
A Meta-Analysis on the Effectiveness of Sertaconazole 2% Cream Compared with Other Topical Therapies for Seborrheic Dermatitis


Abstract
:1. Introduction
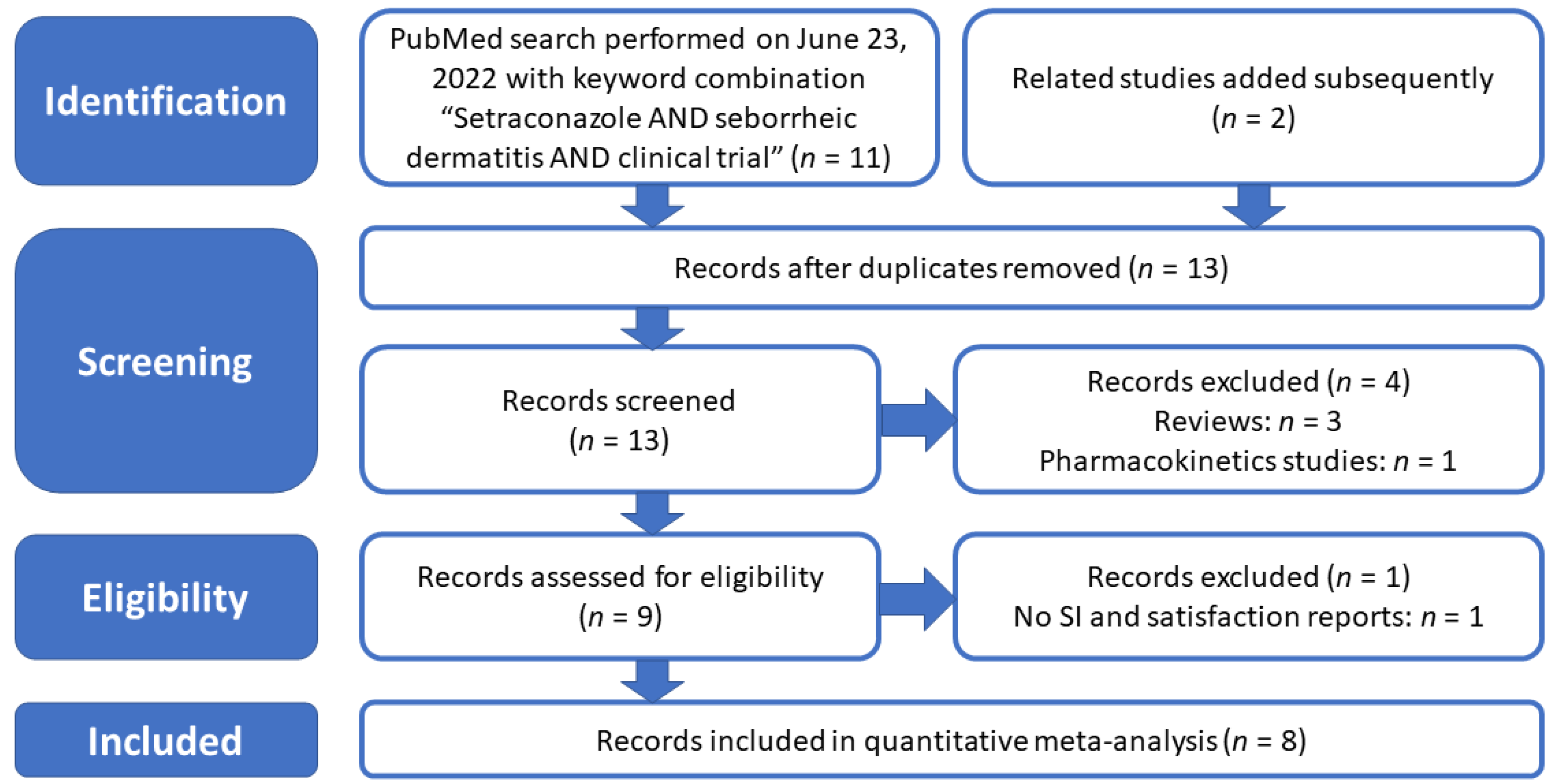
2. Materials and Methods
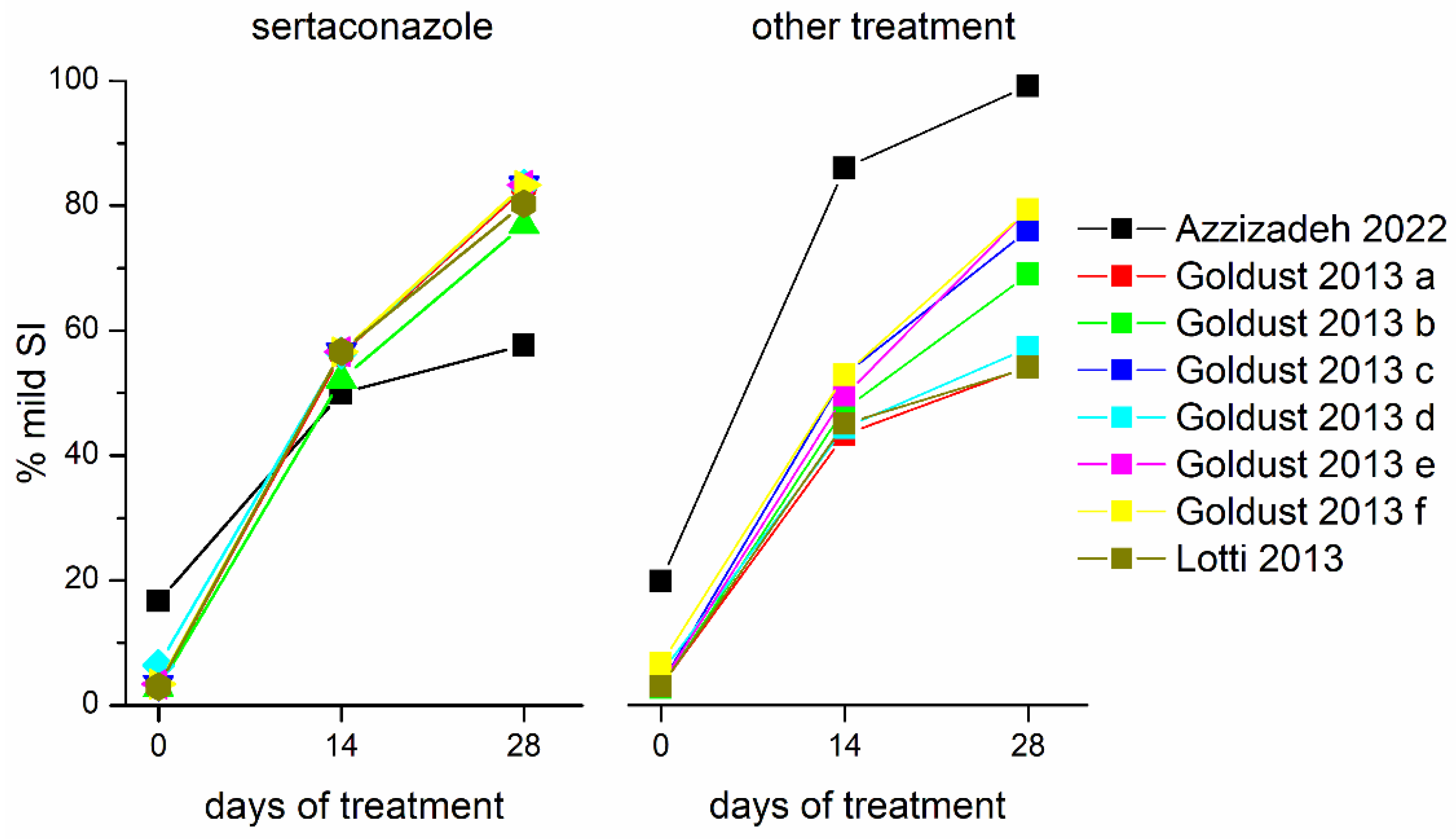
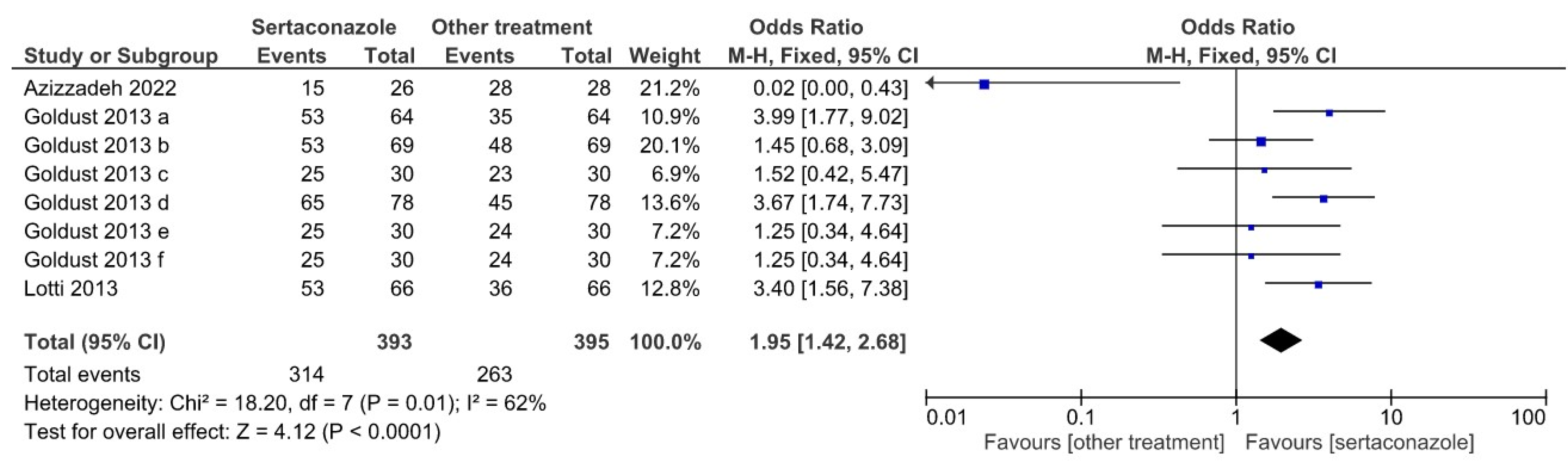
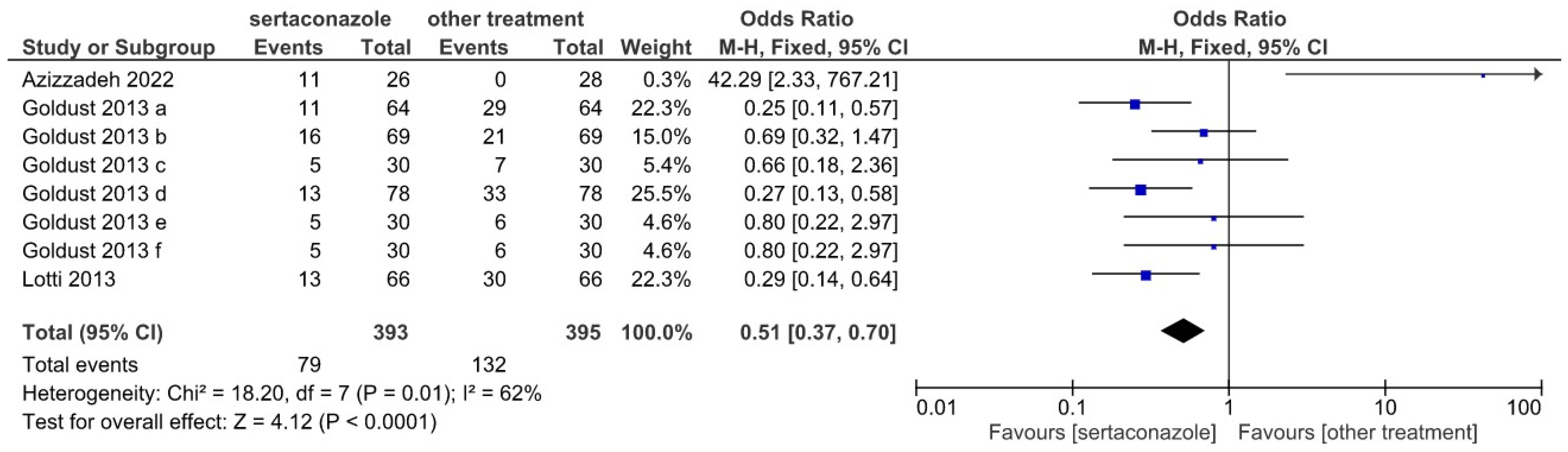
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karakadze, M.A.; Hirt, P.A.; Wikramanayake, T.C. The Genetic Basis of Seborrhoeic Dermatitis: A Review. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Tao, R.; Li, R.; Wang, R. Skin Microbiome Alterations in Seborrheic Dermatitis and Dandruff: A Systematic Review. Exp. Dermatol. 2021, 30, 1546–1553. [Google Scholar] [CrossRef] [PubMed]
- Wikramanayake, T.C.; Borda, L.J.; Miteva, M.; Paus, R. Seborrheic Dermatitis—Looking beyond Malassezia. Exp. Dermatol. 2019, 28, 991–1001. [Google Scholar] [CrossRef] [PubMed]
- Dessinioti, C.; Katsambas, A. Seborrheic Dermatitis: Etiology, Risk Factors, and Treatments: Facts and controversies. Clin. Dermatol. 2013, 31, 343–351. [Google Scholar] [CrossRef]
- Mitran, M.I.; Nicolae, I.; Tampa, M.; Mitran, C.I.; Caruntu, C.; Sarbu, M.I.; Ene, C.D.; Matei, C.; Georgescu, S.R.; Popa, M.I. Reactive Carbonyl Species as Potential Pro-Oxidant Factors Involved in Lichen Planus Pathogenesis. Metabolites 2019, 9, 213. [Google Scholar] [CrossRef]
- Nakai, K.; Tsuruta, D. What Are Reactive Oxygen Species, Free Radicals, and Oxidative Stress in Skin Diseases? Int. J. Mol. Sci. 2021, 22, 10799. [Google Scholar] [CrossRef]
- Trüeb, R.M. Oxidative Stress and Its Impact on Skin, Scalp and Hair. Int. J. Cosmet. Sci. 2021, 43 (Suppl. 1), S9–S13. [Google Scholar] [CrossRef]
- Emre, S.; Kalkan, G.; Erdoğan, S.; Aktaş, A.; Ergin, M. Dynamic Thiol/Disulfide Balance in Patients with Seborrheic Dermatitis: A Case-Control Study. Saudi J. Med. Med. Sci. 2020, 8, 12–16. [Google Scholar] [CrossRef]
