1. Introduction
With a worldwide prevalence of 43.6 million in 2016, atrial fibrillation (AFib) is an increasingly frequent pathology that also creates a significant impact on healthcare costs [
1,
2,
3]. The catheter ablation procedure for the treatment of AFib was first introduced during the 1990s, and when compared with treatment using antiarrhythmic drugs, it improves quality of life by better restoring sinus rhythm [
4,
5] with a lower recurrence rate [
6].
While initially these ablation procedures were performed under conscious sedation, they are now most often performed under general anesthesia [
5]. This approach allows for a comfortable and motionless patient [
7,
8] throughout a potentially long procedure. General anesthesia has been shown to be associated with better stability of the ablation catheter, a better contact force with tissues, and shorter fluoroscopic and procedural times [
8,
9].
Unfortunately, the movement of the chest and its contents during mechanical ventilation may interfere with the procedure. This has led to the use of high-frequency jet ventilation (HFJV) by some practitioners during ablation procedures [
7,
10]. The stability of the mapping and ablation catheter, linked to the near immobility of the thoracic structures during HFJV, allows a reduction in operating and fluoroscopic times, fewer recurrences and improves patient outcomes [
7,
8,
11,
12,
13,
14].
However, despite these advantages, HFJV is currently only used in 14% of ablations in the United States and Canada and 4% elsewhere [
5]. This type of ventilation requires trained operators, the appropriate equipment and close monitoring of gas exchange.
Outside of atrial ablation procedures, HFJV is also proposed for use during radiofrequency or cryoablation of hepatic, renal and pulmonary tumors [
15,
16,
17,
18]. It has also been used for shock wave lithotripsy of kidney stones [
19]. Various authors argue that the use of HFJV limits thoracic, diaphragmatic and intraabdominal organ movements [
15,
16,
17,
18,
19]. This decreased movement is hypothesized to lead to better target contact, lower fluoroscopic time and lower procedure times, with potentially better outcomes. Denys et al. demonstrated the minimal movement of hepatic, renal and pulmonary tumors during HFJV using CT scan measurements. For pulmonary vein isolation, HFJV has also been shown to be associated with optimized catheter contact and better outcomes [
7,
12,
13,
14]. The proposed mechanism is likely at least partially related to the lower tidal volumes for HFJV when compared to normal mechanical ventilation. During HFJV, the total tidal volume consists of both the volume delivered by jet ventilation and the volume added by the Venturi effect [
20]. This volume has been shown to be lower than the tidal volume during normal mechanical ventilation [
21,
22].
To our knowledge, no study has quantified this near immobility of cardiac structures observed during HFJV. As such, the primary objective of our study is to measure the displacement of the heart and, in particular, that of the coronary sinus during conventional mechanical ventilation (IPPV) versus HFJV in order to quantify this proposed decreased movement. This was performed using the EnSite Precision™ cardiac mapping system (Abbott Cardiovascular, Plymouth MN, USA) connected to the mapping and ablation catheter placed in the coronary sinus before the start of the ablation procedure.
We hypothesize that the use of HFJV compared to mechanical ventilation will cause less displacement of heart structures, measured as the movement of the Inquiry catheter (Abbott Cardiovascular, Plymouth MN, USA) within the coronary sinus.
2. Materials and Methods
This single-center study was approved by the Ethics Committee of Erasme University Hospital on 9 May 2019 (Chairperson Pr JM Boeynaems, reference CCB B406201939759). After written informed consent, 21 patients scheduled for atrial fibrillation ablation under general anesthesia were included in this prospective, interventional study. Inclusion criteria were: Patients over 18 years scheduled for ablation of atrial fibrillation, body mass Index (BMI) ≤ 30 kg/m2 and American Society of Anesthesiologists (ASA) score 1–3. Exclusion criteria were: Refusal to participate in the study, pre-existing pulmonary disease, and heart failure defined as a left ventricular ejection fraction <30%.
Patients were equipped with two peripheral intravenous lines, standard monitoring consisting of pulse oximetry, ECG, non-invasive blood pressure monitoring as well as a radial arterial catheter inserted before anesthesia induction. Anesthesia was induced by a target-controlled infusion of propofol and remifentanil. Muscle relaxation was obtained using bolus rocuronium injections adjusted to keep train of four ratio (TOF) <2, measured using a TOF-Watch monitor (Organon, Swords, Ireland). A transesophageal echo (TEE) probe was used for the transeptal puncture and to assess volume status. Mean arterial pressure was maintained at >65 mm Hg using a provider-adjusted norepinephrine infusion.
