

Orthostasis Is Impaired Due to Fatiguing Intensive Acute Concentric Exercise Succeeded by Isometric Weight-Loaded Wall-Sit in Delayed-Onset Muscle Soreness: A Pilot Study
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
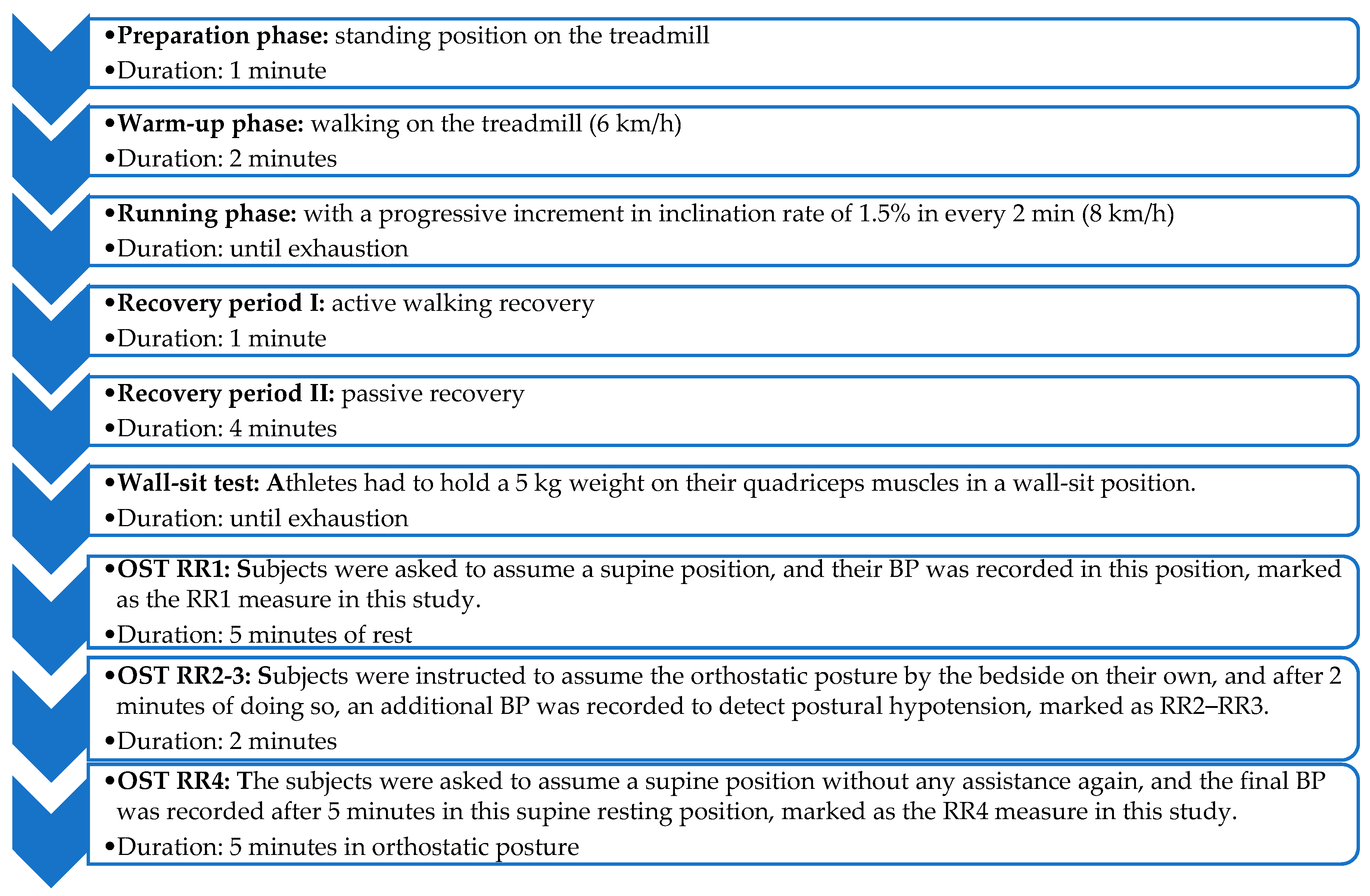
2.3. Procedures
2.3.1. Sports Cardiology Screening with Wall-Sit Test
2.3.2. Orthostatic Stress Test
2.4. Statistical Tests
3. Results
3.1. Orthostatic Hypotension
3.2. VAS Survey
3.3. Decreased Diastolic BP in DOMS
3.4. Dysregulated HR in DOMS
3.5. Substantial Drop in HR in Sustained Standing Position in Some DOMS Subjects
3.6. Self-Reported Dizziness
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cheung, K.; Hume, P.; Maxwell, L. Delayed onset muscle soreness: Treatment strategies and performance factors. Sports Med. 2003, 33, 145–164. [Google Scholar] [CrossRef]
- Clarkson, P.M.; Nosaka, K.; Braun, B. Muscle function after exercise-induced muscle damage and rapid adaptation. Med. Sci. Sports Exerc. 1992, 24, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Sonkodi, B.; Kopa, Z.; Nyirady, P. Post Orgasmic Illness Syndrome (POIS) and Delayed Onset Muscle Soreness (DOMS): Do They Have Anything in Common? Cells 2021, 10, 1867. [Google Scholar] [CrossRef] [PubMed]
- Sonkodi, B. Delayed Onset Muscle Soreness and Critical Neural Microdamage-Derived Neuroinflammation. Biomolecules 2022, 12, 1207. [Google Scholar] [CrossRef] [PubMed]
- Sonkodi, B.; Hegedűs, Á.; Kopper, B.; Berkes, I. Significantly Delayed Medium-Latency Response of the Stretch Reflex in Delayed-Onset Muscle Soreness of the Quadriceps Femoris Muscles Is Indicative of Sensory Neuronal Microdamage. J. Funct. Morphol. Kinesiol. 2022, 7, 43. [Google Scholar] [CrossRef]
- Sonkodi, B. Delayed Onset Muscle Soreness (DOMS): The Repeated Bout Effect and Chemotherapy-Induced Axonopathy May Help Explain the Dying-Back Mechanism in Amyotrophic Lateral Sclerosis and Other Neurodegenerative Diseases. Brain Sci. 2021, 11, 108. [Google Scholar] [CrossRef]
- De Burgh Daly, M. A method for eliciting baroreceptor reflexes from the isolated carotid sinus. J. Physiol. 1955, 128, 33-5P. [Google Scholar]
- De Daly, M.B.; Luck, C.P. The effects of carotid sinus baroreceptor reflexes on pulmonary arterial pressure and pulmonary blood flow in the dog. J. Physiol. 1958, 143, 343–368. [Google Scholar] [CrossRef]
- Zeng, W.Z.; Marshall, K.L.; Min, S.; Daou, I.; Chapleau, M.W.; Abboud, F.M.; Liberles, S.D.; Patapoutian, A. PIEZOs mediate neuronal sensing of blood pressure and the baroreceptor reflex. Science 2018, 362, 464–467. [Google Scholar] [CrossRef]
