

Exploring an Unknown Corner of a Well-Known Topic: HIIE Influence on Renal Health and Filtration in Healthy Individuals Free of Cardiometabolic Diseases
 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject Enrollment and Demographics
2.2. Ethical Approval
2.3. Baseline Physiological Assessment
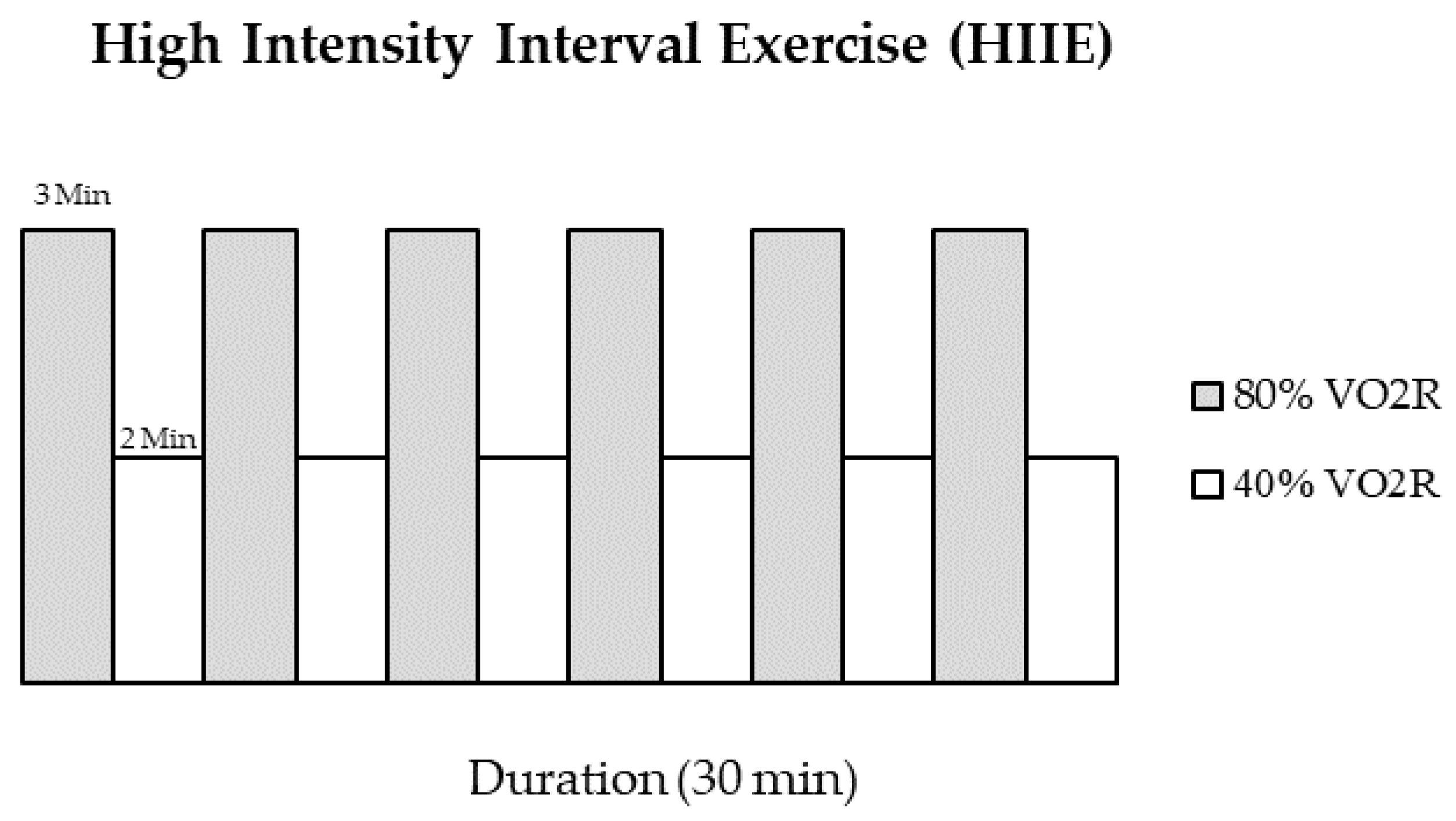
2.4. HIIE Exercise Protocol
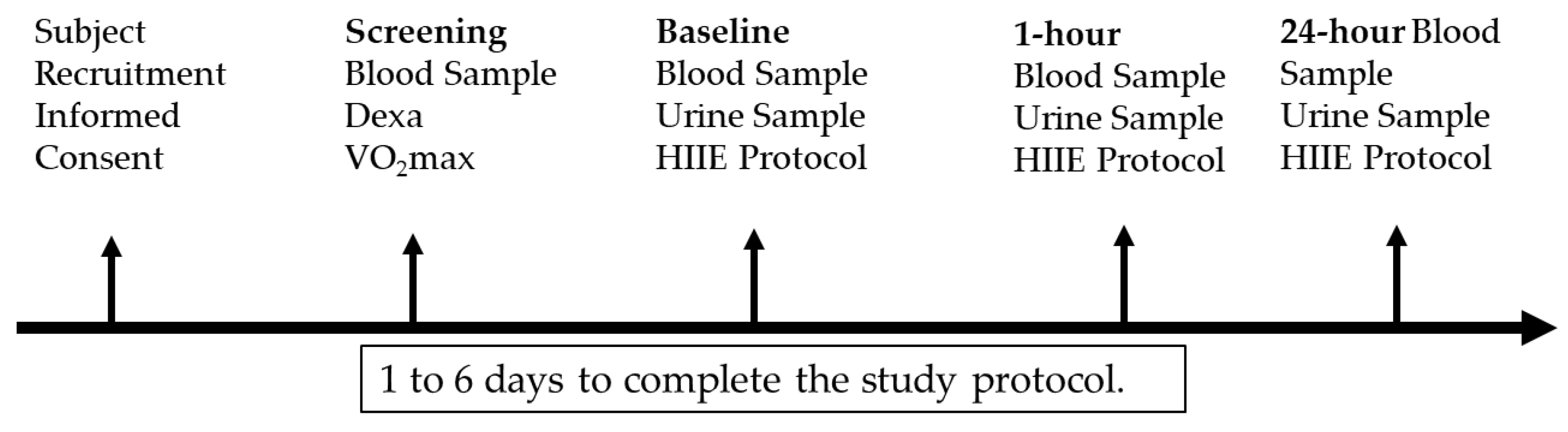
2.5. Specimen Collection
2.6. Biochemical Analysis
2.7. Statistics
3. Results
Renal Biomarker Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Forsse, J.S.; Papadakis, Z.; Peterson, M.N.; Taylor, J.K.; Hess, B.W.; Schwedock, N.; Allison, D.C.; Griggs, J.O.; Wilson, R.L.; Grandjean, P.W. The Influence of an Acute Bout of Aerobic Exercise on Vascular Endothelial Function in Moderate Stages of Chronic Kidney Disease. Life 2022, 12, 91. [Google Scholar] [CrossRef]
- Chapman-Lopez, T.J.; Taylor, J.K.; Torres, R.; Wilburn, D.; Funderburk, L.K.; Allison, D.C.; Forsse, J.S. The Effects of Acute Bouts of Aerobic Exercise on Adipokine Concentrations in Individuals with Moderate Stages of Chronic Kidney Disease. Physiologia 2023, 3, 522–530. [Google Scholar] [CrossRef]
- Forsse, J.S.; Buckley, D.; Ismaeel, A.; Adair, K.; Torres, R.; Lowry, C.; Dhillon, A.; Koutakis, P. In the absence of cardiometabolic diseases, is age an independent factor in assessing renal health and filtration? A pilot study. J. Nephropathol. 2021. [Google Scholar] [CrossRef]
- Forsse, J.S.; Buckley, D.; Ismaeel, A.; Richardson, K.A.; Oliver, A.; Koutakis, P. Effect of Age and Acute-Moderate Intensity Exercise on Biomarkers of Renal Health and Filtration. Biology 2022, 11, 527. [Google Scholar] [CrossRef]
- Adair, K.E.; Ylitalo, K.R.; Forsse, J.S.; Funderburk, L.K.; Bowden, R.G. Metabolic Constellations, Clusters, and Renal Function: Findings from the 2013–2018 National Health and Nutrition Examination Surveys. Life 2021, 11, 904. [Google Scholar] [CrossRef]
- Lindeman, R.D.; Tobin, J.; Shock, N.W. Longitudinal Studies on the Rate of Decline in Renal Function with Age. J. Am. Geriatr. Soc. 1985, 33, 278–285. [Google Scholar] [CrossRef]
- Frassetto, L.A.; Morris, R.C.; Sebastian, A. Effect of age on blood acid-base composition in adult humans: Role of age-related renal functional decline. Am. J. Physiol. Ren. Physiol. 1996, 271, F1114–F1122. [Google Scholar] [CrossRef]
