

Metallic Artifact Reduction in Midfacial CT Scans Using Patient-Specific Polymer Implants Enhances Image Quality
 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
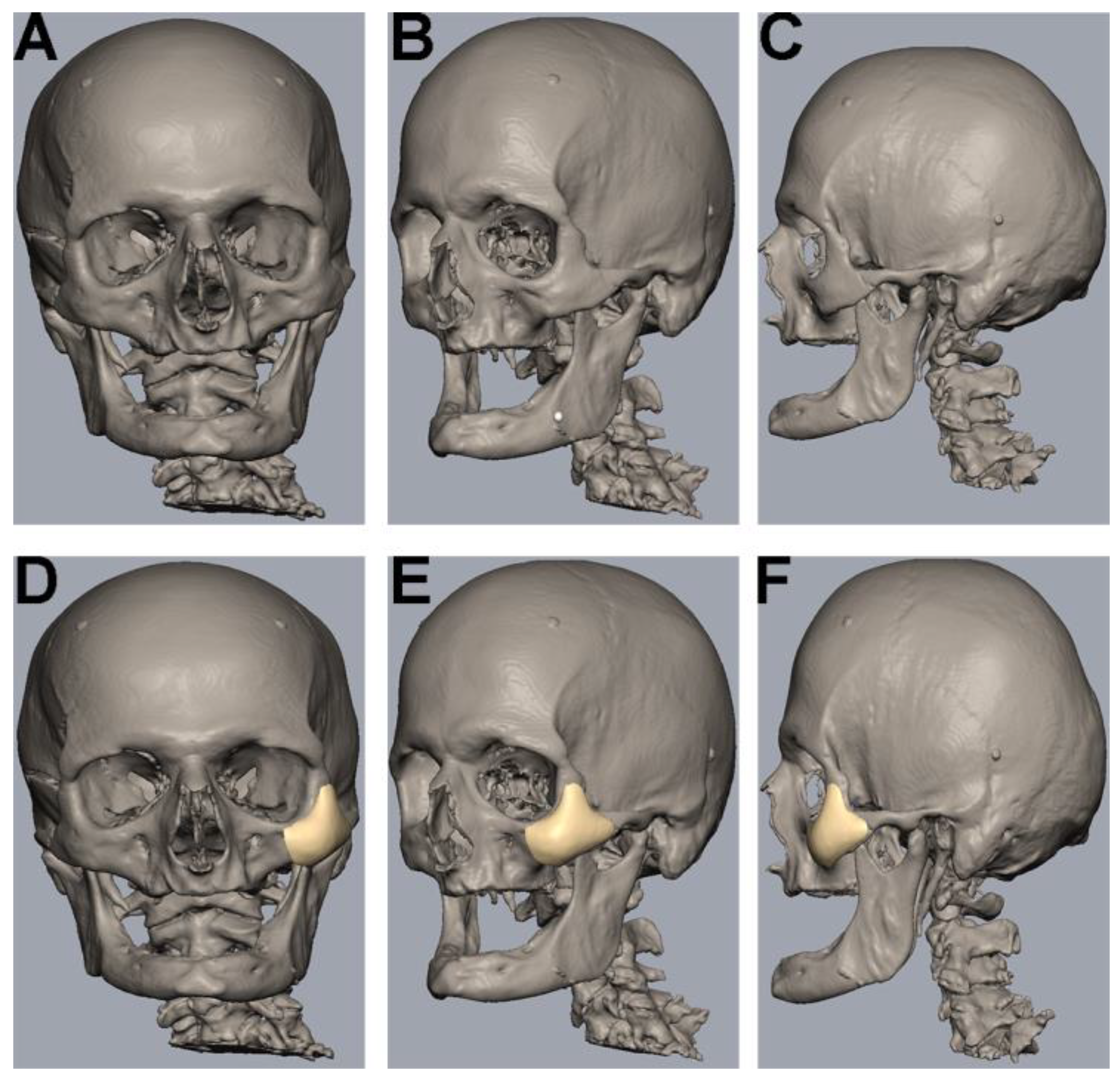
2.2. Human Cadaveric Specimen
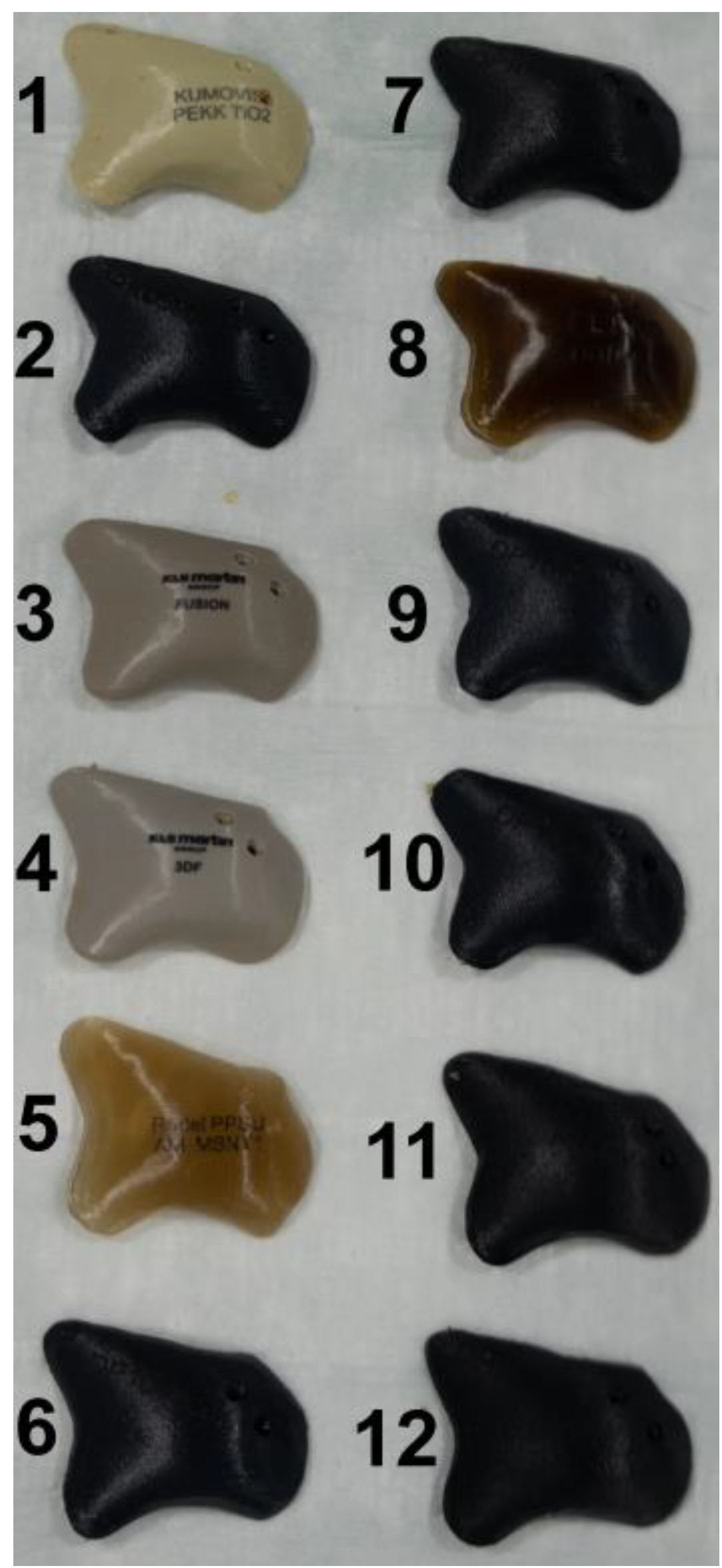
2.3. Virtual Planning and Manufacturing of Patient-Specific Implants
2.4. Preparation
2.5. Plates and Screws
2.6. Computer Tomography (CT) Image Acquisition
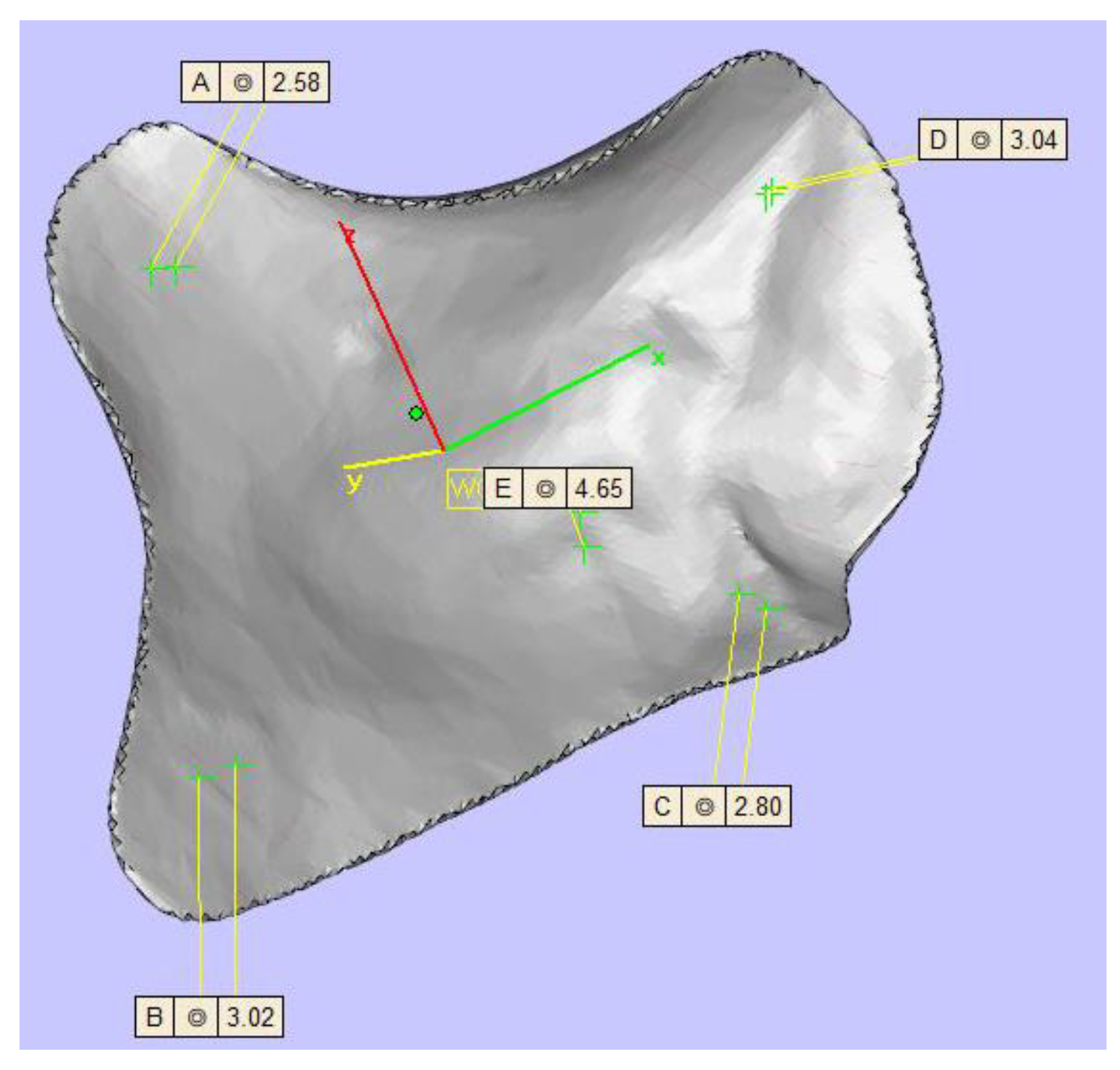
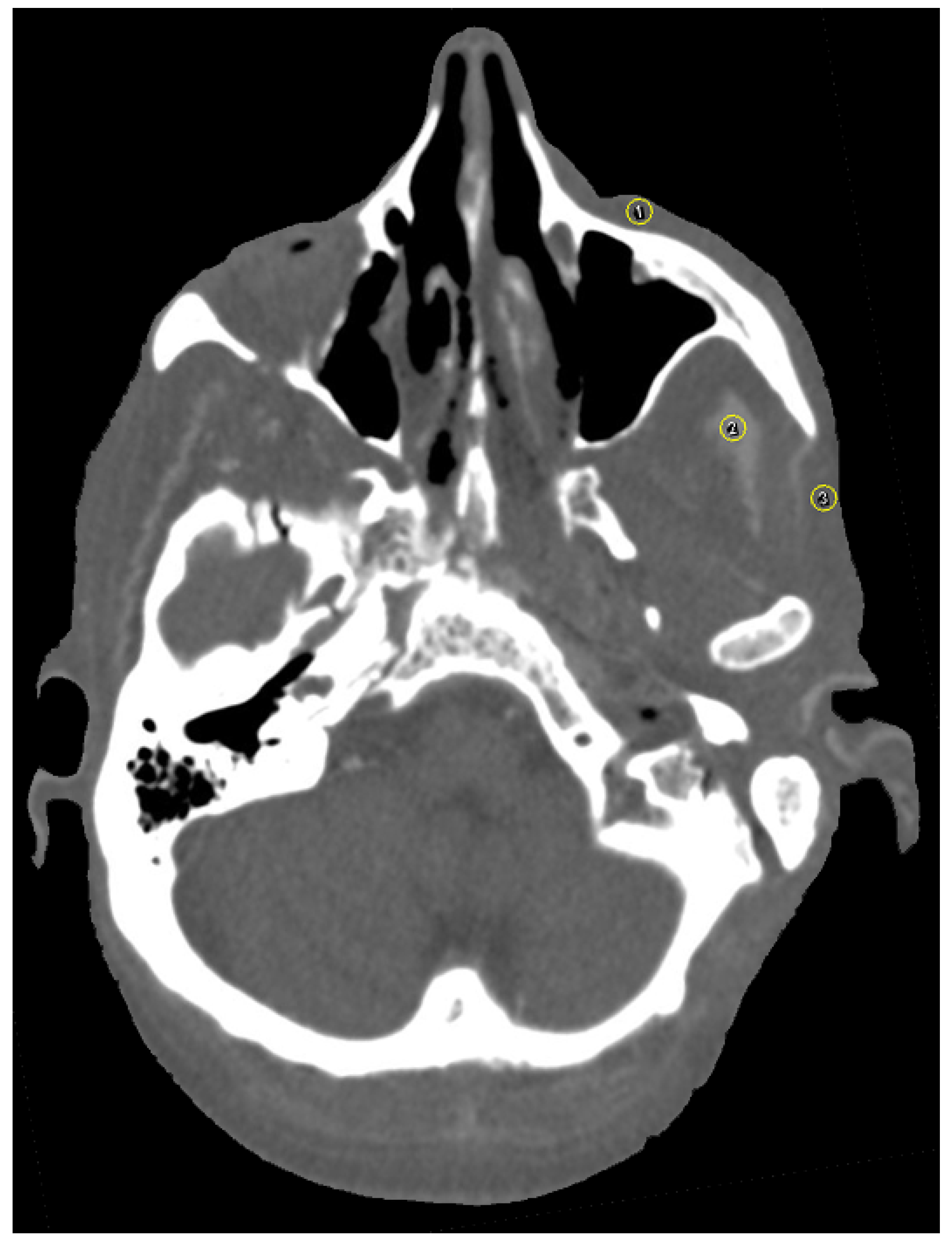
2.7. Image Analysis
2.8. Statistics
3. Results
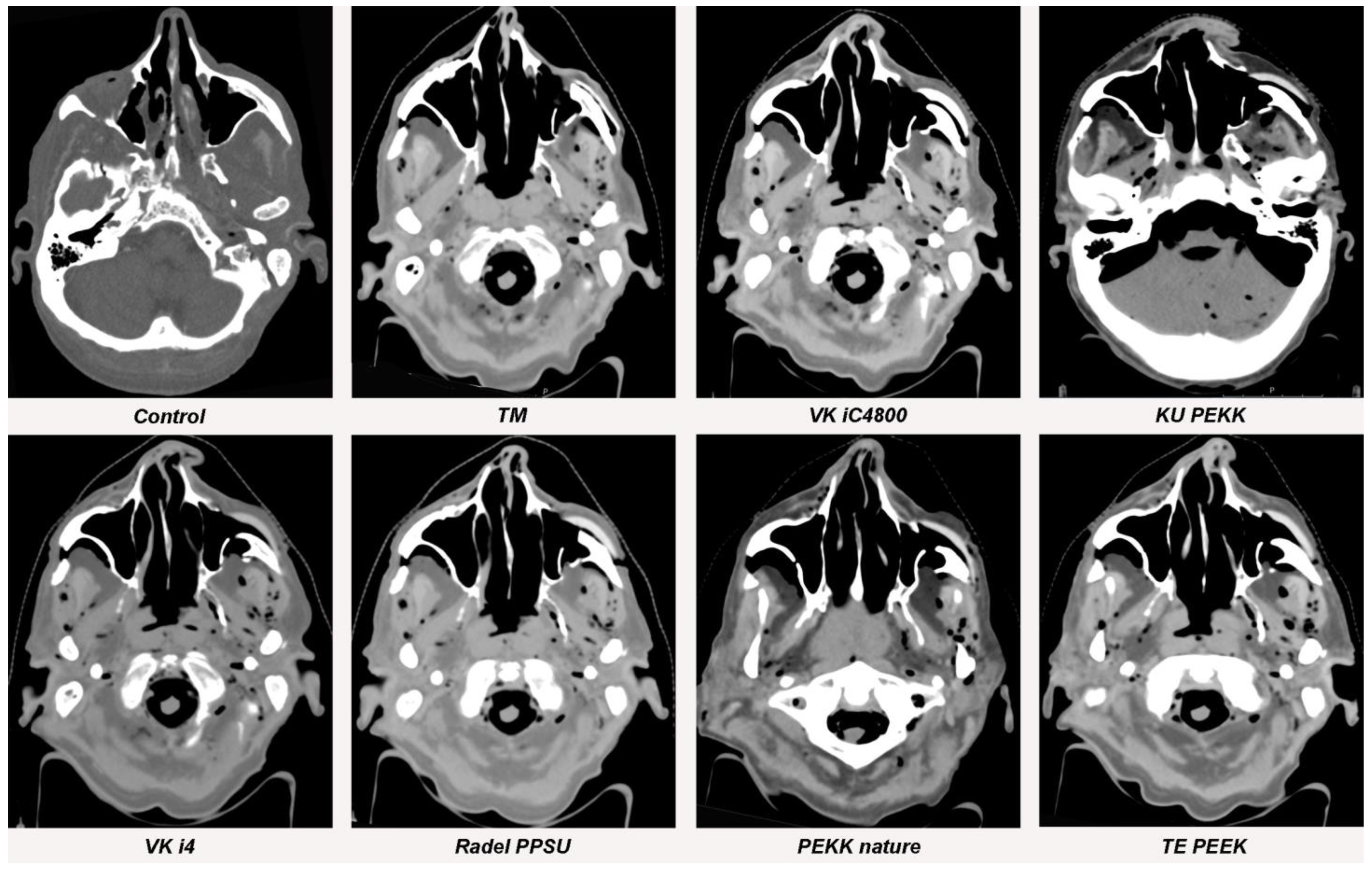
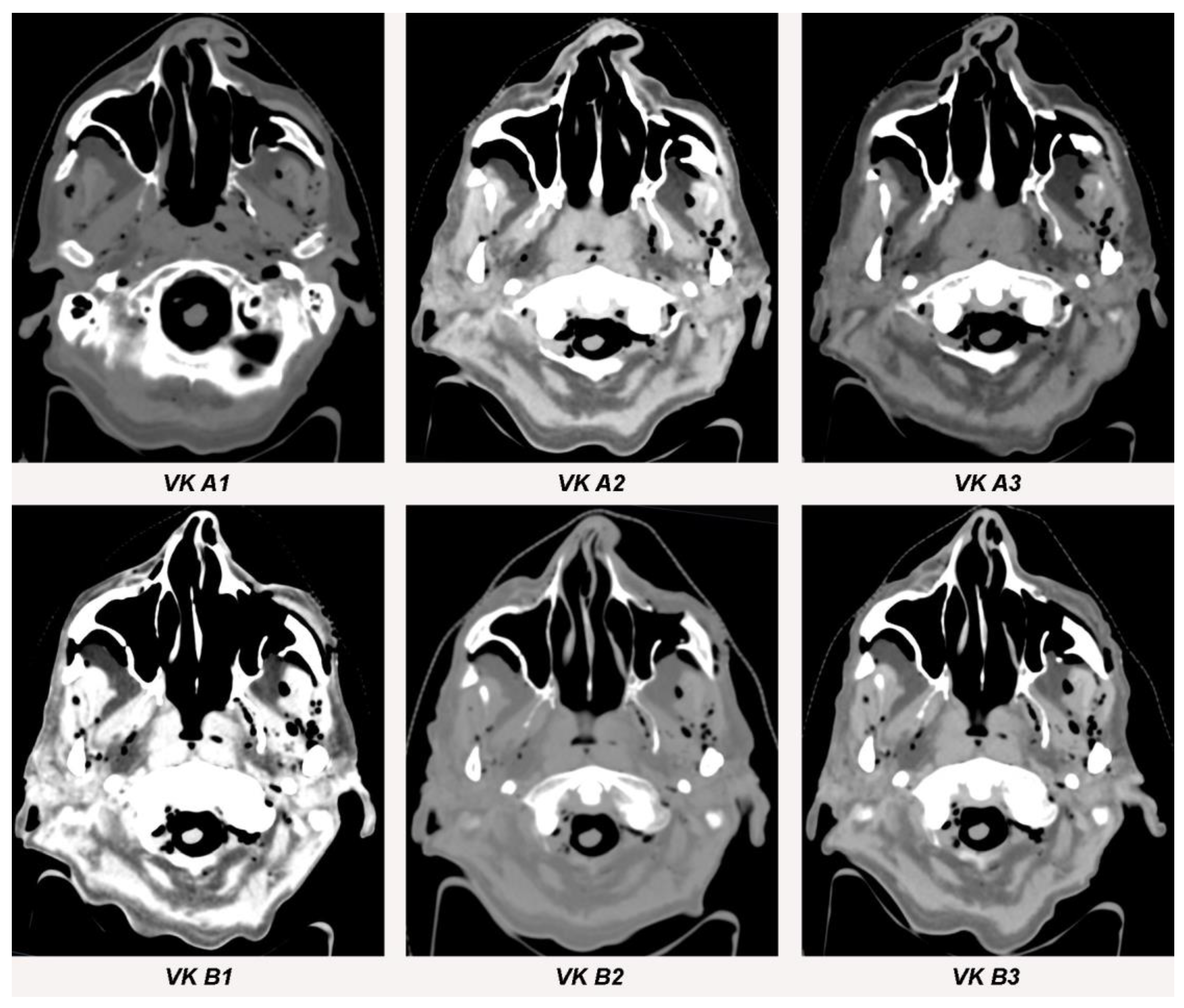
3.1. Streak Artifacts
3.1.1. Implant Material
3.1.2. Metallic Artifact Reduction Algorithm
3.2. Blooming Artifacts
3.2.1. Implant Material
3.2.2. Metallic Artifact Reduction Algorithm
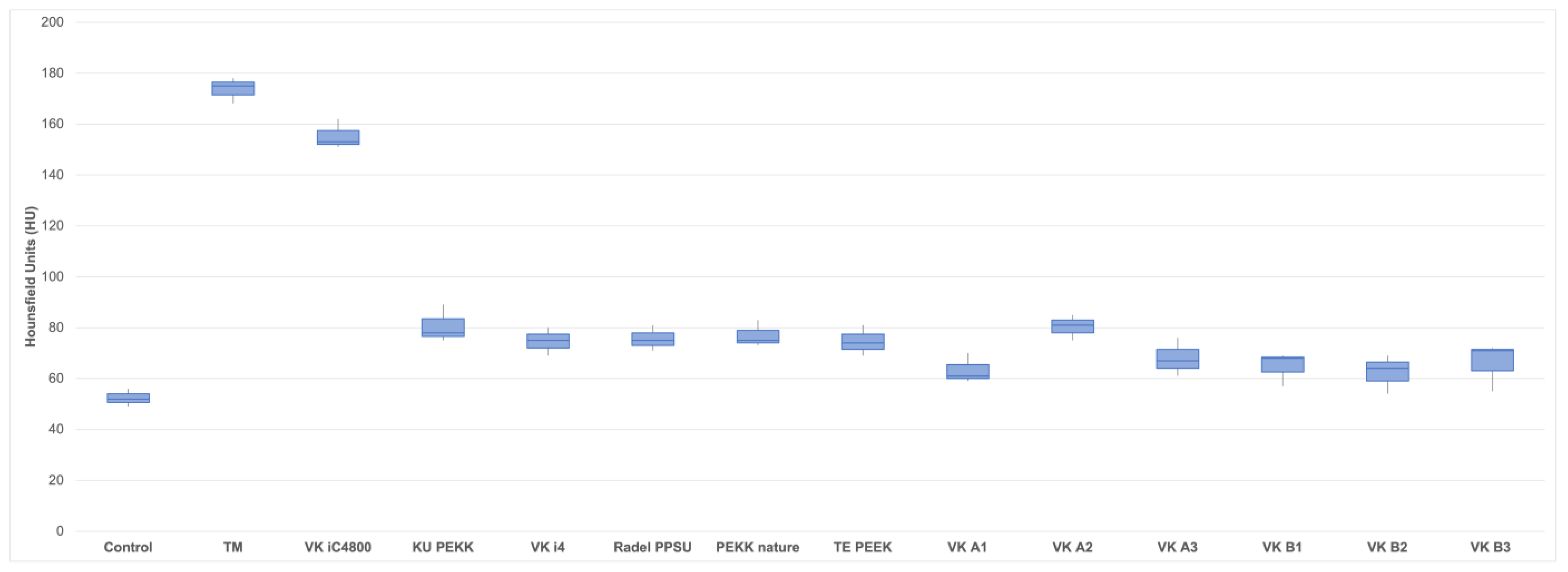
3.3. Image Quality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hinni, M.L.; Ferlito, A.; Brandwein-Gensler, M.S.; Takes, R.P.; Silver, C.E.; Westra, W.H.; Seethala, R.R.; Rodrigo, J.P.; Corry, J.; Bradford, C.R.; et al. Surgical margins in head and neck cancer: A contemporary review. Head Neck 2013, 35, 1362–1370. [Google Scholar] [CrossRef] [PubMed]
- Dort, J.C.; Farwell, D.G.; Findlay, M.; Huber, G.F.; Kerr, P.; Shea-Budgell, M.A.; Simon, C.; Uppington, J.; Zygun, D.; Ljungqvist, O.; et al. Optimal perioperative care in major head and neck cancer surgery with free flap reconstruction: A consensus review and recommendations from the enhanced recovery after surgery society. JAMA Otolaryngol. Head Neck Surg. 2017, 143, 292–303. [Google Scholar] [CrossRef] [Green Version]
- Cramer, J.D.; Burtness, B.; Le, Q.T.; Ferris, R.L. The changing therapeutic landscape of head and neck cancer. Nat. Rev. Clin. Oncol. 2019, 16, 669–683. [Google Scholar] [CrossRef]
- Goodson, A.M.; Kittur, M.A.; Evans, P.L.; Williams, E.M. Patient-specific, printed titanium implants for reconstruction of mandibular continuity defects: A systematic review of the evidence. J. Craniomaxillofac. Surg. 2019, 47, 968–976. [Google Scholar] [CrossRef] [PubMed]
