
Evaluation of Pretreatment Albumin–Bilirubin Grade as a Better Prognostic Factor Compared to Child–Pugh Classification in Patients with Hepatocellular Carcinoma Receiving Transarterial Chemoembolization Combined with Radiotherapy
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Treatments
2.3. Pretreatment Liver Function Assessment and Toxicity Follow-Up
2.4. Statistical Analysis
3. Results
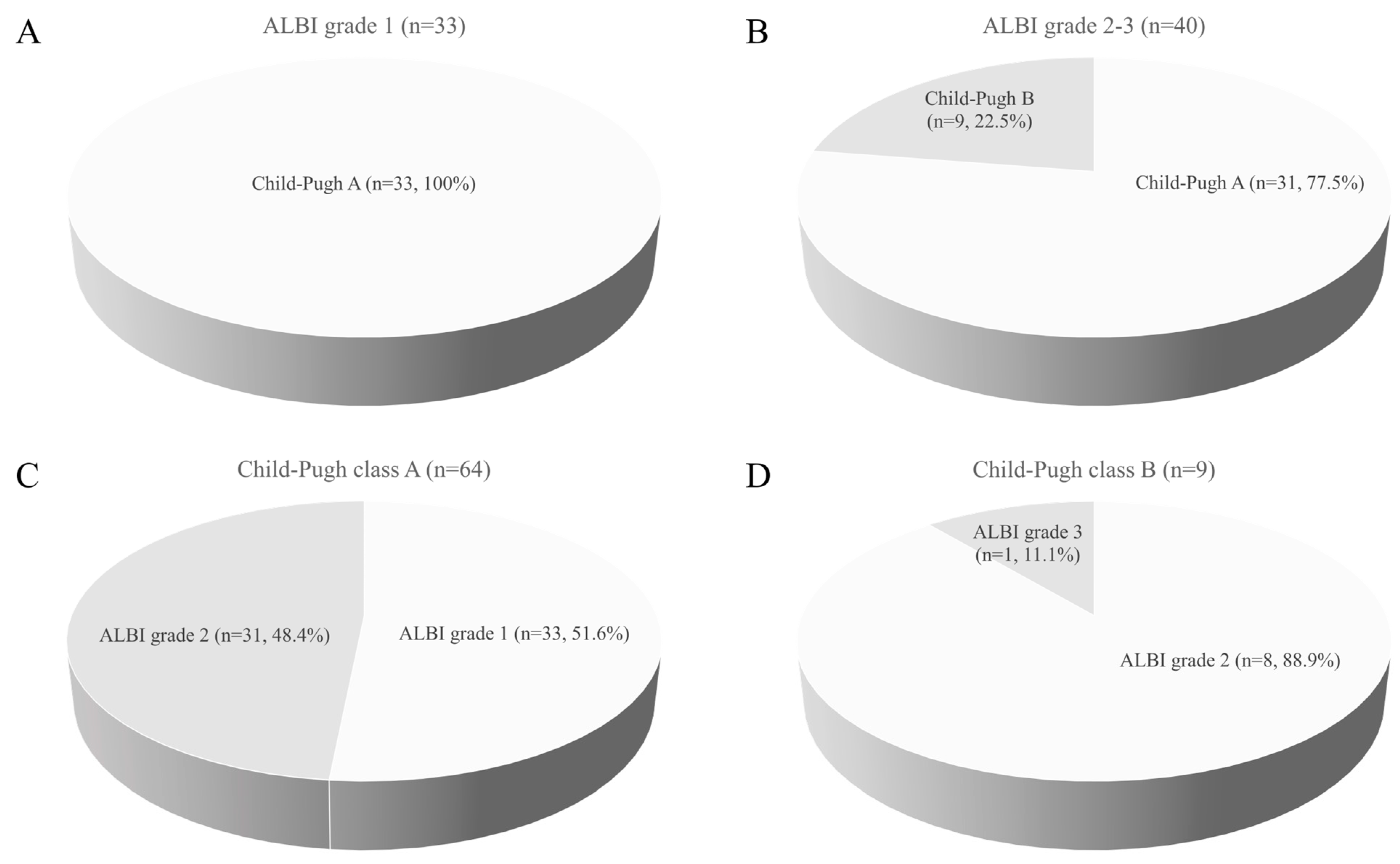
3.1. Patient Characteristics and Liver Function Assessment
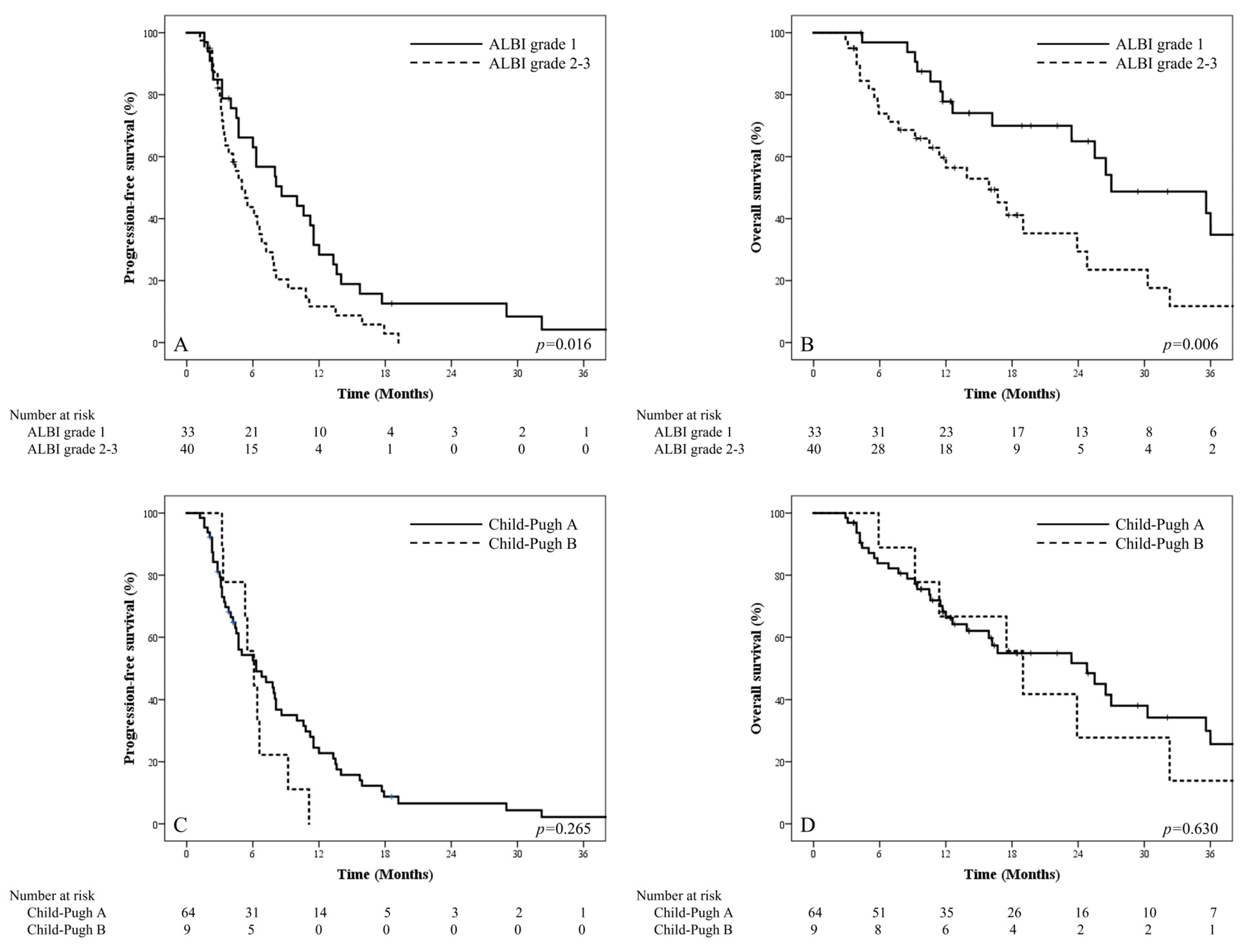
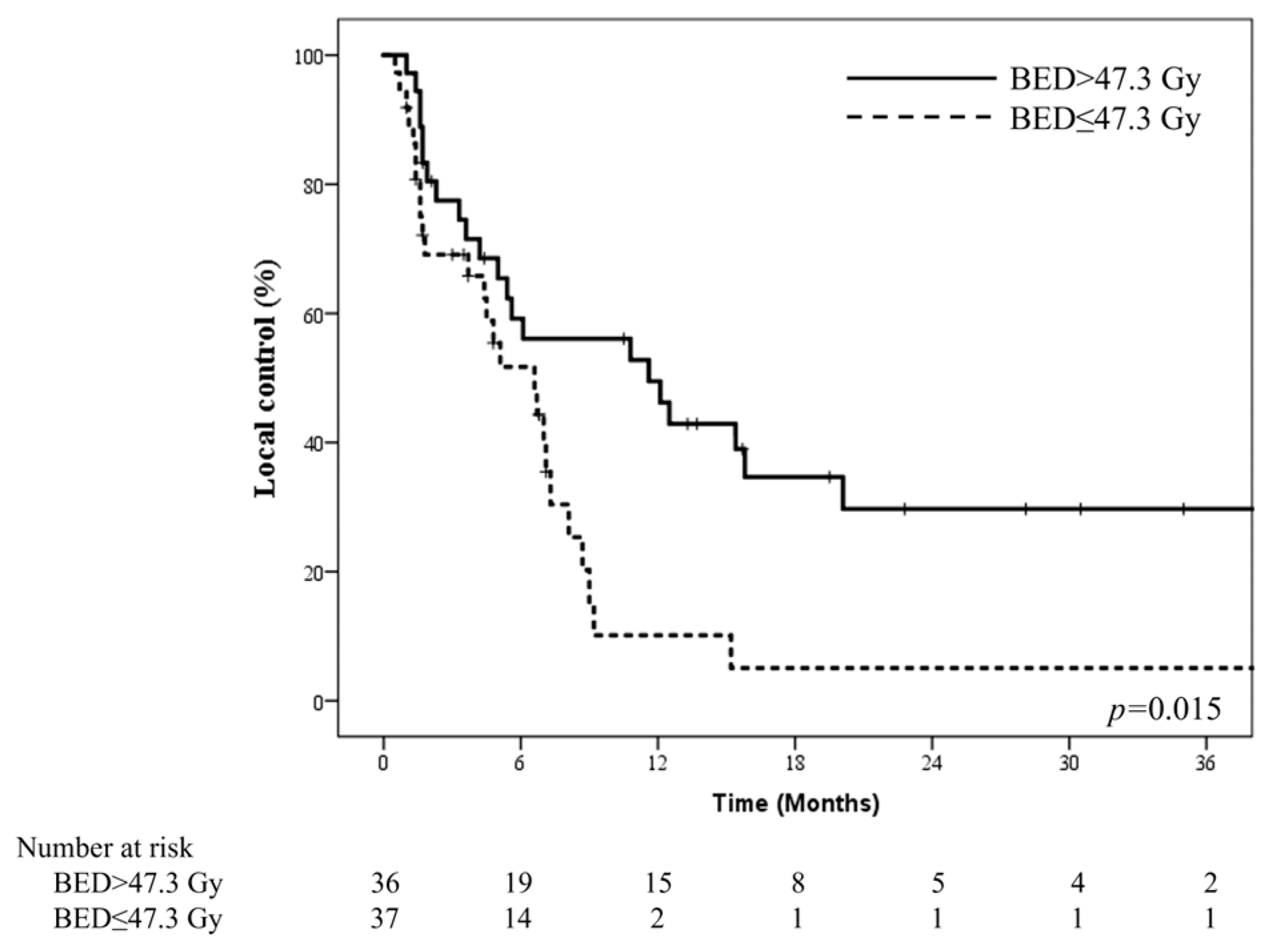
3.2. Survival Outcomes
3.3. Toxicity
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McGlynn, K.A.; Petrick, J.L.; El-Serag, H.B. Epidemiology of Hepatocellular Carcinoma. Hepatology 2021, 73 (Suppl. 1), 4–13. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valery, P.C.; Laversanne, M.; Clark, P.J.; Petrick, J.L.; McGlynn, K.A.; Bray, F. Projections of primary liver cancer to 2030 in 30 countries worldwide. Hepatology 2018, 67, 600–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golabi, P.; Fazel, S.; Otgonsuren, M.; Sayiner, M.; Locklear, C.T.; Younossi, Z.M. Mortality assessment of patients with hepatocellular carcinoma according to underlying disease and treatment modalities. Medicine 2017, 96, e5904. [Google Scholar] [CrossRef]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [Green Version]
- European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Omata, M.; Lesmana, L.A.; Tateishi, R.; Chen, P.-J.; Lin, S.-M.; Yoshida, H.; Kudo, M.; Lee, J.M.; Choi, B.I.; Poon, R.T.P.; et al. Asian Pacific Association for the Study of the Liver consensus recommendations on hepatocellular carcinoma. Hepatol. Int. 2010, 4, 439–474. [Google Scholar] [CrossRef] [Green Version]
- Bruix, J.; Sherman, M. Management of hepatocellular carcinoma: An update. Hepatology 2011, 53, 1020–1022. [Google Scholar] [CrossRef] [Green Version]
