A Theoretical Framework and Conceptual Design for Engaging Children in Therapy at Home—The Design of a Wearable Breathing Trainer


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
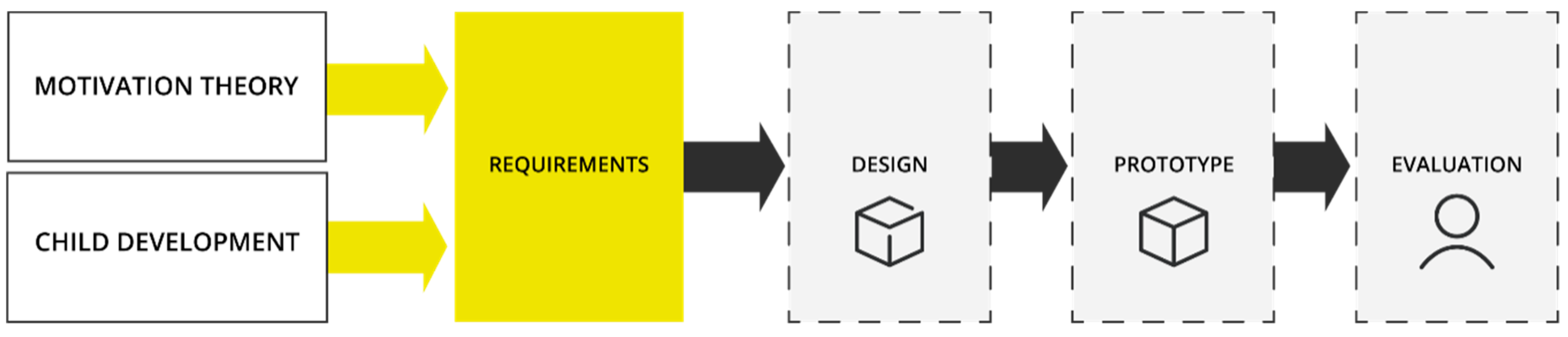
2. Design Methodology
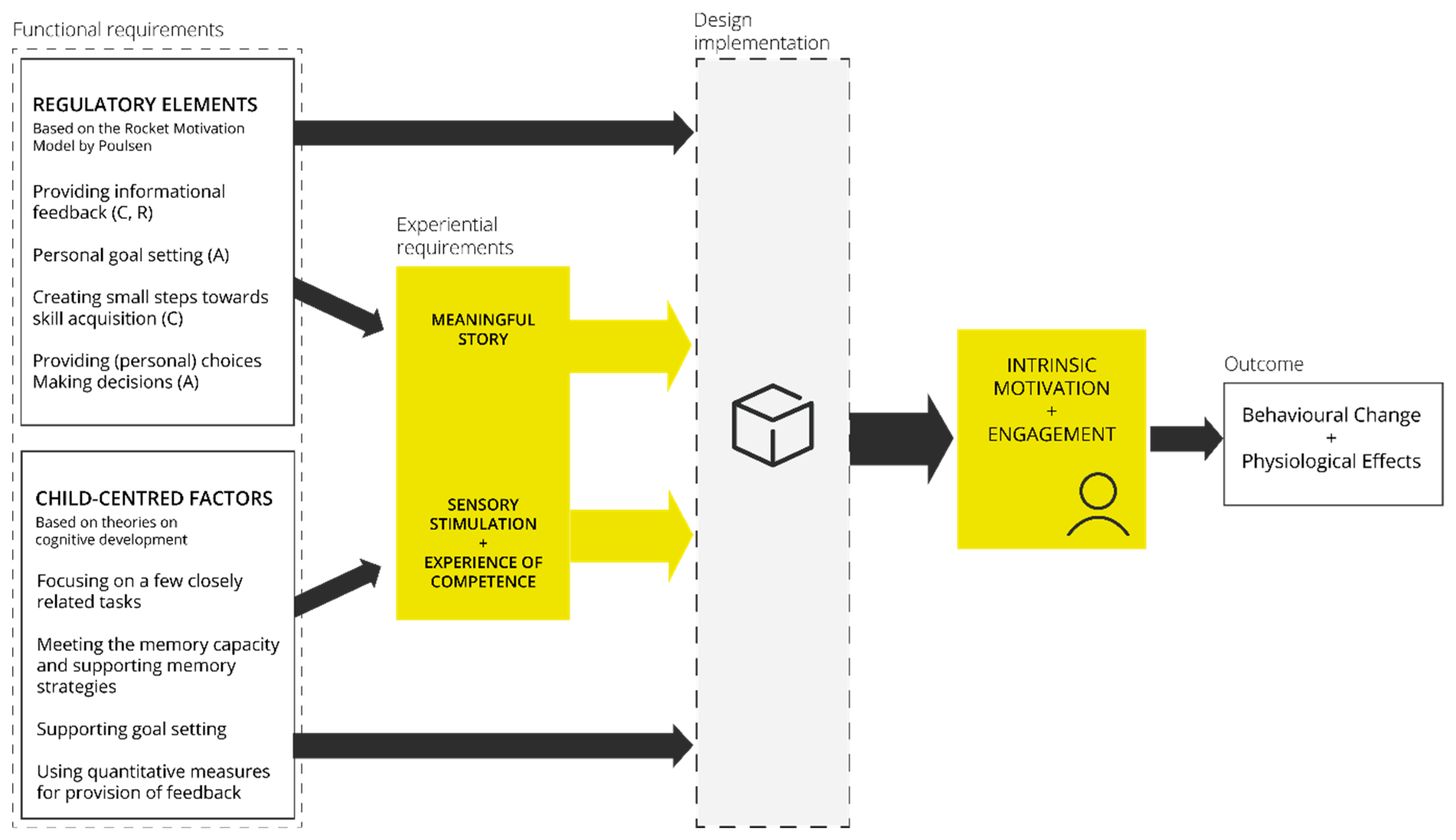
2.1. Theoretical Framework for Engaging Children in Therapy at Home
- Providing (trustworthy) informational feedback
- Offering personal goal setting
- Providing (personal) choices
- Small steps towards skill acquisition
- Letting the child make decisions
- Focus on a few closely related tasks
- Meet the memory capacity (5–6 chunks of information)
- Support memory strategies
- Support goal setting