- Eckstein, F.M.; Zeller, A.N.; Neuhaus, M.T.; Korn, P.; Gellrich, N.C.; Zimmerer, R.M.; Rahlf, B. Referencing for intraoperative navigation: Evaluation of human bias. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Cotic, M.; Vogt, S.; Hinterwimmer, S.; Feucht, M.J.; Slotta-Huspenina, J.; Schuster, T.; Imhoff, A.B. A matched-pair comparison of two different locking plates for valgus-producing medial open-wedge high tibial osteotomy: Peek-carbon composite plate versus titanium plate. Knee Surg Sports Traumatol. Arthrosc. 2015, 23, 2032–2040. [Google Scholar] [CrossRef] [PubMed]
- Fuss, M.; Sturtewagen, E.; De Wagter, C.; Georg, D. Dosimetric characterization of GafChromic EBT film and its implication on film dosimetry quality assurance. Phys. Med. Biol. 2007, 52, 4211–4225. [Google Scholar] [CrossRef]
- Paulis, L.E.; Kroll, J.; Heijnens, L.; Huijnen, M.; Gerretsen, R.; Backes, W.H.; Hofman, P.A.M. Is CT bulletproof? On the use of CT for characterization of bullets in forensic radiology. Int. J. Leg. Med. 2019, 133, 1869–1877. [Google Scholar] [CrossRef] [Green Version]
- Hünemohr, N.; Krauss, B.; Tremmel, C.; Ackermann, B.; Jäkel, O.; Greilich, S. Experimental verification of ion stopping power prediction from dual energy CT data in tissue surrogates. Phys. Med. Biol. 2014, 59, 83–96. [Google Scholar] [CrossRef]
- Glide-Hurst, C.; Chen, D.; Zhong, H.; Chetty, I.J. Changes realized from extended bit-depth and metal artifact reduction in CT. Med. Phys. 2013, 40, 061711. [Google Scholar] [CrossRef]
- Spadea, M.F.; Verburg, J.M.; Baroni, G.; Seco, J. The impact of low-Z and high-Z metal implants in IMRT: A Monte Carlo study of dose inaccuracies in commercial dose algorithms. Med. Phys. 2014, 41, 011702. [Google Scholar] [CrossRef] [PubMed]