- Kok, B.; Abraldes, J.G. Child-Pugh Classification: Time to Abandon? Semin. Liver Dis. 2019, 39, 96–103. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Pinato, D.J.; Sharma, R.; Allara, E.; Yen, C.; Arizumi, T.; Kubota, K.; Bettinger, D.; Jang, J.W.; Smirne, C.; Kim, Y.W.; et al. The ALBI grade provides objective hepatic reserve estimation across each BCLC stage of hepatocellular carcinoma. J. Hepatol. 2017, 66, 338–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foerster, F.; Galle, P.R. Comparison of the current international guidelines on the management of HCC. JHEP Rep. 2019, 1, 114–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foerster, F.; Galle, P.R. Hepatocellular carcinoma: One world, one cancer-different guidelines? Hepatobiliary Surg. Nutr. 2018, 7, 41–43. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.P. Role of Radiotherapy in the Treatment of Hepatocellular Carcinoma. J. Clin. Transl. Hepatol. 2019, 7, 183–190. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.-A.; Shim, J.H.; Yoon, S.M.; Jung, J.; Kim, J.H.; Ryu, M.-H.; Ryoo, B.-Y.; Kang, Y.-K.; Lee, D.; Kim, K.M.; et al. Comparison of chemoembolization with and without radiation therapy and sorafenib for advanced hepatocellular carcinoma with portal vein tumor thrombosis: A propensity score analysis. J. Vasc. Interv. Radiol. 2015, 26, 320–329.e6. [Google Scholar] [CrossRef]
- Cho, J.-Y.; Paik, Y.-H.; Park, H.C.; Yu, J.I.; Sohn, W.; Gwak, G.-Y.; Choi, M.S.; Lee, J.H.; Koh, K.C.; Paik, S.W.; et al. The feasibility of combined transcatheter arterial chemoembolization and radiotherapy for advanced hepatocellular carcinoma. Liver Int. 2014, 34, 795–801. [Google Scholar] [CrossRef]
- Yi, J.W.; Hong, H.P.; Kim, M.S.; Shin, B.S.; Kwon, H.J.; Kim, B.I.; Sohn, W. Comparison of Clinical Efficacy and Safety between 70–150 microm and 100–300 microm Doxorubicin Drug-Eluting Bead Transarterial Chemoembolization for Hepatocellular Carcinoma. Life 2022, 12, 297. [Google Scholar]
- Sohn, W.; Ham, C.B.; Kim, N.H.; Kim, H.J.; Cho, Y.K.; Jeon, W.K.; Kim, B.I. Effect of acute kidney injury on the patients with hepatocellular carcinoma undergoing transarterial chemoembolization. PLoS ONE 2020, 15, e0243780. [Google Scholar] [CrossRef]