- Adair, K.E.; Bowden, R.G.; Funderburk, L.K.; Forsse, J.S.; Ylitalo, K.R. Metabolic Health, Obesity, and Renal Function: 2013–2018 National Health and Nutrition Examination Surveys. Life 2021, 11, 888. [Google Scholar] [CrossRef]
- Saran, A.M.; DuBose, T.D. Cardiovascular disease in chronic kidney disease. Ther. Adv. Cardiovasc. Dis. 2008, 2, 425–434. [Google Scholar] [CrossRef]
- Baylis, C. Nitric oxide deficiency in chronic kidney disease. Am. J. Physiol. Ren. Physiol. 2008, 294, F1–F9. [Google Scholar] [CrossRef]
- Papadakis, Z.; Grandjean, P.W.; Forsse, J.S. Effects of Acute Exercise on Cardiac Autonomic Response and Recovery in Non-Dialysis Chronic Kidney Disease Patients. Res. Q. Exerc. Sport 2023, 94, 812–825. [Google Scholar] [CrossRef] [PubMed]
- Hebert, L.A.; Parikh, S.; Prosek, J.; Nadasdy, T.; Rovin, B.H. Differential Diagnosis of Glomerular Disease: A Systematic and Inclusive Approach. Am. J. Nephrol. 2013, 38, 253–266. [Google Scholar] [CrossRef] [PubMed]
- Wasung, M.E.; Chawla, L.S.; Madero, M. Biomarkers of renal function, which and when? Clin. Chim. Acta 2015, 438, 350–357. [Google Scholar] [CrossRef]
- Delanaye, P.; Cavalier, E.; Moranne, O.; Lutteri, L.; Krzesinski, J.-M.; Bruyère, O. Creatinine-or cystatin C-based equations to estimate glomerular filtration in the general population: Impact on the epidemiology of chronic kidney disease. BMC Nephrol. 2013, 14, 57. [Google Scholar] [CrossRef] [PubMed]
- Chertow, G.; Luyckx, V.; Marsden, P.; Skorecki, K.; Taal, M.; Yu, A. Brenner and Rector’s The Kidney. In Brenner and Rector’s the Kidney; Elsevier: Philadelphia, PA, USA, 2019; p. 2793. ISBN 978-0-323-55085-7. [Google Scholar]
- Adair, K.E.; Heileson, J.L.; Peterson, M.N.; Bowden, R.G.; Forsse, J.S. A Nutritional Assessment Stage 3 Chronic Kidney Disease. Int. J. Dis. Reversal Prev. 2021, 3, e17224. [Google Scholar] [CrossRef]
- Greenwood, S.A.; Koufaki, P.; Mercer, T.H.; MacLaughlin, H.L.; Rush, R.; Lindup, H.; O’Connor, E.; Jones, C.; Hendry, B.M.; Macdougall, I.C.; et al. Effect of Exercise Training on Estimated GFR, Vascular Health, and Cardiorespiratory Fitness in Patients with CKD: A Pilot Randomized Controlled Trial. Am. J. Kidney Dis. 2015, 65, 425–434. [Google Scholar] [CrossRef]
