Evaluation of the Association of Omentin 1 rs2274907 A>T and rs2274908 G>A Gene Polymorphisms with Coronary Artery Disease in Indian Population: A Case Control Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Criteria for Selection of Patients and Controls
2.2. Inclusion Criteria for Patient Selection
2.3. Exclusion Criteria
2.4. Selection of Healthy Controls
2.5. Collection of Case Histroy and Measurement of Certein Biochemical Parametes that are Related to CAD
2.6. Sample Collection and DNA Extraction
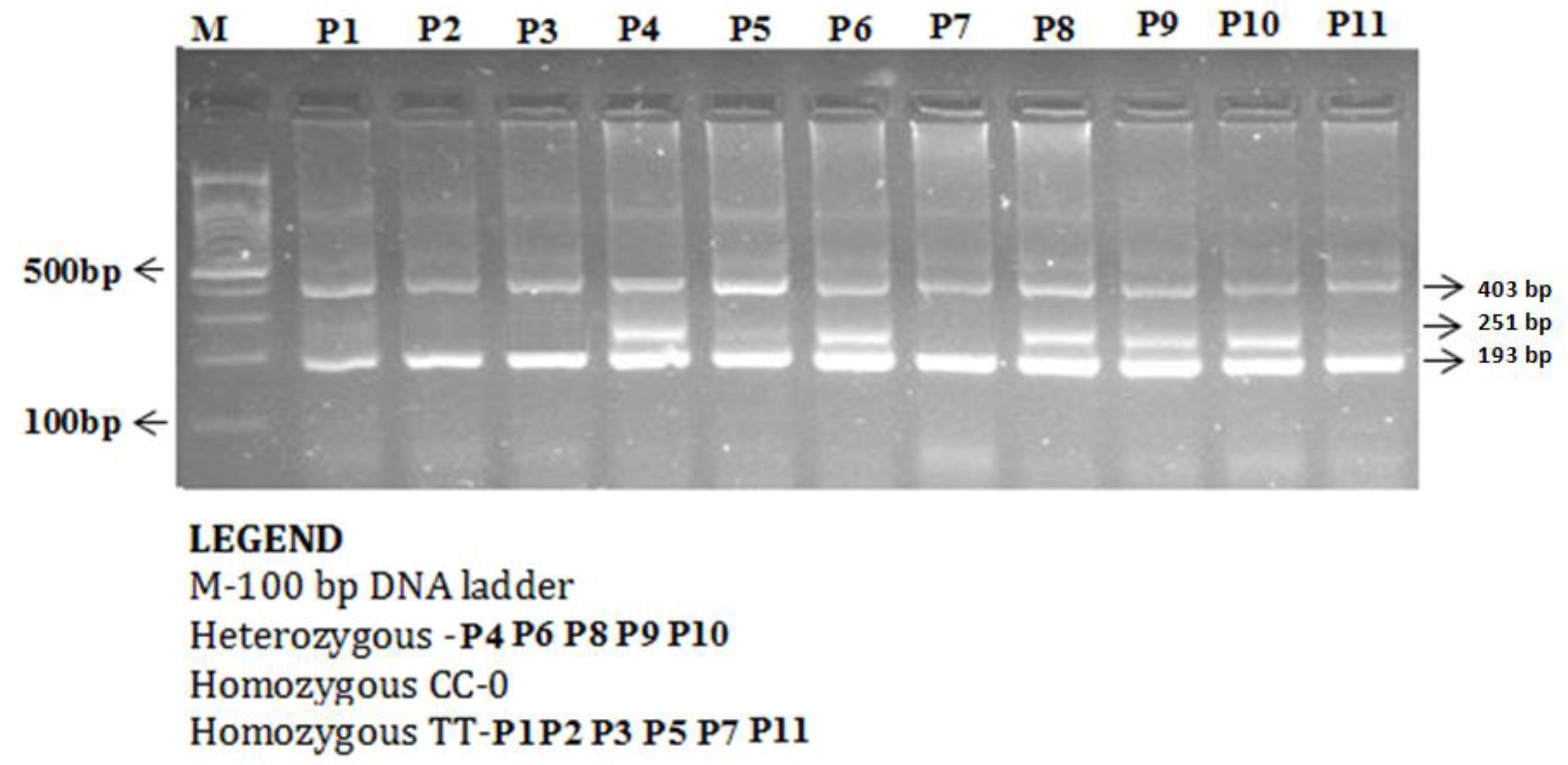
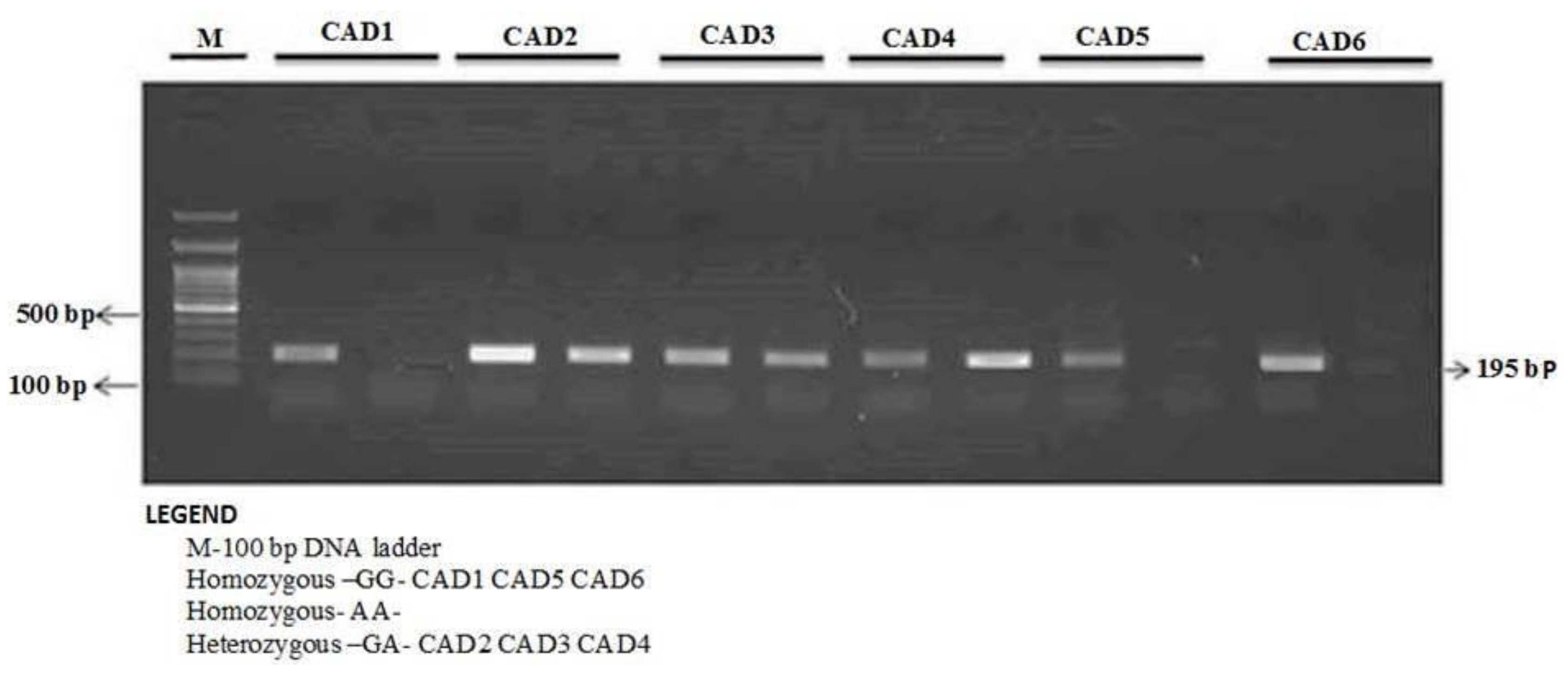
2.7. Detection of ITLN1 rs2274907 A>T rs2274908 G>A Gene Polymorphisms by ARMS-PCR and (AS) PCR
2.8. Statistical Analysis
3. Results
3.1. Baseline Characteristics of CAD Patients and Controls
3.2. The rs2274907 A>T Genotype Distribution in CAD Cases and Controls
3.3. Some Clinical Characteristics of CAD Patients
3.4. Association with Gender and Age
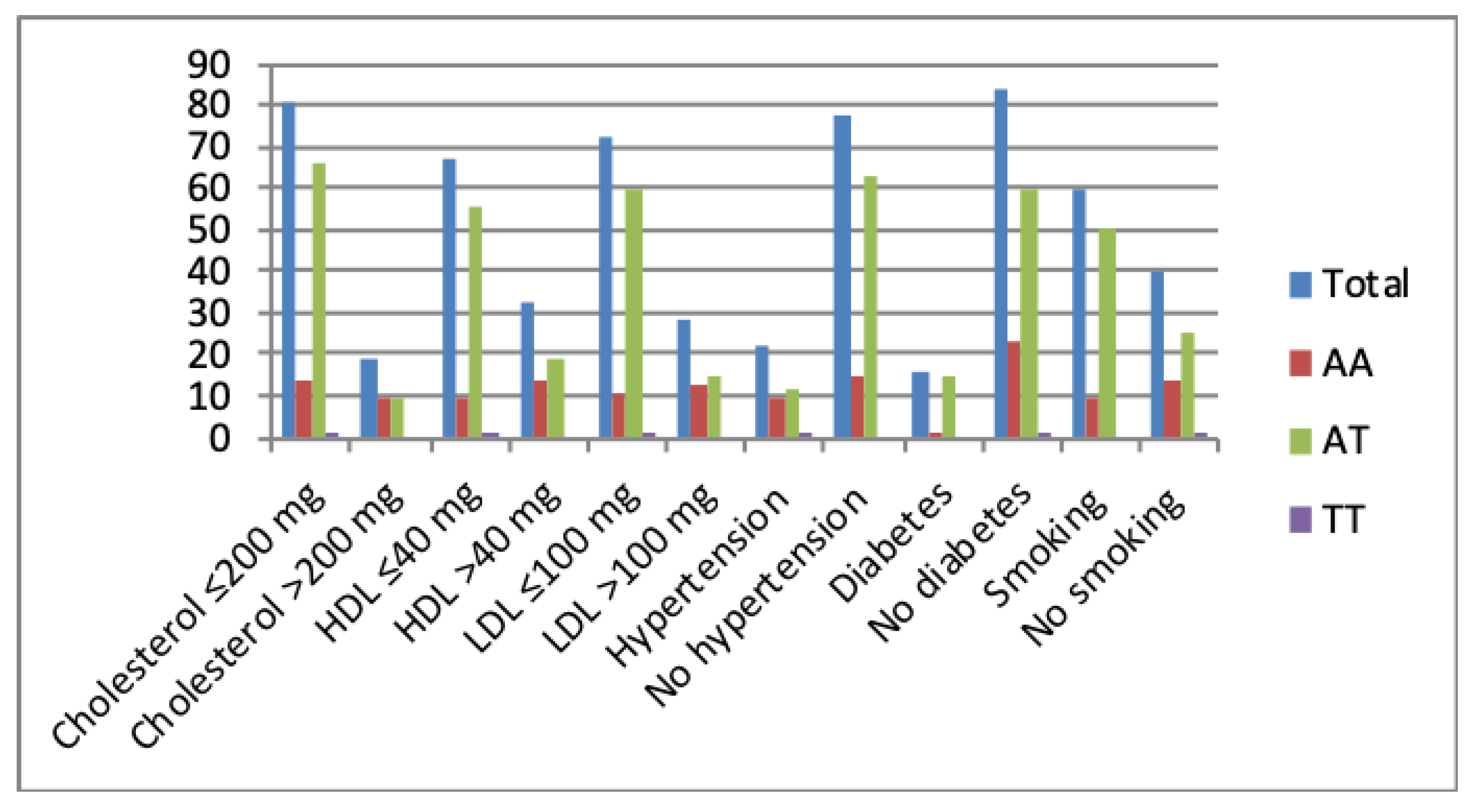
3.5. Correlations with Random Blood Sugar (RBS), Plasma Cholesterol
3.6. Correlation with Hypertension and Diabetes
3.7. Correlation with Smoking and Alcohol Intake
3.8. Association of the rs2274907 A>T Gene Polymorphism with CAD
3.9. The rs2274908 G>A Genotype Distribution in CAD Cases and Controls
3.10. Association of rs2274908 G>A Polymorphism with the Susceptibility to CAD Patients
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Stewart, J.; Manmathan, G.; Wilkinson, P. Primary prevention of cardiovascular disease: A review of contemporary guidance and literature. JRSM Cardiovasc. Dis. 2017, 6, 2048004016687211. [Google Scholar] [CrossRef] [PubMed]
- Prabhakaran, D.; Jeemon, P.; Roy, A. Cardiovascular diseases in India: Current epidemiology and future directions. Circulation 2016, 133, 1605–1620. [Google Scholar] [CrossRef] [PubMed]