- Laux, C.J.; Villefort, C.; Ehrbar, S.; Wilke, L.; Guckenberger, M.; Müller, D.A. Carbon fiber/polyether ether ketone (CF/PEEK) implants allow for more effective radiation in long bones. Materials 2020, 13, 1754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guzzini, M.; Lanzetti, R.M.; Lupariello, D.; Morelli, F.; Princi, G.; Perugia, D.; Ferretti, A. Comparison between carbon-peek plate and conventional stainless steal plate in ankle fractures. A prospective study of two years follow up. Injury 2017, 48, 1249–1252. [Google Scholar] [CrossRef] [PubMed]
- Ese, Z.; Zylka, W. Influence of 12-bit and 16-bit CT values of metals on dose calculation in radiotherapy using PRIMO, a Monte Carlo code for clinical linear accelerators. Curr. Dir. Biomed. Eng. 2019, 5, 597–600. [Google Scholar] [CrossRef] [Green Version]
- Lommen, J.; Schorn, L.; Sproll, C.; Haussmann, J.; Kübler, N.R.; Budach, W.; Rana, M.; Tamaskovics, B. Reduction of CT artifacts using polyetheretherketone (PEEK), polyetherketoneketone (PEKK), polyphenylsulfone (PPSU), and polyethylene (PE) reconstruction plates in oral oncology. J. Oral Maxillofac. Surg. 2022, 80, 1272–1283. [Google Scholar] [CrossRef] [PubMed]
- Lommen, J.; Schorn, L.; Sproll, C.; Kübler, N.R.; Nicolini, L.F.; Merfort, R.; Dilimulati, A.; Hildebrand, F.; Rana, M.; Greven, J. Mechanical fatigue performance of patient-specific polymer plates in oncologic mandible reconstruction. J. Clin. Med. 2022, 11, 3308. [Google Scholar] [CrossRef]
- Zanotti, B.; Zingaretti, N.; Verlicchi, A.; Robiony, M.; Alfieri, A.; Parodi, P.C. Cranioplasty: Review of materials. J. Craniofac. Surg. 2016, 27, 2061–2072. [Google Scholar] [CrossRef]
- Panayotov, I.V.; Orti, V.; Cuisinier, F.; Yachouh, J. Polyetheretherketone (PEEK) for medical applications. J. Mater. Sci. Mater. Med. 2016, 27, 118. [Google Scholar] [CrossRef]
- Nevelsky, A.; Borzov, E.; Daniel, S.; Bar-Deroma, R. Perturbation effects of the carbon fiber-PEEK screws on radiotherapy dose distribution. J. Appl. Clin. Med. Phys. 2017, 18, 62–68. [Google Scholar] [CrossRef]
- Neumann, A.; Unkel, C.; Werry, C.; Herborn, C.U.; Maier, H.R.; Ragoß, C.; Jahnke, K. Prototype of a silicon nitride ceramic-based miniplate osteofixation system for the midface. Otolaryngol. Head Neck Surg. 2006, 134, 923–930. [Google Scholar] [CrossRef]
