

Differences between Squamous Cell Carcinomas of the Base of the Tongue and the Tonsils in Prevalence of HPV16 Infection, Its Type, and Clinical Features
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. DNA Extraction
2.3. Assessment of Transcriptionally Active HPV16 Infection
2.4. Assessment of Viral Load and Viral Genome Status
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics of a Group of 63 Patients with Squamous Cell Carcinoma of the Oropharynx
3.2. Differences between Squamous Cell Carcinoma of Base of Tongue and Tonsil in Epidemiological, Clinical, and Histopathological Features as Well as Prevalence of HPV16 Infection and Its Type
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jordan, K.H.; Fisher, J.L.; Paskett, E.D. Distinct sociodemographic differences in incidence and survival rates for human papillomavirus (HPV)-like, non-HPV-like, and “other”-like oral cavity and pharynx cancers: An analysis of Surveillance, Epidemiology and End Results (SEER) Program data. Front. Oncol. 2022, 12, 980900. [Google Scholar] [CrossRef]
- Maxwell, J.H.; Grandis, J.R.; Ferris, R.L. HPV-Associated Head and Neck Cancer: Unique Features of Epidemiology and Clinical Management. Annu. Rev. Med. 2016, 67, 91–101. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, A.J.; Vokes, E.E. Optimizing Treatment De-Escalation in Head and Neck Cancer: Current and Future Perspectives. Oncol. 2021, 26, 40–48. [Google Scholar] [CrossRef]
- Mehanna, H.; Robinson, M.; Hartley, A.; Kong, A.; Foran, B.; Fulton-Lieuw, T.; Dalby, M.; Mistry, P.; Sen, M.; O’Toole, L.; et al. Radiotherapy plus cisplatin or cetuximab in low-risk human papillomavirus-positive oropharyngeal cancer (De-ESCALaTE HPV): An open-label randomised controlled phase 3 trial. Lancet 2019, 393, 51–60. [Google Scholar] [CrossRef] [Green Version]
- Gillison, M.L.; Trotti, A.M.; Harris, J.; Eisbruch, A.; Harari, P.M.; Adelstein, D.J.; Jordan, R.C.K.; Zhao, W.; Sturgis, E.M.; Burtness, B.; et al. Radiotherapy plus cetuximab or cisplatin in human papillomavirus-positive oropharyngeal cancer (NRG Oncology RTOG 1016): A randomised, multicentre, non-inferiority trial. Lancet 2019, 393, 40–50. [Google Scholar] [CrossRef]
- Dayyani, F.; Etzel, C.J.; Liu, M.; Ho, C.-H.; Lippman, S.M.; Tsao, A.S. Meta-analysis of the impact of human papillomavirus (HPV) on cancer risk and overall survival in head and neck squamous cell carcinomas (HNSCC). Head Neck Oncol. 2010, 2, 15. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Li, J.; Zhou, Y.; Hu, Q.; Zeng, Y.; Mohammadreza, M.M. Human papillomavirus as a favorable prognostic factor in a subset of head and neck squamous cell carcinomas: A meta-analysis. J. Med. Virol. 2016, 89, 710–725. [Google Scholar] [CrossRef]