- Mendis, S.; Puska, P.; Norrving, B.; World Health Organization. Global Atlas on Cardiovascular Disease Prevention and Control Policies, Strategies and Interventions; World Health Organization: Geneva, Switzerland, 2011; p. 164. [Google Scholar]
- Liao, K.P.; Solomon, D.H. Traditional cardiovascular risk factors, inflammation and cardiovascular risk in rheumatoid arthritis. Rheumatology 2013, 52, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Knowles, J.W.; Ashley, E.A. Cardiovascular disease: The rise of the genetic risk score. PLoS Med. 2018, 15, e1002546. [Google Scholar] [CrossRef] [PubMed]
- Price, A.L.; Spencer, C.C.; Donnelly, P. Progress and promise in understanding the genetic basis of common diseases. Proc. Biol. Sci. 2015, 282, 20151684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elfaki, I.; Almutairi, F.M.; Mir, R.; Khan, R.; Abu-Duhier, F. Cytochrome P450 CYP1B1*2 gene and its association with T2D in Tabuk population, northwestern region of Saudi Arabia. Asian J. Pharm. Clin. Res. 2018, 11, 55–59. [Google Scholar] [CrossRef]
- Elfaki, I.; Mir, R.; Almutairi, F.M.; Duhier, F.M.A. Cytochrome P450: Polymorphisms and roles in cancer, diabetes and atherosclerosis. Asian Pac. J. Cancer Prev. 2018, 19, 2057–2070. [Google Scholar] [PubMed]
- Li, Y.Y.; Zhou, Y.H.; Gong, G.; Geng, H.Y.; Yang, X.X. TGF-beta1 Gene -509C/T polymorphism and coronary artery disease: An updated meta-analysis involving 11,701 subjects. Front Physiol. 2017, 8, 108. [Google Scholar]
- Mir, R.; Jha, C.K.; Elfaki, I.; Rehman, S.; Javid, J.; Khullar, N.; Banu, S.; Chahal, S. MicroRNA-224 (rs188519172 A>G) gene variability is associated with a decreased susceptibility to coronary artery disease: A case-control study. MicroRNA 2018, 8, 198–205. [Google Scholar] [CrossRef]