- Korean Liver Cancer Study Group (KLCSG); National Cancer Center, Korea (NCC). 2014 Korean Liver Cancer Study Group-National Cancer Center Korea practice guideline for the management of hepatocellular carcinoma. Korean J. Radiol. 2015, 16, 465–522. [Google Scholar] [CrossRef] [Green Version]
- Korean Liver Cancer Association; National Cancer Center. 2018 Korean Liver Cancer Association-National Cancer Center Korea Practice Guidelines for the Management of Hepatocellular Carcinoma. Gut Liver 2019, 13, 227–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pugh, R.N.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, T.S.; Robertson, J.M.; Anscher, M.S.; Jirtle, R.L.; Ensminger, W.D.; Fajardo, L.F. Hepatic toxicity resulting from cancer treatment. Int. J. Radiat. Oncol. Biol. Phys. 1995, 31, 1237–1248. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.C.; Kavanagh, B.D.; Dawson, L.A.; Li, X.A.; Das, S.K.; Miften, M.; Haken, R.K.T. Radiation-associated liver injury. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S94–S100. [Google Scholar] [CrossRef] [Green Version]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [Green Version]
- Hiraoka, A.; Kumada, T.; Michitaka, K.; Kudo, M. Newly Proposed ALBI Grade and ALBI-T Score as Tools for Assessment of Hepatic Function and Prognosis in Hepatocellular Carcinoma Patients. Liver Cancer 2019, 8, 312–325. [Google Scholar] [CrossRef]
- Demirtas, C.O.; D’Alessio, A.; Rimassa, L.; Sharma, R.; Pinato, D.J. ALBI grade: Evidence for an improved model for liver functional estimation in patients with hepatocellular carcinoma. JHEP Rep. 2021, 3, 100347. [Google Scholar] [CrossRef]
- Soeters, P.B.; Wolfe, R.R.; Shenkin, A. Hypoalbuminemia: Pathogenesis and Clinical Significance. JPEN J. Parenter. Enteral. Nutr. 2019, 43, 181–193. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Li, P.; Lu, J.; Xiong, W.; Oger, J.; Tetzlaff, W.; Cynader, M. Bilirubin possesses powerful immunomodulatory activity and suppresses experimental autoimmune encephalomyelitis. J. Immunol. 2008, 181, 1887–1897. [Google Scholar] [CrossRef] [Green Version]
