

Archival Human Temporal Bone: Anatomical and Histopathological Studies of Cochlear Implantation
Abstract
:1. Introduction
2. Anatomic Considerations: Morphometric Linear and Angular Measurements of the Human Cochlea and the Spiral Ganglion Neurons (SGN)
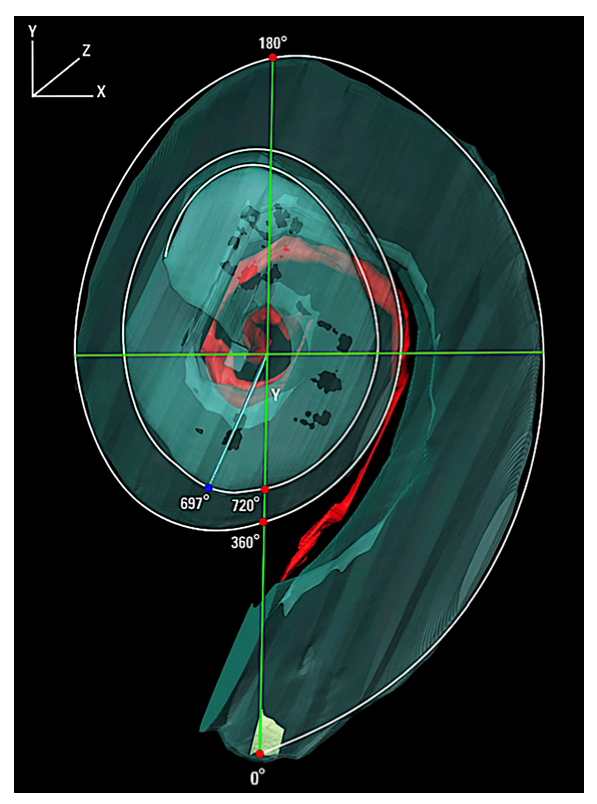
2.1. Angular Measurements of the Human Cochlea in CI Patients Using 3-Dimensional Reconstruction
2.2. Linear Measurements of the Human Cochlea and the Relevance to CI Design
2.3. Interindividual Variability in Cochlear Duct Linear Length and Angular Length
3. Studies of New Tissue Formation in the Human Temporal Bone from Patients with a History of CI
3.1. The Relationship of New Tissue Formation and CI Performance
3.1.1. The Role of Cochlear Hydrops in the Implanted Patient
3.1.2. The Role of Vestibular Hydrops in the Implanted Patient
3.2. Macrophage and Microglial Immune Response to Cochlear Implantation and Subtypes Involved in New Tissue Formation
4. Factors Affecting Fibrosis and Osteoneogenesis Following Cochlear Implantation
4.1. New Tissue Formation and CI Performance
4.2. Evaluating the Effect of Translocation Injury and Other Factors Associated with Higher Degrees of Intracochlear Damage
4.3. Evaluating the Foreign Body Reaction and New Tissue Formation in Human Temporal Bones with Cochlear Implantation
5. Surgical Approaches and Other Factors Affecting Intracochlear Injury
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brown, C.; Gifford, R.H. Expansion of audiological criteria for pediatric cochlear implantation. Otolaryngol. Clin. N. Am. 2021, 54, 1181. [Google Scholar] [CrossRef] [PubMed]
- Danielian, A.; Ishiyama, G.; Lopez, I.A.; Ishiyama, A. Morphometric linear and angular measurements of the human cochlea in implant patients using 3-dimensional reconstruction. Hear Res. 2020, 386, 107874. [Google Scholar] [CrossRef] [PubMed]
- Koch, R.W.; Ladak, H.M.; Elfarnawany, M.; Agrawal, S.K. Measuring cochlear duct length—A historical analysis of methods and results. J. Otolaryngol. Head Neck Surg. 2017, 46, 19–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takagi, A.; Sando, I. Computer-aided three-dimensional reconstruction: A method of measuring temporal bone structures including the length of the cochlea. Ann. Otol. Rhinol. Laryngol. 1989, 98, 515–522. [Google Scholar] [CrossRef]
- Verbist, B.M.; Skinner, M.W.; Cohen, L.T.; Leake, P.A.; James, C.; Boex, C.; Holden, T.A.; Finley, C.C.; Roland, P.S.; Roland, J.T., Jr.; et al. Consensus panel on a cochlear coordinate system applicable in histologic, physiologic, and radiologic studies of the human cochlea. Otol. Neurotol. 2010, 31, 722–730. [Google Scholar] [CrossRef] [Green Version]
- Ariyasu, L.; Galey, F.; Hilsinger, R.; Byl, F. Computer generated three-dimensional reconstruction of the cochlea. Otolaryngol. Head Neck Surg. 1989, 100, 87–91. [Google Scholar] [CrossRef]
- Kawano, A.; Seldon, H.L.; Clark, G.M. Computer-aided three-dimensional reconstruction in human cochlear maps: Measurement of the lengths of organ of Corti, outer wall and Rosenthal’s canal. Ann. Otol. Rhinol. Laryngol. 1996, 105, 701–709. [Google Scholar] [CrossRef] [Green Version]
- Avci, E.; Nauwelaers, T.; Lenarz, T.; Hamacher, V.; Kral, A. Variations in microanatomy of the human cochlea. J. Comp. Neurol. 2014, 522, 3245–3261. [Google Scholar] [CrossRef] [Green Version]
- Stakhovskaya, O.; Sridhar, D.; Bonham, B.H.; Leake, P.A. Frequency map for the human cochlear spiral ganglion: Implications for cochlear implants. J. Assoc. Res. Otolaryngol. 2007, 8, 220–233. [Google Scholar] [CrossRef] [Green Version]
