A Scientific Overview of Smartphone Applications and Electronic Devices for Weight Management in Adults


{kind=link}
{kind=link}
Abstract
:1. Overweight and Obesity
2. Digital and Mobile (m) Health—Definition
3. Digital and Mobile (m) Health—Quality Assessment
3.1. Development, Evaluation, and Certification
3.2. Data Privacy, Data Reliability, and Expert Involvement
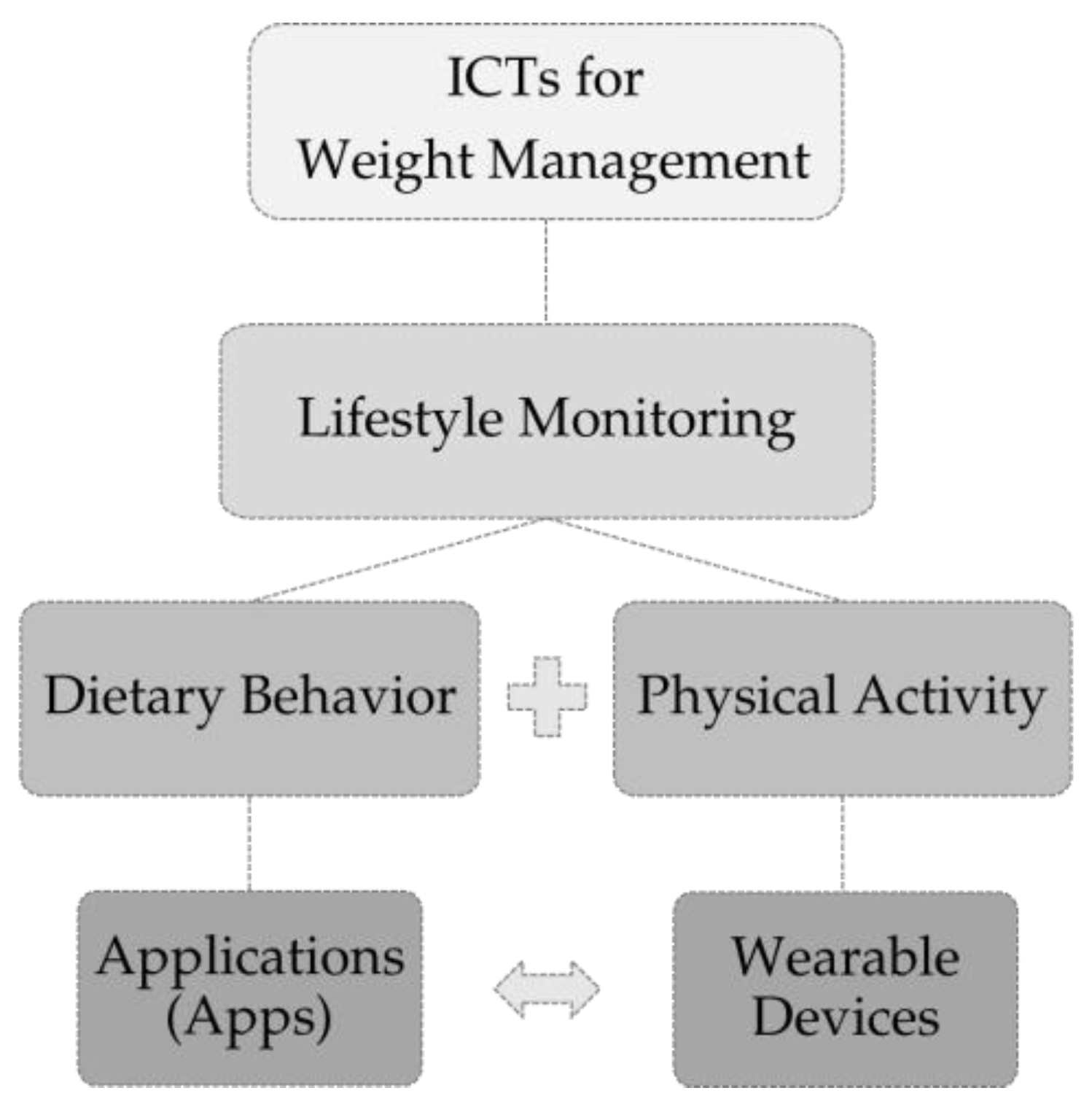
4. Digital Self-Monitoring of Diet and Physical Activity
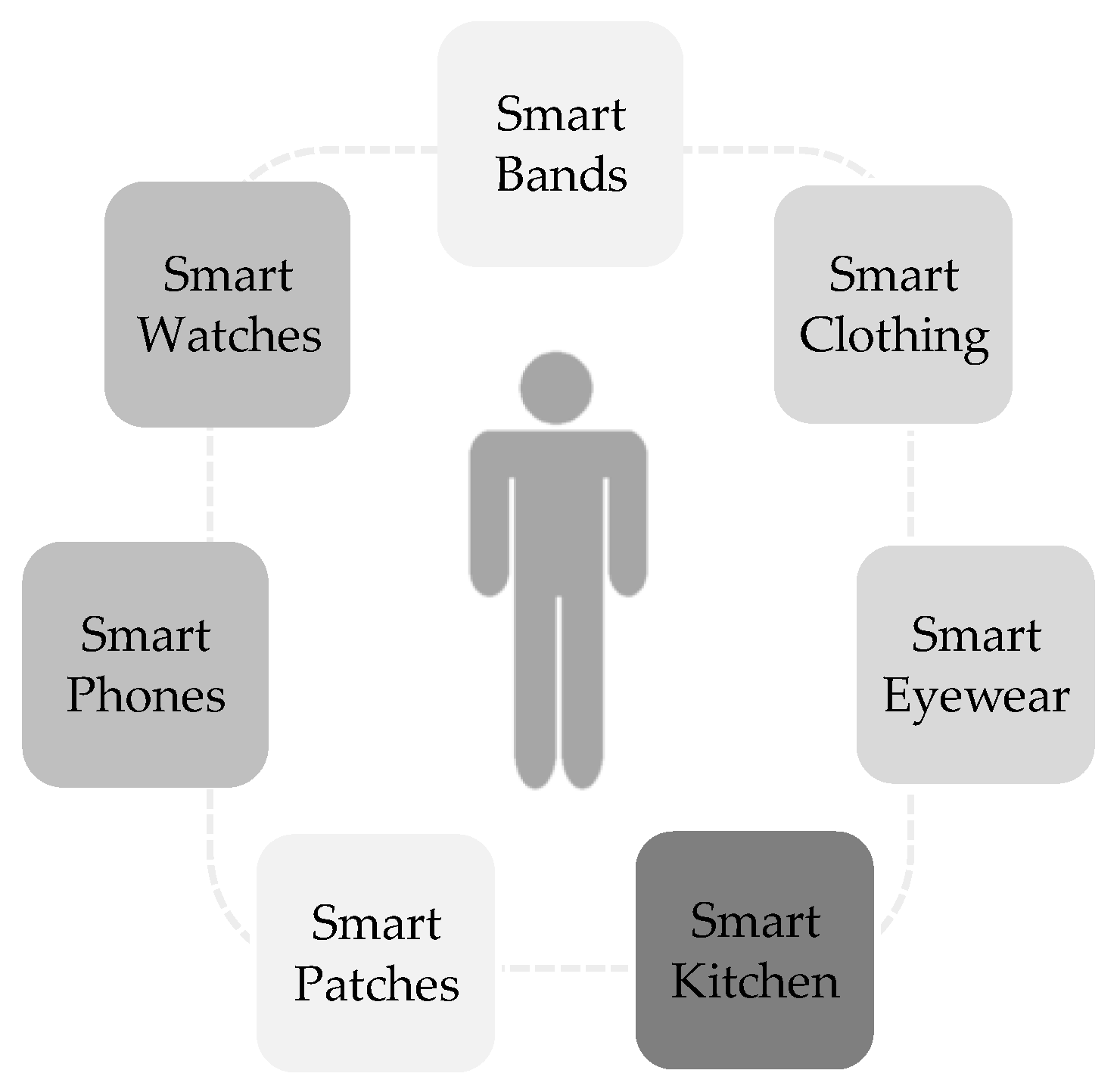
5. Smartphone Applications (Apps) and Wearable Devices (Activity Tracker) for Weight Management
6. Summary and Outlook
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Abarca-Gómez, L.; Abdeen, Z.A.; Hamid, Z.A.; Abu-Rmeileh, N.M.; Acosta-Cazares, B.; Acuin, C.; Adams, R.J.; Aekplakorn, W.; Afsana, K.; Aguilar-Salinas, C.A.; et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Wyatt, S.B.; Winters, K.P.; Dubbert, P.M. Overweight and obesity: Prevalence, consequences, and causes of a growing public health problem. Am. J. Med. Sci. 2006, 331, 166–174. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 22 May 2019).