After the induction of anesthesia, a Wei jet endotracheal tube (Well Lead Medical Co., Ltd., Guangzhou, China) was inserted. This tube allows either conventional mechanical ventilation or HFJV. Positive pressure mechanical ventilation was started with a tidal volume of 5 to 8.5 mL/kg of ideal body weight, a frequency of 10 to 14 breaths per minute adapted to obtain an end-tidal CO2 between 35 and 45 mm Hg, an inspired oxygen fraction adapted to obtain a SpO2 greater than 95%, and a positive end-expiratory pressure (PEEP) of 0–6 cm H2O. HFJV was delivered by a Monsoon III jet ventilator (Acutronic Medical Systems AG, Hirzel, Switzerland). Initial conditions of HFJV were a driving pressure of 1 to 2 bars, an inspired oxygen fraction of 40 to 50%, an injection frequency of 100 to 150 breaths per minute and an inspiratory time to expiratory time (I/E) ratio of 30% to 35%. The gas humidification system of the jet ventilator was used during the procedure.
A blood gas measurement was performed every 30 min [
23]; the driving pressure and the I/E ratio were then adjusted in order to maintain an arterial pH between 7.35 and 7.45 and a PaCO
2 between 35 and 45 mmHg.
The inspired oxygen fraction was set between 40 and 50% and increased if necessary in order to maintain arterial oxygen saturation greater than or equal to 95% of SpO2.
2.1. Ablation Procedure
Atrial fibrillation ablation was done using radiofrequency (Tacticath, Abbott Cardiovascular, Plymouth MN, USA) subsequent to electrophysiological mapping. The mapping catheter (HD grid, Abbott Cardiovascular, Plymouth MN, USA) and a coronary sinus catheter (Abbott Inquiry, Abbott Cardiovascular, Plymouth MN, USA) were inserted through femoral venous access. The mapping and the coronary sinus catheter were connected to the Abbott EnSite Precision cardiac mapping system (Abbott Cardiovascular, Plymouth MN, USA). After a stabilization period, the coronary sinus catheter was locked into position. This reference point was used to measure cardiac displacement during the study protocol. The coronary sinus catheter, together with the Abbott EnSite Precision system, is able to measure a minimum displacement of 0.34 mm [
24,
25].
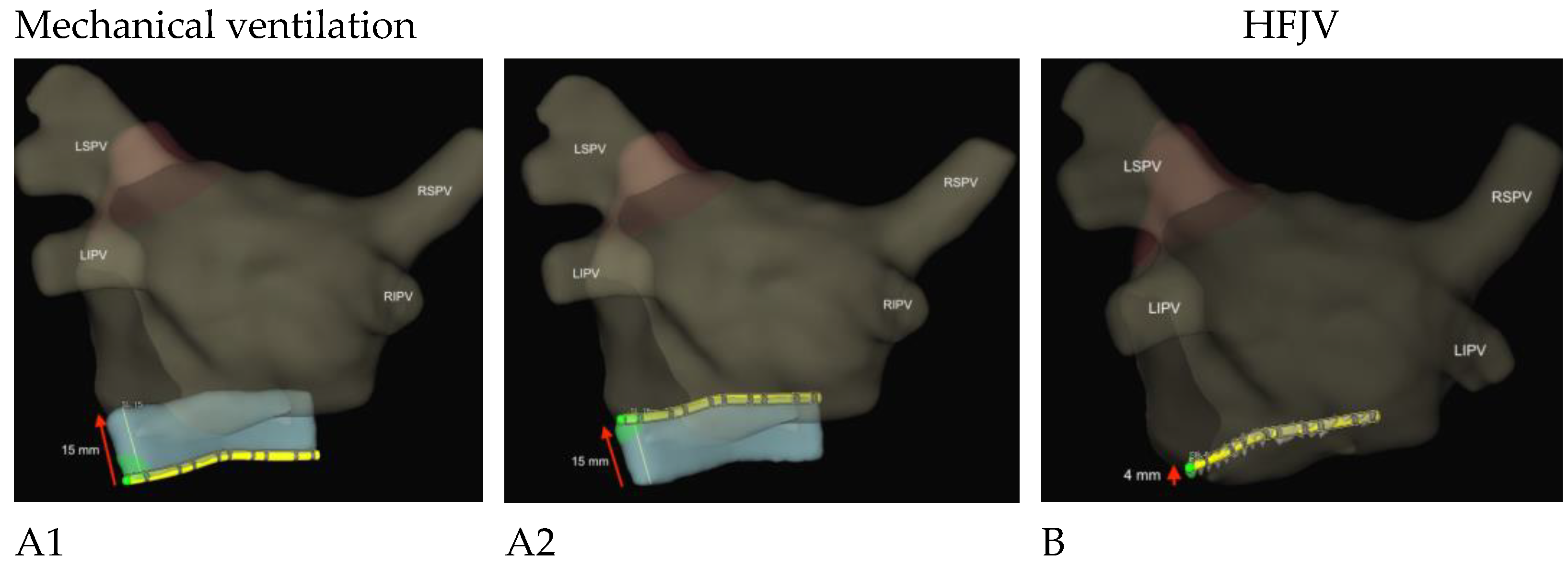
The Abbott Inquiry catheter has multiple electrodes to measure its position. These electrodes are placed in a specific pattern: one electrode, 2 mm spacing, one electrode, 5 mm spacing, and this pattern is repeated five times. The electrodes can be seen in
Figure 1 as black lines on the catheter. A region of interest, seen in blue in
Figure 1, is defined as a three-dimensional volume around the catheter, and the software measures all movement in any direction inside this volume. The software needs between 30 to 45 s to acquire a stable signal to make a correct measurement. We measured the maximum catheter displacement in any direction after this stabilization period. During mechanical ventilation, this represents the movement between the end-inspiratory and end-expiratory positions. During HFJV, there is only an oscillation of the catheter induced by the jet ventilation.
