
The Effect of Interventions on Preventing Musculoskeletal Injuries Related to Nurses Work: Systematic Review
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Eligibility Criteria
2.3. Research Strategy
2.4. Data Extraction, Quality Appraisal, and Data Synthesis
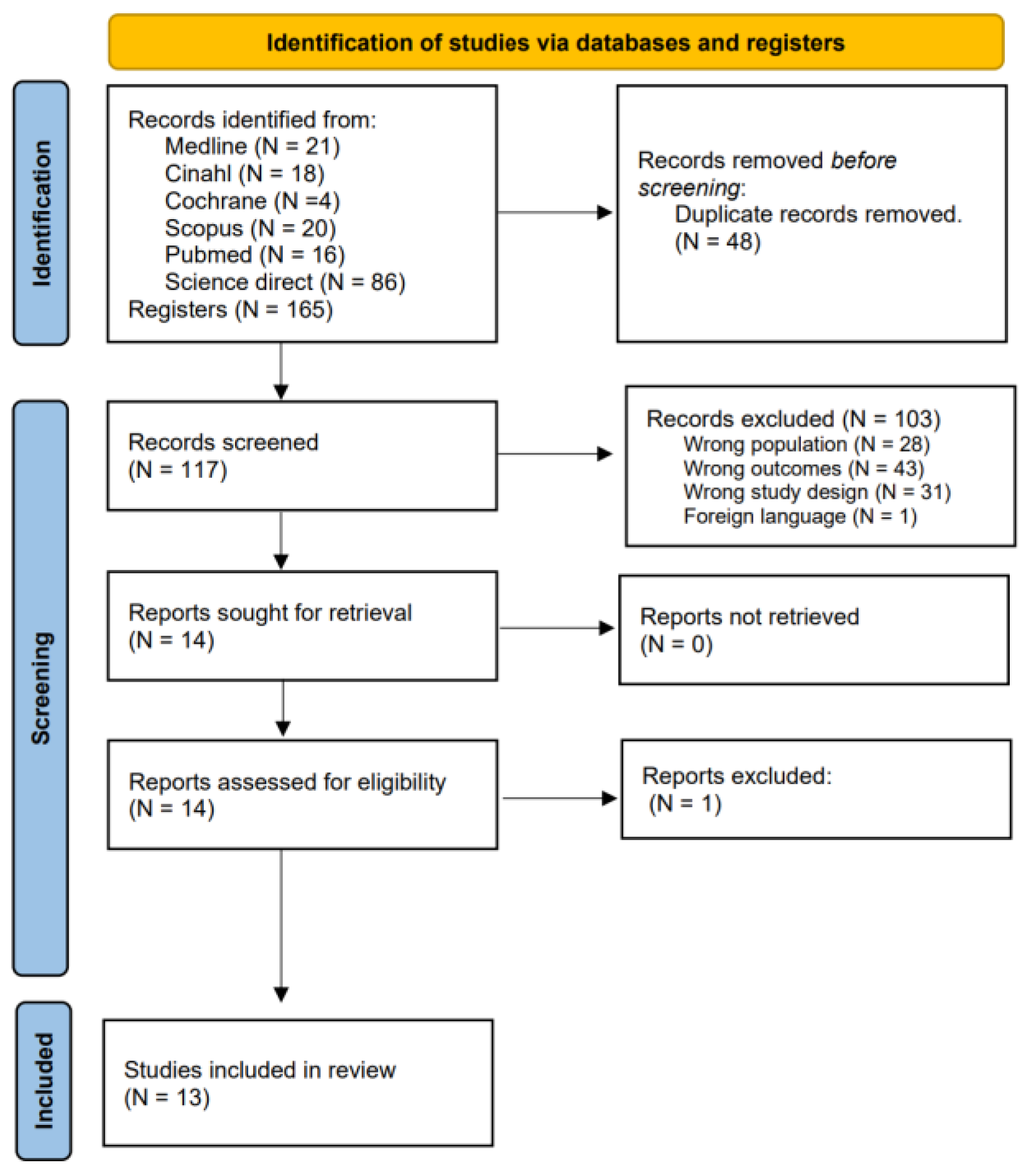
3. Results
3.1. Quality of the Evidence
3.2. Interventions to Prevent Musculoskeletal Disorders Related to Work in Nursing
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thinkhamrop, W.; Sawaengdee, K.; Tangcharoensathien, V.; Theerawit, T.; Laohasiriwong, W.; Saengsuwan, J.; Hurst, C.P. Burden of musculoskeletal disorders among registered nurses: Evidence from the Thai nurse cohort study. BMC Nurs. 2017, 16, 68. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Cui, Y.; He, L.; Xu, X.; Yuan, Z.; Jin, X.; Li, Z. Work-Related Musculoskeletal Disorders and Risk Factors among Chinese Medical Staff of Obstetrics and Gynecology. Int. J. Environ. Res. Public Health 2017, 14, 562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Hoof, W.; O’Sullivan, K.; O’Keeffe, M.; Verschueren, S.; O’Sullivan, P.; Dankaerts, W. The efficacy of interventions for low back pain in nurses: A systematic review. Int. J. Nurs. Stud. 2018, 77, 222–231. [Google Scholar] [CrossRef] [Green Version]
- Ellapen, T.J.; Narsigan, S. Work Related Musculoskeletal Disorders among Nurses: Systematic Review. J. Ergon. 2014, 4, S4-003. [Google Scholar]
- Akbari, H.; Akbari, H.; Abadi, M.B.H.; Fesharaki, M.G.; Ghasemi, M. Assessing the risk of manual handling of patients and its relationship with the prevalence of musculoskeletal disorders among nursing staff: Performance evaluation of the MAPO and PTAI methods. Iran. Red Crescent Med. J. 2017, 19, e39860. [Google Scholar] [CrossRef]
- Maria, T.; Andrianna, K.; Evdokia, B.; Elias, T. Work-related musculoskeletal disorders among female and male nursing personnel in Greece. World J. Res. Rev. 2017, 3, 8–15. [Google Scholar]
- Xu, H.; Zhang, M.; Hudson, A. Occupational Health Protection for Health Workers in China with Lessons Learned From the UK: Qualitative Interview and Policy Analysis. Saf. Health Work 2021, 12, 304–310. [Google Scholar] [CrossRef]
- Adamczyk, M.A. Reducing Intensive Care Unit Staff Musculoskeletal Injuries with Implementation of a Safe Patient Handling and Mobility Program. Crit. Care Nurs. Q. 2018, 41, 264–271. [Google Scholar] [CrossRef]
- Marshall, L.; Villeneuve, J.; Grenier, S. Effectiveness of a multifactorial ergonomic intervention and exercise conditioning kinesiology program for subsequent work related musculoskeletal disorder prevention. Work 2018, 61, 81–89. [Google Scholar] [CrossRef]
- Becker, A.; Angerer, P.; Müller, A. The prevention of musculoskeletal complaints: A randomized controlled trial on additional effects of a work-related psychosocial coaching intervention compared to physiotherapy alone. Int. Arch. Occup. Environ. Health 2017, 90, 357–371. [Google Scholar] [CrossRef]
- Carr, L.J.; Leonhard, C.; Tucker, S.; Fethke, N.; Benzo, R.; Gerr, F. Total Worker Health Intervention Increases Activity of Sedentary Workers. Am. J. Prev. Med. 2016, 50, 9–17. [Google Scholar] [CrossRef]
- Ghadyani, L.; Tavafian, S.S.; Kazemnejad, A.; Wagner, J. Effectiveness of Multidisciplinary Group-Based Intervention versus Individual Physiotherapy for Improving Chronic Low Back Pain in Nursing Staff: A Clinical Trial with 3- and 6-Month Follow-Up Visits from Tehran, Iran. Asian Spine J. 2017, 11, 396–404. [Google Scholar] [CrossRef] [PubMed]
- Richardson, A.; McNoe, B.; Derrett, S.; Harcombe, H. Interventions to prevent and reduce the impact of musculoskeletal injuries among nurses: A systematic review. Int. J. Nurs. Stud. 2018, 82, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Russo, F.; Papalia, G.F.; Vadalà, G.; Fontana, L.; Iavicoli, S.; Papalia, R.; Denaro, V. The Effects of Workplace Interventions on Low Back Pain in Workers: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 12614. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Zhang, H.; Lv, C.; Tang, L.; Tian, S. Comparative efficacy of 12 non-drug interventions on non-specific chronic low back pain in nurses: A systematic review and network meta-analysis. J. Back Musculoskelet. Rehabil. 2021, 34, 499–510. [Google Scholar] [CrossRef] [PubMed]
- Asuquo, E.G.; Tighe, S.M.; Bradshaw, C. Interventions to reduce work-related musculoskeletal disorders among healthcare staff in nursing homes; An integrative literature review. Int. J. Nurs. Stud. Adv. 2021, 3, 100033. [Google Scholar] [CrossRef]
- Clari, M.; Godono, A.; Garzaro, G.; Voglino, G.; Gualano, M.R.; Migliaretti, G.; Gullino, A.; Ciocan, C.; Dimonte, V. Prevalence of musculoskeletal disorders among perioperative nurses: A systematic review and META-analysis. BMC Musculoskelet. Disord. 2021, 22, 226. [Google Scholar] [CrossRef]
- Choi, S.D.; Brings, K. Work-related Musculoskeletal Risks Associated with Nurses and Nursing Assistants Handling Overweight and Obese Patients: A Literature Review. Work 2016, 53, 439–448. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.; Li, L.; Wang, L.; Zeng, J.; Yan, B.; Li, Y. Effectiveness of a multidimensional intervention program in improving occupational musculoskeletal disorders among intensive care unit nurses: A cluster-controlled trial with follow-up at 3 and 6 months. BMC Nurs. 2021, 20, 46. [Google Scholar] [CrossRef]
- Oakman, J.; Clune, S.; Stuckey, R. Work-Related Musculoskeletal Disorders in Australia; Safe Work Australia: Canberra, Australia, 2019. [Google Scholar]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions, version 6.3 (updated February 2022); Cochrane: Hoboken, NJ, USA, 2022. [Google Scholar]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 3, 160. [Google Scholar] [CrossRef] [PubMed]