- O’Rorke, M.A.; Ellison, M.V.; Murray, L.J.; Moran, M.; James, J.; Anderson, L.A. Human papillomavirus related head and neck cancer survival: A systematic review and meta-analysis. Oral Oncol. 2012, 48, 1191–1201. [Google Scholar] [CrossRef]
- Ragin, C.C.R.; Taioli, E. Survival of squamous cell carcinoma of the head and neck in relation to human papillomavirus infection: Review and meta-analysis. Int. J. Cancer 2007, 121, 1813–1820. [Google Scholar] [CrossRef]
- Marur, S.; Li, S.; Cmelak, A.J.; Gillison, M.L.; Zhao, W.J.; Ferris, R.L.; Westra, W.H.; Gilbert, J.; Bauman, J.E.; Wagner, L.I.; et al. E1308: Phase II Trial of Induction Chemotherapy Followed by Reduced-Dose Radiation and Weekly Cetuximab in Patients with HPV-Associated Resectable Squamous Cell Carcinoma of the Oropharynx— ECOG-ACRIN Cancer Research Group. J. Clin. Oncol. 2017, 35, 490–497. [Google Scholar] [CrossRef] [Green Version]
- Alotaibi, M.; Valova, V.; Hänsel, T.; Stromberger, C.; Kofla, G.; Olze, H.; Piwonski, I.; Albers, A.; Ochsenreither, S.; Coordes, A. Impact of Smoking on the Survival of Patients With High-risk HPV-positive HNSCC: A Meta-analysis. Vivo 2021, 35, 1017–1026. [Google Scholar] [CrossRef]
- Janecka-Widła, A.; Majchrzyk, K.; Mucha-Małecka, A.; Słonina, D.; Biesaga, B. Prognostic potential of Akt, pAkt(Ser473) and pAkt(Thr308) immunoreactivity in relation to HPV prevalence in head and neck squamous cell carcinoma patients. Pathol. Res. Pract. 2021, 229, 153684. [Google Scholar] [CrossRef]
- Kwon, S.; Ahn, S.-H.; Jeong, W.-J.; Jung, Y.H.; Bae, Y.J.; Paik, J.H.; Chung, J.-H.; Kim, H. Estrogen receptor α as a predictive biomarker for survival in human papillomavirus-positive oropharyngeal squamous cell carcinoma. J. Transl. Med. 2020, 18, 240. [Google Scholar] [CrossRef]
- Mroz, E.A.; Rocco, J.W. MATH, a novel measure of intratumor genetic heterogeneity, is high in poor-outcome classes of head and neck squamous cell carcinoma. Oral Oncol. 2013, 49, 211–215. [Google Scholar] [CrossRef] [Green Version]
- Mroz, E.A.; Tward, A.D.; Pickering, C.R.; Myers, J.N.; Ferris, R.L.; Rocco, J.W. High intratumor genetic heterogeneity is related to worse outcome in patients with head and neck squamous cell carcinoma. Cancer 2013, 119, 3034–3042. [Google Scholar] [CrossRef]
- Kołodziej-Rzepa, M.; Biesaga, B.; Janecka-Widła, A.; Mucha-Małecka, A. Lack of CD44 and Sox-2 Overexpression as Two Independent Favourable Prognostic Factors in HPV Positive Patients with Oropharyngeal Cancers. Pathobiology 2022, 89, 205–219. [Google Scholar] [CrossRef]
- Ndiaye, C.; Mena, M.; Alemany, L.; Arbyn, M.; Castellsagué, X.; Laporte, L.; Bosch, F.X.; de Sanjosé, S.; Trottier, H. HPV DNA, E6/E7 mRNA, and p16INK4a detection in head and neck cancers: A systematic review and meta-analysis. Lancet Oncol. 2014, 15, 1319–1331. [Google Scholar] [CrossRef]