- Tampa, M.; Nicolae, I.; Ene, C.D.; Sarbu, I.; Matei, C.; Georgescu, S.R. Vitamin C and Thiobarbituric Acid Reactive Substances (TBARS) in Psoriasis Vulgaris Related to Psoriasis Area Severity Index (PASI). Rev. Chim. 2017, 68, 43–47. [Google Scholar] [CrossRef]
- Saunte, D.M.L.; Gaitanis, G.; Hay, R.J. Malassezia-Associated Skin Diseases, the Use of Diagnostics and Treatment. Front. Cell. Infect. Microbiol. 2020, 10, 112. [Google Scholar] [CrossRef]
- Malassez, L. Note Sur Le Champignon Du Pityriasis Simple. Arch. Physiol. 1874, 1, 451–459. [Google Scholar]
- Wang, K.; Cheng, L.; Li, W.; Jiang, H.; Zhang, X.; Liu, S.; Huang, Y.; Qiang, M.; Dong, T.; Li, Y.; et al. Susceptibilities of Malassezia Strains from Pityriasis Versicolor, Malassezia Folliculitis and Seborrheic Dermatitis to Antifungal Drugs. Heliyon 2020, 6, e04203. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Ran, Y.; Xie, Z.; Zhang, R. Identification of Malassezia Species in Patients with Seborrheic Dermatitis in China. Mycopathologia 2013, 175, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Granger, C.; Balato, A.; Goñi-de-Cerio, F.; Garre, A.; Narda, M. Novel Non-Steroidal Facial Cream Demonstrates Antifungal and Anti-Inflammatory Properties in Ex Vivo Model for Seborrheic Dermatitis. Dermatol. Ther. 2019, 9, 571–578. [Google Scholar] [CrossRef]
- Piquero-Casals, J.; Hexsel, D.; Mir-Bonafé, J.F.; Rozas-Muñoz, E. Topical Non-Pharmacological Treatment for Facial Seborrheic Dermatitis. Dermatol. Ther. 2019, 9, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Adalsteinsson, J.A.; Kaushik, S.; Muzumdar, S.; Guttman-Yassky, E.; Ungar, J. An Update on the Microbiology, Immunology and Genetics of Seborrheic Dermatitis. Exp. Dermatol. 2020, 29, 481–489. [Google Scholar] [CrossRef]
- Yu, Y.; Dunaway, S.; Champer, J.; Kim, J.; Alikhan, A. Changing Our Microbiome: Probiotics in Dermatology. Br. J. Dermatol. 2019, 182, 39–46. [Google Scholar] [CrossRef]