- Ma, R.; Tang, T. Current strategies to improve the bioactivity of PEEK. Int. J. Mol. Sci. 2014, 15, 5426–5445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Guevelou, J.; Bastit, V.; Marcy, P.Y.; Lasne-Cardon, A.; Guzene, L.; Gerard, M.; Larnaudie, A.; Coutte, A.; Beddok, A.; Calugaru, V.; et al. Flap delineation guidelines in postoperative head and neck radiation therapy for head and neck cancers. Radiother. Oncol. 2020, 151, 256–265. [Google Scholar] [CrossRef] [PubMed]
- Grégoire, V.; Evans, M.; Le, Q.T.; Bourhis, J.; Budach, V.; Chen, A.; Eisbruch, A.; Feng, M.; Giralt, J.; Gupta, T.; et al. Delineation of the primary tumour Clinical Target Volumes (CTV-P) in laryngeal, hypopharyngeal, oropharyngeal and oral cavity squamous cell carcinoma: AIRO, CACA, DAHANCA, EORTC, GEORCC, GORTEC, HKNPCSG, HNCIG, IAG-KHT, LPRHHT, NCIC CTG, NCRI, NRG Oncology, PHNS, SBRT, SOMERA, SRO, SSHNO, TROG consensus guidelines. Radiother. Oncol. 2018, 126, 3–24. [Google Scholar]
- Barrett, J.F.; Keat, N. Artifacts in CT: Recognition and avoidance. Radiographics 2004, 24, 1679–1691. [Google Scholar] [CrossRef] [PubMed]
- Elliott, M.J.; Slakey, J.B. CT provides precise size assessment of implanted titanium alloy pedicle screws. Clin. Orthop. Relat. Res. 2014, 472, 1605–1609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasparek, M.F.; Töpker, M.; Lazar, M.; Weber, M.; Kasparek, M.; Mang, T.; Apfaltrer, P.; Kubista, B.; Windhager, R.; Ringl, H. Dual-energy CT and ceramic or titanium prostheses material reduce CT artifacts and provide superior image quality of total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1552–1561. [Google Scholar] [CrossRef] [Green Version]