- Min, S.; Chang, R.B.; Prescott, S.L.; Beeler, B.; Joshi, N.R.; Strochlic, D.E.; Liberles, S.D. Arterial Baroreceptors Sense Blood Pressure through Decorated Aortic Claws. Cell Rep. 2019, 29, 2192–2201.e2193. [Google Scholar] [CrossRef]
- Molina, G.E.; da Cruz, C.J.G.; Fontana, K.E.; Soares, E.; Porto, L.G.G.; Junqueira, L.F., Jr. Post-exercise heart rate recovery and its speed are associated with cardiac autonomic responsiveness following orthostatic stress test in men. Scand Cardiovasc. J. 2021, 55, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Edwards, J.J.; Deenmamode, A.H.P.; Griffiths, M.; Arnold, O.; Cooper, N.J.; Wiles, J.D.; O’Driscoll, J.M. Exercise training and resting blood pressure: A large-scale pairwise and network meta-analysis of randomised controlled trials. Br. J. Sports Med. 2023, 57, 1317–1326. [Google Scholar] [CrossRef] [PubMed]
- Cashman, C.R.; Hoke, A. Mechanisms of distal axonal degeneration in peripheral neuropathies. Neurosci. Lett. 2015, 596, 33–50. [Google Scholar] [CrossRef]
- Sundkvist, G.; Lilja, B.; Almer, L.O. Abnormal diastolic blood pressure and heart rate reactions to tilting in diabetes mellitus. Diabetologia 1980, 19, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Thompson, K.J.; Watson, S.; Zanato, C.; Dall’Angelo, S.; De Nooij, J.C.; Pace-Bonello, B.; Shenton, F.C.; Sanger, H.E.; Heinz, B.A.; Broad, L.M.; et al. The atypical ‘hippocampal’ glutamate receptor coupled to phospholipase D that controls stretch-sensitivity in primary mechanosensory nerve endings is homomeric purely metabotropic GluK2. Exp. Physiol. 2023, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Abarkan, M.; Gaitan, J.; Lebreton, F.; Perrier, R.; Jaffredo, M.; Mulle, C.; Magnan, C.; Raoux, M.; Lang, J. The glutamate receptor GluK2 contributes to the regulation of glucose homeostasis and its deterioration during aging. Mol. Metab. 2019, 30, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Brice, N.L.; Varadi, A.; Ashcroft, S.J.; Molnar, E. Metabotropic glutamate and GABA(B) receptors contribute to the modulation of glucose-stimulated insulin secretion in pancreatic beta cells. Diabetologia 2002, 45, 242–252. [Google Scholar] [CrossRef]
- Ye, Y.; Barghouth, M.; Dou, H.; Luan, C.; Wang, Y.; Karagiannopoulos, A.; Jiang, X.; Krus, U.; Fex, M.; Zhang, Q.; et al. A critical role of the mechanosensor PIEZO1 in glucose-induced insulin secretion in pancreatic beta-cells. Nat. Commun. 2022, 13, 4237. [Google Scholar] [CrossRef]