- Tanaka, A.; Cho, O.; Saito, C.; Saito, M.; Tsuboi, R.; Sugita, T. Comprehensive Pyrosequencing Analysis of the Bacterial Microbiota of the Skin of Patients with Seborrheic Dermatitis. Microbiol. Immunol. 2016, 60, 521–526. [Google Scholar] [CrossRef]
- Soares, R.C.; Camargo-Penna, P.H.; de Moraes, V.; De Vecchi, R.; Clavaud, C.; Breton, L.; Braz, A.S.; Paulino, L.C. Dysbiotic Bacterial and Fungal Communities Not Restricted to Clinically Affected Skin Sites in Dandruff. Front. Cell. Infect. Microbiol. 2016, 157. [Google Scholar] [CrossRef]
- Paulino, L.C. New Perspectives on Dandruff and Seborrheic Dermatitis: Lessons We Learned from Bacterial and Fungal Skin Microbiota. Eur. J. Dermatol. 2017, 27 (Suppl. 1), 4–7. [Google Scholar] [CrossRef]
- Carrillo-Muñoz, A.J.; Tur-Tur, C.; Giusiano, G.; Marcos-Arias, C.; Eraso, E.; Jauregizar, N.; Quindós, G. Sertaconazole: An Antifungal Agent for the Topical Treatment of Superficial Candidiasis. Expert Rev. Anti-Infect. Ther. 2013, 11, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Koca, R.; Altinyazar, H.C.; Eştürk, E. Is Topical Metronidazole Effective in Seborrheic Dermatitis? A Double-blind Study. Int. J. Dermatol. 2003, 42, 632–635. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Syst. Rev. 2021, 10, 1–11. [Google Scholar] [CrossRef]
- Cohrane Collaboration. Review Manager (RevMan), version 5.2.3; Computer Program; The Nordic Cochrane Centre: Copenhagen, Denmark, 2012. [Google Scholar]
- Azizzadeh, M.; Pahlevan, D.; Bagheri, B. The Efficacy and Safety of Pimecrolimus 1% Cream vs. Sertaconazole 2% Cream in the Treatment of Patients with Facial Seborrhoeic Dermatitis: A Randomized Blinded Trial. Clin. Exp. Dermatol. 2022, 47, 926–931. [Google Scholar] [CrossRef] [PubMed]
- Goldust, M.; Rezaee, E.; Rouhani, S. Double Blind Study of Sertaconazole 2% Cream vs. Clotrimazole 1% Cream in Treatment of Seborrheic Dermatitis. Ann. Parasitol. 2013, 59, 25–29. [Google Scholar]
