
Sex Differences in the Treatment of Uveal Melanoma in a Group of 1336 Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources, Patients, and Definitions
2.2. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Jovanovic, P.; Mihajlovic, M.; Djordjevic-Jocic, J.; Vlajkovic, S.; Cekic, S.; Stefanovic, V. Ocular melanoma: An overview of the current status. Int. J. Clin. Exp. Pathol. 2013, 6, 1230–1244. [Google Scholar]
- Tan, L.L.Y.; Hong, J.; Goh, W.L.; Chang, E.W.Y.; Yang, V.S.; Poon, E.; Somasundaram, N.; Farid, M.; Chan, A.S.Y.; Chan, J.Y. Clinical features and survival outcomes of ocular melanoma in a multi-ethnic Asian cohort. Sci. Rep. 2020, 10, 16367. [Google Scholar] [CrossRef]
- Kaliki, S.; Shields, C.L. Uveal melanoma: Relatively rare but deadly cancer. Eye 2017, 31, 241–257. [Google Scholar] [CrossRef] [Green Version]
- Virgili, G.; Gatta, G.; Ciccolallo, L.; Capocaccia, R.; Biggeri, A.; Crocetti, E.; Lutz, J.-M.; Paci, E.; EUROCARE Working Group. Incidence of Uveal Melanoma in Europe. Ophthalmology 2007, 114, 2309–2315. [Google Scholar] [CrossRef]
- Nowak, M.; Romanowska-Dixon, B.; Grabska-Liberek, I.; Żurek, M. Incidence and Characteristics of Retinoblastoma in Poland: The First Nationwide Study 2010–2017. Int. J. Environ. Res. Public Health 2021, 18, 6539. [Google Scholar] [CrossRef]
- Ortega, M.A.; Fraile-Martínez, O.; García-Honduvilla, N.; Coca, S.; Álvarez-Mon, M.; Buján, J.; Teus, M.A. Update on uveal melanoma: Translational research from biology to clinical practice (Review). Int. J. Oncol. 2020, 57, 1262–1279. [Google Scholar] [CrossRef]
- Park, S.J.; Oh, C.-M.; Kim, B.-W.; Woo, S.J.; Cho, H.; Park, K.H. Nationwide Incidence of Ocular Melanoma in South Korea by Using the National Cancer Registry Database (1999–2011). Investig. Opthalmology Vis. Sci. 2015, 56, 4719–4724. [Google Scholar] [CrossRef]
- Stang, A.; Parkin, D.M.; Ferlay, J.; Jöckel, K.-H. International uveal melanoma incidence trends in view of a decreasing proportion of morphological verification. Int. J. Cancer 2005, 114, 114–123. [Google Scholar] [CrossRef]
- Nichols, E.E.; Richmond, A.; Daniels, A.B. Disparities in Uveal Melanoma: Patient Characteristics. Semin. Ophthalmol. 2016, 31, 296–303. [Google Scholar] [CrossRef] [Green Version]
- Xu, Y.; Lou, L.; Wang, Y.; Miao, Q.; Jin, K.; Chen, M.; Ye, J. Epidemiological Study of Uveal Melanoma from US Surveillance, Epidemiology, and End Results Program (2010–2015). J. Ophthalmol. 2020, 2020, 3614039. [Google Scholar] [CrossRef]
- Baily, C.; O’Neill, V.; Dunne, M.; Cunningham, M.; Gullo, G.; Kennedy, S.; Walsh, P.M.; Deady, S.; Horgan, N. Uveal Melanoma in Ireland. Ocul. Oncol. Pathol. 2019, 5, 195–204. [Google Scholar] [CrossRef]
- Aronow, M.E.; Topham, A.K.; Singh, A.D. Uveal Melanoma: 5-Year Update on Incidence, Treatment, and Survival (SEER 1973-2013). Ocul. Oncol. Pathol. 2018, 4, 145–151. [Google Scholar] [CrossRef]
- Nowak, M.S.; Romanowska-Dixon, B.; Grabska-Liberek, I.; Żurek, M. Incidence and survival of ocular melanoma in National Cancer Registry of Poland in 2010–2017. Adv. Clin. Exp. Med. 2022, 31, 615–621. [Google Scholar] [CrossRef]
- Central Statistical Office of Poland Data. Available online: http://www.stat.gov.pl (accessed on 1 November 2022).