- Thomas, B.H.; Ciliska, D.; Dobbins, M.; Micucci, S. A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews Evid. Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Yassi, A.; Cooper, J.E.; Tate, R.B.; Gerlach, S.; Muir, M.; Trottier, J.; Massey, K. A randomized controlled trial to prevent patient lift and transfer injuries of health care workers. Spine 2001, 26, 1739–1746. [Google Scholar] [CrossRef] [PubMed]
- Owen, B.D.; Keene, K.; Olson, S. An ergonomic approach to reducing back/shoulder stress in hospital nursing personnel: A five year follow up. Int. J. Nurs. Stud. 2002, 39, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Nelson, A.; Matz, M.; Chen, F.; Siddharthan, K.; Lloyd, J.; Fragala, G. Development and evaluation of a multifaceted ergonomics program to prevent injuries associated with patient handling tasks. Int. J. Nurs. Stud. 2006, 43, 717–733. [Google Scholar] [CrossRef] [Green Version]
- Black, T.R.; Shah, S.M.; Busch, A.J.; Metcalfe, J.; Lim, H.J. Effect of transfer, lifting, and repositioning (TLR) injury prevention program on musculoskeletal injury among direct care workers. J. Occup. Environ. Hyg. 2011, 8, 226–235. [Google Scholar] [CrossRef]
- Zadvinskis, I.M.; Salsbury, S.L. Effects of a multifaceted minimal-lift environment for nursing staff: Pilot results. West. J. Nurs. Res. 2010, 32, 47–63. [Google Scholar] [CrossRef]
- Pourhaji, F.; Delshad, M.H.; Tavafian, S.S.; Niknami, S.; Pourhaji, F. Effects of educational program based on Precede-Proceed model in promoting low back pain behaviors (EPPLBP) in health care workers Shahid Beheshti University of medical sciences: Randomized trial. Heliyon 2020, 6, e05236. [Google Scholar] [CrossRef]
- Kozak, A.; Freitag, S.; Nienhaus, A. Evaluation of a Training Program to Reduce Stressful Trunk Postures in the Nursing Professions: A Pilot Study. Ann. Work Expo. Health 2017, 61, 22–32. [Google Scholar] [CrossRef] [Green Version]
- Van Eerd, D.; D’Elia, T.; Ferron, E.M.; Robson, L.; Amick, B., III. Implementation of participatory organizational change in long term care to improve safety. J. Saf. Res. 2021, 78, 9–18. [Google Scholar] [CrossRef]
- Garg, A.; Kapellusch, J.M. Long-term efficacy of an ergonomics program that includes patient-handling devices on reducing musculoskeletal injuries to nursing personnel. Hum. Factors 2012, 54, 608–625. [Google Scholar] [CrossRef] [PubMed]
- Evanoff, B.; Wolf, L.; Aton, E.; Canos, J.; Collins, J. Reduction in injury rates in nursing personnel through introduction of mechanical lifts in the workplace. Am. J. Ind. Med. 2003, 44, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wolf, L.; Evanoff, B. Use of mechanical patient lifts decreased musculoskeletal symptoms and injuries among health care workers. Inj. Prev. 2004, 10, 212–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, T.T.; Nguyen, T.H.; Hoang, D.L.; Hoang, T.G.; Pham, M.K. Effectiveness of Interventions to Prevent Musculoskeletal Disorders among District Hospital Nurses in Vietnam. Biomed. Res. Int. 2022, 2022, 1539063. [Google Scholar] [CrossRef]
- Fernandes, C.N.; Couto, G.; Carvalho, R.; Fernandes, D.G.; Brito, L.; Carvalho, P.; Ferreira, P.F. Risk observation in the handling of dependent patients in health professionals of a hospital unit. Nurs. Pract. Today 2018, 5, 385–394. [Google Scholar] [CrossRef]
- Azizpour, Y.; Delpisheh, A.; Montazeri, Z.; Sayehmiri, K. Prevalence of low back pain in Iranian nurses: A systematic review and meta-analysis. BMC Nurs. 2017, 16, 50. [Google Scholar] [CrossRef]
- Carneiro, P.; Braga, A.C.; Barroso, M. Workrelated musculoskeletal disorders in home care nurses: Study of the main risk factors. Int. J. Ind. Ergon. 2017, 61, 22–28. [Google Scholar] [CrossRef] [Green Version]
- Grant, M.P.; Okechukwu, C.A.; Hopcia, K.; Sorensen, G.; Dennerlein, J.T. An Inspection Tool and Process to Identify Modifiable Aspects of Acute Care Hospital Patient Care Units to Prevent WorkRelated Musculoskeletal Disorders. Workplace Health Saf. 2018, 66, 144–158. [Google Scholar] [CrossRef] [Green Version]
- Andersen, L.L. Musculoskeletal Disorders in the Healthcare Sector; Occupational Safety and Health Administration: Brussels, Belgium, 2021. [Google Scholar]
- Humrickhous, R.; Knibbe, H.J.J. The Importance of Safe Patient Handling to Create a Culture of Safety: An Evidential Review. Ergon. Open J. 2016, 9, 27–42. [Google Scholar] [CrossRef]
- Ferreira, B.A.l.S.; Gomes, T.J.B.; Baixinho, C.R.S.L.; Ferreira, O.M.R. Transitional care to caregivers of dependente older people: An integrative literature review. Rev. Bras. Enferm. 2020, 73, e20200394. [Google Scholar] [CrossRef]
- Kanaskie, M.L.; Snyder, C. Nurses and nursing assistants decision-making regarding use of safe patient handling and mobility technology: A qualitative study. Appl. Nurs. Res. 2018, 39, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Vaismoradi, M.; Tella, S.; Logan, P.A.; Khakurel, J.; Vizcaya-Moreno, F. Nurses’ Adherence to Patient Safety Principles: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 2028. [Google Scholar] [CrossRef] [PubMed]
- Presado, M.H.; Cardoso, M.; Marques, M.F.M.; Baixinho, C.L. Analysis of student biomechanics in videos of delivery simulation practice. Rev. Esc. Enferm. USP 2019, 53, e03507. [Google Scholar] [CrossRef] [PubMed]
- Stock, S.R.; Nicolakakis, N.; Vézina, N.; Vézina, M.; Gilbert, L.; Turcot, A.; Sultan-Taïeb, H.; Sinden, K.; Denis, M.-A.; Delga, C.; et al. Are work organization interventions effective in preventing or reducing work-related musculoskeletal disorders? A systematic review of the literature. Scand. J. Work Environ. Health 2018, 44, 113–133. [Google Scholar] [CrossRef]
