
Deep Learning-Based Segmentation and Volume Calculation of Pediatric Lymphoma on Contrast-Enhanced Computed Tomographies
 ,
,
Abstract
:1. Introduction
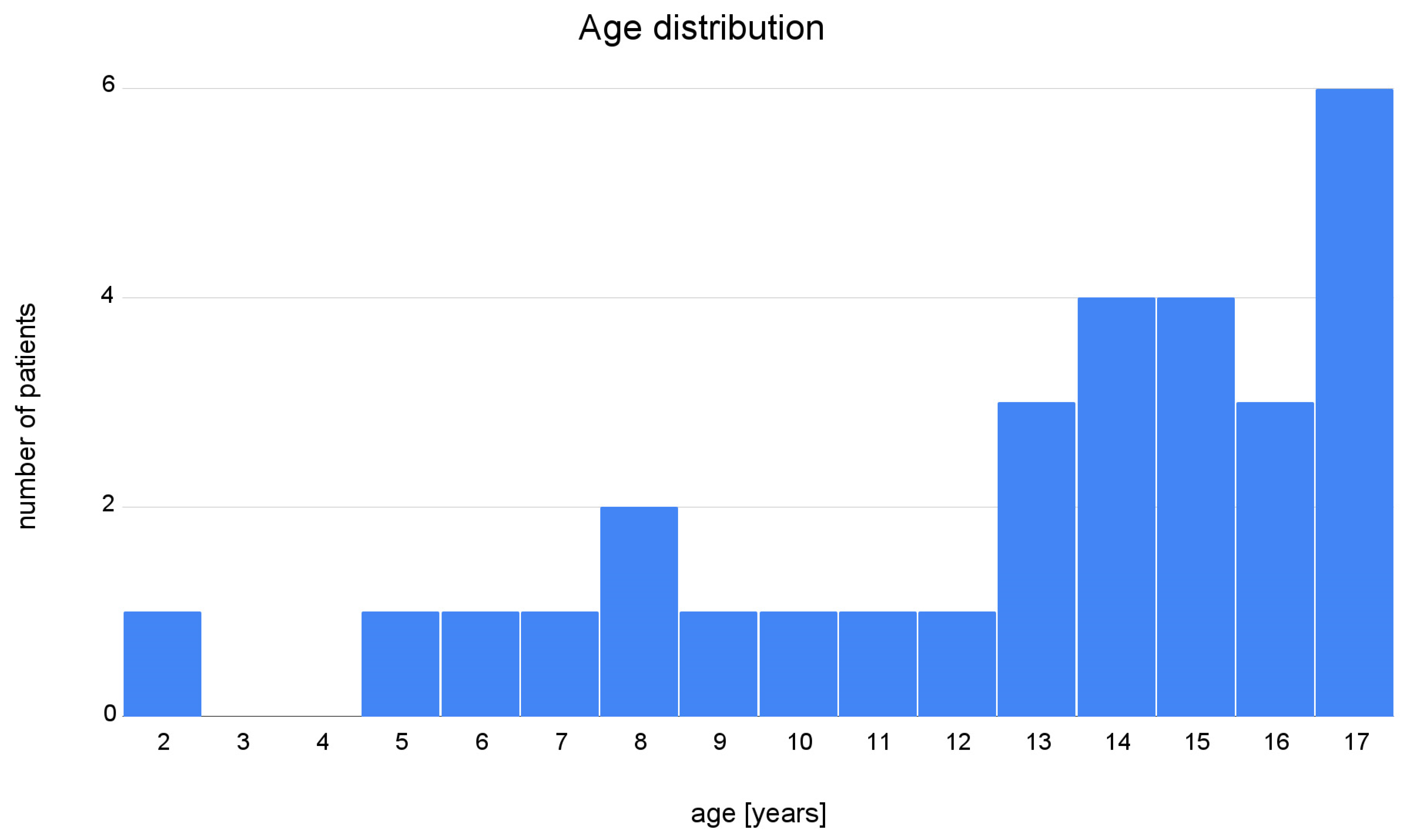
2. Materials and Methods
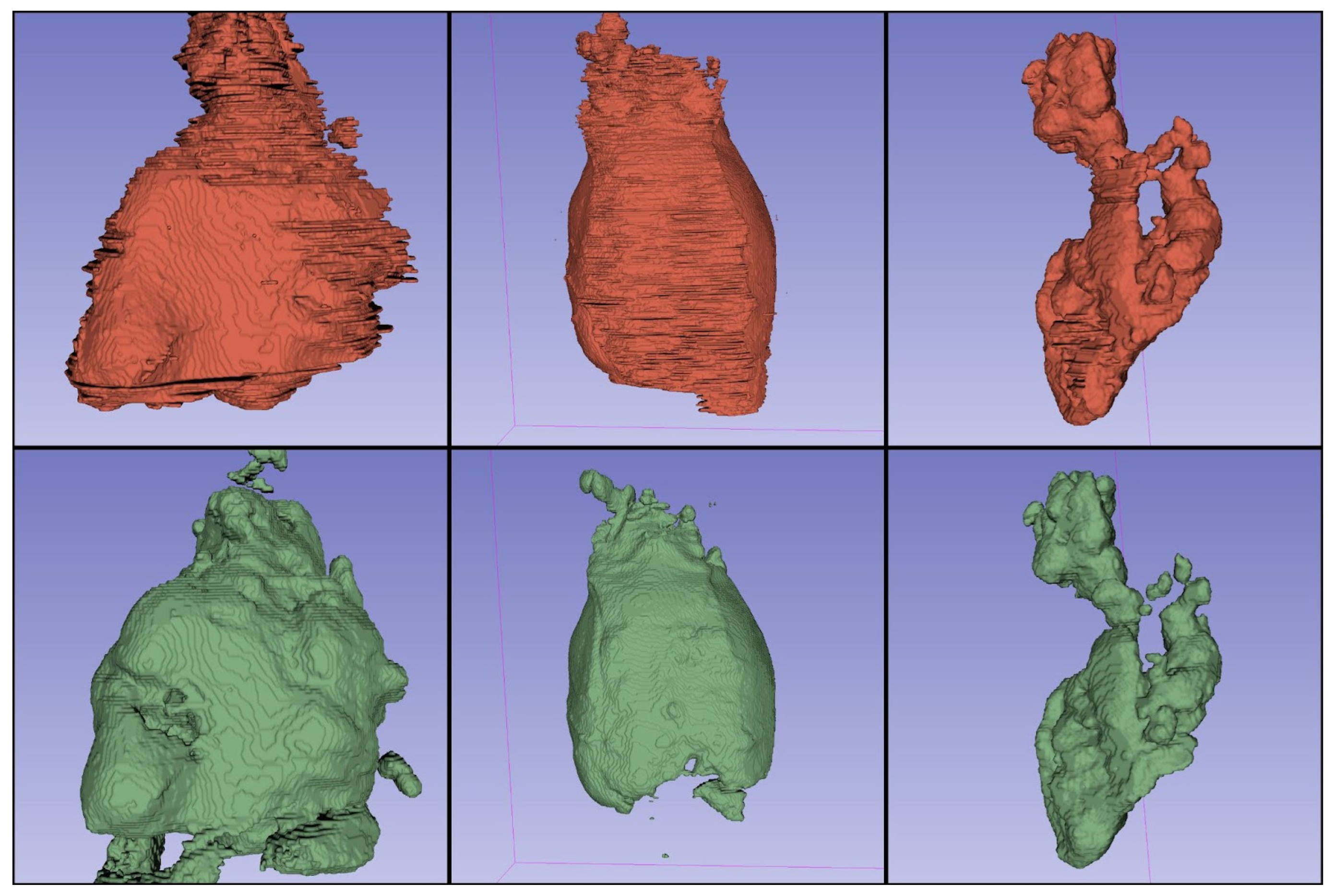
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Morton, L.M.; Wang, S.S.; Devesa, S.S.; Hartge, P.; Weisenburger, D.D.; Linet, M.S. Lymphoma Incidence Patterns by WHO Subtype in the United States, 1992–2001. Blood 2006, 107, 265–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Kostakoglu, L.; Cheson, B.D. Current Role of FDG PET/CT in Lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1004–1027. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A.; Alliance, Australasian Leukaemia and Lymphoma Group; Eastern Cooperative Oncology Group; European Mantle Cell Lymphoma Consortium; et al. Recommendations for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The Lugano Classification. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2014, 32, 3059–3068. [Google Scholar] [CrossRef]
- Barrington, S.F.; Mikhaeel, N.G.; Kostakoglu, L.; Meignan, M.; Hutchings, M.; Müeller, S.P.; Schwartz, L.H.; Zucca, E.; Fisher, R.I.; Trotman, J.; et al. Role of Imaging in the Staging and Response Assessment of Lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J. Clin. Oncol. 2014, 32, 3048–3058. [Google Scholar] [CrossRef] [PubMed]
- Younes, A.; Hilden, P.; Coiffier, B.; Hagenbeek, A.; Salles, G.; Wilson, W.; Seymour, J.F.; Kelly, K.; Gribben, J.; Pfreunschuh, M.; et al. International Working Group Consensus Response Evaluation Criteria in Lymphoma (RECIL 2017). Ann. Oncol. 2017, 28, 1436–1447. [Google Scholar] [CrossRef]
- Möller, J.; Steyn, T.; Combrinck, N.; Joubert, G.; Sherriff, A.; Rensburg, J.J.V. Inter-Observer Variability Influences the Lugano Classification When Restaging Lymphoma. SA J. Radiol. 2018, 22, 1357. [Google Scholar] [CrossRef]
- Girinsky, T.; Ghalibafian, M.; Bonniaud, G.; Bayla, A.; Magne, N.; Ferreira, I.; Lumbroso, J. Is FDG-PET Scan in Patients with Early Stage Hodgkin Lymphoma of Any Value in the Implementation of the Involved-Node Radiotherapy Concept and Dose Painting? Radiother. Oncol. 2007, 85, 178–186. [Google Scholar] [CrossRef]