- Windon, M.J.; Fakhry, C.; Margalit, D.N.; Dey, T.; Rettig, E.M. Epidemiologic distinctions between base of tongue and tonsil oropharyngeal carcinomas. Head Neck 2021, 43, 3076–3085. [Google Scholar] [CrossRef]
- Biesaga, B.; Mucha-Małecka, A.; Janecka-Widła, A.; Kołodziej-Rzepa, M.; Szostek, S.; Słonina, D.; Kowalczyk, A.; Halaszka, K.; Przewoźnik, M. Differences in the prognosis of HPV16-positive patients with squamous cell carcinoma of head and neck according to viral load and expression of P16. J. Cancer Res. Clin. Oncol. 2018, 144, 63–73. [Google Scholar] [CrossRef] [Green Version]
- Biesaga, B.; Janecka, A.; Mucha-Małecka, A.; Adamczyk, A.; Szostek, S.; Słonina, D.; Halaszka, K.; Przewoźnik, M. HPV16 detection by qPCR method in relation to quantity and quality of DNA extracted from archival formalin fixed and paraffin embedded head and neck cancer tissues by three commercially available kits. J. Virol. Methods 2016, 236, 157–163. [Google Scholar] [CrossRef]
- Lewis, J.S.; Chernock, R.D.; Ma, X.-J.; Flanagan, J.J.; Luo, Y.; Gao, G.; Wang, X.; El-Mofty, S.K. Partial p16 staining in oropharyngeal squamous cell carcinoma: Extent and pattern correlate with human papillomavirus RNA status. Mod. Pathol. 2012, 25, 1212–1220. [Google Scholar] [CrossRef] [Green Version]
- Biesaga, B.; Szostek, S.; Klimek, M.; Jakubowicz, J.; Wysocka, J. Comparison of the sensitivity and specificity of real-time PCR and in situ hybridization in HPV16 and 18 detection in archival cervical cancer specimens. Folia Histochem. Cytobiol. 2012, 50, 239–247. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.-P.; Wang, Y.-Q.; Lv, J.-W.; Li, Y.-Q.; Chua, M.L.K.; Le, Q.-T.; Lee, N.; Colevas, A.D.; Seiwert, T.; Hayes, D.N.; et al. Identification and validation of novel microenvironment-based immune molecular subgroups of head and neck squamous cell carcinoma: Implications for immunotherapy. Ann. Oncol. 2019, 30, 68–75. [Google Scholar] [CrossRef]
- Welters, M.J.; Ma, W.; Santegoets, S.J.; Goedemans, R.; Ehsan, I.; Jordanova, E.S.; van Ham, V.J.; van Unen, V.; Koning, F.; van Egmond, S.I.; et al. Intratumoral HPV16-Specific T Cells Constitute a Type I–Oriented Tumor Microenvironment to Improve Survival in HPV16-Driven Oropharyngeal Cancer. Clin. Cancer Res. 2018, 24, 634–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kreimer, A.R.; Clifford, G.M.; Snijders, P.J.; Castellsagué, X.; Meijer, C.J.; Pawlita, M.; Viscidi, R.; Herrero, R.; Franceschi, S. International Agency for Research on Cancer (IARC) Multicenter Oral Cancer Study Group. HPV16 semiquantitative viral load and serologic biomarkers in oral and oropharyngeal squamous cell carcinomas. Int. J. Cancer 2005, 115, 329–332. [Google Scholar] [CrossRef] [PubMed]
- Deng, Z.; Hasegawa, M.; Kiyuna, A.; Matayoshi, S.; Uehara, T.; Agena, S.; Yamashita, Y.; Ogawa, K.; Maeda, H.; Suzuki, M. Viral load, physical status, and E6/E7 mRNA expression of human papillomavirus in head and neck squamous cell carcinoma. Head Neck 2013, 35, 800–808. [Google Scholar] [CrossRef] [PubMed]