- Tersa-Miralles, C.; Bravo, C.; Bellon, F.; Pastells-Peiró, R.; Arnaldo, E.R.; Rubí-Carnacea, F. Effectiveness of workplace exercise interventions in the treatment of musculoskeletal disorders in office workers: A systematic review. BMJ Open 2022, 12, e054288. [Google Scholar] [CrossRef]
- McPhail, S.M.; Schippers, M.; Marshall, A.L.; Waite, M.; Kuipers, P. Perceived barriers and facilitators to increasing physical activity among people with musculoskeletal disorders: A qualitative investigation to inform intervention development. Clin. Interv. Aging 2014, 9, 2113. [Google Scholar] [CrossRef] [Green Version]
- Sipaviciene, S.; Kliziene, I. Effect of different exercise programs on non-specific chronic low back pain and disability in people who perform sedentary work. Clin. Biomech. 2020, 73, 17–27. [Google Scholar] [CrossRef]


{kind=link}
| Search Strategy | Number of Articles | |
|---|---|---|
| #1 | ((((((((nursing[Title/Abstract]) OR (midwive[Title/Abstract])) OR (nurse-midwives[Title/Abstract])) OR (nurs*[Title/Abstract])) OR (midw*[Title/Abstract])) OR (nursing care[MeSH Terms])) OR (midwife[MeSH Terms])) OR (nurse midwife[MeSH Terms])) OR (nurse midwives[MeSH Terms]),,,”““nursing”“[Title/Abstract] OR ““midwive”“[Title/Abstract] OR ““nurse-midwives”“[Title/Abstract] OR ““nurs*”“[Title/Abstract] OR ““midw*”“[Title/Abstract] OR ““nursing care”“[MeSH Terms] OR ““midwifery”“[MeSH Terms] OR ““nurse-midwives”“[MeSH Terms] OR ““nurse-midwives”“[MeSH Terms]” | 1,106,849 |
| #2 | (((((((((((((((((((((occupational injuries[Title/Abstract])) OR (injuries[Title/Abstract])) OR (occupational diseases[Title/Abstract])) OR (musculoskeletal injuries[Title/Abstract])) OR (musculoskeletal disorders[Title/Abstract])) OR (musculoskeletal disorders related to work[Title/Abstract])) OR (musculoskeletal pain[Title/Abstract])) OR (back pain[Title/Abstract])) OR (neck pain[Title/Abstract])) OR (tendinitis[Title/Abstract])) OR (back hernias[Title/Abstract])) OR (hernias of the spinal column[Title/Abstract])) OR (Inj*[Title/Abstract])) OR (Musculos* inj*[Title/Abstract])) OR (abnormalities, musculoskeletal[MeSH Terms])) OR (musculoskeletal diseases[MeSH Terms])) OR (musculoskeletal disease[MeSH Terms])) OR (back pain[MeSH Terms])) OR (tendinitis[MeSH Terms])) ) OR (back pain, low[MeSH Terms])”,,,”““occupational injuries”“[Title/Abstract] OR ““injuries”“[Title/Abstract] OR ““occupational diseases”“[Title/Abstract] OR ““musculoskeletal injuries”“[Title/Abstract] OR ““musculoskeletal disorders”“[Title/Abstract] OR ((““musculoskeletal diseases”“[MeSH Terms] OR (““musculoskeletal”“[All Fields] AND ““diseases”“[All Fields]) OR ““musculoskeletal diseases”“[All Fields] OR (““musculoskeletal”“[All Fields] AND ““disorders”“[All Fields]) OR ““musculoskeletal disorders”“[All Fields]) AND ““related to work”“[Title/Abstract]) OR ““musculoskeletal pain”“[Title/Abstract] OR ““back pain”“[Title/Abstract] OR ““neck pain”“[Title/Abstract] OR ““tendinitis”“[Title/Abstract] OR ((““back”“[MeSH Terms] OR ““back”“[All Fields]) AND ““hernias”“[Title/Abstract]) OR ((““hernia”“[MeSH Terms] OR ““hernia”“[All Fields] OR ““hernias”“[All Fields] OR ““hernia s”“[All Fields] OR ““herniae”“[All Fields]) AND ““the spinal column”“[Title/Abstract]) OR ““inj”“[Title/Abstract] OR (““musculos*”“[All Fields] AND ““inj”“[Title/Abstract]) OR ““musculoskeletal abnormalities”“[MeSH Terms] OR ““musculoskeletal diseases”“[MeSH Terms] OR ““musculoskeletal diseases”“[MeSH Terms] OR ““back pain”“[MeSH Terms] OR ““tendinopathy”“[MeSH Terms] OR ““low back pain”“[MeSH Terms]”, | 4134 |
| #3 | ((((((((((((((intervention[Title/Abstract]) OR (programme[Title/Abstract])) OR (program*[Title/Abstract])) OR (Int*[Title/Abstract])) OR (action[Title/Abstract])) OR (multidimensional intervention[Title/Abstract])) OR (organizational program[Title/Abstract])) OR (preventative measures[Title/Abstract])) OR (preventive actions[Title/Abstract])) OR (prevention measures[Title/Abstract])) OR (prev*[Title/Abstract])) OR (accident prevention[MeSH Terms])) OR (early intervention[MeSH Terms])) OR (measures[MeSH Terms])) OR (assistance program, employee health care[MeSH Terms])”,,,”““intervention”“[Title/Abstract] OR ““programme”“[Title/Abstract] OR ““program*”“[Title/Abstract] OR ““int”“[Title/Abstract] OR ““action”“[Title/Abstract] OR ““multidimensional intervention”“[Title/Abstract] OR ““organizational program”“[Title/Abstract] OR ““preventative measures”“[Title/Abstract] OR ““preventive actions”“[Title/Abstract] OR ““prevention measures”“[Title/Abstract] OR ““prev*”“[Title/Abstract] OR ““accident prevention”“[MeSH Terms] OR ““early intervention, educational”“[MeSH Terms] OR ““weights and measures”“[MeSH Terms] OR ““occupational health services”“[MeSH Terms]” | 1,294,797 |
| #1 AND #2 AND #3 | 21 |
| Study/ Year/Country | Aim | Type of Study/ Sample | Time of Evaluation of Intervention and Participants | Outcomes and Instruments | Conclusions |
|---|---|---|---|---|---|
| Yassi et al. (2001) Canada [25] | “to compare the effectiveness of training and equipment to reduce musculoskeletal injuries, increase comfort, and reduce physical demands on staff performing patient lifts and transfers at a large acute care hospital.” | Randomized controlled trial (RCT) (three-armed) | The baseline was on 1 July 1998, and 6-months, and again at 12-months. The participants 346 nurses | Outcome: The frequency of manual patient-handling tasks, i.e., those tasks during which neither mechanical nor nonmechanical assistive equipment is used, was significantly and markedly decreased in the Arm C “no strenuous lifting” wards by 6 months, by an average of 9 tasks per shift. This decrease was sustained at 1 year. In contrast, there was no significant change over 6 months in frequency of manual handling tasks on Arm A or Arm B. By the time of the 6-month follow-up, there was a significant increase in use of assistive devices