- Nowak, M.S.; Smigielski, J. The Prevalence and Causes of Visual Impairment and Blindness Among Older Adults in the City of Lodz, Poland. Medicine 2015, 94, e505, Erratum in: Medicine 2015, 94, 1. [Google Scholar] [CrossRef]
- Nowak, M.S.; Jurowski, P.; Gos, R.; Smigielski, J. Ocular findings among young men: A 12-year prevalence study of military service in Poland. Acta Ophthalmol. 2010, 88, 535–540. [Google Scholar] [CrossRef]
- Damato, B.E.; Coupland, S.E. Differences in uveal melanomas between men and women from the British Isles. Eye 2012, 26, 292–299. [Google Scholar] [CrossRef] [Green Version]
- Zloto, O.; Pe’Er, J.; Frenkel, S. Gender Differences in Clinical Presentation and Prognosis of Uveal Melanoma. Investig. Ophthalmol. Vis. Sci. 2013, 54, 652–656. [Google Scholar] [CrossRef] [Green Version]
- Liu-Smith, F.; Chiu, C.-Y.; Johnson, D.; Miller, P.; Glazer, E.; Wu, Z.; Wilson, M. The Sex Differences in Uveal Melanoma: Potential Roles of EIF1AX, Immune Response and Redox Regulation. Curr. Oncol. 2021, 28, 2801–2811. [Google Scholar] [CrossRef]
- Stålhammar, G. Sex-based differences in early and late uveal melanoma-related mortality. Cancer Med. 2022. Epub ahead of print. [Google Scholar] [CrossRef]