- Matsukane, R.; Watanabe, H.; Hata, K.; Suetsugu, K.; Tsuji, T.; Egashira, N.; Nakanishi, Y.; Okamoto, I.; Ieiri, I. Prognostic significance of pre-treatment ALBI grade in advanced non-small cell lung cancer receiving immune checkpoint therapy. Sci. Rep. 2021, 11, 15057. [Google Scholar] [CrossRef]
- Takada, K.; Takamori, S.; Shimokawa, M.; Toyokawa, G.; Shimamatsu, S.; Hirai, F.; Tagawa, T.; Okamoto, T.; Hamatake, M.; Tsuchiya-Kawano, Y.; et al. Assessment of the albumin-bilirubin grade as a prognostic factor in patients with non-small-cell lung cancer receiving anti-PD-1-based therapy. ESMO Open 2022, 7, 100348. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, M.A.; Dawson, L.A. Radiation therapy for hepatocellular carcinoma: From palliation to cure. Cancer 2006, 106, 1653–1663. [Google Scholar] [CrossRef] [PubMed]
- Fuss, M.; Salter, B.J.; Herman, T.S.; Thomas, C.R., Jr. External beam radiation therapy for hepatocellular carcinoma: Potential of intensity-modulated and image-guided radiation therapy. Gastroenterology 2004, 127, S206–S217. [Google Scholar] [CrossRef] [PubMed]
- Park, H.C.; Yu, J.I.; Cheng, J.C.-H.; Zeng, Z.C.; Hong, J.H.; Wang, M.L.C.; Kim, M.S.; Chi, K.H.; Liang, P.-C.; Lee, R.-C.; et al. Consensus for Radiotherapy in Hepatocellular Carcinoma from The 5th Asia-Pacific Primary Liver Cancer Expert Meeting (APPLE 2014): Current Practice and Future Clinical Trials. Liver Cancer 2016, 5, 162–174. [Google Scholar] [CrossRef]
- Shim, S.J.; Seong, J.; Han, K.H.; Chon, C.Y.; Suh, C.O.; Lee, J.T. Local radiotherapy as a complement to incomplete transcatheter arterial chemoembolization in locally advanced hepatocellular carcinoma. Liver Int. 2005, 25, 1189–1196. [Google Scholar] [CrossRef]
- Yoon, S.M.; Ryoo, B.Y.; Lee, S.J.; Kim, J.H.; Shin, J.H.; An, J.H.; Lee, H.C.; Lim, Y.S. Efficacy and Safety of Transarterial Chemoembolization Plus External Beam Radiotherapy vs. Sorafenib in Hepatocellular Carcinoma With Macroscopic Vascular Invasion: A Randomized Clinical Trial. JAMA Oncol. 2018, 4, 661–669. [Google Scholar] [CrossRef]