- Odutayo, A.; Cherney, D. Cystatin C and acute changes in glomerular filtration rate. Clin. Nephrol. 2012, 78, 64–75. [Google Scholar] [CrossRef]
- Poussel, M.; Touzé, C.; Allado, E.; Frimat, L.; Hily, O.; Thilly, N.; Rousseau, H.; Vauthier, J.-C.; Chenuel, B. Ultramarathon and Renal Function: Does Exercise-Induced Acute Kidney Injury Really Exist in Common Conditions? Front. Sports Act. Living 2020, 1, 71. [Google Scholar] [CrossRef]
- Shlipak, M.G.; Sarnak, M.J.; Katz, R.; Fried, L.F.; Seliger, S.L.; Newman, A.B.; Siscovick, D.S.; Stehman-Breen, C. Cystatin C and the Risk of Death and Cardiovascular Events among Elderly Persons. N. Engl. J. Med. 2005, 352, 2049–2060. [Google Scholar] [CrossRef]
- Ebert, N.; Shlipak, M.G. Cystatin C is ready for clinical use. Curr. Opin. Nephrol. Hypertens. 2020, 29, 591–598. [Google Scholar] [CrossRef]
- Aybay, C.; Karakus, R.; Yucel, A. Characterization of human epidermal growth factor in human serum and urine under native conditions. Cytokine 2006, 35, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Harskamp, L.R.; Gansevoort, R.T.; van Goor, H.; Meijer, E. The epidermal growth factor receptor pathway in chronic kidney diseases. Nat. Rev. Nephrol. 2016, 12, 496–506. [Google Scholar] [CrossRef] [PubMed]
- Ju, W.; Nair, V.; Smith, S.; Zhu, L.; Shedden, K.; Song, P.X.K.; Mariani, L.H.; Eichinger, F.H.; Berthier, C.C.; Randolph, A.; et al. Tissue transcriptome-driven identification of epidermal growth factor as a chronic kidney disease biomarker. Sci. Transl. Med. 2015, 7, 316ra193. [Google Scholar] [CrossRef] [PubMed]
- Forsse, J.S.; Peterson, M.; Papadakis, Z.; Taylor, J.K.; Hess, B.W.; Schwedock, N.; Allison, C.D.; Griggs, J.O.; Wilson, R.L.; Grandjean, P.W. The Effect of Acute Aerobic Exercise on Biomarkers of Renal Health and Filtration in Moderate-CKD. Res. Q. Exerc. Sport 2023, 1–9. [Google Scholar] [CrossRef]
- Calzavacca, P.; May, C.N.; Bellomo, R. Glomerular haemodynamics, the renal sympathetic nervous system and sepsis-induced acute kidney injury. Nephrol. Dial. Transplant. 2014, 29, 2178–2184. [Google Scholar] [CrossRef]
