14]. Repairs took over 4 years. It is clear that the ductile structure types specified in the codes do not deliver the hospital functionality which is required by the laws and codes. Of the 667 hospitals that lost functionality, all had excessive in-structure accelerations or deformations causing architectural component damage. Of the 41 of 740 hospital buildings that remained functional, 7 implemented SIS isolators, and 34 were just lucky to have low seismic demands at their particular sites. Median floor spectra accelerations over 0.3 g consistently cause loss of hospital functionality, as occurred with the new Ridgecrest Hospital. Structure drifts exceeding 0.3% also consistently cause loss of hospital functionality. All hospitals without SIS isolators have lost functionality when exposed to severe earthquake shaking.
The 2 SIS Functionality Criteria are:
Figure 8.
Hospital Interior Damage.
Figure 8.
Hospital Interior Damage.
Figure 9.
Hospital Patients in the Street.
Figure 9.
Hospital Patients in the Street.
Figure 10.
7 hospitals that lost functionality, and 2 hospitals that retained functionality, plus 8 earthquake ground motion recording stations.
Figure 10.
7 hospitals that lost functionality, and 2 hospitals that retained functionality, plus 8 earthquake ground motion recording stations.
These SIS functionality criteria were checked against the functionality performance of 9 hospitals that experienced Mexico’s 2017 magnitude 7.1 earthquake [
2] (
Figure 10). Earthquake ground motion records were available near these 9 hospitals. Of the 9 hospitals, 7 lost functionality, and 2 retained functionality. The earthquake shaking for the 2 hospitals that retained functionality were significantly less severe than those for the 7 hospitals that lost functionality. 2 hospitals that retained functionality were over 100 km from the epicenter, constructed on shallow stiff soil sites. 3 hospitals that lost functionality were over 100 km from the epicenter, but were on deep soft soil sites. 4 hospitals that lost functionality were closer than 100 km from the epicenter, and were on rock or firm soil sites.
3. Hospital Functionality Is Required by Law and Code
Worldwide, codes and laws require new hospitals to be constructed to be functional after earthquakes (
Figure 11). California was the first government to pass a law that required hospitals to be constructed to remain functional after an earthquake. California’s 1972 Seismic Safety Law states that all new hospitals must be constructed to be “completely functional” after a “major earthquake”. By 2002, the World Health Organization [
8] had formally issued their directives for Safe Hospitals, specifying that all new hospitals be constructed to function at maximum capacity after earthquakes [
8,
17]. The current ASCE 7 and International Building Code specify that all essential facilities must be constructed to be functional after earthquakes. These structure codes also specify prescriptive ductile structures for collapse avoidance, but these ductile structures should never be implemented for hospitals or essential facilities. There are no structure types specified in the structure design codes for retaining post-earthquake functionality. To retain the
functionality of hospitals after earthquakes, the
American Seismic Isolator Standard “SIS” must be implemented together with the applicable structure design code. The SIS is the only construction standard that specifies criteria for retaining the functionality of facilities after earthquakes. Constructing hospitals as ductile structures results in lives lost. Yet, 95% of new hospitals are still being designed as ductile moment resisting frames, which is against the law!
The average of the median floor spectra accelerations is then calculated, representing the average demand experienced by the architectural components and contents for all stories. The structure deformation parameters that correlates best with building damage is using both average story drift and maximum story drift. For the 4 design example facilities, damage was calculated to be less than 2%, when the average median floor spectra accelerations was less than 0.3 g; and the story drift was less than 0.3%.
Figure 11.
Specifications, codes, and laws mandating hospital functionality.
Figure 11.
Specifications, codes, and laws mandating hospital functionality.
Figure 12.
The Seismic Isolator Standard “SIS”.
Figure 12.
The Seismic Isolator Standard “SIS”.