- Tan, S.; Soulez, G.; Diez Martinez, P.; Larrivée, S.; Stevens, L.M.; Goussard, Y.; Mansour, S.; Chartrand-Lefebvre, C. Coronary stent artifact reduction with an edge-enhancing reconstruction kernel—A prospective cross-sectional study with 256-slice CT. PLoS ONE 2016, 11, e0154292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cicchetti, D.V. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 1994, 6, 284. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wayer, D.R.; Kim, N.Y.; Otto, B.J.; Grayev, A.M.; Kuner, A.D. Unintended consequences: Review of new artifacts introduced by iterative reconstruction CT metal artifact reduction in spine imaging. AJNR Am. J. Neuroradiol. 2019, 40, 1973–1975. [Google Scholar] [CrossRef]
- Ducic, Y. Midface reconstruction with titanium mesh and hydroxyapatite cement: A case report. J. Craniomaxillofac. Trauma 1997, 3, 35–39. [Google Scholar]
- Wei, J.; Luo, J.; Herrler, T.; Xu, H.; Deng, N.; Li, Q.; Dai, C. A simple technique for the correction of maxillonasal dysplasia using customized expanded polytetrafluoroethylene (ePTFE) implants. J. Plast. Reconstr. Aesthet. Surg. 2017, 70, 1292–1297. [Google Scholar] [CrossRef] [PubMed]
- Schaller, B.; Matthias Burkhard, J.P.; Chagnon, M.; Beck, S.; Imwinkelried, T.; Assad, M. Fracture healing and bone remodeling with human standard-sized magnesium versus polylactide-Co-glycolide plate and screw systems using a mini-swine craniomaxillofacial osteotomy fixation model. J. Oral. Maxillofac. Surg. 2018, 76, 2138–2150. [Google Scholar] [CrossRef] [PubMed]
- Pang, J.H.; Brooke, S.; Kubik, M.W.; Ferris, R.L.; Dhima, M.; Hanasono, M.M.; Wang, E.W.; Solari, M.G. Staged reconstruction (delayed-immediate) of the maxillectomy defect using CAD/CAM technology. J. Reconstr. Microsurg. 2018, 34, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.D.; Li, D.; Liu, Y.M.; Zhang, Z.D.; Fan, Y.D.; Shi, J.D.; Liu, S. Application of patient-specific PEEK implant for aesthetic considerations in paranasal augmentation. J. Craniofac. Surg. 2022, 33, e877–e880. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Kim, J.W.; Kim, S.J. Midfacial soft-tissue changes after paranasal augmentation with porous polyethylene. Fac. Plast. Surg. FPS 2016, 32, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Furness, S.; Glenny, A.-M.; Worthington, H.V.; Pavitt, S.; Oliver, R.; Clarkson, J.E.; Macluskey, M.; Chan, K.K.; I Conway, D.I. Interventions for the treatment of oral cavity and oropharyngeal cancer: Chemotherapy. Cochrane Database Syst. Rev. 2021, 12, Cd006386. [Google Scholar]