- Holzinger, D.; Schmitt, M.; Dyckhoff, G.; Benner, A.; Pawlita, M.; Bosch, F.X. Viral RNA Patterns and High Viral Load Reliably Define Oropharynx Carcinomas with Active HPV16 Involvement. Cancer Res 2012, 72, 4993–5003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, A.C.; Briolat, J.; Millon, R.; de Reyniès, A.; Rickman, D.; Thomas, E.; Abecassis, J.; Clavel, C.; Wasylyk, B. Biological and clinical relevance of transcriptionally active human papillomavirus (HPV) infection in oropharynx squamous cell carcinoma. Int. J. Cancer 2010, 126, 1882–1894. [Google Scholar] [CrossRef] [PubMed]
- McClory, S.; Hughes, T.; Freud, A.G.; Briercheck, E.L.; Martin, C.; Trimboli, A.J.; Yu, J.; Zhang, X.; Leone, G.; Nuovo, G.; et al. Evidence for a stepwise program of extrathymic T cell development within the human tonsil. J. Clin. Investig. 2012, 122, 1403–1415. [Google Scholar] [CrossRef]
- Ukpo, O.C.; Thorstad, W.L.; Lewis, J.S. B7-H1 Expression Model for Immune Evasion in Human Papillomavirus-Related Oropharyngeal Squamous Cell Carcinoma. Head Neck Pathol. 2013, 7, 113–121. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| All (%) 1 | Localization of Squamous Cell Carcinoma | |||
|---|---|---|---|---|
| Base of Tongue n (%) 2 | Tonsil n (%) | Test χ 2 p * | ||
| All | 63 (100.0) | 19 (30.2) | 44 (69.8) | |
| Age | ||||
| ≤58 years 3 | 36 (57.1) | 12 (33.3) | 24 (66.7) | |
| >58 years | 27 (42.9) | 7 (25.9) | 20 (74.1) | 0.526 |
| Gender | ||||
| Female | 15 (23.8) | 1 (6.7) | 14 (93.3) | |
| Male | 48 (76.2) | 18 (37.5) | 30 (62.5) | 0.023 |
| Status in the Karnofsky scale | ||||
| <80% | 26 (41.3) | 6 (23.1) | 20 (76.9) | |
| ≥80% | 37 (58.7) | 13 (35.1) | 24 (64.9) | 0.304 |
| The level of smoking-Brinkman index 4 | ||||
| ≤520 3 | 34 (54.0) | 8 (23.5) | 26 (76.5) | |
| >520 | 29 (46.0) | 11 (37.9) | 18 (62.1) | 0.214 |
| The level of drinking 5 | ||||
| Low | 28 (44.4) | 5 (17.9) | 23 (82.1) | |
| High | 35 (55.6) | 14 (40.0) | 21 (60.0) | 0.057 |
| T stage | ||||
| 2 | 15 (23.8) | 4 (26.7) | 11 (73.3) | |
| 3 | 32 (50.8) | 7 (21.9) | 25 (78.1) | |
| 4 | 16 (25.4) | 8 (50.0) | 8 (50.0) | 0.045 |
| N stage | ||||
| 0 | 10 (15.9) | 5 (50.0) | 5 (50.0) | |
| 1 | 13 (20.6) | 2 (15.4) | 11 (84.6) | |
| 2 + 3 | 40 (63.5) | 12 (30.0) | 28 (70.0) | 0.971 |
| Grade | ||||
| 1 | 25 (39.7) | 7 (28.0) | 18 (72.0) | |
| 2 + 3 | 38 (60.3) | 12 (31.6) | 26 (68.4) | 0.762 |
| Keratinization | ||||
| Yes | 35 (44.4) | 16 (45.7) | 19 (54.3) | |
| No | 28 (55.6) | 3 (10.7) | 25 (89.3) | 0.003 |
| Transcriptionally active HPV16 infection | ||||
| Yes | 27 (42.9) | 1 (3.7) | 26 (96.3) | |
| Not | 36 (57.1) | 18 (50.0) | 18 (50.0) | 0.000 |
| P16 immunopositivity | ||||
| Yes | 27 (42.9) | 7 (25.9) | 20 (74.1) | |