- Nichols, E.E.; Richmond, A.; Daniels, A.B. Tumor Characteristics, Genetics, Management, and the Risk of Metastasis in Uveal Melanoma. Semin. Ophthalmol. 2016, 31, 304–309. [Google Scholar] [CrossRef] [Green Version]
- Chattopadhyay, C.; Kim, D.W.; Gombos, D.S.; Oba, J.; Qin, Y.; Williams, M.D.; Esmaeli, B.; Grimm, E.A.; Wargo, J.A.; Woodman, S.E.; et al. Uveal melanoma: From diagnosis to treatment and the science in between. Cancer 2016, 122, 2299–2312. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.D.; Turell, M.E.; Topham, A.K. Uveal Melanoma: Trends in Incidence, Treatment, and Survival. Ophthalmology 2011, 118, 1881–1885. [Google Scholar] [CrossRef]
- Bishop, K.D.; Olszewski, A.J. Epidemiology and survival outcomes of ocular and mucosal melanomas: A population-based analysis. Int. J. Cancer 2014, 134, 2961–2971. [Google Scholar] [CrossRef]
- Mahendraraj, K.; Lau, C.S.; Lee, I.; Chamberlain, R.S. Trends in incidence, survival, and management of uveal melanoma: A pop-ulation-based study of 7,516 patients from the Surveillance, Epidemiology, and End Results database (1973–2012). Clin. Ophthalmol. 2016, 10, 2113–2119. [Google Scholar] [CrossRef] [Green Version]
- Vajdic, C.M.; Kricker, A.; Giblin, M.; McKenzie, J.; Aitken, J.; Giles, G.G.; Armstrong, B.K. Incidence of ocular melanoma in Australia from 1990 to 1998. Int. J. Cancer 2003, 105, 117–122. [Google Scholar] [CrossRef]