- Riebe, D.; Franklin, B.A.; Thompson, P.D.; Garber, C.E.; Whitfield, G.P.; Magal, M.; Pescatello, L.S. Updating ACSM’s Recommendations for Exercise Preparticipation Health Screening. Med. Sci. Sports Exerc. 2015, 47, 2473–2479. [Google Scholar] [CrossRef]
- Papadakis, Z.; Forsse, J.S.; Stamatis, A. High-Intensity Interval Exercise Performance and Short-Term Metabolic Responses to Overnight-Fasted Acute-Partial Sleep Deprivation. Int. J. Environ. Res Public Health 2021, 17, 3655. [Google Scholar] [CrossRef]
- Torres, R.; Richardson, K.; Lowry, C.; Beeson, C.; Ismaeel, A.; Koutakis, P.; Forsse, J. The Influence of an Acute Bout of High-Intensity Interval Exercise on Heart Rate Variability Indices and Stress Index in the Absence of Cardiometabolic Diseases. Res. Directs Health Sci. 2022, 2, 5. [Google Scholar] [CrossRef]
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. 2002, 39 (Suppl. S1), S1–S266. [Google Scholar]
- Stevens, L.A.; Levey, A.S. Measured GFR as a Confirmatory Test for Estimated GFR. J. Am. Soc. Nephrol. 2009, 20, 2305–2313. [Google Scholar] [CrossRef]
- Virvidakis, C.; Loukas, A.; Mayopoulou-Symvoulidou, D.; Mountokalakis, T. Renal Responses to Bicycle Exercise in Trained Athletes: Influence of Exercise Intensity. Int. J. Sports Med. 1986, 7, 86–88. [Google Scholar] [CrossRef] [PubMed]
- Hiraki, K.; Kamijo-Ikemori, A.; Yasuda, T.; Hotta, C.; Izawa, K.P.; Watanabe, S.; Sugaya, T.; Kimura, K. Moderate-Intensity Single Exercise Session Does Not Induce Renal Damage. J. Clin. Lab. Anal. 2013, 27, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Neumayr, G.; Pfister, R.; Hoertnagl, H.; Mitterbauer, G.; Getzner, W.; Ulmer, H.; Gaenzer, H.; Joannidis, M. The Effect of Marathon Cycling on Renal Function. Int. J. Sports Med. 2003, 24, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Dharnidharka, V.R.; Kwon, C.; Stevens, G. Serum cystatin C is superior to serum creatinine as a marker of kidney function: A meta-analysis. Am. J. Kidney Dis. 2002, 40, 221–226. [Google Scholar] [CrossRef]
- Bongers, C.C.W.G.; Alsady, M.; Nijenhuis, T.; Hartman, Y.A.W.; Eijsvogels, T.M.H.; Deen, P.M.T.; Hopman, M.T.E. Impact of acute versus repetitive moderate intensity endurance exercise on kidney injury markers. Physiol. Rep. 2017, 5, e13544. [Google Scholar] [CrossRef]