- Kohl, H.W.; Craig, C.L.; Lambert, E.V.; Inoue, S.; Alkandari, J.R.; Leetongin, G.; Kahlmeier, S. The pandemic of physical inactivity: Global action for public health. Lancet 2012, 380, 294–305. [Google Scholar] [CrossRef]
- Stevens, G.A.; Singh, G.M.; Lu, Y.; Danaei, G.; Lin, J.K.; Finucane, M.M.; Bahalim, A.N.; McIntire, R.K.; Gutierrez, H.R.; Cowan, M.; et al. National, regional, and global trends in adult overweight and obesity prevalences. Popul. Health Metr. 2012, 10, 22. [Google Scholar] [CrossRef]
- Harvey, J.; Krukowski, R.; Priest, J.; West, D. Log Often, Lose More: Electronic Dietary Self-Monitoring for Weight Loss. Obesity (Silver Spring) 2019, 27, 380–384. [Google Scholar] [CrossRef] [Green Version]
- Carroll, J.K.; Moorhead, A.; Bond, R.; LeBlanc, W.G.; Petrella, R.J.; Fiscella, K. Who Uses Mobile Phone Health Apps and Does Use Matter? A Secondary Data Analytics Approach. J. Med. Internet Res. 2017, 19, e125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adjekum, A.; Blasimme, A.; Vayena, E. Elements of Trust in Digital Health Systems: Scoping Review. J. Med. Internet Res. 2018, 20, e11254. [Google Scholar] [CrossRef] [PubMed]
- Davis, T.L.; DiClemente, R.; Prietula, M. Taking mHealth Forward: Examining the Core Characteristics. JMIR Mhealth Uhealth 2016, 4, e97. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. mHealth: New Horizons for Health through Mobile Technologies. Global Observatory for eHealth Series—Volume 3; WHO: Geneva, Switzerland. Available online: http://www.who.int/goe/publications/goe_mhealth_web.pdf (accessed on 22 February 2019).
- Oh, H.; Rizo, C.; Enkin, M.; Jadad, A. What is eHealth (3): A systematic review of published definitions. J. Med. Internet Res. 2005, 7, e1. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. Digital Health. Available online: https://www.fda.gov/medicaldevices/digitalhealth/ (accessed on 21 February 2019).
- Braz, V.N.; Lopes, M.H.B.M. Evaluation of mobile applications related to nutrition. Public Health Nutr. 2018, 1–6. [Google Scholar] [CrossRef]
- Albrecht, U.-V.; Engeli, S.; von Jan, U. Mit Apps durch Dick und Dünn? Adipositas Ursachen Folgeerkrankungen Therapie 2016, 10, 43–50. [Google Scholar] [CrossRef]
- Pagoto, S.; Bennett, G.G. How behavioral science can advance digital health. Transl. Behav. Med. 2013, 3, 271–276. [Google Scholar] [CrossRef] [Green Version]
- Schoffman, D.E.; Turner-McGrievy, G.; Jones, S.J.; Wilcox, S. Mobile apps for pediatric obesity prevention and treatment, healthy eating, and physical activity promotion: Just fun and games? Transl. Behav. Med. 2013, 3, 320–325. [Google Scholar] [CrossRef]
- Chen, J.; Cade, J.E.; Allman-Farinelli, M. The Most Popular Smartphone Apps for Weight Loss: A Quality Assessment. JMIR Mhealth Uhealth 2015, 3, e104. [Google Scholar] [CrossRef] [PubMed]
- Bardus, M.; van Beurden, S.B.; Smith, J.R.; Abraham, C. A review and content analysis of engagement, functionality, aesthetics, information quality, and change techniques in the most popular commercial apps for weight management. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 35. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.; Miron-Shatz, T.; Schumacher, N.; Krocza, J.; Diamantidis, C.; Albrecht, U.-V. mHealth 2.0: Experiences, Possibilities, and Perspectives. JMIR Mhealth Uhealth 2014, 2, e24. [Google Scholar] [CrossRef]
- Holzmann, S.L.; Pröll, K.; Hauner, H.; Holzapfel, C. Nutrition apps: Quality and limitations: An explorative investigation on the basis of selected apps. Ernahrungs Umschau 2018, 80–89. [Google Scholar] [CrossRef]
- Federal Institute for Drugs and Medical Devices. BfArM—Guidance on “Medical Apps”: Differentiation between Apps and Medical or Other Devices as well as on the Subsequent Risk Classification According to the MPG. Available online: https://www.bfarm.de/EN/MedicalDevices/Differentiation/MedicalApps/_node.html (accessed on 22 February 2019).