such as transfer belts and sliding devices on Arm B; however, this increase was not sustained at 1 year. The use of these manual assistive devices increased significantly (P 5 0.021) by 6 months on Arm C, but by 1 year use declined significantly. At 6 months nurses on Arm C reported using the sit-stand lift an average of 4.9 times per shift. This declined significantly to 3.2 times per shift at 1 year. The use of total body lifting equipment over time varied significantly by service type. Instruments: Visual analogic scales (VAS); SF36; Oswestry Low Back Pain Disability Questionnaire; Disability of Arms, Shoulder, and Hands (DASH). | After 6 months increased the using of lifting devices, but there was a decrease in one year. The “no strenuous lifting” program, which combined training with assured availability of mechanical and other assistive patient handling equipment, most effectively improved comfort with patient handling, decreased staff fatigue, and decreased physical demands. The fact that injury rates were not statistically significantly reduced may reflect the less sensitive nature of this indicator compared with the subjective indicators. |
| Owen et al. (2002) USA [26] | “to determine the impact of an Ergonomic program on perceived stress ratings, injury rates and patient care.” | Quasi experimental study design | 18-months pre- intervention, 18-months after intervention, and five years follow up period Participants: 319 data collection by nursing staff. | Outcomes: “There were 319 data collection forms completed by the nursing staff after carrying out the patient handling tasks. More than half (n = 182) involved transferring patients from bed to chair/commode and back to bed. (…) The mean of perceived exertion ranged from 0.6 to 1.0 for the shoulder by experimental site subjects and from 3.2 to 5.2 for control site nursing personnel. (…) The mean of perceived exertion to the lower back ranged from 0.5 to 0.7 by experimental site subjects and from 3.3 to 5.0 for control site nursing personnel.” Instruments: Two Likert-type scale, the OSHA 200 forms and the incident report forms generic to the hospitals | The perceived physical exertion was significantly reduced for all tasks at the experimental hospital. The number of back injuries, lost work, and restricted days have also decreased. If one compared the data of 18 months pre intervention to the data of 18 months post intervention, the injuries decreased to 40%, the LWDs decreased from 64 down to 3, and restricted days decreased to 20%. The patients felt more comfortable and more secure when assistive devices were used. |
| Nelson et al. (2006) USA [27] | (1) to design and implement a multifaceted program that successfully integrated evidence-based practice, technology, and safety | Pre-/post design without a control group (Focus groups) | Nine-month pre- intervention (May 2001–January 2002) and the nine-month post- | Outcomes: Key measures included injury rate, lost and modified workdays, job satisfaction, self-reported unsafe patient handling acts, level of support for program, staff and patient acceptance, program effectiveness, costs, and return on investment. | This multi-faceted program resulted in positive outcomes associated with injury rates, modified duty days, job satisfaction, self-reported safety in performing patient handling |
| improvement; (2) to evaluate the impact of the program on injury rate, lost and modified workdays, job satisfaction, self-reported unsafe patient handling acts, level of support for program, staff and patient acceptance, program effectiveness, costs, and return on investment. | intervention (February 2002–October 2002) Participants: 825 nurses | Post-intervention injury rate decreased in 15 of the 23 units, increased in 7 units and remained the same in 1 unit. Overall, the injury rate decreased from 24.0/100 caregivers at baseline and 16.9/100 caregivers’ post-intervention. Post-intervention injury rates were found to be significantly lower X2 (1, n = 46) = 4.42, p = 0.036. The number of modified duty days decreased significantly (p = 0.02) from 1777 modified duty days during the 9-month pre-intervention period, to 539 modified duty days during the 9-month post-intervention period. Instruments: Poisson regression model to test differences pre- and postintervention, Mean values for the number of modified duty days and lost days taken per injury, and survey results were interpreted using the modified Bonferoni approach. | tasks, and cost. The program was well accepted by patients, nursing staff, and administrators. While the total number of lost workdays decreased by 18% post-intervention, this difference was not statistically significant | ||
| Black et al. (2011) Canada [28] | To evaluate the effectiveness of a Transfer, Lifting and Repositioning (TLR) program to reduce musculoskeletal injuries (MSI) among direct health care workers, | Retrospective pre and post-intervention design, utilizing a nonrandomized control group | One year pre- and post-intervention. (September 2002–June 2004; January to December 2005) Participants: 766 TLR injuries cases | Outcomes: The number of injuries by occupation showed that in the control group, the distribution remained unchanged with the exception of therapists (physical therapists, occupational therapists, respiratory therapists) where a significant increase was seen. The most significant change was seen in the decrease in injuries in attendants (from 25.4% to 0%) and increase in injuries in nurse aides (from 1.1% to 11.3%) in the intervention group. Instruments: Analysis of all injuries and time-loss rates. | Significantly reduce both time-loss and no-time-loss injuries and disability related to patient handling. The reductions of claim costs/injury represented a substantial benefit to the intervention hospitals. The program intervention seemed to be more effective in the small hospitals than in the medium or large ones. |