- Batlevi, C.L.; De Frank, S.; Stewart, C.; Hamlin, P.A.; Matasar, M.J.; Gerecitano, J.F.; Moskowitz, A.J.; Hamilton, A.M.; Zelenetz, A.D.; Drullinsky, P.; et al. Phase I/II Clinical Trial of Ibrutinib and Buparlisib in Relapsed/Refractory Diffuse Large B-Cell Lymphoma, Mantle Cell Lymphoma, and Follicular Lymphoma. J. Clin. Oncol. 2018, 36, 7520. [Google Scholar] [CrossRef]
- Munakata, W.; Terauchi, T.; Maruyama, D.; Nagai, H. Revised Staging System for Malignant Lymphoma Based on the Lugano Classification. Jpn. J. Clin. Oncol. 2019, 49, 895–900. [Google Scholar] [CrossRef]
- Juweid, M.E. FDG-PET/CT in Lymphoma. In Positron Emission Tomography, 1st ed.; Juweid, M.E., Hoekstra, O.S., Eds.; Humana Press: Totowa, NJ, USA, 2011; pp. 1–19. ISBN 978-1-61779-062-1. [Google Scholar]
- Im, H.-J.; Bradshaw, T.; Solaiyappan, M.; Cho, S.Y. Current Methods to Define Metabolic Tumor Volume in Positron Emission Tomography: Which One Is Better? Nucl. Med. Mol. Imaging 2018, 52, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Sasanelli, M.; Meignan, M.; Haioun, C.; Berriolo-Riedinger, A.; Casasnovas, R.-O.; Biggi, A.; Gallamini, A.; Siegel, B.A.; Cashen, A.F.; Véra, P.; et al. Pretherapy Metabolic Tumour Volume Is an Independent Predictor of Outcome in Patients with Diffuse Large B-Cell Lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 2017–2022. [Google Scholar] [CrossRef] [PubMed]
- Schöder, H.; Moskowitz, C.H. Metabolic Tumor Volume in Lymphoma: Hype or Hope? J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2016, 34, 3591–3594. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Law, M.W.-M.; Khong, P.-L. Whole-Body PET/CT Scanning: Estimation of Radiation Dose and Cancer Risk. Radiology 2009, 251, 166–174. [Google Scholar] [CrossRef]
- Littooij, A.S.; Kwee, T.C.; Barber, I.; Granata, C.; Vermoolen, M.A.; Enríquez, G.; Zsíros, J.; Soh, S.Y.; de Keizer, B.; Beek, F.J.A.; et al. Whole-Body MRI for Initial Staging of Paediatric Lymphoma: Prospective Comparison to an FDG-PET/CT-Based Reference Standard. Eur. Radiol. 2014, 24, 1153–1165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baues, C.; Görgen, H.; Semrau, R.; Nast-Kolb, B.; Assenmacher, K.; Celik, E.; Morgenthaler, J.; Rosenbrock, J.; Trommer, M.; Houbois, C.; et al. Volumetric Assessment of Mediastinal Lymphoma Masses in Hodgkin Lymphoma. Leuk. Lymphoma 2019, 60, 3244–3250. [Google Scholar] [CrossRef]