- Sonkodi, B.; Pállinger, É.; Radovits, T.; Csulak, E.; Shenker-Horváth, K.; Kopper, B.; Buzás, E.I.; Sydó, N.; Merkely, B. CD3+/CD56+ NKT-like Cells Show Imbalanced Control Immediately after Exercise in Delayed-Onset Muscle Soreness. Int. J. Mol. Sci. 2022, 23, 11117. [Google Scholar] [CrossRef]
- Brignole, M.; Moya, A.; de Lange, F.J.; Deharo, J.C.; Elliott, P.M.; Fanciulli, A.; Fedorowski, A.; Furlan, R.; Kenny, R.A.; Martin, A.; et al. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur. Heart J. 2018, 39, 1883–1948. [Google Scholar] [CrossRef]
- Saltin, B.; Blomqvist, G.; Mitchell, J.H.; Johnson, R.L., Jr.; Wildenthal, K.; Chapman, C.B. Response to exercise after bed rest and after training. Circulation 1968, 38, VII1–VII78. [Google Scholar] [PubMed]
- el-Sayed, H.; Hainsworth, R. Relationship between plasma volume, carotid baroreceptor sensitivity and orthostatic tolerance. Clin. Sci. 1995, 88, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Mtinangi, B.L.; Hainsworth, R. Effects of moderate exercise training on plasma volume, baroreceptor sensitivity and orthostatic tolerance in healthy subjects. Exp. Physiol. 1999, 84, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Faucherre, A.; Kissa, K.; Nargeot, J.; Mangoni, M.E.; Jopling, C. Piezo1 plays a role in erythrocyte volume homeostasis. Haematologica 2014, 99, 70–75. [Google Scholar] [CrossRef]
- Uchida, T.; Shimizu, S.; Yamagishi, R.; Tokuoka, S.M.; Kita, Y.; Honjo, M.; Aihara, M. Mechanical stretch induces Ca(2+) influx and extracellular release of PGE(2) through Piezo1 activation in trabecular meshwork cells. Sci. Rep. 2021, 11, 4044. [Google Scholar] [CrossRef]
- Komka, Z.; Szilagyi, B.; Molnar, D.; Sipos, B.; Toth, M.; Sonkodi, B.; Acs, P.; Elek, J.; Szasz, M. Exercise-related hemoconcentration and hemodilution in hydrated and dehydrated athletes: An observational study of the Hungarian canoeists. PLoS ONE 2022, 17, e0277978. [Google Scholar] [CrossRef]
- Sonkodi, B.; Resch, M.D.; Hortobágyi, T. Is the Sex Difference a Clue to the Pathomechanism of Dry Eye Disease? Watch out for the NGF-TrkA-Piezo2 Signaling Axis and the Piezo2 Channelopathy. J. Mol. Neurosci. 2022, 72, 1598–1608. [Google Scholar] [CrossRef]
- Issurin, V.B. New horizons for the methodology and physiology of training periodization. Sports Med. 2010, 40, 189–206. [Google Scholar] [CrossRef]
