

Hyaluronic Acid as an Adjunct to Coronally Advanced Flap Procedures for Gingival Recessions: A Systematic Review and Meta—Analysis of Randomized Clinical Trials

Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.1.1. Reporting Format
- Intervention: CAF + HA;
- Comparisons: control treatment modalities were: (1) CAF alone, (2) CAF + CTG and/or other biomaterials;
- Outcomes: The primary outcome variables were: mean root coverage (MRC) and reduction of the recession depth (RecRed, obtained from the difference between the baseline recession depth and final recession depth). Secondary outcome variables included: complete root coverage (CRC), probing depth (PD), clinical attachment level (CAL), keratinized tissue width (KTW) and patient-reported outcome measures (PROMs, in terms of post-operative morbidity during at least the first post-operative week);
- Study design: the present systematic review was restricted to randomized clinical trials (RCTs).
2.1.2. Eligibility Criteria
- Randomized clinical trials (RCTs);
- Studies comparing CAF + HA with CAF alone, CAF + CTG and/or in combination with other biomaterials (CAF + biomaterial) in patients with Miller class I or class II (RT1) GR defects;
- Information regarding specific properties of the HA used (type, concentration and application method);
- Follow-up period ≥ 6 months;
- Otherwise periodontally and systemically healthy patients.
- In vitro and animal studies;
- Retrospective studies;
- Case series, case reports and reviews;
- Presence of systemic disease or active periodontal disease.
2.2. Search Strategy
2.2.1. Electronic Search
2.2.2. Manual Search
2.3. Study Selection Process
2.4. Data Extraction
- Author/title/year of study, study affiliation data;
- Study design and follow-up period;
- Sequence generation;
- Allocation concealment;
- Blinding of participants and outcomes assessors;
- Population characteristics;
- Pretreatment;
- Intervention site characteristics, number and localization of GR defects treated;
- Surgical technique;
- HA-related information;
- Control treatment characteristics;
- Post-interventional medication;
- Post-surgical instructions;
- Maintenance therapy;
- Primary and secondary outcomes;
- Information on study funding.
2.5. Quality Assessment of Included Studies (Risk of Bias)
2.6. Data Analysis and Heterogeneity Assessment
3. Results
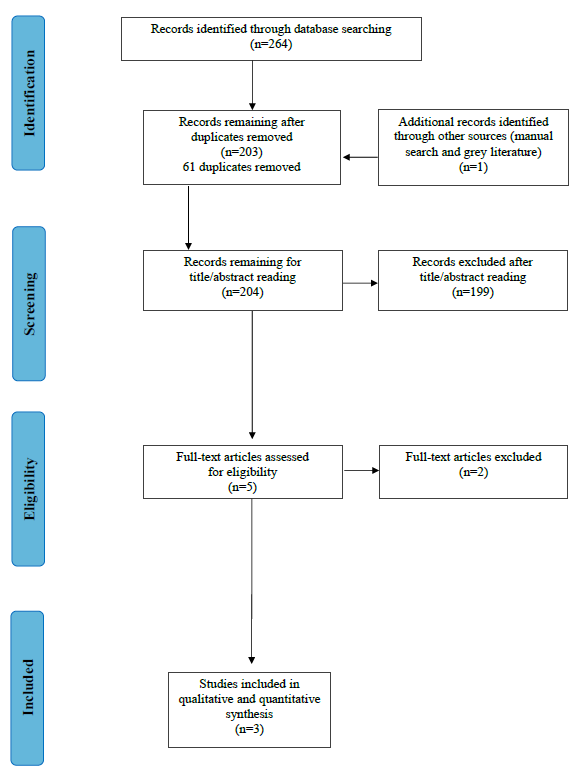
3.1. Search and Screening
3.2. Description of the Included Studies
3.2.1. Study Design
3.2.2. Population Characteristics
3.2.3. Treatment Characteristics (Intervention/Comparison)
- Pre-treatment
- Surgical procedure
- Post-surgical medication and maintenance
3.3. Primary and Secondary Parameters
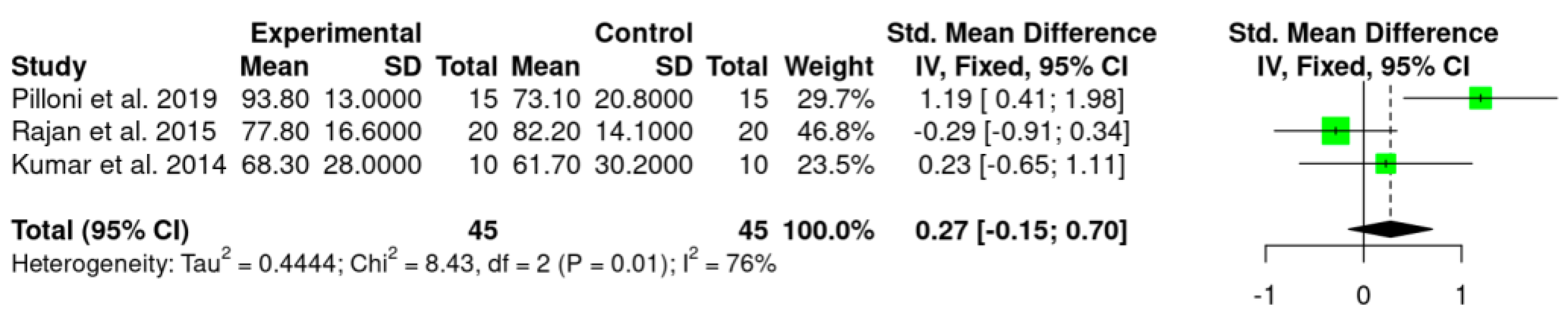
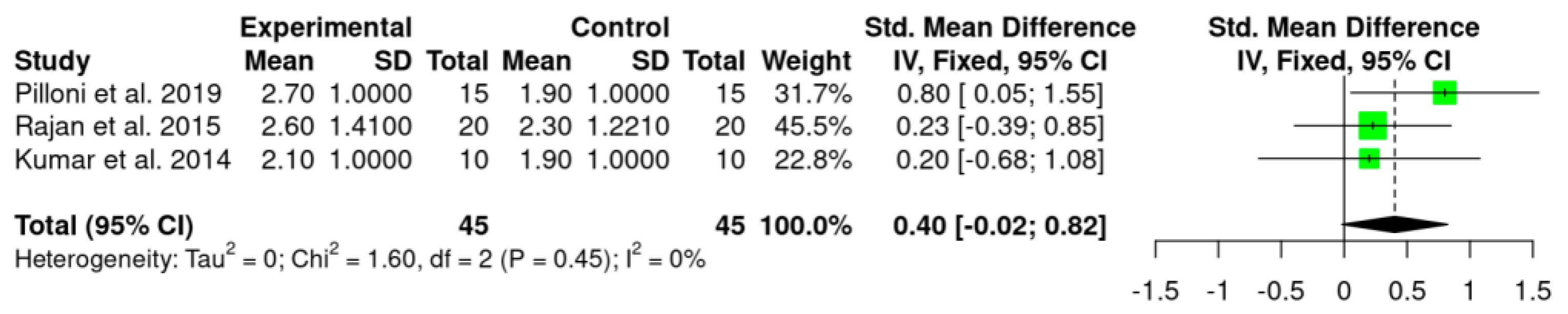
3.3.1. Primary Outcome Variables
- MRC and RecRed
3.3.2. Secondary Outcome Variables
- Complete root coverage (CRC)
- Probing depth (PD)
- Clinical attachment level (CAL)
- Keratinized tissue width (KTW)
- Patient-related outcome measures (PROMs)