- Baxmann, A.C.; Ahmed, M.S.; Marques, N.C.; Menon, V.B.; Pereira, A.B.; Kirsztajn, G.M.; Heilberg, I.P. Influence of Muscle Mass and Physical Activity on Serum and Urinary Creatinine and Serum Cystatin C. Clin. J. Am. Soc. Nephrol. CJASN 2008, 3, 348–354. [Google Scholar] [CrossRef]
- Bongers, C.C.W.G.; Alsady, M.; Nijenhuis, T.; Tulp, A.D.M.; Eijsvogels, T.M.H.; Deen, P.M.T.; Hopman, M.T.E. Impact of acute versus prolonged exercise and dehydration on kidney function and injury. Physiol. Rep. 2018, 6, e13734. [Google Scholar] [CrossRef]
- Konradsen, L.; Nexø, E. Epidermal growth factor in plasma, serum and urine before and after prolonged exercise. Regul. Pept. 1988, 21, 197–203. [Google Scholar] [CrossRef]
- Irving, R.A.; Noakes, T.D.; Irving, G.A.; Van Zyl-Smit, R. The immediate and delayed effects of marathon running on renal function. J. Urol. 1986, 136, 1176–1180. [Google Scholar] [CrossRef]
- Wade, C.E.; Dressendorfer, R.H.; O’Brien, J.C.; Claybaugh, J.R. Renal function, aldosterone, and vasopressin excretion following repeated long-distance running. J. Appl. Physiol. 1981, 50, 709–712. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Mean | SD |
|---|---|---|
| Age (yrs) | 37.6 | 12.4 |
| Height (cm) | 172.8 | 9.4 |
| Weight (kg) | 73.3 | 15.3 |
| Body Fat Percentage (BF%) (%) | 19.2 | 7.1 |
| Systolic Blood Pressure (SBP) (mmHg) | 119.9 | 6.9 |
| Diastolic Blood Pressure (DBP) (mmHg) | 77.1 | 5.9 |
| Resting Heart Rate (HR) (beats per min) | 60.0 | 11.5 |
| Exercise HR (beats per min) | 177.5 | 18.2 |
| VO2max (mL/kg/min−1) | 41.8 | 7.4 |
| Glucose (mg/dL) | 95.0 | 6.5 |
| Total Cholesterol (Chol) (mg/dL) | 178.1 | 32.4 |
| HDL (mg/dL) | 58.5 | 13.7 |
| LDL (mg/dL) | 102.6 | 26.9 |
| Albumin (g/dL) | 4.7 | 0.2 |
| Variables | Baseline | 1-h | 24-h |
|---|---|---|---|
| sCr (mg/dL) | 0.93 ± 0.15 | 0.97 ± 0.17 | 0.92 ± 0.15 |
| sCr MDRD | 84.88 ± 16.09 | 81.13 ± 16.05 | 86.31 ± 17.35 |
| sCr CKD-EPI | 97.02 ± 30.83 | 92.94 ± 30.57 | 95.81 ± 26.76 |
| eGFR CyC | 115.17 ± 52.6 | 111.97 ± 51.49 | 114.81 ± 47.1 |
| eGFR sCr/CyC | 104.4 ± 28.03 | 100.3 ± 26 | 102.75 ± 26.9 |
| uCr (mg/dL) | 212.51 ± 103.24 | 187.78 ± 117.2 | 230.13 ± 124.67 |
| CyC (mg/dL) | 873.9 ± 415.34 | 896.81 ± 443.23 | 862.44 ± 423.59 |
| uEGF (pg/mL) | 31,874.94 ± 19,457.88 | 34,973.52 ± 50,846.85 | 33,904.31 ± 21,158 |