- Stanley, J.; Peake, J.M.; Buchheit, M. Cardiac parasympathetic reactivation following exercise: Implications for training prescription. Sports Med. 2013, 43, 1259–1277. [Google Scholar] [CrossRef]
- Sonkodi, B.; Bardoni, R.; Hangody, L.; Radák, Z.; Berkes, I. Does Compression Sensory Axonopathy in the Proximal Tibia Contribute to Noncontact Anterior Cruciate Ligament Injury in a Causative Way?—A New Theory for the Injury Mechanism. Life 2021, 11, 443. [Google Scholar] [CrossRef]
- Mason, S. Lactate Shuttles in Neuroenergetics-Homeostasis, Allostasis and Beyond. Front. Neurosci. 2017, 11, 43. [Google Scholar] [CrossRef] [PubMed]
- Bompa, T.O.; Haff, G. Periodization: Theory and Methodology of Training, 5th ed.; Human Kinetics: Champaign, IL, USA, 2009. [Google Scholar]
- Sonkodi, B.; Berkes, I.; Koltai, E. Have We Looked in the Wrong Direction for More Than 100 Years? Delayed Onset Muscle Soreness Is, in Fact, Neural Microdamage Rather Than Muscle Damage. Antioxidants 2020, 9, 212. [Google Scholar] [CrossRef]
- Sonkodi, B. LF Power of HRV Could Be the Piezo2 Activity Level in Baroreceptors with Some Piezo1 Residual Activity Contribution. Int. J. Mol. Sci. 2023, 24, 7038. [Google Scholar] [CrossRef] [PubMed]
- Abboud, F.M. Four evolving concepts in molecular and clinical autonomic research. Clin. Auton. Res. 2021, 31, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Rode, B.; Shi, J.; Endesh, N.; Drinkhill, M.J.; Webster, P.J.; Lotteau, S.J.; Bailey, M.A.; Yuldasheva, N.Y.; Ludlow, M.J.; Cubbon, R.M.; et al. Piezo1 channels sense whole body physical activity to reset cardiovascular homeostasis and enhance performance. Nat. Commun. 2017, 8, 350. [Google Scholar] [CrossRef]
- Ellefsen, K.L.; Holt, J.R.; Chang, A.C.; Nourse, J.L.; Arulmoli, J.; Mekhdjian, A.H.; Abuwarda, H.; Tombola, F.; Flanagan, L.A.; Dunn, A.R.; et al. Myosin-II mediated traction forces evoke localized Piezo1-dependent Ca(2+) flickers. Commun. Biol. 2019, 2, 298. [Google Scholar] [CrossRef] [PubMed]
- Liang, D.; Xue, Z.; Xue, J.; Xie, D.; Xiong, K.; Zhou, H.; Zhang, F.; Su, X.; Wang, G.; Zou, Q.; et al. Sinoatrial node pacemaker cells share dominant biological properties with glutamatergic neurons. Protein. Cell 2021, 12, 545–556. [Google Scholar] [CrossRef]
- Aziz, Q.; Li, Y.; Tinker, A. Potassium channels in the sinoatrial node and their role in heart rate control. Channels 2018, 12, 356–366. [Google Scholar] [CrossRef]
- Mangoni, M.E.; Couette, B.; Bourinet, E.; Platzer, J.; Reimer, D.; Striessnig, J.; Nargeot, J. Functional role of L-type Cav1.3 Ca2+ channels in cardiac pacemaker activity. Proc. Natl. Acad. Sci. USA 2003, 100, 5543–5548. [Google Scholar] [CrossRef]