- Greenwood, D. Critical bandwidth and the frequency coordinates of the basilar membrane. J. Acoust. Soc. Am. 1961, 33, 1344–1356. [Google Scholar] [CrossRef]
- Kamakura, T.; Nadol, J.B., Jr. Correlation between word recognition score and intracochlear new bone and fibrous tissue after cochlear implantation in the human. Hear Res. 2016, 339, 132–141. [Google Scholar] [CrossRef] [Green Version]
- Linthicum, F.H., Jr.; Fayad, J.; Otto, S.R.; Galey, F.R.; House, W.F. Cochlear implant histopathology. Am. J. Otol. 1991, 12, 245–311. [Google Scholar] [CrossRef]
- Seyyedi, M.; Nadol, J.B., Jr. Intracochlear inflammatory response to cochlear implant electrodes in humans. Otol. Neurotol. 2014, 35, 1545–1551. [Google Scholar] [CrossRef] [Green Version]
- Fayad, J.; Makarem, A.O.; Linthicum, F.H. Histopathological assessment of fibrosis and new bone formation in implanted human temporal bones using 3-dimensional reconstruction. Otolaryngol. Head Neck Surg. 2009, 141, 247–252. [Google Scholar] [CrossRef] [Green Version]
- Nadol, J.B., Jr. Patterns of neural degeneration in the human cochlea and auditory nerve: Implications for cochlear implantation. Otolaryngol. Head Neck Surg. 1997, 117, 220–228. [Google Scholar] [CrossRef]
- Danielian, A.; Ishiyama, G.; Lopez, I.A.; Ishiyama, A. Predictors of fibrotic and bone tissue formation with 3-D reconstructions of post-implantation human temporal bones. Otol. Neurotol. 2021, 42, e942–e948. [Google Scholar] [CrossRef]
- Handzel, O.; Burgess, B.J.; Nadol, J.B., Jr. Histopathology of the peripheral vestibular system after cochlear implantation in the human. Otol. Neurotol. 2005, 27, 57–64. [Google Scholar] [CrossRef]
- Hodge, S.E.; Ishiyama, G.; Lopez, I.A.; Ishiyama, A. Histopathologic analysis of temporal bones with otosclerosis following cochlear implantation. Otol. Neurotol. 2021, 42, 1492–1498. [Google Scholar] [CrossRef]
- Ishiyama, A.; Doherty, J.; Ishiyama, G.; Quesnel, A.; Lopez, I.A.; Linthicum, F.H. Post hybrid cochlear implant hearing loss and endolymphatic hydrops. Otol. Neurotol. 2016, 37, 1516–1521. [Google Scholar] [CrossRef] [Green Version]
- Ishiyama, A.; Ishiyama, G.; Lopez, I.A.; Linthicum, F.H. Temporal bone histopathology of first-generation cochlear implant electrode translocation. Otol. Neurotol. 2019, 40, e581–e591. [Google Scholar] [CrossRef]
- Knoll, R.M.; Trakimas, D.R.; Wu, M.J.; Lubner, R.J.; Nadol, J.B., Jr.; Ishiyama, A.; Santos, F.; Jung, D.H.; Remenschneider, A.K.; Kozin, E.D. Intracochlear new fibro-ossification and neuronal degeneration following cochlear implant electrode translocation: Long-term histopathological findings in humans. Otol. Neurotol. 2022, 43, e153–e164. [Google Scholar] [CrossRef] [PubMed]
- Li, P.M.M.C.; Somdas, M.A.; Eddington, D.K.; Nadol, J.B., Jr. Analysis of intracochlear new bone and fibrous tissue formation in human subjects with cochlear implantation. Ann. Otol. Rhinol. Laryngol. 2007, 116, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Okayasu, T.; Quesnel, A.M.; O’Malley, J.T.; Kamakura, T.; Nadol, J.B., Jr. The distribution and prevalence of macrophages in the cochlea following cochlear implantation in human: An immunohistochemical study using anti-Iba1 antibody. Otol. Neurotol. 2020, 41, e304–e316. [Google Scholar] [CrossRef] [PubMed]
- Quesnel, A.M.; Nakajima, H.H.; Rosowski, J.J.; Hansen, M.R.; Gantz, B.; Nadol, J.B., Jr. Delayed loss of hearing after hearing preservation cochlear implantation: Human temporal bone pathology and implication for etiology. Hear Res. 2016, 333, 325–334. [Google Scholar] [CrossRef] [Green Version]