- Huo, Y.R.; Eslick, G.D. Transcatheter Arterial Chemoembolization Plus Radiotherapy Compared With Chemoembolization Alone for Hepatocellular Carcinoma: A Systematic Review and Meta-analysis. JAMA Oncol. 2015, 1, 756–765. [Google Scholar] [CrossRef]
- Mohammed, M.A.A.; Khalaf, M.H.; Liang, T.; Wang, D.S.; Lungren, M.P.; Rosenberg, J.; Kothary, N. Albumin-Bilirubin Score: An Accurate Predictor of Hepatic Decompensation in High-Risk Patients Undergoing Transarterial Chemoembolization for Hepatocellular Carcinoma. J. Vasc. Interv. Radiol. 2018, 29, 1527–1534.e1. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.-H.; Liu, M.-Y.; Lee, M.-S.; Yang, J.-F.; Jen, Y.-M.; Lin, C.-S.; Chao, H.-L.; Shen, P.-C.; Huang, W.-Y. Comparison Between Child-Turcotte-Pugh and Albumin-Bilirubin Scores in Assessing the Prognosis of Hepatocellular Carcinoma After Stereotactic Ablative Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 145–152. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 73) | ALBI Grade 1 (n = 33) | ALBI Grade 2–3 (n = 40) | ALBI Grade 1 vs. Grade 2–3 | |
|---|---|---|---|---|
| Characteristic | No. of Patients (%)/ Median (Range) | No. of Patients (%)/ Median (Range) | No. of Patients (%)/ Median (Range) | p Value |
| Gender | 1.000 | |||
| Male | 70 (95.9) | 32 (97.0) | 38 (95.0) | |
| Female | 3 (4.1) | 1 (3.0) | 2 (5.0) | |
| Age at TACE+RT (year) | 62 (27–88) | 64 (26–88) | 61 (39–83) | 0.807 |
| ECOG | 0.040 | |||
| 0–1 | 56 (76.7) | 29 (87.9) | 27 (67.5) | |
| 2–3 | 17 (23.3) | 4 (12.1) | 13 (32.5) | |
| Etiology | 0.697 | |||
| B-viral | 51 (69.9) | 25 (75.8) | 26 (65.0) | |
| C-viral | 6 (8.2) | 1 (3.0) | 5 (12.5) | |
| Non-B, Non-C | 13 (17.8) | 5 (15.2) | 8 (20.0) | |
| Alcoholic | 3 (4.1) | 2 (6.1) | 1 (2.5) | |
| Underlying liver cirrhosis | 0.102 | |||
| Yes | 48 (65.8) | 25 (75.8) | 23 (57.5) | |
| No | 25 (34.2) | 8 (24.2) | 17 (42.5) | |