| Yang et al. (2021) China [19] | To evaluate the effectiveness of a multidimensional intervention program to prevent and reduce WRMDs in ICU nurses. | Quasi-experimental cluster-randomized controlled trial | Baseline, 3 and 6 months after the start of the intervention (December 2017, to January 2018) Participants: 201 nurses | Outcomes: A total of 201 nurses from four mixed ICUs in four hospitals were recruited. From two ICUs, 94 nurses were assigned to the intervention group, and from the two remaining ICUs, 104 nurses were assigned to the control group by cluster random sampling. Ultimately, 190 nurses provided three recorded outcome measurements (intervention group, n = 89 [94.68%]; control group, n = 101 [94.39%]). No significant difference in loss to follow-up was found between the two groups (χ2 = 0.074, p = 0.862). GEE showed that the multidimensional intervention program improved the risk perception of WRMDs (OR = 0.517, p < 0.001) and health behavior application (OR = 0.025, p < 0.001), relative to that of the routine specialist training. Interactions between the measurement time and group were observed (p < 0.001). Age and the length of ICU employment affected the perception of a safe working environment (p = 0.047 and p = 0.011 respectively). The GEE, including age and ICU employment, indicated that the measures of the intervention group and the control group were statistically significant. The perception of an unsafe working environment in the control group was 1.637 times that in the intervention group (OR = 1.637, p = 0.024). | A meticulous planning is essential to make interventions compatible with the daily work routine. The multidimensional intervention program seems applicable from time, financial, and organizational perspectives, he helped to reduce the short-term reported incidence rate of WRMDs, improve the nursing risk perception and health behavior application, and promote a safe working environment. |
| Instruments: Baseline demographic information was collected, true self-reports on-line questionaries—Nordic Musculoskeletal Questionnaire (measure self-perceived symptoms of WRMDs), Chinese version of the Risk Perception of Musculoskeletal Injury (risk perception); Nursing Physical Factors Evaluation Questionnaire (Application of Health behavior); Hospital Safety Climate Questionnaire (Perception of a safe working environment). | |||||
| Zadvinskis et al. (2009) USA [29] | To examine the effectiveness of a multifaceted minimal-lift environment on reported equipment use, musculoskeletal injury rates, and workers’ compensation costs for patient-handling injuries. | A mixed measures design with both descriptive and quasi-experimental design | Baseline and 3 and 12 months after intervention (April 2007) Participants: 77 | Outcomes: 46 were in the intervention group (53% survey response rate) and 29 (39% survey response rate) were in the control group. There were no significant demographic differences between participants in the intervention and control groups. The combined sample (n = 75) was 95% female and ranged in age from 21 to 59 years (mean 33.7). Nursing staff members from the multifaceted minimal-lift environment experienced a reduction in patient-handling injuries and costs compared to nursing staff working in a non–minimal-lift environment. The intervention unit injury incidence rate was 3.26/100 full-time equivalents (FTEs) whereas the control unit injury incidence rate was 3.43/100 FTEs. Injury costs for the intervention unit were $6566 compared with $11,145 for the control unit (a $4579 difference). After subtracting the cost of peer coach education ($1680), the intervention unit experienced a $2899 return on investment. Instruments: Demographic and equipment use data for the intervention and control units were collected through self-report via pen-and-paper survey. | Implementing a successful multifaceted minimal-lift environment for nursing staff can be time consuming and complex. Intervention strategies must match the innovation, target group, and workplace context, and could expand program elements to include ergonomic assessment protocols, after action reviews. |
| Pourhaji et al. (2020) Iran [30] | To investigate the effects of an educational program based on Precede-Proceed model on promoting Low Back Pain (LBP) behaviors among health care workers (HCWs). | A randomized trial | 6 and 12-months follow-ups. Participants: 102 | Outcomes: The present study was conducted on HCWs aged 30 to 55 (The Subjects 75 Intervention Into two group1, 2 and 37 control groups) in the comprehensive Service centers. The mean age of the intervention group was 46.34 ± 1.18, and the mean age of the control group was 47.23 ± 1.15 years (p = 0.598). Prior to the intervention, there was no significant difference between the two intervention groups and one control group. The repeated measure analysis test confirmed that was important and significant difference 6 and 12 months after the Intervention. There was a significant interaction between the factors “group” and “test time” (p < 0.05, p < 0.001). Increasing the mean score of attitude, knowledge, perceived self-efficacy, enabling factors, reinforcing factors, quality of life, public health, and preventive behaviors of LBP in intervention group (p < 0.05, < 0.001), but no significant change in mean score of knowledge, attitude, Self-efficacy, quality of life, general health, reinforcing | Health behaviors require context and access to education through the best and easiest channels, which seems to be appropriate for social media. Different educational approaches can be effective in reducing low back pain, disability and improving the health care workers life. The social media approach has been more successful than long-term face-to-face intervention and may be a better way to deliver training programs because of its ease of access and reduced operating costs |