- Espino, C.M.; Lewis, C.M.; Ortiz, S.; Dalal, M.S.; Garlapalli, S.; Wells, K.M.; O’Neil, D.A.; Wilkinson, K.A.; Griffith, T.N. Na(V)1.1 is essential for proprioceptive signaling and motor behaviors. Elife 2022, 11, e79917. [Google Scholar] [CrossRef]
- Lei, M.; Jones, S.A.; Liu, J.; Lancaster, M.K.; Fung, S.S.; Dobrzynski, H.; Camelliti, P.; Maier, S.K.; Noble, D.; Boyett, M.R. Requirement of neuronal- and cardiac-type sodium channels for murine sinoatrial node pacemaking. J. Physiol. 2004, 559, 835–848. [Google Scholar] [CrossRef] [PubMed]
- Nagy, Z.F.; Sonkodi, B.; Pal, M.; Klivenyi, P.; Szell, M. Likely Pathogenic Variants of Ca(v)1.3 and Na(v)1.1 Encoding Genes in Amyotrophic Lateral Sclerosis Could Elucidate the Dysregulated Pain Pathways. Biomedicines 2023, 11, 933. [Google Scholar] [CrossRef] [PubMed]
- Louradour, J.; Bortolotti, O.; Torre, E.; Bidaud, I.; Lamb, N.; Fernandez, A.; Le Guennec, J.Y.; Mangoni, M.E.; Mesirca, P. L-Type Ca(v)1.3 Calcium Channels Are Required for Beta-Adrenergic Triggered Automaticity in Dormant Mouse Sinoatrial Pacemaker Cells. Cells 2022, 11, 1114. [Google Scholar] [CrossRef] [PubMed]
- Sonkodi, B. Miswired Proprioception in Amyotrophic Lateral Sclerosis in Relation to Pain Sensation (and in Delayed Onset Muscle Soreness)—Is Piezo2 Channelopathy a Principal Transcription Activator in Proprioceptive Terminals Besides Being the Potential Primary Damage? Life 2023, 13, 657. [Google Scholar] [PubMed]
- Lin, H.Y.; Huang, R.C. Glycolytic metabolism and activation of Na(+) pumping contribute to extracellular acidification in the central clock of the suprachiasmatic nucleus: Differential glucose sensitivity and utilization between oxidative and non-oxidative glycolytic pathways. Biomed. J. 2022, 45, 143–154. [Google Scholar] [CrossRef]
- Sonkodi, B. Should We Void Lactate in the Pathophysiology of Delayed Onset Muscle Soreness? Not So Fast! Let’s See a Neurocentric View! Metabolites 2022, 12, 857. [Google Scholar] [CrossRef] [PubMed]
- Yagi, J.; Wenk, H.N.; Naves, L.A.; McCleskey, E.W. Sustained currents through ASIC3 ion channels at the modest pH changes that occur during myocardial ischemia. Circ. Res. 2006, 99, 501–509. [Google Scholar] [CrossRef]


{kind=link}
| With DOMS (n = 16) | Without DOMS (n = 3) | |
|---|---|---|
| Age (years) | 16.8 ± 2.9 | 15.3 ± 2.1 |
| Female (n,%) | 8 (50%) | 2 (67%) |
| Training (hours/week) | 21.1 ± 2.2 | 18.7 ± 2.3 |