- Su-Velez, B.M.; Lopez, I.A.; Ishiyama, A.; Ishiyama, G. Human temporal bone study of vestibular histopathology in cochlear implant patients with cochlear hydrops. Otol. Neurotol. 2020, 41, e607–e614. [Google Scholar] [CrossRef]
- Trakimas, D.R.; Kozin, E.D.; Ghanad, I.; Nadol, J.B., Jr.; Remenschneider, A.K. Human otopathologic findings in cases of folded cochlear implant electrodes. Otol. Neurotol. 2018, 39, 970–978. [Google Scholar] [CrossRef]
- Richard, C.; Fayad, J.N.; Doherty, J.; Linthicum, F.H., Jr. Round window versus cochleostomy technique in cochlear implantation: Histologic findings. Otol. Neurotol. 2012, 33, 1181–1187. [Google Scholar] [CrossRef] [Green Version]
- Alonso, J.E.; Ishiyama, G.; Fujiwara, R.J.T.; Pham, N.; Ledbetter, L.; Ishiyama, A. Cochlear Meniere’s: A distinct clinical entity with isolated cochlear hydrops on high-resolution MRI? Front. Surg. 2021, 8, 680260. [Google Scholar] [CrossRef]
- Enticott, J.C.; Tari, S.; Koh, S.M.; Dowell, R.C.; O’Leary, S.J. Cochlear implant and vestibular function. Otol. Neurotol. 2006, 27, 824–830. [Google Scholar] [CrossRef]
- Hänsel, T.; Gauger, U.; Bernhard, N.; Behzadi, N.; Romo, V.M.G.; Hofmann, V.; Olze, J.; Knopke, S.; Todt, I.; Cooders, A.; et al. Meta-analysis of subjective complaints of vertigo and vestibular tests after cochlear implantation. Laryngoscope 2018, 128, 2110–2123. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, I.; Da Silva, S.D.; Segal, B.; Zeitouni, A. Effect of cochlear implant surgery on vestibular function. Meta-analysis study. J. Otolaryngol. Head Neck Surg. 2017, 46, 44. [Google Scholar] [CrossRef] [Green Version]
- Buchman, C.A.; Joy, J.; Hodges, A.; Telischi, F.F.; Balkany, T.J. Vestibular effects of cochlear implantation. Laryngoscope 2004, 114, 1–22. [Google Scholar] [CrossRef]
- Fina, M.; Skinner, M.; Goebel, J.A.; Piccirillo, J.F.; Neely, J.G. Vestibular dysfunction after cochlear implantation. Otol. Neurotol. 2003, 24, 234–242. [Google Scholar] [CrossRef]
- Nadol, J.B., Jr.; O’Malley, J.T.; Burgess, B.J.; Galler, D. Cellular immunologic responses to cochlear implantation in human. Hear Res. 2014, 318, 11–17. [Google Scholar] [CrossRef] [Green Version]
- O’Malley, J.T.; Nadol, J.B., Jr.; McKenna, M.J. Anti CD163+, Iba1+, and CD68+ cells in the adult human inner ear—Normal distribution of an unappreciated class of macrophages/ microglia and implications for inflammatory otopathology in humans. Otol. Neurotol. 2016, 37, 99–108. [Google Scholar] [CrossRef] [Green Version]
- Noonan, K.Y.; Lopez, I.A.; Ishiyama, G.; Ishiyama, A. Immune response of macrophage population to cochlear implantation: Cochlea immune cells. Otol. Neurotol. 2020, 41, 1288–1295. [Google Scholar] [CrossRef]
- Liu, W.; Molnar, M.; Garnham, C.; Benav, H.; Rask-Anderson, H. Macrophages in the human cochlea: Saviors or predators—A study using super-resolution immunohistochemistry. Front. Immunol. 2018, 9, 223. [Google Scholar] [CrossRef] [Green Version]
- Okayasu, T.; O’Malley, J.T.; Nadol, J.B., Jr. Density of macrophages immunostained with anti-Iba1 antibody in the vestibular endorgans after cochlear implantation in the human. Otol. Neurotol. 2019, 40, e774–e781. [Google Scholar] [CrossRef]
- Okayasu, T.; O’Malley, J.T.; Nadol, J.B., Jr. Prevalence of macrophages within the cochlear vessels following cochlear implantation in the human: An immunohistopathological study using anti-Iba1 antibody. Otol. Neurotol. 2021, 42, e1470–e1477. [Google Scholar] [CrossRef]
- Kawano, A.; Seldon, H.L.; Clark, G.M.; Ramsden, R.T.; Raine, C.H. Intracochlear factors contributing to psychophysical percepts following cochlear implantation. Acta Otolaryngol. 1998, 118, 313–326. [Google Scholar]