- Goldust, M.; Rezaee, E.; Masoudnia, S.; Raghifar, R. Clinical Study of Sertaconazole 2% Cream vs. Hydrocortisone 1% Cream in the Treatment of Seborrheic Dermatitis. Ann. Parasitol. 2013, 59, 119–123. [Google Scholar]
- Goldust, M.; Ranjkesh, M.R.; Amirinia, M.; Golforoushan, F.; Rezaee, E.; Rezazadeh Saatlou, M.A. Sertaconazole 2% Cream versus Hydrocortisone 1% Cream in the Treatment of Seborrheic Dermatitis. J. Dermatolog. Treat. 2013, 1–3. [Google Scholar] [CrossRef]
- Goldust, M.; Rezaee, E.; Raghifar, R. A Double Blind Study of the Effectiveness of Sertaconazole 2% Cream vs. Metronidazole 1% Gel in the Treatment of Seborrheic Dermatitis. Ann. Parasitol. 2013, 59, 173–177. [Google Scholar]
- Goldust, M.; Rezaee, E.; Raghifar, R. Treatment of Seborrheic Dermatitis: Comparison of Sertaconazole 2% Cream versus Pimecrolimus 1% Cream. Ir. J. Med. Sci. 2013, 182, 703–706. [Google Scholar] [CrossRef]
- Goldust, M.; Rezaee, E.; Raghifar, R.; Hemayat, S. Treatment of Seborrheic Dermatitis: The Efficiency of Sertaconazole 2% Cream vs. Tacrolimus 0.03% Cream. Ann. Parasitol. 2013, 59, 73–77. [Google Scholar] [PubMed]
- Lotti, T.; Goldust, M.; Rezaee, E. Treatment of Seborrheic Dermatitis, Comparison of Sertaconazole 2% Cream versus Ketoconazole 2% Cream. J. Dermatol. Treat. 2013, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Georgescu, S.R.; Mitran, C.I.; Mitran, M.I.; Matei, C.; Popa, G.L.; Erel, O.; Tampa, M. Thiol-Disulfide Homeostasis in Skin Diseases. J. Clin. Med. 2022, 11, 1507. [Google Scholar] [CrossRef] [PubMed]
- Borda, L.J.; Perper, M.; Keri, J.E. Treatment of Seborrheic Dermatitis: A Comprehensive Review. J. Dermatol. Treat. 2019, 30, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, G. Optimizing Treatment Approaches in Seborrheic Dermatitis. J. Clin. Aesthet. Dermatol. 2013, 6, 44–49. [Google Scholar]