| uEGF/uCr (ng/mL)/(mg/dL) | 15.23 ± 7.52 | 19.9 ± 31.55 | 15.26 ± 7.04 |
| Log2 (uEGF/uCr) | 1.33 ± 0.46 | 1.4 ± 0.84 | 1.34 ± 0.43 |
| Variable | Pre- and 1 h | 1 h & 24 h | Pre- & 24 h | Effect of Time | Effect of Age | Age * Time Interaction | ES 1 h | ES 24 h |
|---|---|---|---|---|---|---|---|---|
| sCr | 0.0024 * | <0.0001 * | 0.2385 | 0.0002 * | 0.8022 | 0.6074 | −0.24 | 0.15 |
| sCr MDRD | 0.0031 * | 0.0033 * | 0.4522 | 0.0062 * | 0.0532 | 0.6028 | 0.23 | −0.08 |
| sCr CKD-EPI | 0.0122 * | 0.5559 | 0.8114 | 0.5919 | 0.6028 | 0.1775 | 0.13 | 0.04 |
| CyC (eGFR) | 0.5741 | 0.5874 | 0.9382 | 0.7892 | 0.4607 | 0.1323 | 0.06 | 0.007 |
| sCr/CyC (eGFR) | 0.0067 * | 0.3768 | 0.5603 | 0.2421 | 0.0268 * | 0.6225 | 0.15 | 0.06 |
| uCr | 0.2091 | 0.0248 * | 0.3911 | 0.1007 | 0.7973 | 0.9950 | 0.22 | −0.15 |
| CyC | 0.4513 | 0.2425 | 0.6381 | 0.4637 | 0.2478 | 0.6711 | −0.05 | 0.02 |
| uEGF | 0.7584 | 0.8974 | 0.6351 | 0.9279 | 0.2921 | 0.5783 | −0.08 | −0.09 |
| uEGF/uCr | 0.3632 | 0.3747 | 0.9999 | 0.4310 | 0.2176 | 0.3547 | −0.20 | −0.04 |
| Log2 (uEGF/uCr) | 0.6088 | 0.6896 | 0.9324 | 0.8227 | 0.2481 | 0.3192 | −0.10 | −0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forsse, J.S.; Richardson, K.A.; Torres, R.; Lowry, C.; Taylor, J.K.; Beeson, C.L.; Ward, J.; Dhillon, A.; Niceler, B.; Ismaeel, A.; et al. Exploring an Unknown Corner of a Well-Known Topic: HIIE Influence on Renal Health and Filtration in Healthy Individuals Free of Cardiometabolic Diseases. Sports 2023, 11, 210. https://doi.org/10.3390/sports11110210
Forsse JS, Richardson KA, Torres R, Lowry C, Taylor JK, Beeson CL, Ward J, Dhillon A, Niceler B, Ismaeel A, et al. Exploring an Unknown Corner of a Well-Known Topic: HIIE Influence on Renal Health and Filtration in Healthy Individuals Free of Cardiometabolic Diseases. Sports. 2023; 11(11):210. https://doi.org/10.3390/sports11110210
Chicago/Turabian StyleForsse, Jeffrey S., Kathleen A. Richardson, Ricardo Torres, Catherine Lowry, James Kyle Taylor, Cassidy L. Beeson, Jacob Ward, Anurag Dhillon, Brock Niceler, Ahmed Ismaeel, and et al. 2023. "Exploring an Unknown Corner of a Well-Known Topic: HIIE Influence on Renal Health and Filtration in Healthy Individuals Free of Cardiometabolic Diseases" Sports 11, no. 11: 210. https://doi.org/10.3390/sports11110210