| mUICC stage | 0.205 | |||
| 1 | 1 (1.4) | 0 (0.0) | 1 (2.5) | |
| 2 | 7 (9.6) | 5 (15.2) | 2 (5.0) | |
| 3 | 23 (31.5) | 12 (36.4) | 11 (27.5) | |
| 4A | 42 (57.5) | 16 (48.5) | 26 (65.0) | |
| Pre-TACE AFP (ng/mL) | 80.3 (1.3–60,500.0) | 14.1 (1.3–24,707.0) | 129.6 (2.1–60,500.0) | 0.029 |
| Pre-TACE PIVKA-II (mAU/mL) | 496.5 (13.0–300,000.0) | 397.0 (13.0–75,000.0) | 554.0 (15.0–300,000.0) | 0.570 |
| Previous resection | 0.233 | |||
| Yes | 7 (9.6) | 5 (15.2) | 2 (5.0) | |
| No | 66 (90.4) | 28 (84.8) | 38 (95.0) | |
| No. of previous TACE &/or RFA | 0.473 | |||
| 0 | 33 (45.2) | 12 (36.4) | 21 (52.5) | |
| 1 | 17 (23.3) | 8 (27.3) | 9 (22.5) | |
| 2 | 6 (8.2) | 3 (9.1) | 3 (7.5) | |
| 3 | 4 (5.5) | 4 (12.1) | 0 (0.0) | |
| ≥4 | 13 (17.8) | 6 (18.2) | 7 (17.5) | |
| Pre-TACE Child-Pugh grade | 0.003 | |||
| A | 64 (87.7) | 33 (100.0) | 31 (77.5) | |
| B | 9 (12.3) | 0 (0.0) | 9 (22.5) | |
| RT dose (Total) (Gy) | 35.0 (15.0–54.0) | 40.0 (20.0–48.0) | 35.0 (15.0–54.0) | 0.416 |
| RT dose (BED10) (Gy) | 47.3 (19.5–105.6) | 56.0 (30.0–105.6) | 47.3 (19.5–70.2) | 0.084 |
| TACE-RT interval (weeks) | 6.6 (1.0–21.7) | 7.4 (2.0–20.0) | 6.1 (1.0–21.7) | 0.395 |
| Causes | No. of patients (%) |
| PVTT | 29 (39.7) |
| Incomplete TACE | 24 (32.9) |
| Regional LN metastasis | 4 (5.5) |
| Other vessel invasions | 3 (4.1) |
| Combination of the above-mentioned causes | 13 (17.8) |
| RT sites | No. of patients (%) |
| Tumor thrombus | 31 (42.5) |
| Liver parenchyma | 28 (38.4) |
| Regional LN alone | 1 (1.4) |
| Liver parenchyma + Tumor thrombi | 9 (12.3) |
| Liver parenchyma + Regional LNs | 3 (4.1) |
| Liver parenchyma + Regional LN + Tumor thrombus | 1 (1.4) |
| Progression-Free Survival | Overall Survival | |||||||
|---|---|---|---|---|---|---|---|---|
| UVA | MVA | UVA | MVA | |||||
| Variable | Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value |
| Age at TACE+RT ≤60 vs. >60 | 0.571 (0.338–0.964) | 0.036 | 0.670 (0.387–1.162) | 0.154 | 1.029 (0.549–1.927) | 0.930 | - | - |