- Wang, K.; Zanation, A.M.; Chera, B.S. The role of radiation therapy in the management of sinonasal and ventral skull base malignancies. Otolaryngol. Clin. N. Am. 2017, 50, 419–432. [Google Scholar] [CrossRef]
- Wang, X.; Yang, J.N.; Li, X.; Tailor, R.; Vassilliev, O.; Brown, P.; Rhines, L.; Chang, E. Effect of spine hardware on small spinal stereotactic radiosurgery dosimetry. Phys. Med. Biol. 2013, 58, 6733–6747. [Google Scholar] [CrossRef] [PubMed]
- Mulder, S.L.; Heukelom, J.; McDonald, B.A.; Van Dijk, L.; Wahid, K.A.; Sanders, K.; Salzillo, T.C.; Hemmati, M.; Schaefer, A.; Fuller, C.D. MR-guided adaptive radiotherapy for OAR sparing in head and neck cancers. Cancers 2022, 14, 1909. [Google Scholar] [CrossRef] [PubMed]
- Byrne, M.; Archibald-Heeren, B.; Hu, Y.; Greer, P.; Luo, S.; Aland, T. Assessment of semi-automated stereotactic treatment planning for online adaptive radiotherapy in ethos. Med. Dosim. 2022, 47, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.Y.; Followill, D.S.; Howell, R.M.; Liu, X.; Mirkovic, D.; Stingo, F.C.; Kry, S.F. Approaches to reducing photon dose calculation errors near metal implants. Med. Phys. 2016, 43, 5117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pawałowski, B.; Ryczkowski, A.; Panek, R.; Sobocka-Kurdyk, U.; Graczyk, K.; Piotrowski, T. Accuracy of the doses computed by the Eclipse treatment planning system near and inside metal elements. Sci. Rep. 2022, 12, 5974. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Implant Material | Abbreviation | Manufacturer |
|---|---|---|
| Titanium Mesh | TM | KLS Martin Group®, Tuttlingen, Germany |
| VESTAKEEP iC4800 3DF | VK iC4800 | EVONIK Industries AG, Essen, Germany |
| KUMOVIS PEKK WHITE | KU PEKK | KUMOVIS GmbH, Munich, Germany |