- European Commission. Green Paper on Mobile Health (“mHealth”). 2014. Available online: Ec.europa.eu/newsroom/dae/document.cfm?doc_id=5147 (accessed on 19 February 2019).
- European Commission. Privacy Code of Conduct on Mobile Health Apps. Available online: https://ec.europa.eu/digital-single-market/en/privacy-code-conduct-mobile-health-apps (accessed on 22 February 2019).
- Agarwal, S.; LeFevre, A.E.; Lee, J.; L’Engle, K.; Mehl, G.; Sinha, C.; Labrique, A. Guidelines for reporting of health interventions using mobile phones: Mobile health (mHealth) evidence reporting and assessment (mERA) checklist. BMJ 2016, 352, i1174. [Google Scholar] [CrossRef] [PubMed]
- Xcertia. Xcertia-mHealth App Guidelines. Available online: https://www.xcertia.org/the-guidelines/ (accessed on 22 February 2019).
- Stoyanov, S.R.; Hides, L.; Kavanagh, D.J.; Zelenko, O.; Tjondronegoro, D.; Mani, M. Mobile app rating scale: A new tool for assessing the quality of health mobile apps. JMIR Mhealth Uhealth 2015, 3, e27. [Google Scholar] [CrossRef]
- DiFilippo, K.N.; Huang, W.; Chapman-Novakofski, K.M. A New Tool for Nutrition App Quality Evaluation (AQEL): Development, Validation, and Reliability Testing. JMIR Mhealth Uhealth 2017, 5, e163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albrecht, U.-V. Transparency of health-apps for trust and decision making. J. Med. Internet Res. 2013, 15, e277. [Google Scholar] [CrossRef]
- Albrecht, U.-V.; Hillebrand, U.; von Jan, U. Relevance of Trust Marks and CE Labels in German-Language Store Descriptions of Health Apps: Analysis. JMIR Mhealth Uhealth 2018, 6, e10394. [Google Scholar] [CrossRef]
- Kramer, U. HealthOn-App Ehrenkodex für Gesundheits-Apps. Available online: https://www.healthon.de/ehrenkodex (accessed on 22 February 2019).
- Düsseldorfer Kreis. Orientierungshilfe zu den Datenschutzanforderungen an App-Entwickler und App-Anbieter. Available online: https://www.baden-wuerttemberg.datenschutz.de/wp-content/uploads/2013/02/OH_Apps_20140616.pdf (accessed on 22 February 2019).
- Zentrum für Telematik und Telemedizin GmbH. AppCheck: Die Informations- und Bewertungsplattform für Gesundheits-Apps. Available online: https://appcheck.de/technische-pruefung/ (accessed on 22 February 2019).
- Fraunhofer-Institut für Offene Kommunikationssysteme. APPKRI Kriterien für Gesundheits-Apps. Available online: https://ehealth-services.fokus.fraunhofer.de/BMG-APPS/impressum (accessed on 22 February 2019).
- Albrecht, U.-V. (Ed.) Chances and Risks of Mobile Health Apps (CHARISMHA). Available online: https://charismha.weebly.com/uploads/7/4/0/7/7407163/charismha_abr_v.01.1e-20160606.pdf (accessed on 22 February 2019).