| factors, enabling factors and preventive behaviors of LBP in the control group (p > 0.05). Instruments: Visual Analogue Scale (VAS) for measuring LBP, for measuring pain-related disability, the Quebec Back Pain Disability Scale (QBPDS) was used. The social media approach to maintaining behavior for a long time (6 months) was more successful than the face-to-face approach | |||||
| Kozak et al. (2017) Germany [31] | To evaluate metrologically the effectiveness of a training program on the reduction of stressful trunk postures in geriatric nursing professions. | Pilot study | 2-weeks before and 6-months after intervention Participants: 42 | Outcomes: Measurement data were available from 23 participants at baseline and from 19 participants at a 6-month follow-up. After the intervention, the median proportion of time spent in sagittal inclinations exceeding 20° was significantly reduced, by 29% (p < 0.001), from 1772 to 1708 median trunk movements per shift. The proportion of very pronounced inclinations exceeding 60° was reduced by 60% (p = 0.002), from 288 to 135 inclinations per shift. A significant reduction in static inclinations was also detected (22%; p < 0.001), from 462 to 329 inclinations per shift (numbers of inclinations not in the table). The median time spent in sagittal inclinations exceeding 20° was reduced by 27 min per shift. esults of the video analyses at the second measure ment show that in total 217 basic care activities at the bedside were observed. As recommended by the seminar instructor, the bed was raised to hip height in 44.7% of all care situations. However, in 44.2% of situations, the bed was partially raised, and in 11.1%, the bed was not raised at all. In total, 52 care situations in the bathroom were observed. A stool was used in 67.3% of these situations to perform basic care in the sitting position; in 32.7% of the situations, the stool was not used by the nurses. Instruments: The CUELA measurement system and video analyses were used to evaluate this intervention. | This study showed a significant improvement in body postures after implementation of a training concept consisting of instruction on frequent body postures in nursing, physical exercises, instructions in practical ergonomic work at the bedside and in the bathroom, and reorganization of work environment. |
| Van Eerd et al. (2021) Canada [32] | To follow the implementation of a participatory organizational change intervention and assess the program implementation effects on important intermediate outcomes. | Mixed methods implementation | Baseline pre- intervention (Time 1—pre- implementation), 6 months (Time 2—mid-point of implementation), and 12 months (Time 3—end of implementation). Participants:197 | Outcomes: there were 132 participants with 65 from the control sites and 67 from the intervention sites. Control group self-efficacy score did not increase over time whereas for the intervention group, self-efficacy scores increase over time. Three of the six measures (back (motion), shoulder/arm, wrist/hand) favored the intervention sites. Respondents concerns about safety and worker health most often concerned MSDs, stress levels and staff safety. They often referred to MSD hazards related to force and posture. They noted a culture of resistance to change, even though many felt the changes were likely to be beneficial Instruments: Three different methods: (1) self-administered questionnaires; (2) staff observations; (3) interviews and focus groups. | The increase in operational leadership confidence to address MSD hazards is important for programs implementation but also for program impact and sustainability. An important facilitator to implementing a participatory approach is early frontline staff involvement. |
| Garg et al. (2012) USA [33] | To evaluate long-term efficacy of an ergonomics program that included patient-handling devices in six long-term care facilities (LTC) and one chronic care hospital (CCH). | A pre- and postintervention design without a control group | During the intervention and postintervention. Participants: 504 | Outcomes: “Compared with preintervention data, posintervention data showed significant improvements in injuries, lost workdays, modified-duty days, and workers ‘compensation costs associated with patient-handling activities. Decreased by 59.8%, lost workdays by 86.7%, modified-duty days by 78.8%, and workers ‘compensation cost by 90.6%. Instruments: For each nursing facility, mean values for patient-handling injuries, lost workdays, modified-duty days, and workers’ compensation costs were calculated per 100 nursing full-time equivalent employees (FTEs) per year for both pre- and postintervention. They rated each device for stresses to low back and shoulders on the Borg CR-10 Scale pacient comfort on a 7-point comfort scale and patient safety on a 7-point scale similar to Corlett and Bishop’s scale. They also rated the manual transfer method using gait belt for lofting and transferring patients from bed to wheelchair and draw sheet for repositioning in bed. | The study demonstrated that the implementation of patient-handling devices along with a comprehensive ergonomics program was effective in reducing injuries, lost workdays, modified-duty days, and workers compensation costs. They identified that for effective implementation of patient-handling devices, are no-manual-lifting policy, not readily available device, inadequate training of nursing, concerns for patient safety and longer transfer time with devices than with manual methods. |