3.4. Risk of Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pini Prato, G. Mucogingival deformities. Ann. Periodontol. 1999, 4, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, P.; Bissada, N.F. Mucogingival conditions in the natural dentition: Narrative review, case definitions, and diagnostic considerations. J. Periodontol. 2018, 89 (Suppl. S1), S204–S213. [Google Scholar] [CrossRef] [PubMed]
- Kassab, M.M.; Cohen, R.E. The etiology and prevalence of gingival recession. J. Am. Dent. Assoc. 2003, 134, 220–225. [Google Scholar] [CrossRef]
- Jepsen, K.; Stefanini, M.; Sanz, M.; Zucchelli, G.; Jepsen, S. Long-Term Stability of Root Coverage by Coronally Advanced Flap Procedures. J. Periodontol. 2017, 88, 626–633. [Google Scholar] [CrossRef]
- Joss-Vassalli, I.; Grebenstein, C.; Topouzelis, N.; Sculean, A.; Katsaros, C. Orthodontic therapy and gingival recession: A systematic review. Orthod. Craniofac. Res. 2010, 13, 127–141. [Google Scholar] [CrossRef] [PubMed]
- Merijohn, G.K. Management and prevention of gingival recession. Periodontology 2000 2016, 71, 228–242. [Google Scholar] [CrossRef]
- Khocht, A.; Simon, G.; Person, P.; Denepitiya, J.L. Gingival recession in relation to history of hard toothbrush use. J. Periodontol. 1993, 64, 900–905. [Google Scholar] [CrossRef]
- Serino, G.; Wennström, J.L.; Lindhe, J.; Eneroth, L. The prevalence and distribution of gingival recession in subjects with a high standard of oral hygiene. J. Clin. Periodontol. 1994, 21, 57–63. [Google Scholar] [CrossRef]
- Rajapakse, P.S.; McCracken, G.I.; Gwynnett, E.; Steen, N.D.; Guentsch, A.; Heasman, P.A. Does tooth brushing influence the development and progression of non-inflammatory gingival recession? A systematic review. J. Clin. Periodontol. 2007, 34, 1046–1061. [Google Scholar] [CrossRef]
- Wennström, J.L. Mucogingival therapy. Ann. Periodontol. 1996, 1, 671–701. [Google Scholar] [CrossRef]
- Clauser, C.; Nieri, M.; Franceschi, D.; Pagliaro, U.; Pini-Prato, G. Evidence-based mucogingival therapy. Part 2: Ordinary and individual patient data meta-analyses of surgical treatment of recession using complete root coverage as the outcome variable. J. Periodontol. 2003, 74, 741–756. [Google Scholar] [CrossRef] [PubMed]
- Chambrone, L.; Tatakis, D.N. Periodontal soft tissue root coverage procedures: A systematic review from the AAP Regeneration Workshop. J Periodontol. 2015, 86 (Suppl. S2), S8–S51. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, G.; Mounssif, I. Periodontal plastic surgery. Periodontol 2000 2015, 68, 333–368. [Google Scholar] [CrossRef] [PubMed]
- Grupe, H.; Warren, R. Repair of gingival defects by a sliding flap operation. J. Periodontol. 1956, 27, 92–95. [Google Scholar] [CrossRef]
- Cohen, D.W.; Ross, S.E. The double papillae repositioned flap in periodontal therapy. J. Periodontol. 1968, 39, 65–70. [Google Scholar] [CrossRef]
- Pennel, B.M.; Higgason, J.D.; Towner, J.D.; King, K.O.; Fritz, B.D.; Salder, J.F. Oblique Rotated Flap. J. Periodontol. 1965, 36, 305–309. [Google Scholar] [CrossRef]