| VESTAKEEP i4 3DF | VK i4 | EVONIK Industries AG, Essen, Germany |
| Radel PPSU AM MSNT1 | Radel PPSU | Solvay GmbH, Hannover, Germany |
| PEKK nature | PEKK nature | KUMOVIS GmbH, Munich, Germany |
| TECAFIL PEEK VX CF | TE PEEK | Ensinger GmbH, Nufringen, Germany |
| VESTAKEEP CF Filament-Fiber A1 | VK A1 | EVONIK Industries AG, Essen, Germany |
| VESTAKEEP CF Filament-Fiber A2 | VK A2 | EVONIK Industries AG, Essen, Germany |
| VESTAKEEP CF Filament-Fiber A3 | VK A3 | EVONIK Industries AG, Essen, Germany |
| VESTAKEEP CF Filament-Fiber B1 | VK B1 | EVONIK Industries AG, Essen, Germany |
| VESTAKEEP CF Filament-Fiber B2 | VK B2 | EVONIK Industries AG, Essen, Germany |
| VESTAKEEP CF Filament-Fiber B3 | VK B3 | EVONIK Industries AG, Essen, Germany |
| Implant Material | Abbreviation | Mean Standard Deviation (HU) | Differencea | p-Valuea |
|---|---|---|---|---|
| Titanium Mesh | TM | 173.7 (±5.1) | 121.3 (±5.4) | <0.001 * |
| VESTAKEEP iC4800 3DF | VK iC4800 | 155.3 (±5.9) | 103.0 (±4.2) | 0.007 * |
| KUMOVIS PEKK WHITE | KU PEKK | 80.7 (±7.4) | 28.3 (±8.5) | 0.084 |
| VESTAKEEP i4 3DF | VK i4 | 74.7 (±5.5) | 22.3 (±6.2) | 0.123 |
| Radel PPSU AM MSNT1 | Radel PPSU | 75.7 (±5.0) | 23.3 (±7.4) | 0.125 |
| PEKK nature | PEKK nature | 77.0 (±5.3) | 24.7 (±3.3) | 0.110 |
| TECAFIL PEEK VX CF | TE PEEK | 74.7 (±6.0) | 22.3 (±4.3) | 0.125 |
| VESTAKEEP CF Filament-Fiber A1 | VK A1 | 63.3 (±5.9) | 11.0 (±2.4) | 0.213 |
| VESTAKEEP CF Filament-Fiber A2 | VK A2 | 80.3 (±5.0) | 28.0 (±6.1) | 0.085 |
| VESTAKEEP CF Filament-Fiber A3 | VK A3 | 68.0 (±7.5) | 15.7 (±3.3) | 0.151 |
| VESTAKEEP CF Filament-Fiber B1 | VK B1 | 64.7 (±6.7) | 12.3 (±3.9) | 0.164 |
| VESTAKEEP CF Filament-Fiber B2 | VK B2 | 62.3 (±7.6) | 10.0 (±2.8) | 0.243 |
| VESTAKEEP CF Filament-Fiber B3 | VK B3 | 66.0 (±9.5) | 13.7 (±3.1) | 0.155 |
| Implant Material | Abbreviation | Real Diameter (mm) | CT Diameter (mm) | Virtual Growth (mm) | p Value | Image Qualitya |
|---|---|---|---|---|---|---|
| Titanium Mesh | TM | 0.45 | 0.5 (±0.5) | 0.05 (±0.5) | 0.987 | 2 |