From 30 years of observing which hospitals retained functionality, and which hospitals lost functionality, it was observed that when damage was less than 2% the hospital retained functionality, and when damage exceeded 2% most hospitals lost functionality [
2,
3]. The effectiveness of the SIS to retain functionality after earthquakes has been proven by the 100% functionality of 18 essential structures in 8 major earthquakes. To retain functionality, the SIS is specified as the product standard for the seismic isolators, and as the seismic design standard for the structure. Over 4 million square meters of hospitals have implemented SIS pendulum isolators, designed to retain functionality of the facility being protected. Implementing SIS isolators in hospitals has been simple and economical. The construction costs were on average about the same as for building special moment frames without isolators. The
Seismic Isolator Standard “
SIS” (
Figure 12) specifies functionality design criteria that limit building damage to less than 2% of replacement costs, and thus reliably retaining functionality after earthquakes [
1]. The greatest impediment to implementing functionality has been to convince the structural engineers to implement SIS structures instead of the ductile moment frames which take less time and cost less to engineer.
5. Implementing Seismic Isolators without the SIS Is Dangerous
The SIS results in structures that are: not damaged by severe earthquakes; retain 100% post-earthquake functionality; have initial structure construction costs less than that of special ductile moment frames; and save many lives by enabling post-earthquake emergency services. The Seismic Isolator Standard “SIS” specifies the isolator tests that assure reliable and safe isolators: Qualification Tests; Capacity Tests; Dynamic Property Tests; and Quality Control Tests. For all structural members, compliance with an adequate product standard is critical to structural safety. Isolators can protect against earthquake damage, or they can cause a structure collapse, depending on which isolator product standard is implemented. Thousands of isolators that did not comply with the SIS have failed during earthquakes, including the collapses of isolators during two earthquakes [
11]. Hundreds of other isolators have resulted in more earthquake damage than structures built without isolators [
14,
30]. Seismic isolators should never be implemented using the seismic design procedures specified in codes developed to avoid the collapse of ductile structures.
EN15129 is the European product standard for seismic isolators [
30]. During Turkey’s 2023 earthquakes several seismically isolated hospital buildings with EN15129 isolators suffered extensive damage because the polyethylene liners stuck to the concave surfaces [
31]. Those buildings suffered more damage than they would have if isolators had not been used. The seismic design load of the structures had been reduced expecting that the isolators would reduce the seismic forces, but the seismic forces were not reduced, because the isolators stuck to the concave surfaces. Dynamic heating in seismic isolators during earthquake shaking causes a softening of the polyethylene material, which increases the sticking. Adhesion to the mating surfaces has been a known problem of polyethylene materials for decades [
32]. Yet, the use of polyethylene liners in EN15129 isolators has continued because of their low costs. These failures of the isolators to reduce the seismic forces was the direct result of the unreliable isolator materials permitted under the EN15129 isolator product standard.
Christchurch Women’s Hospital was constructed with rubber isolators designed for compliance with New Zealand’s structure code. Building accelerations and displacements were recorded during two 2011 Magnitude 6 earthquakes. Canterbury University reported that the rubber isolators did not displace, and the “structure responded as if it was fixed base” [
14]. Fletcher Construction Company was paid to repair the earthquake damage, which took 4 years. Fletcher reported the repair costs exceeded 30% of the building replacement cost. Rubber isolators are typically too stiff to retain functionality. Recognizing that the rubber isolators in the Christchurch Women’s Hospital were completely ineffective for avoiding damage, Wellington’s Children’s Hospitals used the much more flexible SIS compliant Triple Pendulum Isolators with 3 times the displacement capacity.
Another problem with EN isolators is the collapse hazard. When EN15129 isolators are installed at the tops of columns, they can cause a total structure pancake collapse, because the entire building will fall one story, once the isolator’s sliding displacement capacity is exceeded. Then all other stories will also collapse. (Figs. Dangerous EN15129 Isolators) Turkey’s 1999 magnitude 7.2 earthquake caused the European seismic isolators to slide past their displacement capacities, resulting in the near total collapse of 2.5 km of elevated highway [
12]. The bridge girders of the Trans European Motorway ended up not being supported by the bridge piers. The repair costs were equal to the original construction costs. The near total collapse of this highway was the direct result of implementing a dangerous European isolation system, instead of SIS isolators. Over 2500 seismic isolation system components sold by European companies suffered structural failure. All the European isolation system components were removed and replaced with SIS pendulum isolators. Rubber isolators designed for structure code compliance also suffered collapse during Japan’s 2011 earthquake [
13].