- Bernimoulin, J.P.; Lüscher, B.; Mühlemann, H.R. Coronally repositioned periodontal flap. Clinical evaluation after one year. J Clin. Periodontol. 1975, 2, 1–13. [Google Scholar] [CrossRef]
- Tarnow, D.P. Semilunar coronally repositioned flap. J. Clin. Periodontol. 1986, 13, 182–185. [Google Scholar] [CrossRef]
- Allen, A.L. Use of the supraperiosteal envelope in soft tissue grafting for root coverage. I. Rationale and technique. Int. J. Periodontics Restor. Dent. 1994, 14, 216–227. [Google Scholar]
- de Sanctis, M.; Zucchelli, G. Coronally advanced flap: A modified surgical approach for isolated recession-type defects: Three-year results. J. Clin. Periodontol. 2007, 34, 262–268. [Google Scholar] [CrossRef]
- Zucchelli, G.; De Sanctis, M. Treatment of multiple recession-type defects in patients with esthetic demands. J. Periodontol. 2000, 71, 1506–1514. [Google Scholar] [CrossRef] [PubMed]
- Aroca, S.; Molnár, B.; Windisch, P.; Gera, I.; Salvi, G.E.; Nikolidakis, D.; Sculean, A. Treatment of multiple adjacent Miller class I and II gingival recessions with a Modified Coronally Advanced Tunnel (MCAT) technique and a collagen matrix or palatal connective tissue graft: A randomized, controlled clinical trial. J. Clin. Periodontol. 2013, 40, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Sculean, A.; Allen, E.P. The Laterally Closed Tunnel for the Treatment of Deep Isolated Mandibular Recessions: Surgical Technique and a Report of 24 Cases. Int. J. Periodontics Restor. Dent. 2018, 38, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Carranza, N.; Pontarolo, C.; Rojas, M.A. Laterally Stretched Flap With Connective Tissue Graft to Treat Single Narrow Deep Recession Defects on Lower Incisors. Clin. Adv. Periodontics 2019, 9, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Pini Prato, G.; Clauser, C.; Cortellini, P.; Tinti, C.; Vincenzi, G.; Pagliaro, U. Guided tissue regeneration versus mucogingival surgery in the treatment of human buccal recessions. A 4-year follow-up study. J. Periodontol. 1996, 67, 1216–1223. [Google Scholar] [CrossRef]
- Pilloni, A.; Paolantonio, M.; Camargo, P.M. Root coverage with a coronally positioned flap used in combination with enamel matrix derivative: 18-month clinical evaluation. J. Periodontol. 2006, 77, 2031–2039. [Google Scholar] [CrossRef]
- Zucchelli, G.; Tavelli, L.; McGuire, M.K.; Rasperini, G.; Feinberg, S.E.; Wang, H.; Giannobile, W.V. Autogenous soft tissue grafting for periodontal and peri-implant plastic surgical reconstruction. J. Periodontol. 2020, 91, 9–16. [Google Scholar] [CrossRef]
- da Silva, R.C.; Joly, J.C.; de Lima, A.F.; Tatakis, D.N. Root coverage using the coronally positioned flap with or without a subepithelial connective tissue graft. J. Periodontol. 2004, 75, 413–419. [Google Scholar] [CrossRef]
- Novaes, A.B., Jr.; Palioto, D.B. Experimental and clinical studies on plastic periodontal procedures. Periodontology 2000 2019, 79, 56–80. [Google Scholar] [CrossRef]