| Evanoff et al. (2003) USA [34] | To evaluate the effectiveness of mechanical patient hoists at reducing musculoskeletal injuries following the deployment of such lifts in acute care hospitals and long-term care (LTC) facilities | A pre and post intervention study | Pre-intervention it was between January 1, 1996 and the date lifts were deployed-1997 or 1998, post-intervention was after the lifts were deployed until 31 December 2000. Participants: 412 | Outcomes: “we observed 412 recordable musculoskeletal injuries during the study period, from a heath care worker population of 13,6 million productive hours (equivalent to 6835 full-time work years). Data combining the acute care and LTC units showed a RR of recordable injury of 0.82 (95% CI: 0.68–1.00), RR of lost day injury of 0.56 (0.41–0.78). And RR for lost day rate of 0.38, comparing the post intervention to the pre-intervention period. The injury rate decreased from 6.59 injuries annually per 100 FTE during the pre-intervention period to 5.70 injuries during the post-intervention period. Lost time rate also declined markedly in the post-intervention period. Instruments: Data on injuries and lost days were collected through OSHA 200 logs kept by each hospital. The interview asked how many times the worker had personally used a lift for transferring or weighing patients during the previous full-shift they worked, how many times they saw others use a lift for transferring or weighing patients on the previous shift, and why they did not use lifts more often. | The implementation of patient lifts can be effective in reducing occupational musculoskeletal injuries to nursing personnel in both LTC and acute care settings. In future work should focus on strategies to facilitate greater use of mechanical lifting device. |
| Li et al. (2004) USA [35] | To evaluate the effectiveness of mechanical patient lifts in reducing musculoskeletal symptoms, injuries, lost workday injuries, and workers’ compensation costs in workers at a community hospital | A pre and post intervention study | The pre-intervention period (July 1999 to January 2001), intervention period (August 2000 to January 2001), post-intervention period (February 2001 to March 2003). Participants:138 | Outcomes: Of a total of 138 health care workers in the three intervention units, 61 (44%) completed the baseline symptom survey in June 2000. Compared with the pre-intervention period, post-intervention surveys showed statistically significant improvements in musculoskeletal comfort levels (p, 0.05) for all nine body parts surveyed. the nursing staff reported a statistically significant improvement in general health (0.2 out of a five point scale, p = 0.008). There was little change in the perceived intensity and difficulty of work, while statistically significant improvements were reported in job satisfaction, willingness to recommend their job to others, and in helpfulness of supervisor (all 0.4 out of a four point scale, p, 0.05. Instruments: At the training sessions, participants were given baseline ergonomic surveys (levels of musculoskeletal comfort of different body parts, the presence and severity of pain, and the levels of physical and mental exhaustion experienced ‘‘at the end of a typical workday’’). Other questions are information on several aspects of their work, such as the degree of support received from their supervisors, the amount of time available to complete tasks, and their level of job satisfaction. | Many nursing staff are reluctant to use mechanical lifts for patient handling tasks, the main reason reported was the lack of perceived need, followed by the lack of time and the lack of maneuvering space. They suggest that must be encouraged by management, and a policy of no manual lifting must be adopted. |
| Nguyen et al. (2022) Vietnam [36] | To evaluate the effectiveness of basic interventions (education, physical exercise) to prevent MSDs among district hospital nurses in Vietnam | A quasi-experimental before/after study | Pre- and postintervention evaluation. Participants: 290 nurses | Outcomes: “an intervention for 162 nurses and had a total of 128 nurses in the control group. Some general characteristics between the intervention group and the control group at baseline were quite similar, shown by p values in the Student´s t-test and the Chi2 test, both higher than 0.05. (…) Regarding impact on the prevalence of MSDs, there was a significant difference of the GEE´s test on the prevalence of MSDs in the last 7 days between the 2 groups before and after the intervention with the p value = 0.016. In more detail, the prevalence of MSDs in the last 7 days in the control group was 1.9 times higher than in the intervention group after the intervention. For the prevalence of MSDs in the last 12 months, the test did not provide significance by showing that the p value is equal to 0.059 (…) the intervention measures are probably effective in reducing the prevalence of MSDs at 4 anatomical sites: neck, shoulder/upper arm, wrists/hand, and lower back. Instruments: A Sociodemographic Questionnaire; The Standardized Nordic Questionnaire; The Short Form of the Quality-of-Life Enjoyment and Satisfaction Questionnaire (Q-LES-Q-SF); the Kessler Psychological Distress Scale. | The intervention measures are probably effective in reducing the prevalence of MSDs at these neck, shoulder/upper arm, wrists/hand, and lower back. One of the limitations of the educational intervention in this study is that it only provides of theoretical information and knowledge to nurses but does not monitor the application of these measurements by nurses in their actual work. |
| Study | D1 | D2 | D3 | D4 | D5 | Overall |
|---|---|---|---|---|---|---|