- Use quantitative measures for the provision of feedback
2.2. Applying the Framework to Design a Wearable Breathing Trainer
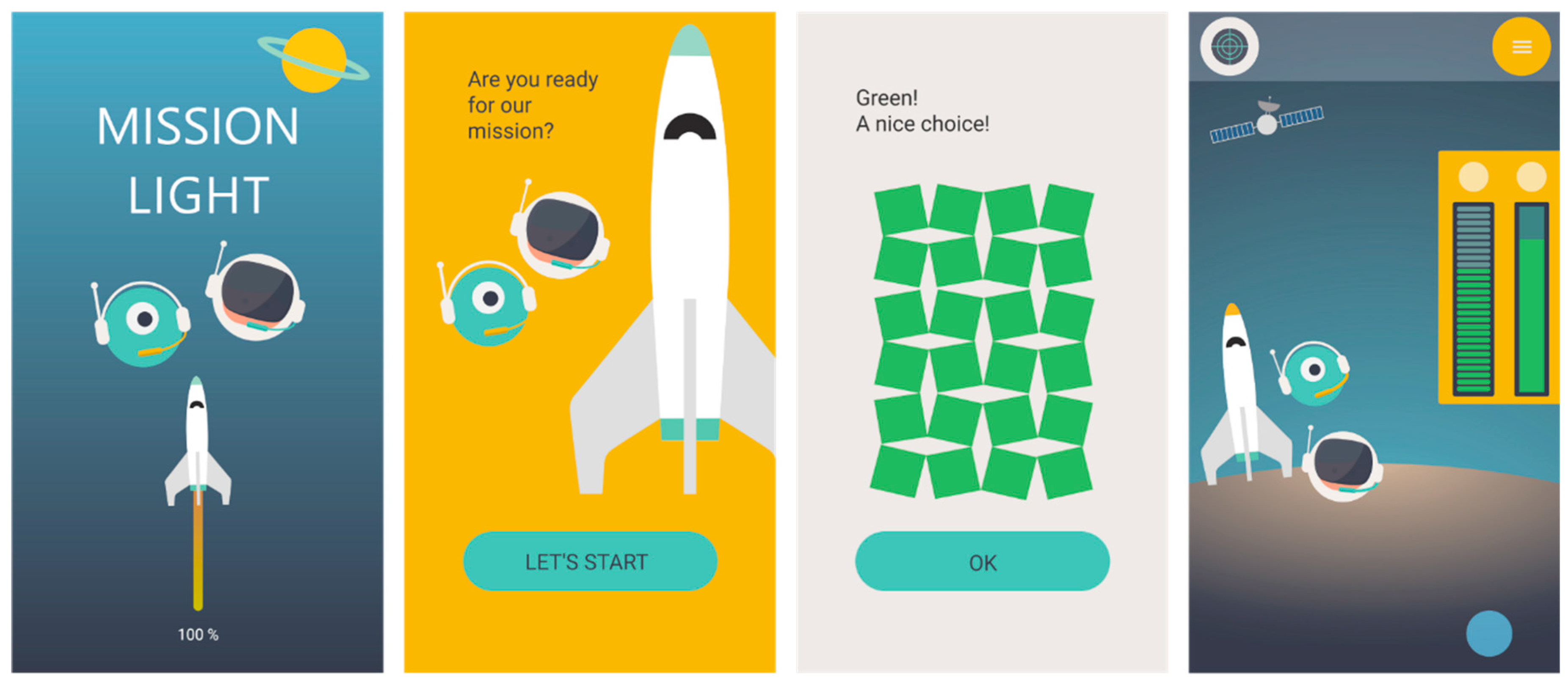
2.2.1. Design
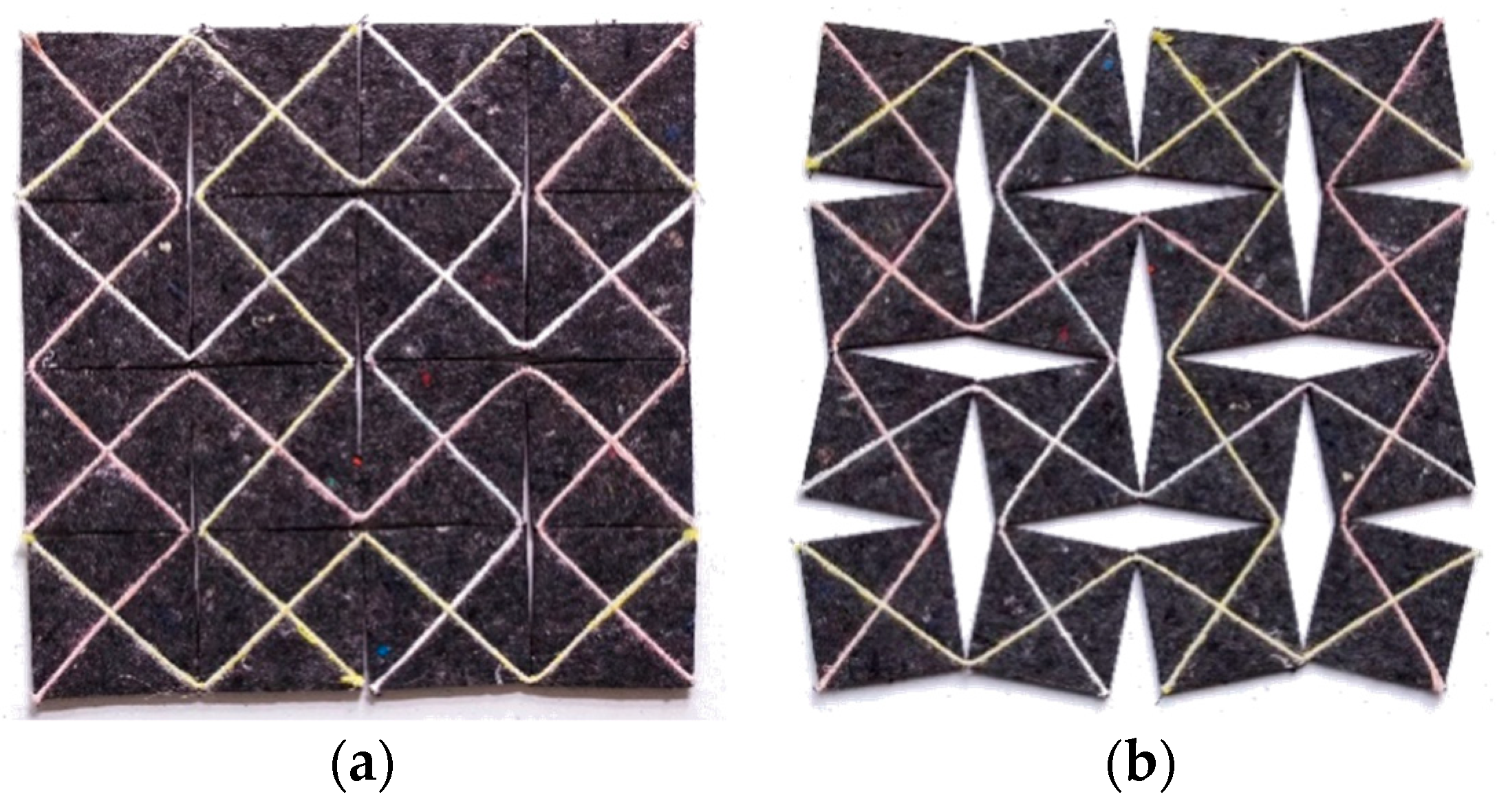
2.2.2. Prototyping
3. Formative Evaluation of the Design
3.1. Evaluation by Experts
3.2. Evaluation by the Target Group
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Harte, R.; Quinlan, L.; Glynn, L.; Rodriguez-Molinero, A.; Scharf, T.; Carenas, C.; Reixach, E.; Garcia, J.; Carrabina, J.; ÓLaighin, G.; et al. A Multi-Stage Human Factors and Comfort Assessment of Instrumented Insoles Designed for Use in a Connected Health Infrastructure. J. Pers. Med. 2015, 5, 