- Tavelli, L.; Asa’ad, F.; Acunzo, R.; Pagni, G.; Consonni, D.; Rasperini, G. Minimizing Patient Morbidity Following Palatal Gingival Harvesting: A Randomized Controlled Clinical Study. Int. J. Periodontics Restor. Dent. 2018, 38, e127–e134. [Google Scholar] [CrossRef]
- Jhaveri, H.M.; Chavan, M.S.; Tomar, G.B.; Deshmukh, V.L.; Wani, M.R.; Miller, P.D., Jr. Acellular dermal matrix seeded with autologous gingival fibroblasts for the treatment of gingival recession: A proof-of-concept study. J. Periodontol. 2010, 81, 616–625. [Google Scholar] [CrossRef]
- Cheng, G.-L.; Fu, E.; Tu, Y.-K.; Shen, E.-C.; Chiu, H.-C.; Huang, R.-Y.; Yuh, D.-Y.; Chiang, C.-Y. Root coverage by coronally advanced flap with connective tissue graft and/or enamel matrix derivative: A meta-analysis. J. Periodontal Res. 2015, 50, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Dahiya, P.; Kamal, R. Hyaluronic Acid: A boon in periodontal therapy. N. Am. J. Med. Sci. 2013, 5, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.Y.; Abatangelo, G. Functions of hyaluronan in wound repair. Wound Repair Regen. 1999, 7, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Aya, K.L.; Stern, R. Hyaluronan in wound healing: Rediscovering a major player. Wound Repair Regen. 2014, 22, 579–593. [Google Scholar] [CrossRef]
- Asparuhova, M.B.; Kiryak, D.; Eliezer, M.; Mihov, D.; Sculean, A. Activity of two hyaluronan preparations on primary human oral fibroblasts. J. Periodontal Res. 2019, 54, 33–45. [Google Scholar] [CrossRef]
- Jentsch, H.; Pomowski, R.; Kundt, G.; Göcke, R. Treatment of gingivitis with hyaluronan. J. Clin. Periodontol. 2003, 30, 159–164. [Google Scholar] [CrossRef]
- Eick, S.; Renatus, A.; Heinicke, M.; Pfister, W.; Stratul, S.I.; Jentsch, H. Hyaluronic Acid as an adjunct after scaling and root planing: A prospective randomized clinical trial. J. Periodontol. 2013, 84, 941–949. [Google Scholar] [CrossRef]
- Pilloni, A.; Zeza, B.; Kuis, D.; Vrazic, D.; Domic, T.; Olszewska-Czyz, I.; Popova, C.; Kotsilkov, K.; Firkova, E.; Dermendzieva, Y.; et al. Treatment of Residual Periodontal Pockets Using a Hyaluronic Acid-Based Gel: A 12 Month Multicenter Randomized Triple-Blinded Clinical Trial. Antibiotics 2021, 10, 924. [Google Scholar] [CrossRef]
- Pilloni, A.; Schmidlin, P.R.; Sahrmann, P.; Sculean, A.; Rojas, M.A. Effectiveness of adjunctive hyaluronic acid application in coronally advanced flap in Miller class I single gingival recession sites: A randomized controlled clinical trial. Clin. Oral Investig. 2019, 23, 1133–1141, Erratum in Clin. Oral Investig. 2018, 22, 2961–2962. [Google Scholar] [CrossRef]
- Pilloni, A.; Nardo, F.; Rojas, M.A. Surgical Treatment of a Cemental Tear-Associated Bony Defect Using Hyaluronic Acid and a Resorbable Collagen Membrane: A 2-Year Follow-Up. Clin. Adv. Periodontics 2019, 9, 64–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilloni, A.; Rojas, M.A.; Marini, L.; Russo, P.; Shirakata, Y.; Sculean, A.; Iacono, R. Healing of intrabony defects following regenerative surgery by means of single-flap approach in conjunction with either hyaluronic acid or an enamel matrix derivative: A 24-month randomized controlled clinical trial. Clin. Oral Investig. 2021, 25, 5095–5107. [Google Scholar] [CrossRef] [PubMed]