| Yassi et al. (2001) [25] |  | | some concerns | | | some concerns |
| Pourhaji et al. (2020) [30] | | | | | | |
| Quality Assessment of before–after Studies with No Control Group | |||||
|---|---|---|---|---|---|
| Nelson et al. (2006) [27] | Black et al. (2011) [28] | Garg et al. (2012) [33] | Evanoff et al. (2003) [34] | Li et al. (2004) [35] | |
| Study question or objective clearly stated | Yes | Yes | Yes | Yes | Yes |
| Eligibility/selection criteria for the study population prespecified and clearly described | No | Yes | No | No | No |
| Participants in the study were representative of those who would be eligible for the intervention | No | No | Yes | Yes | Yes |
| Eligible participants were all enrolled | No | Yes | NR | NR | NR |
| The sample size was sufficiently large | Yes | Yes | Yes | Yes | Yes |
| The intervention was clearly described and delivered consistently | Yes | Yes | Yes | Yes | Yes |
| The outcome measures were pre-specified, clearly defined, valid, reliable, and assessed consistently | Yes | Yes | Yes | Yes | Yes |
| Outcomes were assessed blindly | Yes | Yes | No | Yes | No |
| The loss to follow-up after baseline was 20% or less | No | Yes | NR | ||
| Were those lost to follow-up accounted for in the analysis? | Yes | Yes | NR | NR | NR |
| The statistical methods examine changes in outcome measures from before to after the intervention and statistical tests provided values for the pre-to-post changes | Yes | Yes | Yes | Yes | Yes |
| Outcome measures were taken multiple times before the intervention and multiple times after the intervention | No | No | No | No | No |
| If the intervention was conducted at a group level (e.g., a health unit, a community, Etc.), the statistical analysis took into account the use of individual-level data to determine effects at the group level | Yes | Yes | Yes | No | No |
| Quality Assessment of Papers Describing an Observational and Quasi-Experimental Study | ||||||
|---|---|---|---|---|---|---|
| Owen et al. (2002) [26] | Yang et al. (2021) [19] | Zadvinskis et al. (2009) [29] | Kozak et al. (2017) [31] | Van Eerd D et al. (2021) [32] | Nguyen et al. (2022) [36] | |
| Was the study described as randomized, a randomized trial, a randomized clinical trial, or an RCT? | No | No | No | No | No | No |
| Was the method of randomization adequate (i.e., use of randomly generated assignment)? | No | No | No | No | No | Yes |
| Was the treatment allocation concealed (so that assignments could not be predicted)? | No | No | No | No | No | No |
| Were study participants and providers blinded to treatment group assignment? | NR | No | No | No | No | No |
| Were the people assessing the outcomes blinded to the participants’ group assignments? | NR | No | Yes | No | NR | No |
| Were the groups similar at baseline on important characteristics that could affect outcomes? | No | No | No | No | No | Yes |
| Was the overall drop-out rate from the study at endpoint 20% or lower than the number allocated to treatment? | No | No | NR | No | NR | NR |
| Was the differential drop-out rate (between treatment groups) at endpoint 15 percentage points or lower? | No | No | NR | No | NR | NR |
| Was there high adherence to the intervention protocols for each treatment group? | NA | NA | NA | NA | NA | NA |
| Were other interventions avoided or similar in the groups (e.g., similar background treatments)? | No | No | No | No | No | No |
| Were outcomes assessed using valid and reliable measures that were implemented consistently across all study participants? | Yes | Yes | Yes | Yes | Yes | Yes |
| Did the authors report that the sample size was sufficiently large to be able to detect a difference in the main outcome between groups with at least 80% power? | No | Yes | No | No | No | No |
| Were outcomes reported or subgroups analyzed prespecified (i.e., identified before analyses were conducted)? | No | No | Yes | No | No | Yes |
| Were all randomized participants analyzed in the group to which they were originally assigned, i.e., did they use an intention-to-treat analysis? | Yes | Yes | Yes | Yes | Yes | Yes |
| Study | Training Patient-Handling Devices | Ergonomics Education | Involving the Management Chain | Handling Protocol/Algorithms | Acquire Ergonomics Equipment’s | No-Manual Lifting | Others |
|---|---|---|---|---|---|---|---|
| Yassi et al. (2001) [22] | √ | √ | |||||
| Owen et al. (2002) [23] | √ | √ | |||||
| Nelson et al. (2006) [24] | √ | √ | √ | √ | √ | ||
| Black et al. (2011) [25] | √ | √ | √ | ||||
| Yang et al. (2021) [16] | √ | √ | √ | √ | |||
| Zadvinskis et al. (2009) [26] | √ | √ | |||||
| Pourhaji et al. (2020) [27] | √ | MA; W/SN | |||||
| Kozak et al. (2017) [28] | √ | √ | √ | PE | |||
| Van Eerd D et al. (2021) [29] | √ | √ | √ | N/M | |||
| Garg et al. (2012) [30] | √ | √ | √ | ||||
| Evanoff et al. (2003) [31] | √ | √ | |||||
| Li et al. (2004) [32] | √ | √ | |||||
| Nguyen et al. (2022) [33] | √ | √ | √ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sousa, A.D.; Baixinho, C.L.; Presado, M.H.; Henriques, M.A. The Effect of Interventions on Preventing Musculoskeletal Injuries Related to Nurses Work: Systematic Review. J. Pers. Med. 2023, 13, 185. https://doi.org/10.3390/jpm13020185
Sousa AD, Baixinho CL, Presado MH, Henriques MA. The Effect of Interventions on Preventing Musculoskeletal Injuries Related to Nurses Work: Systematic Review. Journal of Personalized Medicine. 2023; 13(2):185. https://doi.org/10.3390/jpm13020185
Chicago/Turabian StyleSousa, Armando David, Cristina Lavareda Baixinho, Maria Helena Presado, and Maria Adriana Henriques. 2023. "The Effect of Interventions on Preventing Musculoskeletal Injuries Related to Nurses Work: Systematic Review" Journal of Personalized Medicine 13, no. 2: 185. https://doi.org/10.3390/jpm13020185