- Gigerenzer, G.; Schlegel-Matthies, K.; Wagner, G.G. Digitale Welt und Gesundheit. eHealth und mHealth—Chancen und Risiken der Digitalisierung im Gesundheitsbereich. 2016. Available online: http://www.svr-verbraucherfragen.de/dokumente/digitale-welt-und-gesundheit-ehealth-und-mhealth-chancen-und-risiken-der-digitalisierung-im-gesundheitsbereich/ (accessed on 19 February 2019).
- Aktionsbündnis Patientensicherheit e.V. Digitalisierung und Patientensicherheit. Checkliste für die Nutzung von Gesundheits-Apps. 2018. Available online: www.aps-ev.de/wp-content/uploads/2018/05/2018_APS-Checkliste_GesundheitsApps.pdf (accessed on 22 February 2019).
- Knöppler, K.; Neisecke, T.; Nölke, L. Digital-Health-Anwendungen für Bürger. Kontext, Typologie und Relevanz aus Public-Health-Perspektive Entwicklung und Erprobung eines Klassifikationsverfahrens. Available online: https://www.bertelsmann-stiftung.de/fileadmin/files/BSt/Publikationen/GrauePublikationen/Studie_VV_Digital-Health-Anwendungen_2016.pdf (accessed on 19 February 2019).
- Kramer, U. Wie gut sind Gesundheits-Apps? Aktuel Ernahrungsmed 2017, 42, 193–205. [Google Scholar] [CrossRef] [Green Version]
- Weichert, T. Gesundheitsdatenschutz in vernetzten Zeiten. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2018, 61, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Hutton, L.; Price, B.A.; Kelly, R.; McCormick, C.; Bandara, A.K.; Hatzakis, T.; Meadows, M.; Nuseibeh, B. Assessing the Privacy of mHealth Apps for Self-Tracking: Heuristic Evaluation Approach. JMIR Mhealth Uhealth 2018, 6, e185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, G.; Cheung, C.; Nebeker, C.; Bietz, M.; Bloss, C. Privacy Policies for Apps Targeted Toward Youth: Descriptive Analysis of Readability. JMIR Mhealth Uhealth 2018, 6, e3. [Google Scholar] [CrossRef] [Green Version]
- Sunyaev, A.; Dehling, T.; Taylor, P.L.; Mandl, K.D. Availability and quality of mobile health app privacy policies. J. Am. Med. Inform. Assoc. 2015, 22, e28–e33. [Google Scholar] [CrossRef]
- Ellis, D.A.; Piwek, L. Failing to encourage physical activity with wearable technology: What next? J. R. Soc. Med. 2018, 111, 310–313. [Google Scholar] [CrossRef] [PubMed]
- Subhi, Y.; Bube, S.H.; Rolskov Bojsen, S.; Skou Thomsen, A.S.; Konge, L. Expert Involvement and Adherence to Medical Evidence in Medical Mobile Phone Apps: A Systematic Review. JMIR Mhealth Uhealth 2015, 3, e79. [Google Scholar] [CrossRef] [PubMed]
- Nikolaou, C.K.; Lean, M.E.J. Mobile applications for obesity and weight management: Current market characteristics. Int. J. Obes. 2017, 41, 200–202. [Google Scholar] [CrossRef] [PubMed]
- Rivera, J.; McPherson, A.; Hamilton, J.; Birken, C.; Coons, M.; Iyer, S.; Agarwal, A.; Lalloo, C.; Stinson, J. Mobile Apps for Weight Management: A Scoping Review. JMIR Mhealth Uhealth 2016, 4, e87. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, U.-V.; von Jan, U. Safe, sound and desirable: Development of mHealth apps under the stress of rapid life cycles. Mhealth 2017, 3, 27. [Google Scholar] [CrossRef] [PubMed]
- Piwek, L.; Ellis, D.A.; Andrews, S.; Joinson, A. The Rise of Consumer Health Wearables: Promises and Barriers. PLoS Med. 2016, 13, e1001953. [Google Scholar] [CrossRef]