Thousands of isolator failures have shown that seismic isolators can either avoid damage, or cause damage and collapse, depending on which isolator product standard is specified. The dangers of implementing isolators not compliant with the SIS have been extensive and well documented.
Failed Trans-European Motorway, Turkey (
Figure 13). The European seismic isolators and supplemental dampers suffered collapse during a magnitude 7 earthquake. Earthquake damage repair costs were equal to 100% of the original construction costs. All 2500 components of the European isolation system were removed and replaced with SIS compliant pendulum isolators. The SIS pendulum isolators had 4 times the displacement capacity and shear strength, yet cost less to buy than the original price of the European isolation system.
Christchurch Womens’s Hospital, New Zealand, with failed rubber seismic isolators (
Figure 14). Canterbury University reported that the rubber isolators did not displace during 2 magnitude 6 earthquakes, and that the “structure responded as if it was fixed base”. Fletcher Construction Company was paid to repair the earthquake damage, which took 4 years. Fletcher reported the repair costs exceeded 30% of the building replacement cost.
To retain facility functionality, and isolator and structure stability, and it is necessary to specify the American Seismic Isolator Standard “SIS” as the product standard for all isolators. The SIS establishes the long term reliability of the isolator materials, properties, design capacities, factors of safety, and isolator design load limits. ASCE 7 and AASHTO specify the minimum seismic design loads, and do not specify functionality design criteria. The ASCE7, AASHTO, and the Eurocode specify design criteria for avoiding the collapse of isolated structures. The SIS establishes the additional seismic design criteria needed to avoid facility damage, and maintaining functionality. It is the structural product standards that specify the factors of safety required for structural member strength capacities. Despite the Eurocode intention to avoid structure collapse, EN15129 isolators implemented under the Eurocode have resulted in the highest collapse hazards of any new structures constructed during the past 20 years. The SIS requires an isolator shear strength factor of safety of 3.0, which is needed to comply with ASCE 7 and AASHTO Target Reliability for Structural Stability [
11,
33]. The EN15129 shear strength factor of safety is 1.0, which is no factor of safety. EN15129 isolators are dangerous! (
Figure 15 and
Figure 16).
6. SIS Seismic Isolator Technology
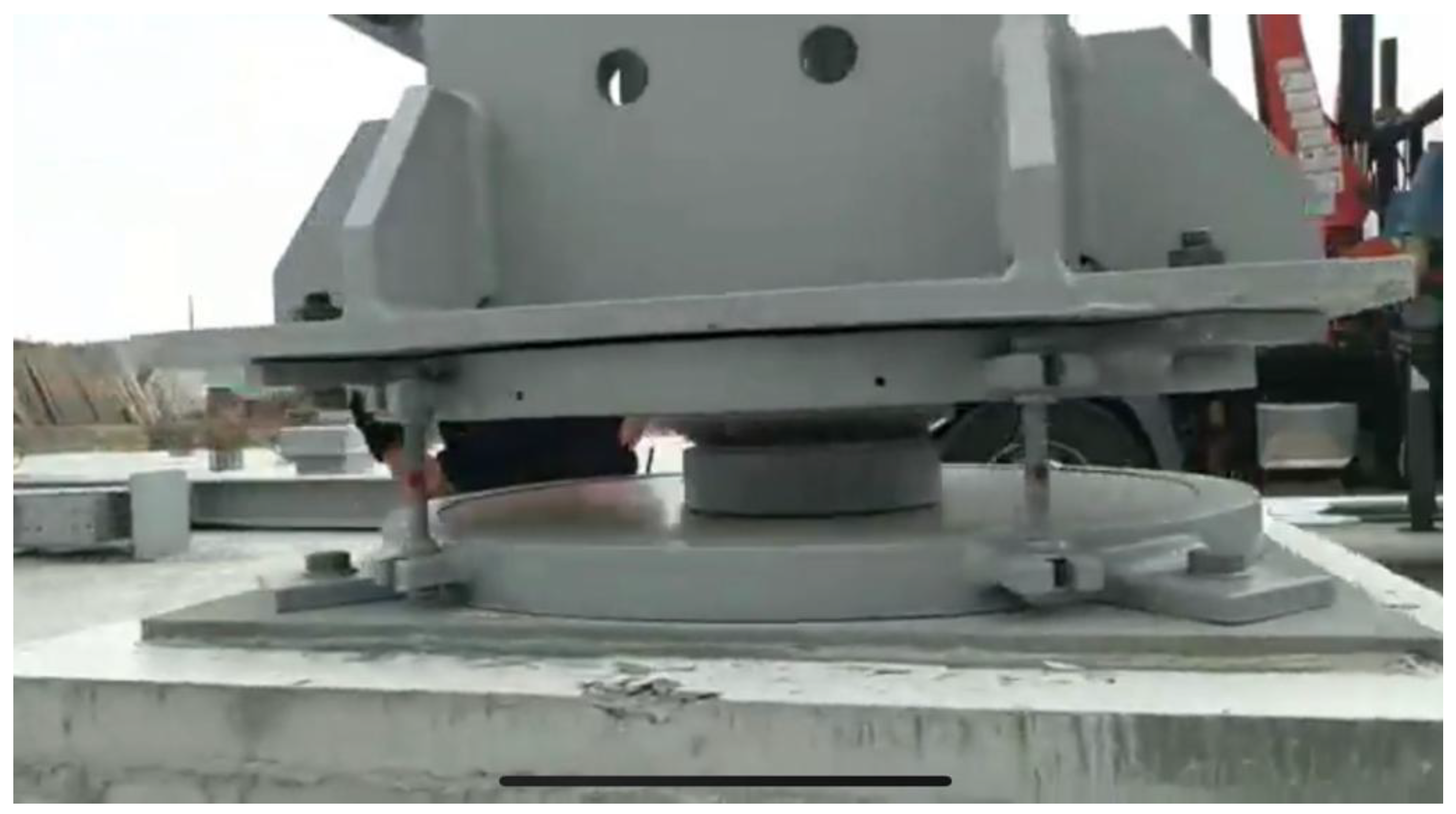
Triple Pendulum Isolators (