487–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vegesna, A.; Tran, M.; Angelaccio, M.; Arcona, S. Remote Patient Monitoring via Non-Invasive Digital Technologies: A Systematic Review. Telemed. e-Health 2017, 23, 3–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banaee, H.; Ahmed, M.; Loutfi, A.; Banaee, H.; Ahmed, M.U.; Loutfi, A. Data Mining for Wearable Sensors in Health Monitoring Systems: A Review of Recent Trends and Challenges. Sensors 2013, 13, 17472–17500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, S.; Park, H.; Bonato, P.; Chan, L.; Rodgers, M. A review of wearable sensors and systems with application in rehabilitation. J. Neuroeng. Rehabil. 2012, 9, 21. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, M.M.; Pai, V.M.; Conroy, R.S. Recent Advances in Wearable Sensors for Health Monitoring. IEEE Sens. J. 2015, 15, 3119–3126. [Google Scholar] [CrossRef]
- Kromer, R. Begriffsdefinitionen und Abgrenzungen. In Smart Clothes: Ideengenerierung, Bewertung und Markteinführung; Springer: Wiesbaden, Germany, 2011; pp. 13–20. [Google Scholar]
- Smelik, A.; Toussaint, L.; Van Dongen, P. Solar fashion: An embodied approach to wearable technology. Int. J. Fash. Stud. 2016, 3, 287–303. [Google Scholar] [CrossRef]
- by-wire.net. Closed Loop Smart Athleisure Fashion. Available online: http://www.by-wire.net/clsaf/ (accessed on 14 February 2019).