| Training history (years) | 11.9 ± 3.5 | 10.3 ± 1.2 |
| Last training before exam (h) | 28.5 ± 18.2 | 13.7 ± 8.5 |
| Last training length (min) | 103.8 ± 39.8 | 110.0 ± 45.8 |
| Wall-sit time (s) | 119.2 ± 44.0 | 169.4 ± 39.0 |
| Muscle fever pre-exercise (VAS 1 1–10) | 1.7 ± 2.1 | - |
| Muscle fever post-exercise 1st day (VAS 1 1–10) | 3.8 ± 2.3 | - |
| Muscle fever post-exercise 2nd day (VAS 1 1–10) | 3.5 ± 2.3 | - |
| Load time (min) | 13.4 ± 1.0 | 13.2 ± 1.6 |
| Peak lactate (mmol/L) | 10.1 ± 2.7 | 11.6 ± 1.4 |
| Restitution lactate (mmol/L) | 9.6 ± 2.9 | 9.4 ± 1.9 |
| VO2 max 2 male (mL/kg/min) | 58.0 ± 1.8 | 59.6 ± 0 |
| VO2 max 2 female (mL/kg/min) | 52.9 ± 3.1 | 50.1 ± 2.5 |
| VO2 max 2 (mL/kg/min) | 55.5 ± 3.6 | 53.3 ± 5.8 |
| Volume consumption (mL) | 500.0 ± 316.2 | 733.3 ± 251.7 |
| RR1 1 | RR2 2 | RR3 3 | RR4 4 | |
|---|---|---|---|---|
| Systolic BP (mmHg) average | 156.1 a | 111.2 a | 113.1 b | 129.9 b |
| SD | 14.6 | 22.1 | 17.6 | 13.3 |
| RR1 | RR2 | RR3 | RR4 | |
|---|---|---|---|---|
| Diastolic BP (mmHg) average | 80.7 | 75.8 | 72.1 | 73.6 |
| SD | 9.7 | 18.1 | 12.4 | 11.2 |
| HR Absolute Statistical Variability | ||||
|---|---|---|---|---|
| With DOMS | Without DOMS | |||
| HR3 1 | HR4 2 | HR3 1 | HR4 2 | |
| Average | 16.4 a | 12.7 b | 2.6 a | 0.4 b |
| SD | 11.2 | 21.1 | 1.5 | 0.2 |
| Subjects Experiencing DOMS, with Substantially Lower HR3 than HR1 | ||
|---|---|---|
| HR1 1 | HR3 2 | |
| Subject 1 | 143 | 74 |
| Subject 2 | 109 | 74 |
| Subject 3 | 119 | 79 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sonkodi, B.; Radovits, T.; Csulak, E.; Kopper, B.; Sydó, N.; Merkely, B. Orthostasis Is Impaired Due to Fatiguing Intensive Acute Concentric Exercise Succeeded by Isometric Weight-Loaded Wall-Sit in Delayed-Onset Muscle Soreness: A Pilot Study. Sports 2023, 11, 209. https://doi.org/10.3390/sports11110209
Sonkodi B, Radovits T, Csulak E, Kopper B, Sydó N, Merkely B. Orthostasis Is Impaired Due to Fatiguing Intensive Acute Concentric Exercise Succeeded by Isometric Weight-Loaded Wall-Sit in Delayed-Onset Muscle Soreness: A Pilot Study. Sports. 2023; 11(11):209. https://doi.org/10.3390/sports11110209
Chicago/Turabian StyleSonkodi, Balázs, Tamás Radovits, Emese Csulak, Bence Kopper, Nóra Sydó, and Béla Merkely. 2023. "Orthostasis Is Impaired Due to Fatiguing Intensive Acute Concentric Exercise Succeeded by Isometric Weight-Loaded Wall-Sit in Delayed-Onset Muscle Soreness: A Pilot Study" Sports 11, no. 11: 209. https://doi.org/10.3390/sports11110209