The primary endpoint was observed mobility, which was calculated as the displacement of the heart during conventional mechanical ventilation (IPPV) versus HFJV. This measurement was performed by the EnSite Precision™ cardiac mapping system connected to the Inquiry catheter placed in the coronary sinus before the start of the ablation procedure.
The secondary objectives were to assess the quality of ventilation by monitoring PaO2 and PaCO2 during HFJV.
2.2. Statistics
Based on observational data in our institution, we calculated a required sample size of 15 patients to show a significant difference between the 2 ventilation modes. Assuming a 25% dropout ratio, we decided to include at least 21 patients. Data are presented as median and 25th, 75th percentiles.
The primary endpoint was compared during conventional ventilation and jet ventilation using Student’s t-test for paired data.
Ventilation parameters were compared using an analysis of variance for repeated measures with mixed models. If a p-value <0.05 was obtained for the analysis of variance, a Bonferroni test was used for individual comparison of time points.
All statistical tests were two-tailed, and a p-value < 0.05 was considered statistically significant. All analyses were performed using the NCSS 20.0.3 statistical package (NCSS, LLC; Kaysville, UT, USA).
3. Results
From 22 May 2019 to 11 March 2020, 73 patients scheduled for AFib ablation were screened. Of these, 52 patients were excluded: 14 patients refused to participate, 27 patients did not meet the inclusion criteria or had an exclusion criterion (3 pulmonary arterial hypertension, 6 pulmonary diseases, 5 heart failures with an ejection fraction less than 30%, 13 BMI greater than 30 kg/m2) and 11 patients had a logistical problem (e.g., HFJV ventilation not available).
Patient characteristics are shown in
Table 1.
Coronary Sinus Movement
The primary endpoint, coronary sinus movement during ventilation, was decreased during jet ventilation compared with conventional ventilation.
The median [Q1–Q4] displacement was 2.0 [0.6–2.8] mm during HFJV and 10.5 [9.3–13.0] mm during conventional ventilation (p < 0.000001).
The three images (
Figure 1) illustrate this displacement during conventional ventilation (15 mm) and HFJV (4 mm) in patient n ° 1.
Table 2 shows the evolution of oxygenation and carbon dioxide elimination.
In both groups, 86% of patients needed a norepinephrine infusion to maintain arterial blood pressure above 65 mm Hg.
4. Discussion
In this study, we have demonstrated that during HFJV, as compared to classic mechanical ventilation, coronary sinus movement is significantly decreased. Many authors praise HFJV for a motionless field, but this has rarely been quantified. Denys et al. measured the movement of renal, hepatic and pulmonary tumors during radiofrequency treatment by CT scan [
18]. They found movements of less than 0.3 mm in the
x- and
y-axis; in the
z-axis, the movement was less than the slice thickness of 3.75 mm. Goode et al. found that for AFib ablation, HFJV leads to a shorter procedural time, more stable conditions in the left atrium and fewer ablation attempts [
7]. They explain their findings as secondary to a more stable field with less movement during HFJV. Sivasambu et al. reported a better outcome for AFib ablation using HFJV as the time to atrial fibrillation recurrence was greater after HFJV [
12].