- Rajeshuni, N.; Zubair, T.; Ludwig, C.A.; Moshfeghi, D.M.; Mruthyunjaya, P. Evaluation of Racial, Ethnic, and Socioeconomic Associations With Treatment and Survival in Uveal Melanoma, 2004–2014. JAMA Ophthalmol. 2020, 138, 876–884. [Google Scholar] [CrossRef]
- Schefler, A.C.; Kim, R.S. Recent advancements in the management of retinoblastoma and uveal melanoma. Fac. Rev. 2021, 10, 51. [Google Scholar] [CrossRef]
- Virgili, G.; Gatta, G.; Ciccolallo, L.; Capocaccia, R.; Biggeri, A.; Crocetti, E.; Lutz, J.-M.; Paci, E. Survival in Patients With Uveal Melanoma in Europe. Arch. Ophthalmol. 2008, 126, 1413–1418. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
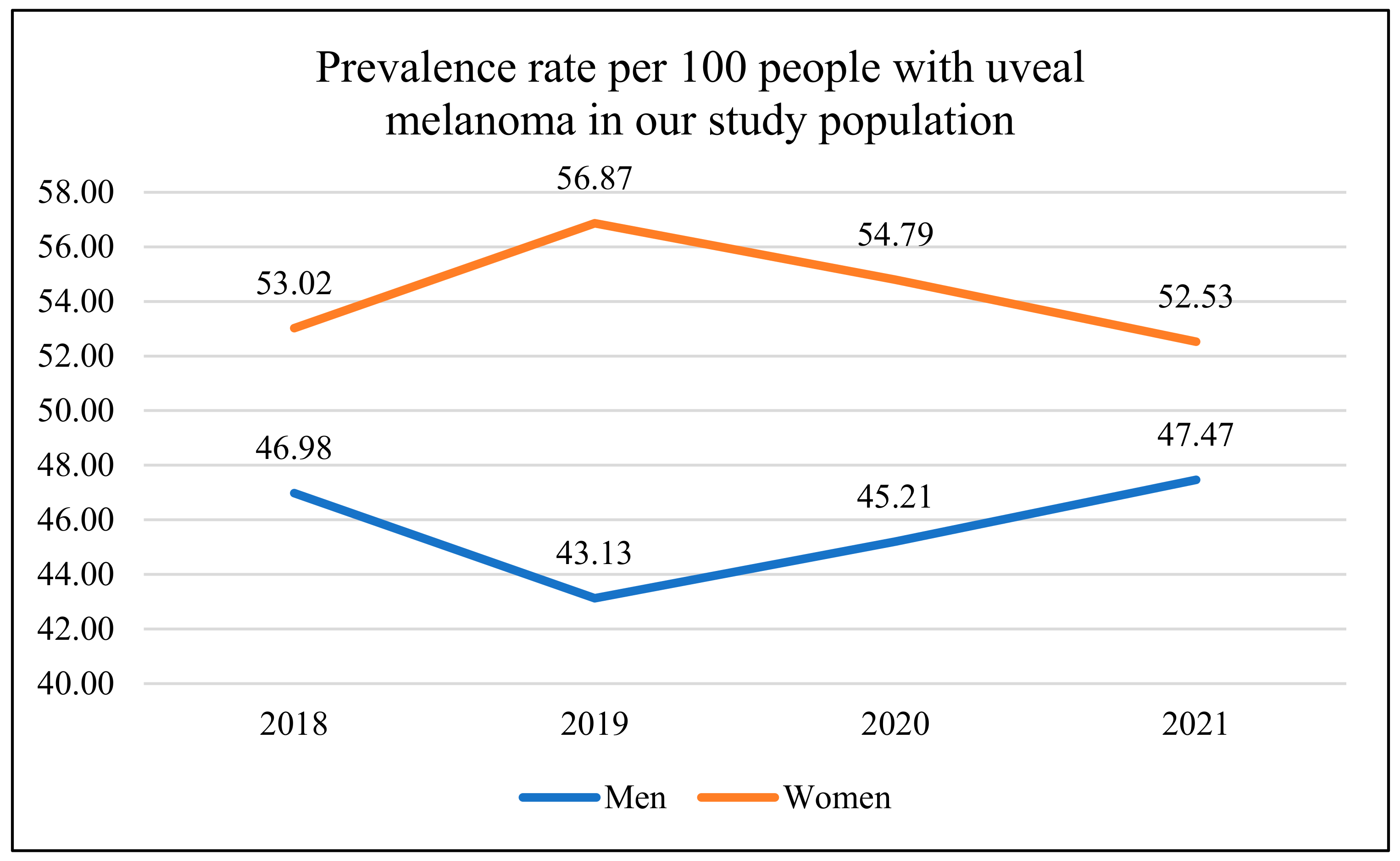
| 2018 | 2019 | 2020 | 2021 | All | |
|---|---|---|---|---|---|
| Men n% | 171 (46.98%) | 157 (43.13%) | 132 (45.21%) | 150 (47.47%) | 610 (45.66%) |
| Women n% | 193 (53.02%) | 207 (56.87%) | 160 (54.79%) | 166 (52.53%) | 726 (54.34%) |
| All n% | 364 (100%) | 364 (100%) | 292 (100%) | 316 (100%) | 1336 (100%) |
| Localization of Tumor | Sex | All n (%) | |
|---|---|---|---|
| Men n (%) | Women n (%) | ||
| Choroid | 486 (79.67%) | 538 (74.10%) | 1024 (76.65%) |