- Jha, C.K.; Mir, R.; Elfaki, I.; Khullar, N.; Rehman, S.; Javid, J.; Banu, S.; Chahal, S. Potential impact of microRNA-423 gene variability in coronary artery disease. Endoc. Metab. Immune Disord. Drug Targ. 2018, 19, 67–74. [Google Scholar] [CrossRef]
- Jha, C.K.; Mir, R.; Khullar, N.; Banu, S.; Chahal, S.M.S. LDLR rs688 TT genotype and T allele are associated with increased susceptibility to coronary artery disease—A case-control study. J. Cardiovasc. Dev. Dis. 2018, 5, 31. [Google Scholar] [CrossRef] [PubMed]
- Mir, R.; Jha, C.K.; Elfaki, I.; Javid, J.; Rehman, S.; Khullar, N.; Banu, S.; Chahal, S.M.S. Incidence of MicroR-4513C/T gene variability in coronary artery disease—A case-control study. Endoc. Metab. Immune Disord. Drug Targ. 2019, 19, 1. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Zhang, B.; Hao, C.; Huang, X.; Li, X.; Huang, Y.; Luo, Z. Omentin-A novel adipokine in respiratory diseases. Int. J. Mol. Sci. 2017, 19, 73. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Ji, Q.; Cai, L.; Huang, F.; Lai, Y.; Liu, Y.; Yu, J.; Han, B.; Zhu, E.; Zhang, J.; et al. Association between omentin-1 expression in human epicardial adipose tissue and coronary atherosclerosis. Cardiovasc. Diabetol. 2016, 15, 90. [Google Scholar] [CrossRef]
- Tan, Y.L.; Zheng, X.L.; Tang, C.K. The protective functions of omentin in cardiovascular diseases. Clin. Chim. Acta 2015, 448, 98–106. [Google Scholar] [CrossRef]
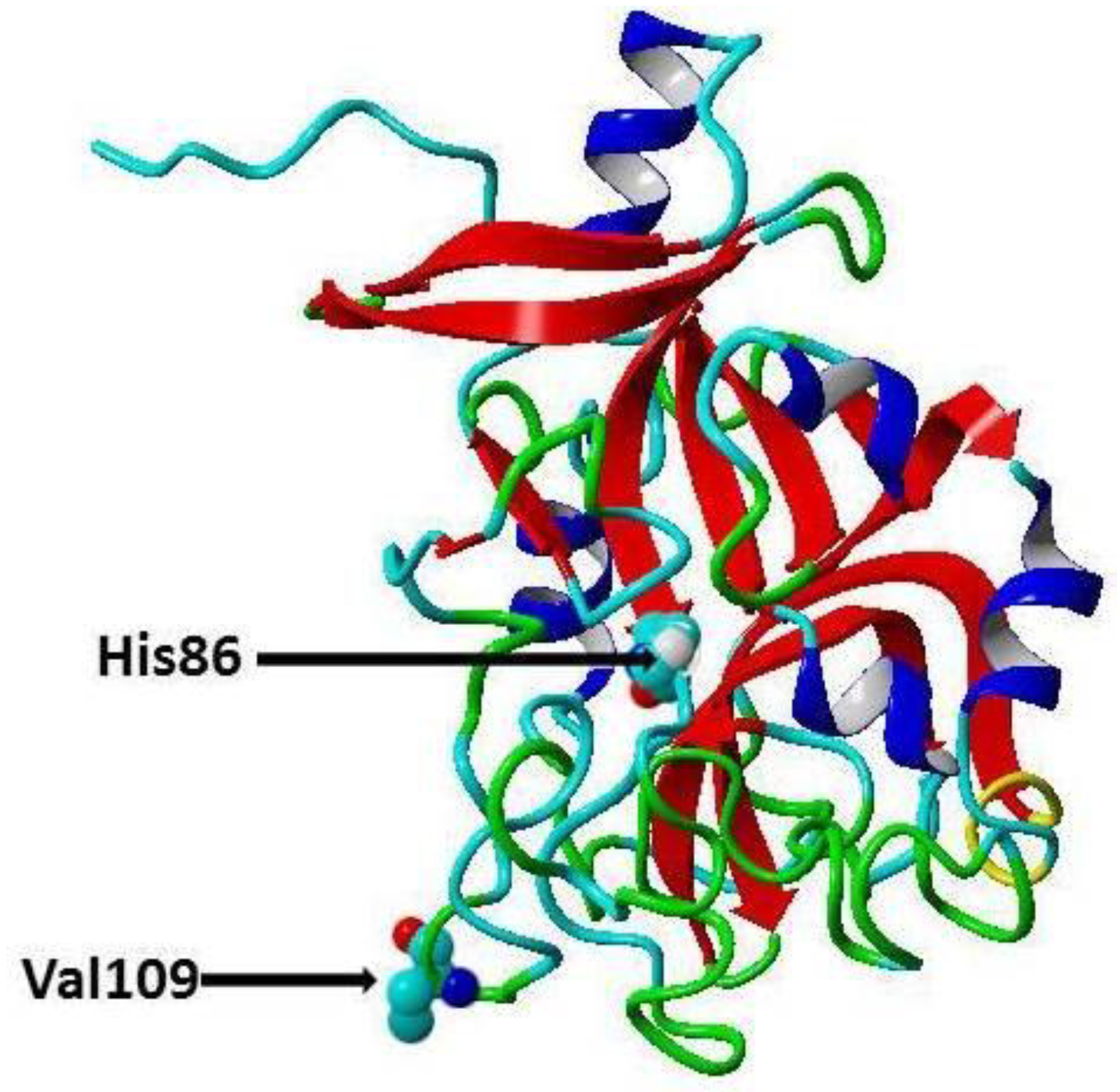
- Jamshidi, J.; Ghanbari, M.; Asnaashari, A.; Jafari, N.; Valizadeh, G.A. Omentin Val109Asp polymorphism and risk of coronary artery disease. Asian Cardiovasc. Thorac. Ann. 2017, 25, 199–203. [Google Scholar] [CrossRef]
- Nazar, S.; Zehra, S.; Azhar, A. Association of single nucleotide missence polymorphism Val109Asp of Omentin-1 gene and coronary artery disease in Pakistani population: Multicenter study. Pak. J. Med. Sci. 2017, 33, 1128–1133. [Google Scholar]