Our study is in concordance with these and other studies from the literature, citing a stable field as the main reason for the improved quality of AFib ablation using HFJV [
10]. One strength of our study is the use of the cardiac mapping system to measure coronary sinus displacement. The EnSight system is capable of measuring very small movements, thus allowing for a true measurement of the movement of cardiac structures. Additionally, every patient was their own control as measurements were done in every patient during mechanical ventilation and during HFJV.
Oxygenation and paCO
2 remained stable throughout the procedure, with no difference between HFJV and traditional mechanical ventilation. PaO
2 and SaO
2 were similar between the two ventilation modes without the need to increase the inspired oxygen fraction. Carlon et al. also demonstrated that at a similar PEEP level, HFJV and conventional mechanical ventilation resulted in similar arterial oxygenation [
26]. PaCO
2 is dependent on the driving pressure and the I/E ratio. The average driving pressure in our study did not exceed 2 bar, staying within the limits of safety [
21,
22]. The need to do arterial blood gas analysis to measure paCO
2 is a disadvantage of HFJV [
27]; however, an arterial line is also useful for repeated activated clotting time measurements necessary in atrial fibrillation ablation. As atrial fibrillation ablation becomes a common procedure, it should be noted that many institutions no longer perform routinely invasive arterial pressure management. In this context, the difficulty in measuring paCO
2 during HFJV represents a challenge. We must emphasize that our study was not powered to evaluate a difference within the secondary outcomes, so these findings are hypothesis-generating only.
When discussing limitations, one might argue that the coronary sinus catheter is moving in the much larger coronary sinus and, thus, is not a correct surrogate for the movement of cardiac structures. However, in this study, after placement in the coronary sinus, the Inquiry catheter was locked in this position, making an isolated movement of the catheter highly improbable. As discussed above, there have been studies linking HFJV with improved atrial fibrillation ablation outcomes [
12,
13]. As our study quantifies the minimal movement of cardiac structures during HFJV, it is tempting to link the absence of movement to better contact between the cardiac structures and the ablation catheter and, thus, better results. However, this hypothesis must be proven in prospective randomized trials before advocating for the more widespread use of HFJV [
28]. There may be potential unforeseen issues that may only present in randomized studies. For instance, Simvasambu et al. found that norepinephrine infusion was required in a higher proportion of patients during HFJV [
12]. In our study, the same proportion of patients (86%) needed norepinephrine infusions to keep mean arterial pressure above 65 mm Hg during mechanical ventilation as well as during HFJV, although our crossover design is slightly different. Our study was designed as an observational, pragmatic study, the sequence of ventilation modes was not randomized, and patients were ventilated according to standard practice. Finally, we limited our study to patients with a BMI ≤ 30 kg/m2, and as Hu et al. demonstrated, HFJV may be more challenging in obese patients [
29].
5. Conclusions
Cardiac displacement during HFJV is 5 times less than during conventional mechanical ventilation. This study quantifies the minimal movement of cardiac structures in patients undergoing atrial fibrillation ablation ventilated using HFJV. Whether this immobility leads to a better outcome must be confirmed in further prospective trials.