- Gayathri Devi, K.; Radhakrishnan, R. Automatic Segmentation of Colon in 3D CT Images and Removal of Opacified Fluid Using Cascade Feed Forward Neural Network. Comput. Math. Methods Med. 2015, 2015, 670739. [Google Scholar] [CrossRef]
- Hofmanninger, J.; Prayer, F.; Pan, J.; Röhrich, S.; Prosch, H.; Langs, G. Automatic Lung Segmentation in Routine Imaging Is Primarily a Data Diversity Problem, Not a Methodology Problem. Eur. Radiol. Exp. 2020, 4, 50. [Google Scholar] [CrossRef]
- Wasserthal, J.; Meyer, M.; Breit, H.-C.; Cyriac, J.; Yang, S.; Segeroth, M. TotalSegmentator: Robust Segmentation of 104 Anatomical Structures in CT Images 2022. arXiv 2022, arXiv:2208.05868. [Google Scholar]
- Klimont, M.; Oronowicz-Jaśkowiak, A.; Flieger, M.; Rzeszutek, J.; Jończyk-Potoczna, K. Pediatric Chest Lymphoma with Segmentation. Zenodo 2022. [Google Scholar] [CrossRef]
- Klimont, M.; Oronowicz-Jaśkowiak, A.; Flieger, M.; Rzeszutek, J.; Jończyk-Potoczna, K. Pretrained Model for Pediatric Chest Lymphoma Segmentation. Zenodo 2022. [Google Scholar] [CrossRef]
- Deep Learning-Based Segmentation and Volume Calculation of Pediatric Lymphoma as an Alternative for Staging and Monitoring. Available online: https://github.com/fast-radiology/lymphoma (accessed on 13 November 2022).
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an Image Computing Platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5–10 October 2015; pp. 234–241. [Google Scholar]
- Siddique, N.; Paheding, S.; Elkin, C.P.; Devabhaktuni, V. U-Net and Its Variants for Medical Image Segmentation: A Review of Theory and Applications. IEEE Access 2021, 9, 82031–82057. [Google Scholar] [CrossRef]
- Isensee, F.; Jaeger, P.F.; Kohl, S.A.A.; Petersen, J.; Maier-Hein, K.H. NnU-Net: A Self-Configuring Method for Deep Learning-Based Biomedical Image Segmentation. Nat. Methods 2021, 18, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Fastai. Available online: https://docs.fast.ai/index.html (accessed on 1 November 2022).
- Taha, A.A.; Hanbury, A. Metrics for Evaluating 3D Medical Image Segmentation: Analysis, Selection, and Tool. BMC Med. Imaging 2015, 15, 29. [Google Scholar] [CrossRef] [Green Version]