- Papp, K.A.; Papp, A.; Dahmer, B.; Clark, C.S. Single-Blind, Randomized Controlled Trial Evaluating the Treatment of Facial Seborrheic Dermatitis with Hydrocortisone 1% Ointment Compared with Tacrolimus 0.1% Ointment in Adults. J. Am. Acad. Dermatol. 2012, 67, e11–e15. [Google Scholar] [CrossRef]
- Kastarinen, H.; Oksanen, T.; Okokon, E.O.; Kiviniemi, V.V.; Airola, K.; Jyrkkä, J.; Oravilahti, T.; Rannanheimo, P.K.; Verbeek, J.H. Topical Anti-Inflammatory Agents for Seborrhoeic Dermatitis of the Face or Scalp. Cochrane Database Syst. Rev. 2014, 5, CD009446. [Google Scholar] [CrossRef]
- Joly, P.; Tejedor, I.; Tetart, F.; Cailleux, H.C.; Barrel, A.; De Preville, P.A.; Mion-Mouton, N.; Gabison, G.; Baricault, S. Tacrolimus 0.1% versus Ciclopiroxolamine 1% for Maintenance Therapy in Patients with Severe Facial Seborrheic Dermatitis: A Multicenter, Double-Blind, Randomized Controlled Study. J. Am. Acad. Dermatol. 2021, 84, 1278–1284. [Google Scholar] [CrossRef]
- Okokon, E.O.; Verbeek, J.H.; Ruotsalainen, J.H. Topical Antifungals for Seborrhoeic Dermatitis. Cochrane Database Syst. Rev. 2015, 5, CD008138. [Google Scholar] [CrossRef]
- Gupta, A.K.; Richardson, M.; Paquet, M. Systematic Review of Oral Treatments for Seborrheic Dermatitis. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 16–26. [Google Scholar] [CrossRef]
- Chatterjee, D.; Ghosh, S.K.; Sen, S.; Sarkar, S.; Hazra, A.; De, R. Efficacy and Tolerability of Topical Sertaconazole versus Topical Terbinafine in Localized Dermatophytosis: A Randomized, Observer-Blind, Parallel Group Study. Indian J. Pharmacol. 2016, 48, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Torres, J.; Márquez, M.; Camps, F. Sertaconazole in the Treatment of Mycoses: From Dermatology to Gynecology. Int. J. Gynecol. Obstet. 2000, 71, 3–20. [Google Scholar] [CrossRef]
- Palacín, C.; Tarrago, C.; Ortiz, J. Sertaconazole: Pharmacology of a Gynecological Antifungal Agent. Int. J. Gynecol. Obstet. 2000, 71, 37–46. [Google Scholar] [CrossRef]