Author Contributions
Conceptualization, C.M.; methodology, C.M. and P.N.; validation, T.T.; formal analysis, C.M. and E.E.; investigation, C.M., P.N., R.C.-A. and J.-P.A.D.T.; data curation, C.M. and E.E.; writing—original draft preparation, C.M..; writing—review and editing, C.M., B.A. and D.S.; visualization, C.M., E.E. and D.S.; supervision, C.M. and T.T.; project administration, C.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Erasme University Hospital on 9 May 2019 (Chairperson Pr JM Boeynaems, reference CCB B406201939759).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chugh, S.S.; Havmoeller, R.; Narayanan, K.; Singh, D.; Rienstra, M.; Benjamin, E.J.; Gillum, R.F.; Kim, Y.H.; McAnulty, J.H., Jr.; Zheng, Z.J.; et al. Worldwide epidemiology of atrial fibrillation: A Global Burden of Disease 2010 Study. Circulation 2014, 129, 837–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allan, V.; Honarbakhsh, S.; Casas, J.P.; Wallace, J.; Hunter, R.; Schilling, R.; Perel, P.; Morley, K.; Banerjee, A.; Hemingway, H. Are cardiovascular risk factors also associated with the incidence of atrial fibrillation? A systematic review and field synopsis of 23 factors in 32 population-based cohorts of 20 million participants. Thromb. Haemost. 2017, 117, 837–850. [Google Scholar] [CrossRef] [Green Version]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomstrom-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Wilber, D.J.; Pappone, C.; Neuzil, P.; De Paola, A.; Marchlinski, F.; Natale, A.; Macle, L.; Daoud, E.G.; Calkins, H.; Hall, B.; et al. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: A randomized controlled trial. Jama 2010, 303, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Calkins, H.; Hindricks, G.; Cappato, R.; Kim, Y.H.; Saad, E.B.; Aguinaga, L.; Akar, J.G.; Badhwar, V.; Brugada, J.; Camm, J.; et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm 2017, 14, e275–e444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Packer, D.L.; Mark, D.B.; Robb, R.A.; Monahan, K.H.; Bahnson, T.D.; Poole, J.E.; Noseworthy, P.A.; Rosenberg, Y.D.; Jeffries, N.; Mitchell, L.B.; et al. Effect of Catheter Ablation vs. Antiarrhythmic Drug Therapy on Mortality, Stroke, Bleeding, and Cardiac Arrest Among Patients With Atrial Fibrillation: The CABANA Randomized Clinical Trial. Jama 2019, 321, 1261–1274. [Google Scholar] [CrossRef]
- Goode, J.S., Jr.; Taylor, R.L.; Buffington, C.W.; Klain, M.M.; Schwartzman, D. High-frequency jet ventilation: Utility in posterior left atrial catheter ablation. Heart Rhythm 2006, 3, 13–19. [Google Scholar] [CrossRef]
- Di Biase, L.; Conti, S.; Mohanty, P.; Bai, R.; Sanchez, J.; Walton, D.; John, A.; Santangeli, P.; Elayi, C.S.; Beheiry, S.; et al. General anesthesia reduces the prevalence of pulmonary vein reconnection during repeat ablation when compared with conscious sedation: Results from a randomized study. Heart Rhythm 2011, 8, 368–372. [Google Scholar] [CrossRef]
- Chikata, A.; Kato, T.; Yaegashi, T.; Sakagami, S.; Kato, C.; Saeki, T.; Kawai, K.; Takashima, S.I.; Murai, H.; Usui, S.; et al. General anesthesia improves contact force and reduces gap formation in pulmonary vein isolation: A comparison with conscious sedation. Heart Vessel. 2017, 32, 997–1005. [Google Scholar] [CrossRef]
- Alvarez, C.K.; Zweibel, S.; Stangle, A.; Panza, G.; May, T.; Marieb, M. Anesthetic Considerations in the Electrophysiology Laboratory: A Comprehensive Review. J. Cardiothorac. Vasc. Anesth. 2023, 37, 96–111. [Google Scholar] [CrossRef]
- Elkassabany, N.; Garcia, F.; Tschabrunn, C.; Raiten, J.; Gao, W.; Chaichana, K.; Dixit, S.; Speck, R.M.; Zado, E.; Marchlinski, F.; et al. Anesthetic management of patients undergoing pulmonary vein isolation for treatment of atrial fibrillation using high-frequency jet ventilation. J. Cardiothorac. Vasc. Anesth. 2012, 26, 433–438. [Google Scholar] [CrossRef]