Figure 17) were developed to limit in-structure accelerations and deformations to comply with the SIS Functionality Design Criteria. Triple Pendulum Isolators use 4 concave spherical surfaces to absorb the earthquake displacements. Each Triple Pendulum Isolator has 3 independent pendulum mechanisms. The 3 pendulum mechanisms are optimized to minimize: construction costs; earthquake damage; and collapse risks. The first pendulum typically has a friction of less than 0.5%, and a pendulum period less than 2 s, which filters out the high accelerations associated with high frequency earthquake ground motions. The first pendulum protects facility contents and equipment, and architectural components from acceleration related damage. The second pendulum’s period and friction are selected to reduce structure deformations as needed to protect architectural components from deformation related damage. The third pendulum’s period and friction are selected to protect the structure from damage from the Design Earthquake.
The safety retainer rings in SIS isolators protect the structure from collapse for earthquakes stronger than the code Maximum Considered Earthquake. How SIS isolators protect against earthquake damage is illustrated in
Figure 18,
Figure 19,
Figure 20,
Figure 21 and
Figure 22.
Figure 13.
Failed Trans-European Motorway Isolation System.
Figure 13.
Failed Trans-European Motorway Isolation System.
Figure 14.
Christchurch Women’s Hospital with Failed Rubber Isolators.
Figure 14.
Christchurch Women’s Hospital with Failed Rubber Isolators.
Figure 15.
Dangerous EN15129 essentially flat isolator installed in a hospital in Ecuador.
Figure 15.
Dangerous EN15129 essentially flat isolator installed in a hospital in Ecuador.
Figure 16.
Dangerous EN15129 isolators installed on columns in a hospital in Ecuador.
Figure 16.
Dangerous EN15129 isolators installed on columns in a hospital in Ecuador.
Pendulum seismic isolators were developed specifically for maintaining the functionality of facilities after earthquakes [
34,
35]. They result in much lower in-structure accelerations, deformations, and seismic forces than the older “rubber base isolators”. Since 1985, pendulum isolators have been the most widely implemented new structural technology for the construction of buildings, bridges, and industrial facilities. By supporting the weight of a structure on sliders that slide along concave spherical surfaces, the structure responds to earthquakes with small amplitude pendulum motions. Absorbing earthquake displacements in pendulum isolators is far more reliable than absorbing large inelastic deformations within ductile structure members. The world’s largest governments and corporations rely on SIS pendulum isolators to protect their most important assets from earthquake damage [
36].