| Choroid and ciliary body | 69 (11.31% | 82 (11.30%) | 151 (11.30%) |
| Iris | 20 (3.28) | 29 (3.99%) | 49 (3.67%) |
| Iris and ciliary body | 24 (3.93%) | 47 (6.48%) | 71 (5.31%) |
| Ciliary body | 7 (1.15%) | 22 (3.03%) | 29 (2.17%) |
| Iris, ciliary body and choroid | 4 (0.66%) | 8 (1.10%) | 12 (0.90%) |
| All | 610 (100%) | 726 (100%) | 1336 (100%) |
| Cancer Stage TNM | Sex | All n (%) | |
|---|---|---|---|
| Men n (%) | Women n (%) | ||
| T1 | 170 (27.87%) | 177 (24.38%) | 347 (25.97%) |
| T2 | 165 (27.05%) | 227 (31.27%) | 392 (29.35%) |
| T3 | 165 (27.05) | 217 (29.89%) | 382 (28.59%) |
| T4 | 110 (18.03%) | 105 (14.46%) | 215 (16.09%) |
| All | 610 (100%) | 726 (100%) | 1336 (100%) |
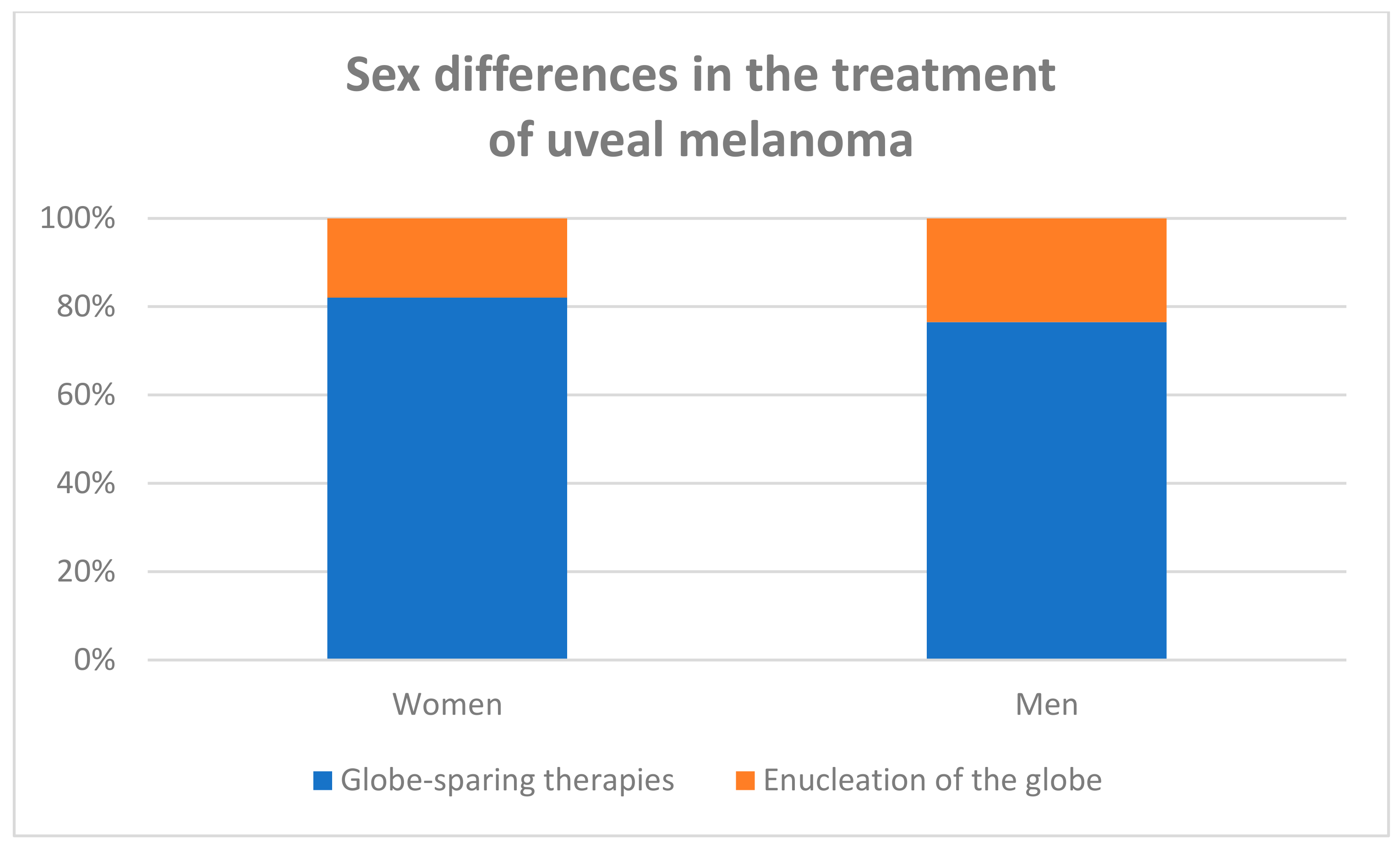
| Treatment Methods | Sex | All n (%) | |
|---|---|---|---|
| Men n (%) | Women n (%) | ||
| Plaque brachytherapy with iodine-125 | 188 (30.82% | 217 (29.89%) | 405 (30.31%) |
| Plaque brachytherapy with rhutenium-106 | 212 (34.75%) | 292 (40.22%) | 504 (37.72%) |
| Local surgery with plaque brachytherapy | 10 (1.65) | 26(3.58%) | 36 (2.70%) |
| Proton beam irradiation (PBI) | 57 (9.34%) | 60 (8.27%) | 117 (8.76%) |
| Enucleation | 143 (23.44%) | 131 (18.04%) | 274 (20.51%) |
| All | 610 (100%) | 726 (100%) | 1336 (100%) |