- Wang, Q.; Chen, W.; Timmermans, A.A.A.; Karachristos, C.; Martens, J.B.; Markopoulos, P. Smart Rehabilitation Garment for posture monitoring. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milano, Italy, August 2015; pp. 5736–5739. [Google Scholar]
- Schneegass, S.; Amft, O. Introduction to Smart Textiles. In Smart Textiles: Fundamentals, Design, and Interaction; Schneegass, S., Amft, O., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 1–15. [Google Scholar]
- Du, J.; Markopoulos, P.; Wang, Q.; Toeters, M.; Gong, T. ShapeTex. In Proceedings of the Twelfth International Conference on Tangible, Embedded, and Embodied Interaction—TEI ’18; ACM Press: New York, NY, USA, 2018; pp. 166–176. [Google Scholar]
- RUAH—Giulia Tomasello. Available online: https://gitomasello.com/RUAH (accessed on 15 February 2019).
- Morgan, M.D.L. Dysfunctional breathing in asthma: Is it common, identifiable and correctable? Thorax 2002, 57 (Suppl. 2), II31–II35. [Google Scholar] [PubMed]
- Barker, N.J.; Elphick, H.; Everard, M.L. The impact of a dedicated physiotherapist clinic for children with dysfunctional breathing. ERJ Open Res. 2016, 2, 00103–02015. [Google Scholar] [CrossRef] [PubMed]
- De Groot, E.P. Breathing abnormalities in children with breathlessness. Paediatr. Respir. Rev. 2011, 12, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Lawlor, M.C. The Particularities of Engagement: Intersubjectivity in Occupational Therapy Practice. OTJR Occup. Particip. Heal. 2012, 32, 151–159. [Google Scholar] [CrossRef]
- Galotti, K.M. Cognitive Development: Infancy through Adolescence; Sage Publications: Thousand Oaks, CA, USA, 2015; ISBN 9781483379173. [Google Scholar]
- Perski, O.; Blandford, A.; West, R.; Michie, S. Conceptualising engagement with digital behaviour change interventions: A systematic review using principles from critical interpretive synthesis. Transl. Behav. Med. 2017, 7, 254–267. [Google Scholar] [CrossRef] [PubMed]
- Garris, R.; Ahlers, R.; Driskell, J.E. Games, Motivation, and Learning: A Research and Practice Model. Simul. Gaming 2002, 33, 441–467. [Google Scholar] [CrossRef] [Green Version]
- Ryan, R.M.; Rigby, C.S.; Przybylski, A. The Motivational Pull of Video Games: A Self-Determination Theory Approach. Motiv. Emot. 2006, 30, 344–360. [Google Scholar] [CrossRef] [Green Version]
- Przybylski, A.K.; Rigby, C.S.; Ryan, R.M. A motivational model of video game engagement. Rev. Gen. Psychol. 2010, 14, 154–166. [Google Scholar] [CrossRef]
- Denis, G.; Jouvelot, P. Motivation-driven educational game design. In Proceedings of the 2005 ACM SIGCHI International Conference on Advances in computer entertainment technology—ACE ’05; ACM Press: New York, NY, USA, 2005; pp. 462–465. [Google Scholar]
- Guay, F.; Ratelle, C.F.; Chanal, J. Optimal learning in optimal contexts: The role of self-determination in education. Can. Psychol. Can. 2008, 49, 233–240. [Google Scholar] [CrossRef]
- Poulsen, A.; Ziviani, J.; Cuskelly, M. Understanding motivation in the context of engaging children in therapy. In The art and science of the motivation: A therapists guide to working with children; Poulsen, A., Ziviani, J., Cuskelly, M., Eds.; Jessica Kingsley Publishers: London, UK, 2013; pp. 23–32. [Google Scholar]
- Hourcade, J.P. Interaction Design and Children. Found. Trends® Human-Computer Interact. 2007, 1, 277–392. [Google Scholar] [CrossRef] [Green Version]