- Lim, D.S.W.; Makmur, A.; Zhu, L.; Zhang, W.; Cheng, A.J.L.; Sia, D.S.Y.; Eide, S.E.; Ong, H.Y.; Jagmohan, P.; Tan, W.C.; et al. Improved Productivity Using Deep Learning–Assisted Reporting for Lumbar Spine MRI. Radiology 2022, 305, 220076. [Google Scholar] [CrossRef]
- Tingelhoff, K.; Eichhorn, K.W.G.; Wagner, I.; Kunkel, M.E.; Moral, A.I.; Rilk, M.E.; Wahl, F.M.; Bootz, F. Analysis of Manual Segmentation in Paranasal CT Images. Eur. Arch. Otorhinolaryngol. 2008, 265, 1061–1070. [Google Scholar] [CrossRef]
- Roth, H.; Lu, L.; Seff, A.; Cherry, K.M.; Hoffman, J.; Wang, S.; Liu, J.; Turkbey, E.; Summers, R.M. A New 2.5 D Representation for Lymph Node Detection in CT. Med. Image Comput. Comput. Assist. Interv. 2014, 17, 520–527. [Google Scholar]
- Einstein, D.M.; Singer, A.A.; Chilcote, W.A.; Desai, R.K. Abdominal Lymphadenopathy: Spectrum of CT Findings. Radiographics 1991, 11, 457–472. [Google Scholar] [CrossRef] [Green Version]
- Dornheim, J.; Seim, H.; Preim, B.; Hertel, I.; Strauss, G. Segmentation of Neck Lymph Nodes in CT Datasets with Stable 3D Mass-Spring Models: Segmentation of Neck Lymph Nodes. Acad. Radiol. 2007, 14, 1389–1399. [Google Scholar] [CrossRef]
- Feulner, J.; Kevin Zhou, S.; Hammon, M.; Hornegger, J.; Comaniciu, D. Lymph Node Detection and Segmentation in Chest CT Data Using Discriminative Learning and a Spatial Prior. Med. Image Anal. 2013, 17, 254–270. [Google Scholar] [CrossRef] [PubMed]
- Iuga, A.-I.; Carolus, H.; Höink, A.J.; Brosch, T.; Klinder, T.; Maintz, D.; Persigehl, T.; Baeßler, B.; Püsken, M. Automated Detection and Segmentation of Thoracic Lymph Nodes from CT Using 3D Foveal Fully Convolutional Neural Networks. BMC Med. Imaging 2021, 21, 69. [Google Scholar] [CrossRef] [PubMed]
- Varoquaux, G.; Cheplygina, V. Machine Learning for Medical Imaging: Methodological Failures and Recommendations for the Future. Npj Digit. Med. 2022, 5, 48. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Region/Issue | Solution |
|---|---|
| Cervical lymph nodes not always distinguishable from surrounding tissues | Include cervical lymph nodes whenever possible |
| Unsharp border between lymphoma and thymic tissue | Exclude thymus from segmentation only when a clear border between lymphoma and thymus is visible; include thymus in segmentation when no clear border is visible |