- McClung, H.L.; Ptomey, L.T.; Shook, R.P.; Aggarwal, A.; Gorczyca, A.M.; Sazonov, E.S.; Becofsky, K.; Weiss, R.; Das, S.K. Dietary Intake and Physical Activity Assessment: Current Tools, Techniques, and Technologies for Use in Adult Populations. Am. J. Prev. Med. 2018, 55, e93–e104. [Google Scholar] [CrossRef] [Green Version]
- Roess, A. The Promise, Growth, and Reality of Mobile Health—Another Data-free Zone. N. Engl. J. Med. 2017, 377, 2010–2011. [Google Scholar] [CrossRef] [PubMed]
- Svetkey, L.P.; Batch, B.C.; Lin, P.-H.; Intille, S.S.; Corsino, L.; Tyson, C.C.; Bosworth, H.B.; Grambow, S.C.; Voils, C.; Loria, C.; et al. Cell phone intervention for you (CITY): A randomized, controlled trial of behavioral weight loss intervention for young adults using mobile technology. Obesity (Silver Spring) 2015, 23, 2133–2141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carter, M.C.; Burley, V.J.; Nykjaer, C.; Cade, J.E. Adherence to a smartphone application for weight loss compared to website and paper diary: Pilot randomized controlled trial. J. Med. Internet Res. 2013, 15, e32. [Google Scholar] [CrossRef] [PubMed]
- Thranberend, T.; Knöppler, K.; Neisecke, T. Gesundheits-Apps. Bedeutender Hebel für Patient Empowerment—Potenziale Jedoch Bislang Kaum Genutzt. 2016. Available online: https://www.bertelsmann-stiftung.de/fileadmin/files/BSt/Publikationen/GrauePublikationen/SpotGes_Gesundheits-Apps_dt_final_web.pdf (accessed on 19 February 2019).
- Ernsting, C.; Dombrowski, S.U.; Oedekoven, M.; O Sullivan, J.L.; Kanzler, M.; Kuhlmey, A.; Gellert, P. Using Smartphones and Health Apps to Change and Manage Health Behaviors: A Population-Based Survey. J. Med. Internet Res. 2017, 19, e101. [Google Scholar] [CrossRef]
- Campbell, M. Apple Patent Hints at Non-Invasive Glucose Monitoring Tech for Apple Watch. Available online: https://appleinsider.com/articles/18/08/23/apple-patent-suggests-work-on-non-invasive-glucose-monitoring-tech (accessed on 14 March 2019).
- Khan, S.; Ali, S.; Bermak, A. Recent Developments in Printing Flexible and Wearable Sensing Electronics for Healthcare Applications. Sensors 2019, 19, 1230. [Google Scholar] [CrossRef]
- Fernández-Caramés, T.; Fraga-Lamas, P. Towards the Internet-of-Smart-Clothing: A Review on IoT Wearables and Garments for Creating Intelligent Connected E-Textiles. Electronics 2018, 7, 405. [Google Scholar] [CrossRef]
- Gilmore, L.A.; Duhé, A.F.; Frost, E.A.; Redman, L.M. The technology boom: A new era in obesity management. J. Diabetes Sci. Technol. 2014, 8, 596–608. [Google Scholar] [CrossRef] [PubMed]
- DiFilippo, K.N.; Huang, W.-H.; Andrade, J.E.; Chapman-Novakofski, K.M. The use of mobile apps to improve nutrition outcomes: A systematic literature review. J. Telemed. Telecare 2015, 21, 243–253. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-Martínez, A.; Solé-Sedeño, J.M.; Mancebo-Moreno, G.; Medina, F.X.; Carreras-Collado, R.; Saigí-Rubió, F. Use of mobile phones as a tool for weight loss: A systematic review. J. Telemed. Telecare 2014, 20, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Flores Mateo, G.; Granado-Font, E.; Ferré-Grau, C.; Montaña-Carreras, X. Mobile Phone Apps to Promote Weight Loss and Increase Physical Activity: A Systematic Review and Meta-Analysis. J. Med. Internet Res. 2015, 17, e253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, F.; Kong, X.; Cao, J.; Chen, S.; Li, C.; Huang, J.; Gu, D.; Kelly, T.N. Mobile phone intervention and weight loss among overweight and obese adults: A meta-analysis of randomized controlled trials. Am. J. Epidemiol. 2015, 181, 337–348. [Google Scholar] [CrossRef]