- Gelderblom, H.; Kotzé, P. Ten design lessons from the literature on child development and children’s use of technology. In Proceedings of the 8th International Conference on Interaction Design and Children—IDC ’09; ACM Press: New York, NY, USA, 2009; p. 52. [Google Scholar]
- Janssen, J.; Verschuren, O.; Renger, W.J.; Ermers, J.; Ketelaar, M.; van Ee, R. Gamification in Physical Therapy. Pediatr. Phys. Ther. 2017, 29, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Deterding, S.; Dixon, D.; Khaled, R.; Nacke, L. From game design elements to gamefulness. In Proceedings of the 15th International Academic MindTrek Conference on Envisioning Future Media Environments—MindTrek ’11; ACM Press: New York, NY, USA, 2011; p. 9. [Google Scholar]
- Sailer, M.; Hense, J.U.; Mayr, S.K.; Mandl, H. How gamification motivates: An experimental study of the effects of specific game design elements on psychological need satisfaction. Comput. Human Behav. 2017, 69, 371–380. [Google Scholar] [CrossRef]
- Greber, C.; Hinojosa, J.; Ziviani, J. Achieving success - Facilitating skill aquisition and enabling participation. In The art and science of the motivation: A therapists guide to working with children; Ziviani, J., Poulsen, A.A., Cuskelly, M., Eds.; Jessica Kingsley Publishers: London, UK, 2013; pp. 123–157. [Google Scholar]
- van Rees, H.; Mader, A.H.; Smits, M.; Ludden, G.D.S.; Lamontagne, V. Textile waste and haptic feedback for wearable robotics 2018. In Proceedings of the Design Research Society 2018, Limerick, Ireland, 25–28 June 2018. [Google Scholar]
- Ludden, G.D.S.; van Rompay, T.J.L. How does it feel? Exploring touch on different levels of product experience. J. Eng. Des. 2015, 26, 157–168. [Google Scholar] [CrossRef]
- ARDUINO. Available online: https://www.arduino.cc/ (accessed on 15 March 2019).
- Blandford, A.; Gibbs, J.; Newhouse, N.; Perski, O.; Singh, A.; Murray, E. Seven lessons for interdisciplinary research on interactive digital health interventions. Digit. Heal. 2018, 4. [Google Scholar] [CrossRef] [PubMed]
- Zaman, B. Evaluating games with children. In Proceedings of the Interact 2005 Workshop on Child computer Interaction: Methodological Research, Rome, Italy, September 2005. [Google Scholar]
- Huisman, G.; van Hout, M. The development of a graphical emotion measurement instrument using caricatured expressions: The LEMtool. In Proceedings of the Emotion in HCI—Designing for People. Proceedings of the 2008 International Workshop; Frauenhofer Verlag: Stuttgart, Germany, 2010; pp. 5–8. [Google Scholar]







© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siering, L.; Ludden, G.D.S.; Mader, A.; van Rees, H. A Theoretical Framework and Conceptual Design for Engaging Children in Therapy at Home—The Design of a Wearable Breathing Trainer. J. Pers. Med. 2019, 9, 27. https://doi.org/10.3390/jpm9020027
Siering L, Ludden GDS, Mader A, van Rees H. A Theoretical Framework and Conceptual Design for Engaging Children in Therapy at Home—The Design of a Wearable Breathing Trainer. Journal of Personalized Medicine. 2019; 9(2):27. https://doi.org/10.3390/jpm9020027
Chicago/Turabian StyleSiering, Lara, Geke D.S. Ludden, Angelika Mader, and Hellen van Rees. 2019. "A Theoretical Framework and Conceptual Design for Engaging Children in Therapy at Home—The Design of a Wearable Breathing Trainer" Journal of Personalized Medicine 9, no. 2: 27. https://doi.org/10.3390/jpm9020027