- Wesener, D.A.; Wangkanont, K.; McBride, R.; Song, X.; Kraft, M.B.; Hodges, H.L.; Zarling, L.C.; Splain, R.A.; Smith, D.F.; Cummings, R.D.; et al. Recognition of microbial glycans by human intelectin-1. Nat. Struct. Mol. Biol. 2015, 22, 603. [Google Scholar] [CrossRef]
- Frostegard, J. Immunity, atherosclerosis and cardiovascular disease. BMC Med. 2013, 11, 117. [Google Scholar] [CrossRef]
- Rafieian-Kopaei, M.; Setorki, M.; Doudi, M.; Baradaran, A.; Nasri, H. Atherosclerosis: Process, indicators, risk factors and new hopes. Int. J. Prev. Med. 2014, 5, 927–946. [Google Scholar]
- Stefanadis, C.; Antoniou, C.K.; Tsiachris, D.; Pietri, P. Coronary atherosclerotic vulnerable plaque: Current perspectives. J. Am. Heart Assoc. 2017, 6, e005543. [Google Scholar] [CrossRef] [PubMed]
- Shibata, R.; Ouchi, N.; Takahashi, R.; Terakura, Y.; Ohashi, K.; Ikeda, N.; Higuchi, A.; Terasaki, H.; Kihara, S.; Murohara, T. Omentin as a novel biomarker of metabolic risk factors. Diabetol. Metabol. Syndr. 2012, 4, 37. [Google Scholar] [CrossRef] [PubMed]
- Shibata, R.; Ouchi, N.; Kikuchi, R.; Takahashi, R.; Takeshita, K.; Kataoka, Y.; Ohashi, K.; Ikeda, N.; Kihara, S.; Murohara, T. Circulating omentin is associated with coronary artery disease in men. Atherosclerosis 2011, 219, 811–814. [Google Scholar] [CrossRef] [PubMed]
- Saely, C.H.; Leiherer, A.; Muendlein, A.; Vonbank, A.; Rein, P.; Geiger, K.; Malin, C.; Drexel, H. High plasma omentin predicts cardiovascular events independently from the presence and extent of angiographically determined atherosclerosis. Atherosclerosis 2016, 244, 38–43. [Google Scholar] [CrossRef]