- Romeo, U.; Libotte, F.; Palaia, G.; Galanakis, A.; Gaimari, G.; Tenore, G.; Del Vecchio, A.; Polimeni, A. Oral soft tissue wound healing after laser surgery with or without a pool of amino acids and sodium hyaluronate: A randomized clinical study. Photomed. Laser Surg. 2014, 32, 10–16. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Miller, P.D., Jr. A classification of marginal tissue recession. Int. J. Periodontics Restor. Dent. 1985, 5, 8–13. [Google Scholar]
- Cairo, F.; Nieri, M.; Cincinelli, S.; Mervelt, J.; Pagliaro, U. The interproximal clinical attachment level to classify gingival recessions and predict root coverage outcomes: An explorative and reliability study. J. Clin. Periodontol. 2011, 38, 661–666. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef]
- Khurshid, Z.; Tariq, R.; Asiri, F.Y.; Abid, K.; Zafar, M.S. Literature search strategies in dental education and research. J. Taibah Univ. Med. Sci. 2021, 16, 799–806. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Peacock, R. Effectiveness and efficiency of search methods in systematic reviews of complex evidence: Audit of primary sources. BMJ 2005, 331, 1064–1065. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0. 2011. Available online: https://handbook-5-1.cochrane.org (accessed on 30 April 2022).
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Brignardello-Petersen, R. Hyaluronic acid used as an adjunct to coronally advanced flap probably results in an increase in recession reduction and root coverage in patients with single Miller class I gingival recessions. J. Am. Dent. Assoc. 2019, 150, e12. [Google Scholar] [CrossRef] [PubMed]
- Zukorlic, H.; Jakoba, N.N. Effects of topical application of hyaluronic acid gel on wound healing following gingival recession treatment. Eur. J. Med. Res. 2011, 16, 113. [Google Scholar]
- Rajan, P.; Rao, N.M.; Nera, M.; Rahaman, S.M. Hyaluronon as an adjunct to coronally advanced flap for the treatment of gingival recession defects. Natl. J. Integr. Res. Med. 2015, 6, 94–100. [Google Scholar]
- Kumar, R.; Srinivas, M.; Pai, J.; Suragimath, G.; Prasad, K.; Polepalle, T. Efficacy of hyaluronic acid (hyaluronan) in root coverage procedures as an adjunct to coronally advanced flap in Millers Class I recession: A clinical study. J. Indian Soc. Periodontol. 2014, 18, 746–750. [Google Scholar] [CrossRef]
- Zucchelli, G.; Stefanini, M.; Ganz, S.; Mazzotti, C.; Mounssif, I.; Marzadori, M. Coronally Advanced Flap with Different Designs in the Treatment of Gingival Recession: A Comparative Controlled Randomized Clinical Trial. Int. J. Periodontics Restor. Dent. 2016, 36, 319–327. [Google Scholar] [CrossRef]