- Choi, C.; Oghalai, J. Predicting the effect of post-implant cochlear fibrosis on residual hearing. Hear Res. 2005, 205, 193–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishai, R.; Herrmann, B.S.; Nadol, J.B.; Quesnel, A.M. The pattern and degree of capsular fibrous sheaths surrounding cochlear electrode arrays. Hear Res. 2017, 348, 44–53. [Google Scholar] [CrossRef] [Green Version]
- Nadol, J.B.; Shiao, J.; Burgess, B.; Ketten, D.R.; Eddington, D.K.; Gantz, B.J.; Kos, I.; Montandon, P.; Coker, N.J.; Roland, J.T., Jr.; et al. Histopathology of cochlear implants in humans. Ann. Otol. Rhinol. Laryngol. 2001, 110, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Lehnhardt, E. Intracochlear placement of cochlear implant electrodes in soft surgery technique. HNO 1993, 41, 356–359. [Google Scholar] [PubMed]
- Carlson, M.L.; Driscoll, C.L.; Gifford, R.H.; Service, G.J.; Tombers, N.M.; Hughes-Borst, B.J.; Neff, B.A.; Beatty, C.W. Implications of minimizing trauma during conventional cochlear implantation. Otol. Neurotol. 2011, 32, 962–968. [Google Scholar] [CrossRef] [Green Version]
- Eisenhut, F.; Lang, S.; Taha, L.; Hoelter, P.; Wiesmueller, M.; Uder, M.; Iro, H.; Doerfler, A.; Homung, J. Identification of anatomic risk factors for scalar translocation in cochlear implant patients. Z. Med. Phys. 2021, 31, 254–264. [Google Scholar] [CrossRef]
- O’Malley, J.T.; Burgess, B.J.; Galler, D.; Nadol, J.B., Jr. Foreign body response to silicone in cochlear implant electrodes in the human. Otol. Neurotol. 2017, 38, 970–977. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Studies Using Reconstruction | Number Temporal Bones | Method | SGN Angular Length | Rosenthal’s Canal (RC) Length of SGN | Inner Wall Alongside SGN | Outer Wall Alongside SGN | Total Cochlear Duct (CD) | % RC/CD Length and Angular |
|---|---|---|---|---|---|---|---|---|
| Ariyasu et al. [6] | 2 | 3D from H&E 25 µm light microscopy | 1.75 turns (630°) | |||||
| Kawano et al. [7] | 8 | 3D reconstruction from H&E 3 µm light microscopy | 1.75 to 2 turns (630°–720°) | 14.73–18.38 mm (X = 15.98 mm) | 945°–1080° 37.9–43.8 mm | 41–49.8% length | ||
| Avci et al. [8] | 16 fresh frozen | Micro CT dimensional analysis using MATLAB | 1.4 to 1.7 turns (510°–615°) | 859°–1024° | ||||
| Stakhovskaya et al. [9] | 9 | Serial surface preparations 1% osmium tetroxide | 1.75 to 2 turns (630°–720°) | 12.54–14.62 mm (X = 13.69 mm) | 14.35–16.33 mm (X = 15.49 mm) | 30.5–36.87 mm (X = 33.13 mm) (Measured at Organ of Corti) | 40–43 % length X = 41% | |
| Danielian et al. [2] | 15 | 3D reconstruction from H&E 20 µm light microscopy | 1.9 to 1.95 X = 695° | 14.44–16.97 mm X = 15.9 mm | 16.34–18.92 mm X = 17.9 mm | 31.38 –36.44 mm X = 34.5 mm | 876°–1052° X = 947° 35.4–43.6 mm | 34–46% length X = 40% 65–80% Angular X = 74% |
| All studies | Nearly 2 turns | 14.3 mm to 18.4 mm | ~18 mm | ~35 mm | 35 to 44 mm | ~40% length ~74% angular |
| Studies | Methodology | Main Findings |
|---|---|---|
| Danielian et al. [16] | 15 HTB | Years of implantation is a predictor of osteoneogenesis but not fibrosis. Cochleostomy is associated with greater new tissue formation compared with round window. |
| Fayad et al. [14] | 10 HTB histopathology | New tissue formation was negatively associated with spiral ganglion neuronal counts in the basal cochlea |
| Handzel et al. [17] | 17 HTB | 59% of the implanted had cochlear hydrops with most of these having a collapse of the saccule. Scarpa’s ganglion neuronal counts were unchanged from contralateral unimplanted (n = 8). |