- Schaffler, A.; Zeitoun, M.; Wobser, H.; Buechler, C.; Aslanidis, C.; Herfarth, H. Frequency and significance of the novel single nucleotide missense polymorphism Val109Asp in the human gene encoding omentin in Caucasian patients with type 2 diabetes mellitus or chronic inflammatory bowel diseases. Cardiovasc. Diabetol. 2007, 6, 3. [Google Scholar] [CrossRef]
- Greulich, S.; Chen, W.J.; Maxhera, B.; Rijzewijk, L.J.; van der Meer, R.W.; Jonker, J.T.; Mueller, H.; de Wiza, D.H.; Floerke, R.R.; Smiris, K.; et al. Cardioprotective properties of omentin-1 in type 2 diabetes: Evidence from clinical and in vitro studies. PLoS ONE 2013, 8, e59697. [Google Scholar] [CrossRef]
- Yamawaki, H.; Tsubaki, N.; Mukohda, M.; Okada, M.; Hara, Y. Omentin, a novel adipokine, induces vasodilation in rat isolated blood vessels. In Biochemical and Biophysical Research Communications; Elsevier: Amsterdam, The Netherlands, 2010; pp. 668–672. [Google Scholar]
- Elsaid, N.H.; Sadik, N.A.; Ahmed, N.R.; Fayez, S.E.; Mohammed, N.A.E. Serum omentin-1 levels in type 2 diabetic obese women in relation to glycemic control, insulin resistance and metabolic parameters. J. Clin. Transl. Endocrinol. 2018, 13, 14–19. [Google Scholar] [CrossRef]
- Napoli, C.; Crudele, V.; Soricelli, A.; Al-Omran, M.; Vitale, N.; Infante, T.; Mancini, F.P. Primary prevention of atherosclerosis: A clinical challenge for the reversal of epigenetic mechanisms? Circulation 2012, 125, 2363–2373. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primers sequences of ARMS-PCR for Genotyping of rs2274907 A>T | ||||
|---|---|---|---|---|
| Fo-outer primer | F1 | 5-ACCCCTACCTTCCAGCCATCCC-3 | 403 bp | 60 °C |
| Ro-outer primer | R1 | 5-CATGGGGCTGAAATGAACCCTCAGC-3 | ||
| FI-T-inner primer | T allele | 5-TGCCGTCCCCCTCTGGGTAGT-3 | 251 bp | |
| RIA-inner primer | A allele | 5-GTCAGCAGGGCAGCAAAGCAGA-3 | 193 bp | |
| Primers sequence of Allele Specific -PCR for genotyping of rs2274908 G>A | ||||