- Croxtall, J.D.; Plosker, G.L. Sertaconazole: A Review of Its Use in the Management of Superficial Mycoses in Dermatology and Gynaecology. Drugs 2009, 69, 339–359. [Google Scholar] [CrossRef] [PubMed]
- Liebel, F.; Lyte, P.; Garay, M.; Babad, J.; Southall, M.D. Anti-Inflammatory and Anti-Itch Activity of Sertaconazole Nitrate. Arch. Dermatol. Res. 2006, 298, 191–199. [Google Scholar] [CrossRef]
- Kaur, S.; Sur, R.; Liebel, F.T.; Southall, M.D. Induction of Prostaglandin D2 through the P38 MAPK Pathway Is Responsible for the Antipruritic Activity of Sertaconazole Nitrate. J. Investig. Dermatol. 2010, 130, 2448–2456. [Google Scholar] [CrossRef]
- Zhang, W.; Zhou, L.; Qin, S.; Jiang, J.; Huang, Z.; Zhang, Z.; Zhang, X.; Shi, Z.; Lin, J. Sertaconazole Provokes Proapoptotic Autophagy via Stabilizing TRADD in Nonsmall Cell Lung Cancer Cells. MedComm 2021, 2, 821–837. [Google Scholar] [CrossRef]
- Saki, N.; Jowkar, F.; Alyaseen, S. Comparison of Sertaconazole 2% Cream versus Hydrocortisone 1% Ointment in the Treatment of Atopic Dermatitis. J. Dermatol. Treat. 2013, 24, 447–449. [Google Scholar] [CrossRef]
- Elewski, B.E.; Cantrell, W.C. An Open-Label Study of the Safety and Efficacy of Sertaconazole Nitrate in the Treatment of Seborrheic Dermatitis. J. Drugs Dermatol. JDD 2011, 10, 895–899. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Double Blinded | Rando-Mized | Groups | Mean Age | Sex | Kind of Lesion | Treatment |
|---|---|---|---|---|---|---|---|
| Azizzadeh et al., 2022 [26] | Y | Y | pimecrolimus 1% cream vs. sertaconazole 2% cream | 27.5 | M/F | - | twice a day for four weeks |
| Goldust et al., 2013 a [27] | Y | Y | sertaconazole 2% cream vs. clotrimazole 1% cream | 36.62 ±13.18 | M/F | localized: 57% generalized: 43% | twice a day for four weeks |
| Goldust et al., 2013 b [28] | Y | Y | sertaconazole 2% cream vs. hydrocortisone 1% cream | 36.45 ±13.23 | M/F | localized: 59.4% generalized: 40.6% | twice a day for four weeks |