| VESTAKEEP iC4800 3DF | VK iC4800 | 4.65 | 4.8 (±0.2) | 0.15 (±0.2) | 0.956 | 2 |
| KUMOVIS PEKK WHITE | KU PEKK | 4.65 | 4.8 (±0.3) | 0.15 (±0.3) | 0.956 | 2 |
| VESTAKEEP i4 3DF | VK i4 | 4.65 | 4.7 (±0.1) | 0.05 (±0.1) | 0.987 | 1 |
| Radel PPSU AM MSNT1 | Radel PPSU | 4.65 | 4.7 (±0.1) | 0.05 (±0.1) | 0.987 | 2 |
| PEKK nature | PEKK nature | 4.65 | 4,9 (±0.2) | 0.25 (±0.2) | 0.932 | 2 |
| TECAFIL PEEK VX CF | TE PEEK | 4.65 | 4.7 (±0.1) | 0.05 (±0.1) | 0.987 | 1 |
| VESTAKEEP CF Filament-Fiber A1 | VK A1 | 4.65 | 4.8 (±0.1) | 0.15 (±0.1) | 0.956 | 2 |
| VESTAKEEP CF Filament-Fiber A2 | VK A2 | 4.65 | 4.7 (±0.2) | 0.05 (±0.2) | 0.987 | 2 |
| VESTAKEEP CF Filament-Fiber A3 | VK A3 | 4.65 | 4.9 (±0.4) | 0.25 (±0.4) | 0.932 | 2 |
| VESTAKEEP CF Filament-Fiber B1 | VK B1 | 4.65 | 4.8 (±0.2) | 0.15 (±0.2) | 0.956 | 2 |
| VESTAKEEP CF Filament-Fiber B2 | VK B2 | 4.65 | 4.9 (±0.1) | 0.25 (±0.1) | 0.932 | 1 |
| VESTAKEEP CF Filament-Fiber B3 | VK B3 | 4.65 | 4.7 (±0.1) | 0.05 (±0.1) | 0.987 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lommen, J.; Schorn, L.; Sproll, C.; Kerkfeld, V.; Aksu, A.; Reinauer, F.; Kübler, N.R.; Budach, W.; Rana, M.; Tamaskovics, B. Metallic Artifact Reduction in Midfacial CT Scans Using Patient-Specific Polymer Implants Enhances Image Quality. J. Pers. Med. 2023, 13, 236. https://doi.org/10.3390/jpm13020236
Lommen J, Schorn L, Sproll C, Kerkfeld V, Aksu A, Reinauer F, Kübler NR, Budach W, Rana M, Tamaskovics B. Metallic Artifact Reduction in Midfacial CT Scans Using Patient-Specific Polymer Implants Enhances Image Quality. Journal of Personalized Medicine. 2023; 13(2):236. https://doi.org/10.3390/jpm13020236
Chicago/Turabian StyleLommen, Julian, Lara Schorn, Christoph Sproll, Valentin Kerkfeld, Adem Aksu, Frank Reinauer, Norbert R. Kübler, Wilfried Budach, Majeed Rana, and Bálint Tamaskovics. 2023. "Metallic Artifact Reduction in Midfacial CT Scans Using Patient-Specific Polymer Implants Enhances Image Quality" Journal of Personalized Medicine 13, no. 2: 236. https://doi.org/10.3390/jpm13020236