- Dubey, P.; Narasimhan, M.; Sehgal, N.K.; Yanni, P.; Kim, J.W.; Kapila, Y.L.; Lin, G.-H. Connective Tissue Graft with or without Enamel Matrix Derivative for Treating Gingival Recession Defects: A Systematic Review and Meta-Analysis. J. Evid. Based Dent. Pract. 2021, 21, 101635. [Google Scholar] [CrossRef]
- Li, F.; Yu, F.; Xu, X.; Li, C.; Huang, D.; Zhou, X.; Ye, L.; Zheng, L. Evaluation of Recombinant Human FGF-2 and PDGF-BB in Periodontal Regeneration: A Systematic Review and Meta-Analysis. Sci. Rep. 2017, 7, 65. [Google Scholar] [CrossRef]
- Miron, R.J.; Moraschini, V.; Del Fabbro, M.; Piattelli, A.; Fujioka-Kobayashi, M.; Zhang, Y.; Saulacic, N.; Schaller, B.; Kawase, T.; Cosgarea, R.; et al. Use of platelet-rich fibrin for the treatment of gingival recessions: A systematic review and meta-analysis. Clin. Oral Investig. 2020, 24, 2543–2557. [Google Scholar] [CrossRef]
- Chambrone, L.; Botelho, J.; Machado, V.; Mascarenhas, P.; Mendes, J.J.; Avila-Ortiz, G. Does the subepithelial connective tissue graft in conjunction with a coronally advanced flap remain as the gold standard therapy for the treatment of single gingival recession defects? A systematic review and network meta-analysis. J. Periodontol. 2022. ahead of print. [Google Scholar] [CrossRef]
- Moraschini, V.; de Almeida, D.C.F.; Sartoretto, S.; Bailly Guimarães, H.; Chaves Cavalcante, I.; Diuana Calasans-Maia, M. Clinical efficacy of xenogeneic collagen matrix in the treatment of gingival recession: A systematic review and meta-analysis. Acta Odontol. Scand. 2019, 77, 457–467. [Google Scholar] [CrossRef]
- Shirakata, Y.; Imafuji, T.; Nakamura, T.; Nakamura, T.; Kawakami, Y.; Shinohara, Y.; Noguchi, K.; Pilloni, A.; Sculean, A. Periodontal wound healing/regeneration of two-wall intrabony defects following reconstructive surgery with cross-linked hyaluronic acid-gel with or without a collagen matrix: A preclinical study in dogs. Quintessence Int. 2021, 52, 308–316. [Google Scholar] [CrossRef]
- Sasaki, T.; Watanabe, C. Stimulation of osteoinduction in bone wound healing by high-molecular hyaluronic acid. Bone 1995, 16, 9–15. [Google Scholar] [CrossRef]
- Deed, R.; Rooney, P.; Kumar, P.; Norton, J.D.; Smith, J.; Freemont, A.J.; Kumar, S. Early-response gene signalling is induced by angiogenic oligosaccharides of hyaluronan in endothelial cells. Inhibition by non-angiogenic, high-molecular-weight hyaluronan. Int. J. Cancer 1997, 71, 251–256. [Google Scholar] [CrossRef]
- Bertolami, C.N.; Messadi, D.V. The role of proteoglycans in hard and soft tissue repair. Crit. Rev. Oral Biol. Med. 1994, 5, 311–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pini Prato, G.P.; Franceschi, D.; Cortellini, P.; Chambrone, L. Long-term evaluation (20 years) of the outcomes of subepithelial connective tissue graft plus coronally advanced flap in the treatment of maxillary single recession-type defects. J. Periodontol. 2018, 89, 1290–1299. [Google Scholar] [CrossRef] [PubMed]
- Gurtner, G.C.; Werner, S.; Barrandon, Y.; Longaker, M.T. Wound repair and regeneration. Nature 2008, 453, 314–321. [Google Scholar] [CrossRef]