| Goldust et al., 2013 c [29] | Y | Y | sertaconazole 2% cream vs. hydrocortisone 1% cream | 32.23 ±12.09 | M/F | localized: 58.3% generalized: 41.7% | twice a day for four weeks |
| Goldust et al., 2013 d [30] | Y | Y | sertaconazole 2% cream vs. metronidazole 1% gel | 32.34 ±12.56 | M/F | localized: 56.4% generalized: 43.7% | twice a day for four weeks |
| Goldust et al., 2013 e [31] | Y | Y | sertaconazole 2% cream vs. pimecrolimus 1% cream | 30.12 ±12.56 | M/F | localized: 60% generalized: 40% | twice a day for four weeks |
| Goldust et al., 2013 f [32] | Y | Y | sertaconazole 2% cream vs. tacrolimus 0.03% cream | 32.45 ±12.78 | M/F | localized: 58.3% generalized: 41.7% | twice a day for four weeks |
| Lotti et al., 2013 [33] | Y | Y | sertaconazole 2% cream vs. ketoconazole 2% cream | 42 ±14.36 | M/F | localized: 36.5% generalized: 29.5% | twice a day for four weeks |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Georgescu, S.R.; Mitran, C.I.; Mitran, M.I.; Amuzescu, A.; Matei, C.; Tampa, M. A Meta-Analysis on the Effectiveness of Sertaconazole 2% Cream Compared with Other Topical Therapies for Seborrheic Dermatitis. J. Pers. Med. 2022, 12, 1540. https://doi.org/10.3390/jpm12091540
Georgescu SR, Mitran CI, Mitran MI, Amuzescu A, Matei C, Tampa M. A Meta-Analysis on the Effectiveness of Sertaconazole 2% Cream Compared with Other Topical Therapies for Seborrheic Dermatitis. Journal of Personalized Medicine. 2022; 12(9):1540. https://doi.org/10.3390/jpm12091540
Chicago/Turabian StyleGeorgescu, Simona Roxana, Cristina Iulia Mitran, Madalina Irina Mitran, Andreea Amuzescu, Clara Matei, and Mircea Tampa. 2022. "A Meta-Analysis on the Effectiveness of Sertaconazole 2% Cream Compared with Other Topical Therapies for Seborrheic Dermatitis" Journal of Personalized Medicine 12, no. 9: 1540. https://doi.org/10.3390/jpm12091540