- Sivasambu, B.; Hakim, J.B.; Barodka, V.; Chrispin, J.; Berger, R.D.; Ashikaga, H.; Ciuffo, L.; Tao, S.; Calkins, H.; Marine, J.E.; et al. Initiation of a High-Frequency Jet Ventilation Strategy for Catheter Ablation for Atrial Fibrillation: Safety and Outcomes Data. JACC Clin. Electrophysiol. 2018, 4, 1519–1525. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, M.D.; Garcia, F.C.; Mandel, J.E.; Elkassabany, N.; Zado, E.S.; Riley, M.P.; Cooper, J.M.; Bala, R.; Frankel, D.S.; Lin, D.; et al. Efforts to enhance catheter stability improve atrial fibrillation ablation outcome. Heart Rhythm 2013, 10, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Aizer, A.; Qiu, J.K.; Cheng, A.V.; Wu, P.B.; Barbhaiya, C.R.; Jankelson, L.; Linton, P.; Bernstein, S.A.; Park, D.S.; Holmes, D.S.; et al. Rapid pacing and high-frequency jet ventilation additively improve catheter stability during atrial fibrillation ablation. J. Cardiovasc. Electrophysiol. 2020, 31, 1678–1686. [Google Scholar] [CrossRef]
- Raiten, J.; Elkassabany, N.; Mandel, J.E. The use of high-frequency jet ventilation for out of operating room anesthesia. Curr. Opin. Anaesthesiol. 2012, 25, 482–485. [Google Scholar] [CrossRef]
- Buchan, T.; Walkden, M.; Jenkins, K.; Sultan, P.; Bandula, S. High-Frequency Jet Ventilation During Cryoablation of Small Renal Tumours. Cardiovasc. Interv. Radiol. 2018, 41, 1067–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galmen, K.; Harbut, P.; Freedman, J.; Jakobsson, J.G. High frequency jet ventilation for motion management during ablation procedures, a narrative review. Acta Anaesthesiol. Scand. 2017, 61, 1066–1074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denys, A.; Lachenal, Y.; Duran, R.; Chollet-Rivier, M.; Bize, P. Use of high-frequency jet ventilation for percutaneous tumor ablation. Cardiovasc. Interv. Radiol. 2014, 37, 140–146. [Google Scholar] [CrossRef] [Green Version]
- Mucksavage, P.; Mayer, W.A.; Mandel, J.E.; Van Arsdalen, K.N. High-frequency jet ventilation is beneficial during shock wave lithotripsy utilizing a newer unit with a narrower focal zone. Can. Urol. Assoc. J. J. De L’association Des Urol. Du Can. 2010, 4, 333–335. [Google Scholar] [CrossRef]
- Conlon EC. High-frequency Jet Ventilation Anesthesia Tutorial of the Week. Available online: https://resources.wfsahq.org/atotw/high-frequency-jet-ventilation-anaesthesia-tutorial-of-the-week-271. (accessed on 16 August 2022).
- Klain, M.; Keszler, H. High-frequency jet ventilation. Surg. Clin. N. Am. 1985, 65, 917–930. [Google Scholar] [CrossRef]
- Evans, E.; Biro, P.; Bedforth, N. Jet ventilation. Contin. Educ. Anaesth. Crit. Care Pain 2007, 7, 2–5. [Google Scholar] [CrossRef]
- Fujii, S.; Zhou, J.R.; Dhir, A. Anesthesia for Cardiac Ablation. J. Cardiothorac. Vasc. Anesth. 2018, 32, 1892–1910. [Google Scholar] [CrossRef] [PubMed]
- Abbott. INSTRUCTIONS FOR USE. In EnSite Precision™ Cardiac Mapping System Model EE3000, software 2.0; (document on file); Abbott Cardiovascular: Chicago, IL, USA, 2016. [Google Scholar]
- Abbott. ENSITE PRECISION™ CARDIAC MAPPING SYSTEM, Accuracy of the EnSite™ NavX™ Navigation and Visualization Technology, Sensor Enabled™, SJM-ENS-0916-0097; (document on file); Abbott Cardiovascular: Chicago, IL, USA.
- Carlon, G.C.; Howland, W.S.; Ray, C.; Miodownik, S.; Griffin, J.P.; Groeger, J.S. High-frequency jet ventilation. A prospective randomized evaluation. Chest 1983, 84, 551–559. [Google Scholar] [CrossRef]
- Babapoor-Farrokhran, S.; Alzubi, J.; Port, Z.; Khraisha, O.; Mainigi, S.K.J. Utility of high-frequency jet ventilation in atrial fibrillation ablation. J. Innov. Cardiac. Rhythm Manag. 2021, 12, 4590–4593. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Morton, J.B.; Halloran, K.; Spence, S.J.; Lee, G.; Wong, M.C.; Kistler, P.M.; Kalman, J.M. Effect of respiration on catheter-tissue contact force during ablation of atrial arrhythmias. Heart Rhythm 2012, 9, 1041–1047e1. [Google Scholar] [CrossRef]
- Tang, F.; Li, S.Q.; Chen, L.H.; Miao, C.H. The comparison of various ventilation modes and the association of risk factors with CO(2) retention during suspension laryngoscopy. Laryngoscope 2011, 121, 503–508. [Google Scholar] [CrossRef] [PubMed]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 

{kind=link}