| ITLN1-F1 Wild | G allele | ACTTCCCACGCATGTCATTCTCG | 195 bp | 63 °C |
| ITLN1-F2 mutant | A allele | ACTTCCCACGCATGTCATTCTCA | 195 bp | |
| ITLN1-R common | Reverse | CTTTCTTGTCATGGGGCTGAAATGAAC | ||
| Variables | No. of CAD Cases (N = %) | No. of Healthy Controls (N = %) | |
|---|---|---|---|
| No-of cases | 100 (100%) | No-of controls | 100 (100%) |
| Males | 88 (88%) | Males | 85 (85%) |
| Females | 12(12%) | Females | 15 (15%) |
| Age ≤ 50 | 47(47%) | Age ≤ 50 | 45 (45%) |
| Age > 50 | 53(53%) | Age > 50 | 55 (55%) |
| Allele/Genotype | N | AA | % | A/T | % | TT | % | Chi-square | Degree of Freedom (DF) | P-Value |
|---|---|---|---|---|---|---|---|---|---|---|
| CAD patients | 100 | 24 | 24% | 75 | 75% | 1 | 1% | 14.13 | 2 | 0.009 |
| Healthy controls | 100 | 49 | 49% | 51 | 51% | 0 | 0% |
| Subjects | N = 100 | AA | AT | TT | X2 | DF | P-Value |
|---|---|---|---|---|---|---|---|
| Association with gender | |||||||
| Males | 88 | 19 | 68 | 1 | 2.41 | 2 | 0.29 |
| Females | 12 | 5 | 7 | 0 | |||
| Association with Age | |||||||
| Age ≤ 50 | 47 | 14 | 32 | 1 | 2.93 | 2 | 0.23 |
| Age > 50 | 53 | 10 | 43 | 0 | |||
| Association with RBS | |||||||
| RBS ≤ 140 mg | 64 | 14 | 50 | 0 | 1.1 | 2 | 0.371 |
| RBS > 140 mg | 36 | 10 | 25 | 1 | |||
| Association with Cholesterol | |||||||
| Cholesterol ≤ 200 mg | 81 | 14 | 66 | 1 | 10.63 | 2 | 0.0049 |
| Cholesterol > 200 mg | 19 | 10 | 9 | 0 | |||
| Association with HDL | |||||||
| HDL ≤ 40 mg | 67 | 10 | 56 | 1 | 9.45 | 2 | 0.008 |
| HDL > 40 mg | 33 | 14 | 19 | 0 | |||
| Association with LDL | |||||||
| LDL ≤ 100 mg | 72 | 11 | 60 | 1 | 10.92 | 2 | 0.004 |
| LDL > 100 mg | 28 | 13 | 15 | 0 | |||
| Association with TGL | |||||||
| TGL ≤ 150 mg | 58 | 14 | 44 | 0 | 1.42 | 2 | 0.49 |
| TGL > 150 mg | 42 | 10 | 31 | 1 | |||
| Association with hypertension | |||||||