| Not | 36 (57.1) | 20 (55.6) | 16 (44.4) | 0.019 |
| Viral load (only in HPV16 positive, n = 27) | ||||
| >6764.3 copies/cell 3 | 17 (63.0) | 0 (0.0) | 17 (100.0) | |
| ≤6764.3 copies/cell | 10 (37.0) | 4 (40.0) | 6 (60.0) | 0.024 * |
| Physical genome status (only in HPV16 positive, n = 27) | ||||
| Integrated | 8 (29.6) | 0 (0.0) | 8 (100.0) | |
| Mixed | 19 (70.4) | 4 (21.1) | 15 (78.9) | 0.508 |
| Treatment | ||||
| Definitive CisPt-CRT or surgery + CisPt-CRT | 28 (44.4) | 4 (14.3) | 24 (85.7) | |
| Definitive RT or surgery + RT | 19 (30.2) | 8 (42.1) | 11 (57.9) | |
| Induction CT + definitive RT | 16 (25.4) | 7 (43.7) | 9 (56.3) | 0.058 |
| Treatment outcome | ||||
| Regression of cancer disease | 45 (71.4) | 9 (20.0) | 36 (80.0) | |
| Treatment failure | 2 (3.2) | 1 (50.0) | 1 (50.0) | |
| Local recurrence | 12 (19.1) | 7 (58.3) | 5 (41.7) | |
| Distant metastases | 2 (6.3) | 1 (50.0) | 1 (50.0) | 0.049 |
| Survival | ||||
| Alive at the last follow-up | 34 (54.0) | 3 (8.8) | 31 (91.2) | |
| Death from cancer disease | 15 (20.0) | 9 (60.0) | 6 (40.0) | |
| Death from other reasons | 14 (35.7) | 7 (50.0) | 7 (50.0) | 0.000 |
| 5-Year Disease Free Survival | ||||
|---|---|---|---|---|
| Response n (%) | HR | 95% CI | Log-Rank p | |
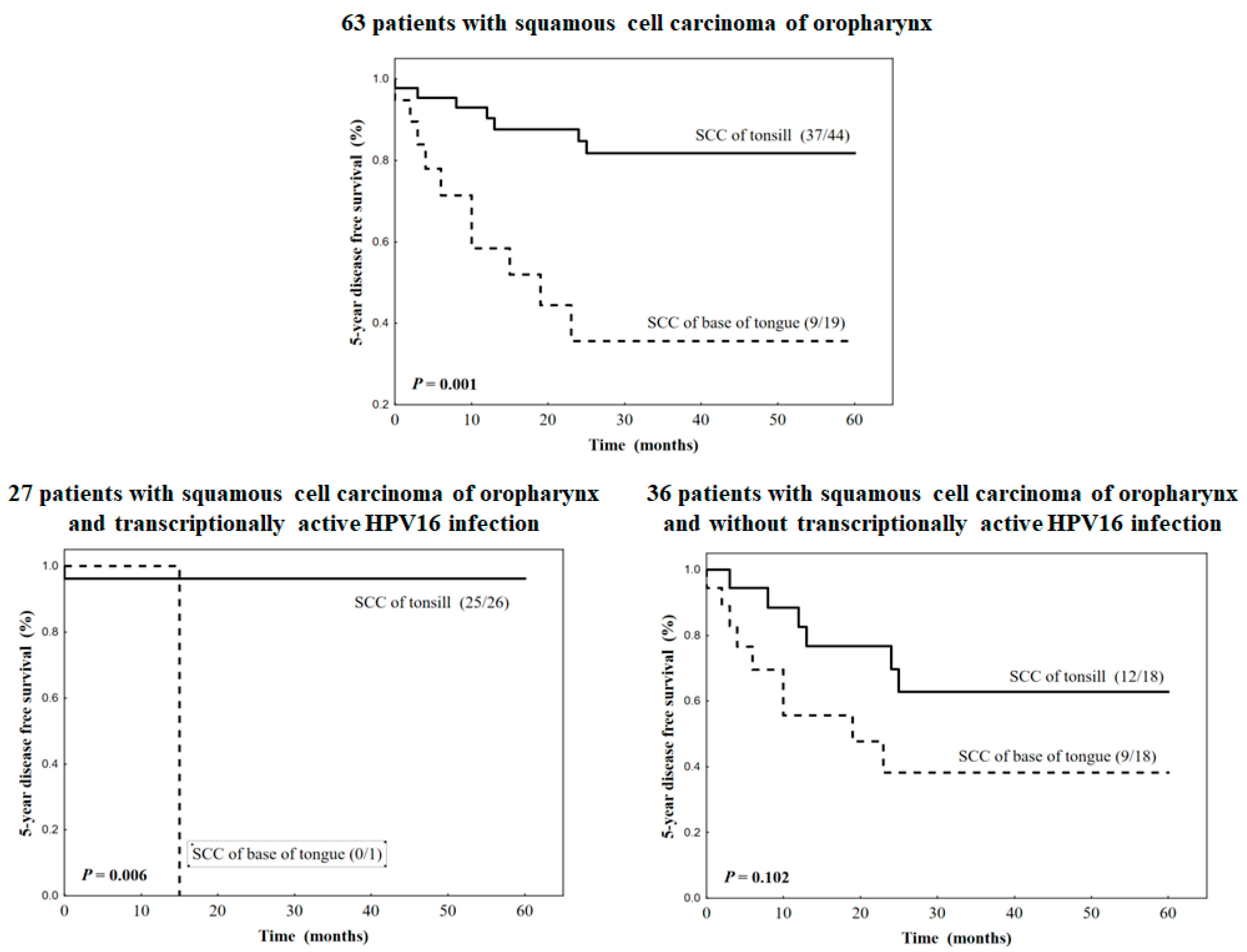
| 63 patients with squamous cell carcinoma of head and neck | ||||
| Base of tongue | 9/19 (47.4) | 5.138 | 1.927–13.706 | 0.001 |
| Tonsil | 37/44 (84.1) | 1.000 | ||
| 27 patients with squamous cell carcinoma of head and neck and transcriptionally active HPV16 infection | ||||
| Base of tongue | 0/1 (0.0) | 12.220 | 1.378–25.283 | 0.006 |
| Tonsil | 25/26 (96.1) | 1.000 | ||
| 36 patients with squamous cell carcinoma of head and neck and without transcriptionally active HPV16 infection | ||||
| Base of tongue | 9/18 (50.0%) | 2.372 | 0.836–6.732 | 0.102 |
| Tonsil | 12/18 (66.7) | 1.000 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biesaga, B.; Mucha-Małecka, A.; Janecka-Widla, A.; Małecki, K. Differences between Squamous Cell Carcinomas of the Base of the Tongue and the Tonsils in Prevalence of HPV16 Infection, Its Type, and Clinical Features. J. Pers. Med. 2023, 13, 361. https://doi.org/10.3390/jpm13020361
Biesaga B, Mucha-Małecka A, Janecka-Widla A, Małecki K. Differences between Squamous Cell Carcinomas of the Base of the Tongue and the Tonsils in Prevalence of HPV16 Infection, Its Type, and Clinical Features. Journal of Personalized Medicine. 2023; 13(2):361. https://doi.org/10.3390/jpm13020361
Chicago/Turabian StyleBiesaga, Beata, Anna Mucha-Małecka, Anna Janecka-Widla, and Krzysztof Małecki. 2023. "Differences between Squamous Cell Carcinomas of the Base of the Tongue and the Tonsils in Prevalence of HPV16 Infection, Its Type, and Clinical Features" Journal of Personalized Medicine 13, no. 2: 361. https://doi.org/10.3390/jpm13020361