| Variables | Univariate Logistic Regression OR, 95% CI, p-Value | Multivariate Logistic Regression OR, 95% CI, p-Value |
|---|---|---|
| Gender: women vs. men | 0.72 (0.55–0.96) p = 0.024 | 0.73 (0.59–1.02) p = 0.063 |
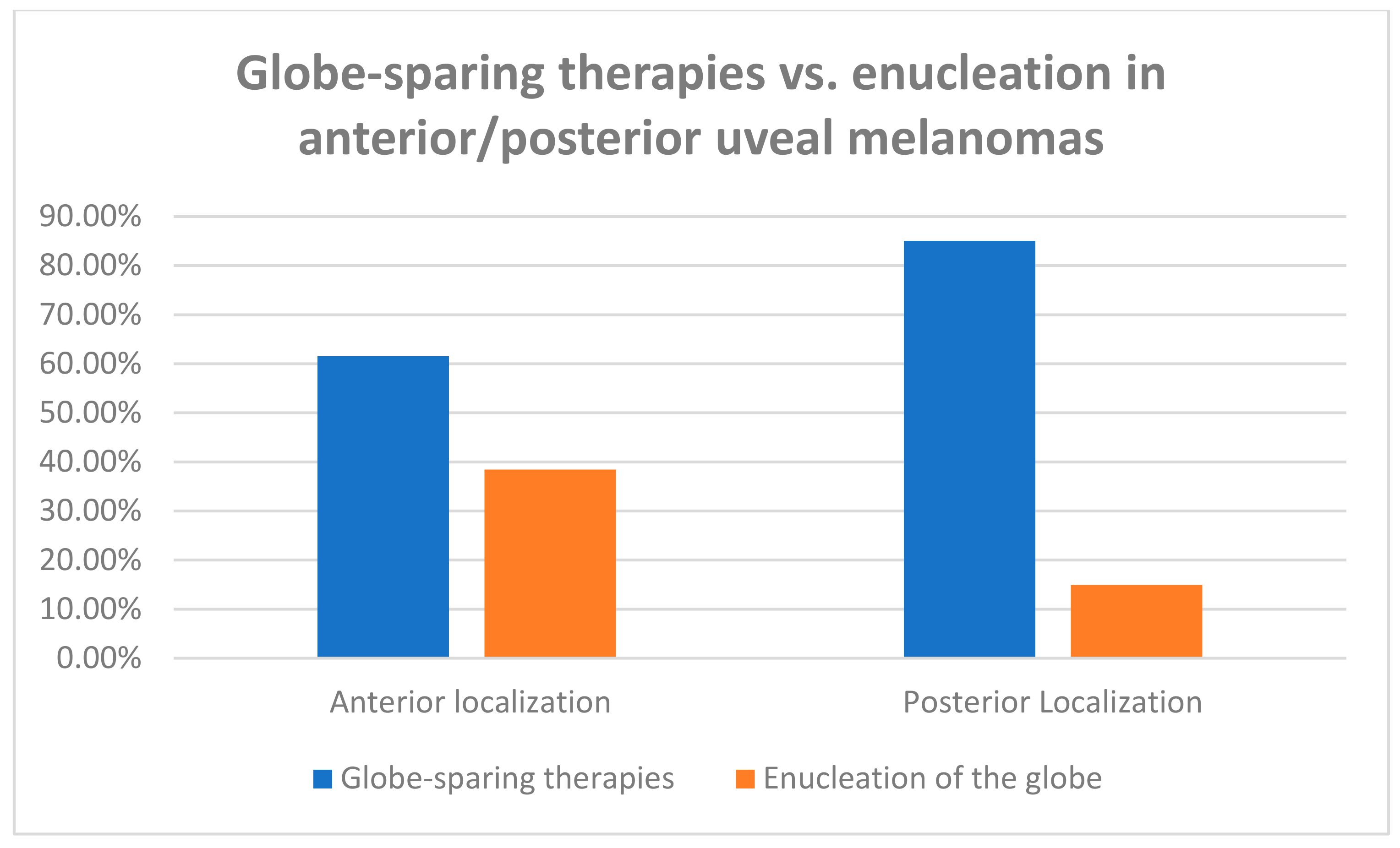
| Tumor localization: anterior vs. posterior to the equator of eye globe Size: according to TNM Classification | 3.56 (2.67–4.73) p < 0.000 3.46 (2.92–4.09) p < 0.000 | 4.18 (2.96–5.89) p < 0.000 3.48 (2.92–4.15) p < 0.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romanowska-Dixon, B.; Dębicka-Kumela, M.; Śmigielski, J.; Nowak, M.S. Sex Differences in the Treatment of Uveal Melanoma in a Group of 1336 Patients. J. Pers. Med. 2023, 13, 353. https://doi.org/10.3390/jpm13020353
Romanowska-Dixon B, Dębicka-Kumela M, Śmigielski J, Nowak MS. Sex Differences in the Treatment of Uveal Melanoma in a Group of 1336 Patients. Journal of Personalized Medicine. 2023; 13(2):353. https://doi.org/10.3390/jpm13020353
Chicago/Turabian StyleRomanowska-Dixon, Bożena, Magdalena Dębicka-Kumela, Janusz Śmigielski, and Michał Szymon Nowak. 2023. "Sex Differences in the Treatment of Uveal Melanoma in a Group of 1336 Patients" Journal of Personalized Medicine 13, no. 2: 353. https://doi.org/10.3390/jpm13020353