| Hypertension | 22 | 9 | 12 | 1 | 8.48 | 2 | 0.014 |
| No hypertension | 78 | 15 | 63 | 0 | |||
| Association with Diabetes | |||||||
| Diabetes | 16 | 1 | 15 | 0 | 8.16 | 2 | 0.016 |
| No Diabetes | 84 | 23 | 60 | 1 | |||
| Association with family history of CHD | |||||||
| Coronary heart disease (CHD) | 10 | 6 | 4 | 0 | 1.4 | 2 | 0.56 |
| No CHD | 90 | 18 | 71 | 1 | |||
| Association with Smoking | |||||||
| Smoking | 60 | 10 | 50 | 0 | 6.25 | 2 | 0.041 |
| No Smoking | 40 | 14 | 25 | 1 | |||
| Association with Alcohol | |||||||
| Alcohol | 35 | 10 | 25 | 0 | 1.1 | 2 | 0.57 |
| No Alcohol | 65 | 14 | 50 | 1 | |||
| Association with Pan Masala | |||||||
| Pan Masala | 2 | 1 | 1 | 0 | 0.77 | 2 | 0.68 |
| No Pan Masala | 98 | 23 | 74 | 1 | |||
| Genotypes | Healthy Controls | CAD Cases | OR (95% CI) | Risk Ratio (RR) | P-Value |
|---|---|---|---|---|---|
| (N = 100) | (N = 100) | ||||
| Codominant | |||||
| ITLN1-AA | 49 | 24 | 1 (ref.) | 1 (ref.) | |
| ITLN1-AT | 51 | 75 | 3.0 (1.64 to 5.49) | 1.65 (1.27 to 2.163) | 0.002 |
| ITLN1-TT | 0 | 1 | 6.0 (0.23 to 154.31) | 2.67 (0.24 to 29.66) | 0.422 |
| Dominant | |||||
| ITLN1-AA | 49 | 24 | 1 (ref.) | 1 (ref.) | |
| ITLN1-(AT + TT) | 51 | 76 | 3.0 (1.66 to 5.56) | 1.67 (1.28 to 2.18) | 0.003 |
| Recessive | |||||
| ITLN1-(AA + AT) | 100 | 99 | 1 (ref.) | 1 (ref.) | |
| ITLN1-TT | 0 | 1 | 3.03 (0.12 to 75.28) | 2.0 (0.181 to 22.255) | 0.49 |
| Allele | |||||
| ITLN1-A | 149 | 123 | 1 (ref.) | 1 (ref.) | |
| ITLN1-T | 51 | 77 | 1.82 (1.193 to 2.80) | 1.37 (1.08 to 1.74) | 0.005 |
| Subjects | N | GG | % | G/A | % | AA | % | Chi-Square | DF | P-Value |
|---|---|---|---|---|---|---|---|---|---|---|
| CAD patients | 100 | 21 | 21% | 78 | 78% | 1 | 1% | 1.9 | 2 | 0.386 |
| Healthy controls | 100 | 16 | 16% | 84 | 84% | 0 | 0% |