| Hodge et al. [18] | 13 implanted HTB and 4 contralateral unimplanted in otosclerosis | Cochleostomy is associated with increased new tissue formation and osteoneogenesis. |
| Ishiyama et al. [19] | 29 HTB histopathology | All 17 bones with cochlear hydrops had implantation by cochleostomy. Fibrosis near the ductus reuniens was associated with cochlear hydrops. Round window technique was associated with minimal fibrosis and was not associated with hydrops. |
| Ishiyama et al. [20] | 13 HTB with translocation 6 with localized cochlear damage and 7 with translocation and lateral wall damage | Translocation with lateral wall injury (n = 7) was associated with lower SGN counts, poorer speech performance, and more abundant new tissue formation than localized translocation (n = 6). In 6/7, there was severe hydrops. All 7 had placement by cochleostomy with relatively longer electrode. Translocation tended to occur at about 180°. |
| Kamakura and Nadol [11] | 17 HTB histopathology | 17 / 17 had fibrous tissue and new bone formation. Positive correlation between SGN count and speech scores. % Volume of new tissue increased with damage to the basilar membrane. |
| Knoll et al. [21] | 19 HTB with translocation | Average angle of translocation was 159.2° which was associated with fibroosseous changes and lower SGN counts |
| Li et al. [22] | 12 HTB | Fibroosseous change in 12/ 12 and greater if there was lateral wall damage. |
| Linthicum et al. [12] | 22 HTB from 13 patients | All had varied amount of fibrosis, and some had ossification, mostly basal. One HTB 14 years post implantation. |
| Okayasu et al. [23] | 20 HTB from 10 patients with unilateral CI | Iba1+ macrophages within the fibrous sheath surrounding the electrode with phagocytosis of foreign material. Multinucleated foreign body giant cells along electrode track. |
| Quesnel et al. [24] | HTB 8 years after Iowa/Nucleus Hybrid S8 with history of delayed loss of residual low frequency hearing at 18 weeks postoperative | Deposition of fibrous tissue and osteoid in the basal turn may cause cochlear mechanical changes. Cochlear hydrops was noted. Organ of Corti and SGN similar to unimplanted contralateral side. |
| Seyyedi and Nadol [13] | 28 HTB from 21 patients | 96,4% had varying degrees of new tissue formation. 25% had eosinophilic infiltrate. Foreign-body giant cell formation and lymphocytic infiltration at cochleostomy site and electrodes. |
| Su-Velez et al. [25] | 15 HTB from CI patients with histopathology of cochlear hydrops (Meniere’s disease excluded) | 22.2% had semicircular hydrops 72% had saccular hydrops 33.3% had utricular hydrops of which all had delayed presentation of vertigo/dizziness |
| Trakimas et al. [26] | 4 HTB with folded tip | Folded electrodes were associated with greater volume of osseous tissue and lowered SGN counts. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishiyama, P.; Ishiyama, G.; Lopez, I.A.; Ishiyama, A. Archival Human Temporal Bone: Anatomical and Histopathological Studies of Cochlear Implantation. J. Pers. Med. 2023, 13, 352. https://doi.org/10.3390/jpm13020352
Ishiyama P, Ishiyama G, Lopez IA, Ishiyama A. Archival Human Temporal Bone: Anatomical and Histopathological Studies of Cochlear Implantation. Journal of Personalized Medicine. 2023; 13(2):352. https://doi.org/10.3390/jpm13020352
Chicago/Turabian StyleIshiyama, Paul, Gail Ishiyama, Ivan A. Lopez, and Akira Ishiyama. 2023. "Archival Human Temporal Bone: Anatomical and Histopathological Studies of Cochlear Implantation" Journal of Personalized Medicine 13, no. 2: 352. https://doi.org/10.3390/jpm13020352