- Stephens, J.; Allen, J. Mobile phone interventions to increase physical activity and reduce weight: A systematic review. J. Cardiovasc. Nurs. 2013, 28, 320–329. [Google Scholar] [CrossRef]
- Schippers, M.; Adam, P.C.G.; Smolenski, D.J.; Wong, H.T.H.; de Wit, J.B.F. A meta-analysis of overall effects of weight loss interventions delivered via mobile phones and effect size differences according to delivery mode, personal contact, and intervention intensity and duration. Obes. Rev. 2017, 18, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-H.; Hwang, J.; Choi, Y.-K. Effect of Mobile Health on Obese Adults: A Systematic Review and Meta-Analysis. Healthc. Inform. Res. 2019, 25, 12–26. [Google Scholar] [CrossRef] [PubMed]
- Marcolino, M.S.; Oliveira, J.A.Q.; D’gostino, M.; Ribeiro, A.L.; Alkmim, M.B.M.; Novillo-Ortiz, D. The Impact of mHealth Interventions: Systematic Review of Systematic Reviews. JMIR Mhealth Uhealth 2018, 6, e23. [Google Scholar] [CrossRef] [Green Version]
- Lin, P.-H.; Grambow, S.; Intille, S.; Gallis, J.A.; Lazenka, T.; Bosworth, H.; Voils, C.L.; Bennett, G.G.; Batch, B.; Allen, J.; et al. The Association Between Engagement and Weight Loss Through Personal Coaching and Cell Phone Interventions in Young Adults: Randomized Controlled Trial. JMIR Mhealth Uhealth 2018, 6, e10471. [Google Scholar] [CrossRef] [Green Version]
- Thomas, J.G.; Bond, D.S.; Raynor, H.A.; Papandonatos, G.D.; Wing, R.R. Comparison of Smartphone-Based Behavioral Obesity Treatment with Gold Standard Group Treatment and Control: A Randomized Trial. Obesity (Silver Spring) 2019. [Google Scholar] [CrossRef]
- Turner-McGrievy, G.M.; Wilcox, S.; Boutté, A.; Hutto, B.E.; Singletary, C.; Muth, E.R.; Hoover, A.W. The Dietary Intervention to Enhance Tracking with Mobile Devices (DIET Mobile) Study: A 6-Month Randomized Weight Loss Trial. Obesity (Silver Spring) 2017, 25, 1336–1342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burke, L.E.; Styn, M.A.; Sereika, S.M.; Conroy, M.B.; Ye, L.; Glanz, K.; Sevick, M.A.; Ewing, L.J. Using mHealth technology to enhance self-monitoring for weight loss: A randomized trial. Am. J. Prev. Med. 2012, 43, 20–26. [Google Scholar] [CrossRef]
- Zheng, Y.; Burke, L.E.; Danford, C.A.; Ewing, L.J.; Terry, M.A.; Sereika, S.M. Patterns of self-weighing behavior and weight change in a weight loss trial. Int. J. Obes. 2016, 40, 1392–1396. [Google Scholar] [CrossRef] [PubMed]
- Romeo, A.; Edney, S.; Plotnikoff, R.; Curtis, R.; Ryan, J.; Sanders, I.; Crozier, A.; Maher, C. Can Smartphone Apps Increase Physical Activity? Systematic Review and Meta-Analysis. J. Med. Internet Res. 2019, 21, e12053. [Google Scholar] [CrossRef]
- Richardson, C.R.; Newton, T.L.; Abraham, J.J.; Sen, A.; Jimbo, M.; Swartz, A.M. A meta-analysis of pedometer-based walking interventions and weight loss. Ann. Fam. Med. 2008, 6, 69–77. [Google Scholar] [CrossRef]
- Bravata, D.M.; Smith-Spangler, C.; Sundaram, V.; Gienger, A.L.; Lin, N.; Lewis, R.; Stave, C.D.; Olkin, I.; Sirard, J.R. Using Pedometers to Increase Physical Activity and Improve Health: A Systematic Review. JAMA 2007, 298, 2296–2304. [Google Scholar] [CrossRef]