Figure 17.
Triple Pendulum Isolators.
Figure 17.
Triple Pendulum Isolators.
Figure 18.
Code-designed structures designed for collapse avoidance.
Figure 18.
Code-designed structures designed for collapse avoidance.
Figure 19.
SIS structure designed for functionality.
Figure 19.
SIS structure designed for functionality.
Figure 20.
Seismic isolator sizes and force loops.
Figure 20.
Seismic isolator sizes and force loops.
Figure 21.
Triple pendulum isolator.
Figure 21.
Triple pendulum isolator.
Figure 22.
SIS Building damage estimate curves.
Figure 22.
SIS Building damage estimate curves.
Leading structural engineers worldwide have implemented SIS pendulum isolators in 40 million square meters of important structures [
36]. Selected examples showing the breath of applications of SIS are shown in the photographs. Design examples for implementing SIS isolators for specific facilities are provided in the references authored by Zayas [
27,
28,
29]. The average initial construction cost of implementing the SIS isolators in these applications was about the same as constructing ductile moment resisting frames designed according to the structure codes for only collapse avoidance. Special considerations for implementing SIS isolators in hospitals were summarized by Vallenas [
37]. The life-cycle cost-benefits of implementing SIS isolators to avoid earthquake damage are reported in the reference by Terzic, Merrifield, and Mahin [
38].
In 1989, SIS pendulum seismic isolators protected the Emergency Fire and Cooling Water Tank at the DOW Chemical Plant from damage during California’ magnitude 6.9 earthquake. Constructed on similar soft bay muds, a major highway structure in nearby Oakland, and part of the San Francisco-Oakland Bay Bridge collapsed. Consequentially, in 1982 the US Federal Court in San Francisco was retrofitted with these pendulum isolators [
10]. Over 3 decades of implementations have proven that pendulum isolators, implemented according to the Seismic Isolator Standard, “SIS”, are a practical and economical means of avoiding earthquake damage.
Structure codes worldwide specify minimum seismic design loads that limit collapse risks to “acceptable levels”. ASCE 7 limits collapse risks for ordinary structures to 10%, and for essential facilities to 2.5%. Structure codes avoid collapse by specifying ductile structure types that remain stable when deformed to 20 times their elastic deformation limits. Absorbing earthquake displacements and energy in inelastic member deformations causes structural damage. Currently, there are no structure codes that specify seismic design criteria for avoiding damage and maintaining post-earthquake functionality. To construct structures that retain functionality after earthquakes, it is necessary to implement the Seismic Isolator Standard. Implementing the SIS avoids damage by absorbing the earthquake displacements and energy in the seismic isolators. It has been conclusively proven that structures with SIS isolators perform more reliably, avoid damage, and cost less to build, as compared to special ductile moment frame structures.
Structures with isolators should not be designed according to the structure codes without specifying the American Seismic Isolator Standard, SIS. The prescriptive ductile structure types specified in ASCE 7 were developed in the 1970s for collapse avoidance. Now having SIS technology available, the seismic performance objective should be functionality. ASCE 7 Chapter 17 specifies the isolator design displacement and design shear to deliver the same reliability against structure collapse as is achieved by the Chapter 12 ductile structures. The same structure drift of 2% apply to Chapter 17 isolated structures, and Chapter 12 ductile structures. The Chapter 17 structure drift limits of 2% are 6.7 times greater than the SIS drift limit of 0.3%. Chapter 17 does not specify any limits on in-structure accelerations. It is not possible to retain the functionality of facilities without limiting the in-structure accelerations. As compared to Chapter 17 designed isolators, SIS compliant pendulum isolators have 1/2 the lateral stiffness and damping for the Functionality Level Earthquakes; and 3 to 8 times the shear strength to resist the commonly occurring earthquakes that are much stronger that the Maximum Considered Earthquakes.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




