| Genotypes | Healthy Controls | CAD Cases | OR (95% CI) | Risk Ratio (RR) | P-Value |
|---|---|---|---|---|---|
| (N = 100) | (N = 100) | ||||
| Codominant | |||||
| ITLN1-GG | 16 | 21 | 1 (ref.) | 1 (ref.) | |
| ITLN1-GA | 84 | 78 | 0.70 (0.344 to 1.45) | 0.83 (0.56 to 1.24) | 0.34 |
| ITLN1-AA | 0 | 1 | 2.30 (0.08 to 60.23) | 1.73 (0.15 to 19.68) | 0.61 |
| Dominant | |||||
| ITLN1-GG | 16 | 21 | 1 (ref.) | 1 (ref.) | |
| ITLN1-(GA + AA) | 84 | 79 | 0.71 (0.34 to 1.47) | 0.83 (0.56 to 1.24) | 0.36 |
| Recessive | |||||
| ITLN1-(GG + GA) | 100 | 99 | 1 (ref.) | 1 (ref.) | |
| ITLN1-AA | 0 | 1 | 3.03 (0.12 to 75.28) | 2.0 (0.181 to 22.255) | 0.49 |
| Allele | |||||
| ITLN1-G | 116 | 120 | 1 (ref.) | 1 (ref.) | |
| ITLN1-A | 84 | 80 | 0.92 (0.61 to 1.37) | 0.95 (0.78 to 1.16) | 0.68 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jha, C.K.; Mir, R.; Elfaki, I.; Javid, J.; Babakr, A.T.; Banu, S.; Chahal, S.M.S. Evaluation of the Association of Omentin 1 rs2274907 A>T and rs2274908 G>A Gene Polymorphisms with Coronary Artery Disease in Indian Population: A Case Control Study. J. Pers. Med. 2019, 9, 30. https://doi.org/10.3390/jpm9020030
Jha CK, Mir R, Elfaki I, Javid J, Babakr AT, Banu S, Chahal SMS. Evaluation of the Association of Omentin 1 rs2274907 A>T and rs2274908 G>A Gene Polymorphisms with Coronary Artery Disease in Indian Population: A Case Control Study. Journal of Personalized Medicine. 2019; 9(2):30. https://doi.org/10.3390/jpm9020030
Chicago/Turabian StyleJha, Chandan K, Rashid Mir, Imadeldin Elfaki, Jamsheed Javid, Abdullatif Taha Babakr, Shaheena Banu, and S. M. S. Chahal. 2019. "Evaluation of the Association of Omentin 1 rs2274907 A>T and rs2274908 G>A Gene Polymorphisms with Coronary Artery Disease in Indian Population: A Case Control Study" Journal of Personalized Medicine 9, no. 2: 30. https://doi.org/10.3390/jpm9020030