| Unsharp borders between lymphoma/liquefactive necrosis and fluid in pericardium and pleural cavities | Try to exclude any pericardial and pleural effusion and include liquefactive necrosis in the segmentation (difficult in some cases) |
| Abdominal lymph nodes | Do not include in the segmentation |
| Parameter | Value |
|---|---|
| Batch size | 2D: 12 |
| 3D: 2 | |
| Float precision 16-bit | Yes |
| Max number of epochs * | 1000 |
| Number of batches per epoch * | 250 |
| Number of input channels | 1 |
| Initial learning rate * | 0.01 |
| Momentum * | 0.99 |
| Optimizer * | SGD |
| Patch size | 2D: 512 × 512 |
| 3D: 96 × 160 × 160 | |
| Weight decay * | 0.00003 |
| Model | Average Dice Coefficient |
|---|---|
| 2D U-Net | 0.7065 |
| 3D U-Net | 0.7262 |
| 3D U-Net Cascade | 0.7024 |
| 2D U-Net + 3D U-Net | 0.7221 |
| 2D U-Net + 3D U-Net Cascade | 0.7203 |
| 3D U-Net + 3D U-Net Cascade | 0.7148 |
| Patient | Dice | Manual Segmentation [cm3] | Automatic Segmentation [cm3] | Volume Difference [cm3] |
|---|---|---|---|---|
| Patient 1 | 0.88 | 288.79 | 257.68 | 31.11 |
| Patient 2 | 0.73 | 631.34 | 865.01 | −233.67 |
| Patient 3 | 0.92 | 776.99 | 686.14 | 90.85 |
| Patient 4 | 0.55 | 146.19 | 331.21 | −185.02 |
| Patient 5 | 0.95 | 354.63 | 352.09 | 2.54 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klimont, M.; Oronowicz-Jaśkowiak, A.; Flieger, M.; Rzeszutek, J.; Juszkat, R.; Jończyk-Potoczna, K. Deep Learning-Based Segmentation and Volume Calculation of Pediatric Lymphoma on Contrast-Enhanced Computed Tomographies. J. Pers. Med. 2023, 13, 184. https://doi.org/10.3390/jpm13020184
Klimont M, Oronowicz-Jaśkowiak A, Flieger M, Rzeszutek J, Juszkat R, Jończyk-Potoczna K. Deep Learning-Based Segmentation and Volume Calculation of Pediatric Lymphoma on Contrast-Enhanced Computed Tomographies. Journal of Personalized Medicine. 2023; 13(2):184. https://doi.org/10.3390/jpm13020184
Chicago/Turabian StyleKlimont, Michał, Agnieszka Oronowicz-Jaśkowiak, Mateusz Flieger, Jacek Rzeszutek, Robert Juszkat, and Katarzyna Jończyk-Potoczna. 2023. "Deep Learning-Based Segmentation and Volume Calculation of Pediatric Lymphoma on Contrast-Enhanced Computed Tomographies" Journal of Personalized Medicine 13, no. 2: 184. https://doi.org/10.3390/jpm13020184