| Gender | 1.122 (0.346–3.632) | 0.848 | - | - | 2.077 (0.633–6.818) | 0.228 | - | - |
| ECOG 0–1 vs. 2–3 | 1.201 (0.680–2.122) | 0.527 | - | - | 1.399 (0.696–2.818) | 0.346 | - | - |
| mUICC stage 1–3 vs. 4A | 1.640 (0.997–2.698) | 0.051 | 1.394 (0.825–2.354) | 0.215 | 2.703 (1.374–5.319) | 0.004 | 2.472 (1.251–4.885) | 0.009 |
| Pre-TACE AFP (ng/mL) ≤80 vs. >80 | 1.518 (0.921–2.503) | 0.102 | - | - | 1.108 (0.597–2.059) | 0.745 | - | - |
| Pre-TACE PIVKA-II (mAU/mL) ≤496.5 vs. >496.5 | 1.305 (0.748–2.278) | 0.349 | - | - | 1.150 (0.558–2.370) | 0.705 | - | - |
| Pre-TACE Child-Pugh grade | 1.503 (0.727–3.107) | 0.272 | - | - | 1.222 (0.540–2.768) | 0.631 | - | - |
| Pre-TACE ALBI grade 1 vs. 2–3 | 1.840 (1.111–3.049) | 0.018 | 1.728 (1.038–2.875) | 0.035 | 2.411 (1.256–4.628) | 0.008 | 2.161 (1.124–4.156) | 0.021 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.J.B.; Park, J.S.; Hong, H.P.; Kim, M.S.; Koo, D.-H.; Lee, H.; Nam, H. Evaluation of Pretreatment Albumin–Bilirubin Grade as a Better Prognostic Factor Compared to Child–Pugh Classification in Patients with Hepatocellular Carcinoma Receiving Transarterial Chemoembolization Combined with Radiotherapy. J. Pers. Med. 2023, 13, 354. https://doi.org/10.3390/jpm13020354
Lee JJB, Park JS, Hong HP, Kim MS, Koo D-H, Lee H, Nam H. Evaluation of Pretreatment Albumin–Bilirubin Grade as a Better Prognostic Factor Compared to Child–Pugh Classification in Patients with Hepatocellular Carcinoma Receiving Transarterial Chemoembolization Combined with Radiotherapy. Journal of Personalized Medicine. 2023; 13(2):354. https://doi.org/10.3390/jpm13020354
Chicago/Turabian StyleLee, Jason Joon Bock, Jun Su Park, Hyun Pyo Hong, Myung Sub Kim, Dong-Hoe Koo, Hyebin Lee, and Heerim Nam. 2023. "Evaluation of Pretreatment Albumin–Bilirubin Grade as a Better Prognostic Factor Compared to Child–Pugh Classification in Patients with Hepatocellular Carcinoma Receiving Transarterial Chemoembolization Combined with Radiotherapy" Journal of Personalized Medicine 13, no. 2: 354. https://doi.org/10.3390/jpm13020354