- Lewis, Z.H.; Lyons, E.J.; Jarvis, J.M.; Baillargeon, J. Using an electronic activity monitor system as an intervention modality: A systematic review. BMC Public Health 2015, 15, 585. [Google Scholar] [CrossRef] [PubMed]
- Goode, A.P.; Hall, K.S.; Batch, B.C.; Huffman, K.M.; Hastings, S.N.; Allen, K.D.; Shaw, R.J.; Kanach, F.A.; McDuffie, J.R.; Kosinski, A.S.; et al. The Impact of Interventions that Integrate Accelerometers on Physical Activity and Weight Loss: A Systematic Review. Ann. Behav. Med. 2017, 51, 79–93. [Google Scholar] [CrossRef] [PubMed]
- Finkelstein, E.A.; Haaland, B.A.; Bilger, M.; Sahasranaman, A.; Sloan, R.A.; Nang, E.E.K.; Evenson, K.R. Effectiveness of activity trackers with and without incentives to increase physical activity (TRIPPA): A randomised controlled trial. Lancet Diabetes Endocrinol. 2016, 4, 983–995. [Google Scholar] [CrossRef]
- Jakicic, J.M.; Davis, K.K.; Rogers, R.J.; King, W.C.; Marcus, M.D.; Helsel, D.; Rickman, A.D.; Wahed, A.S.; Belle, S.H. Effect of Wearable Technology Combined with a Lifestyle Intervention on Long-term Weight Loss: The IDEA Randomized Clinical Trial. JAMA 2016, 316, 1161–1171. [Google Scholar] [CrossRef] [PubMed]
- Alkhaldi, G.; Hamilton, F.L.; Lau, R.; Webster, R.; Michie, S.; Murray, E. The Effectiveness of Prompts to Promote Engagement with Digital Interventions: A Systematic Review. J. Med. Internet Res. 2016, 18, e6. [Google Scholar] [CrossRef] [PubMed]
- Shaw, R.; Levine, E.; Streicher, M.; Strawbridge, E.; Gierisch, J.; Pendergast, J.; Hale, S.; Reed, S.; McVay, M.; Simmons, D.; et al. Log2Lose: Development and Lessons Learned from a Mobile Technology Weight Loss Intervention. JMIR Mhealth Uhealth 2019, 7, e11972. [Google Scholar] [CrossRef] [PubMed]
- Deutsche Adipositas-Gesellschaft (DAG) e.V.; Deutsche Diabetes Gesellschaft (DDG); Deutsche Gesellschaft für Ernährung (DGE) e.V.; Deutsche Gesellschaft für Ernährungsmedizin (DGEM) e.V. Interdisziplinäre Leitlinie der Qualität S3 zur “Prävention und Therapie der Adipositas”. Available online: https://www.adipositas-gesellschaft.de/fileadmin/PDF/Leitlinien/050-001l_S3_Adipositas_Praevention_Therapie_2014-11.pdf (accessed on 20 May 2019).
- Mazza, D.; McCarthy, E.; Carey, M.; Turner, L.; Harris, M. “90% of the time, it’s not just weight”: General practitioner and practice staff perspectives regarding the barriers and enablers to obesity guideline implementation. Obes. Res. Clin. Pract. 2019. [Google Scholar] [CrossRef] [PubMed]


© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holzmann, S.L.; Holzapfel, C. A Scientific Overview of Smartphone Applications and Electronic Devices for Weight Management in Adults. J. Pers. Med. 2019, 9, 31. https://doi.org/10.3390/jpm9020031
Holzmann SL, Holzapfel C. A Scientific Overview of Smartphone Applications and Electronic Devices for Weight Management in Adults. Journal of Personalized Medicine. 2019; 9(2):31. https://doi.org/10.3390/jpm9020031
Chicago/Turabian StyleHolzmann, Sophie Laura, and Christina Holzapfel. 2019. "A Scientific Overview of Smartphone Applications and Electronic Devices for Weight Management in Adults" Journal of Personalized Medicine 9, no. 2: 31. https://doi.org/10.3390/jpm9020031