- McGuire, M.K.; Nunn, M. Evaluation of human recession defects treated with coronally advanced flaps and either enamel matrix derivative or connective tissue. Part 1: Comparison of clinical parameters. J. Periodontol. 2003, 74, 1110–1125. [Google Scholar] [CrossRef]
- Snetkov, P.; Zakharova, K.; Morozkina, S.; Olekhnovich, R.; Uspenskaya, M. Hyaluronic Acid: The Influence of Molecular Weight on Structural, Physical, Physico-Chemical, and Degradable Properties of Biopolymer. Polymers 2020, 12, 1800. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author Year | Study Design | Follow-Up | Masking | Intervention (C versus T Group) | Power Calculation | Setting | Funding |
|---|---|---|---|---|---|---|---|
| Pilloni et al. 2019 [41] | RCT Double-arm | 18 mo | Single- blind | CAF versus CAF + HA | Yes | U | No |
| Rajan et al. 2015 [54] | RCT Split-mouth | 9 mo | NA | CAF + SCTG versus CAF + HA | No | U | No |
| Kumar et al. 2014 [55] | RCT Split-mouth | 6 mo | NA | CAF versus CAF + HA | Unclear | U | No |
| Author Year | Patient’s Characteristics | Teeth and Defect Characteristics | |||||
|---|---|---|---|---|---|---|---|
| Group | Number of Patients | Gender (m/f) | Years M [IQR] Range | Drop-Out | Number/ Type of Tooth | Number/ Type of GR Defect | |
| Pilloni et al. 2019 [41] | C T | 15 15 | 8/7 8/7 | 30 [12] 30 [15] | 0 0 | 15 (5 UC, 1 LC, 7 UPM, 2 LPM) 15 (2 UC, 2 LC, 7 UPM, 4 LPM) | 15 Miller Class I (RT1) 15 Miller Class I (RT1) |
| Rajan et al. 2015 [54] | C/T | 20 | 7/13 | 26–42 years | 0 | 40 NA | 40 Miller Class I/II(RT1) |
| Kumar et al. 2014 [55] | C/T | 10 | 7/3 | NA | 0 | 20 NA | 20 Miller Class I (RT1) |
| Author Year | Primary Outcome Variables | ||||||
|---|---|---|---|---|---|---|---|
| MRC (%) | RD (M [IQR]/Mean ± SD) | RecRed (M [IQR]/Mean ± SD) | |||||
| Time points | C | T | C | T | C | T | |
| Pilloni et al. 2019 [41] | Baseline | - | - | 3.0 [1.0] | 3.0 [1.0] | - | - |
| 18 mo | 73.1 ± 20.8% | 93.8 ± 13.0% * | 0.0 [0.0] | 1.0 [1.0] * | 1.9 [1.0] | 2.7 [1.0] * | |
| Rajan et al. 2015 [54] | Baseline | - | - | 3.45 ± 0.94 | 3.65 ± 1.09 | - | - |
| 1 mo | - | - | 2.45 ± 1.05 | 2.05 ± 0.69 * | - | - | |
| 3 mo | 48.07 ± 13.35% | 58.43 ± 8.80% * | 1.80 ± 0.77 | 1.50 ± 0.51 | - | - | |
| 9 mo | 82.15 ± 14.05% | 77.84 ± 16.56% | 1.15 ± 0.59 | 1.05 ± 0.76 | 2.3 ± 0.94 | 2.6 ± 1.09 | |
| Kumar et al. 2014 [55] | Baseline | - | - | 2.90 ± 0.73 | 3.20 ± 0.78 | - | - |
| 1 w | - | - | 0.00 ± 0.00 | 0.10 ± 0.31 | - | - | |
| 3 w | - | - | 0.30 ± 0.48 | 0.30 ± 0.67 | - | - | |
| 6 w | - | - | 0.50 ± 0.52 | 0.70 ± 0.82 | - | - | |
| 3 mo | - | - | 0.90 ± 0.73 | 0.90 ± 0.87 | - | - | |
| 6 mo | 61.67 ± 30.22% | 68.33 ± 28% | 1.00 ± 0.66 | 1.10 ± 0.99 | 1.9 ± 0.73 | 2.1 ± 0.99 | |
| Author Year | Domains | |||||
|---|---|---|---|---|---|---|
| Adequate Sequence Generation? | Allocation Concealment? | Blinding? | Incomplete Outcome Data Addressed? | Free of Selective Reporting? | Free of Other Bias? | |
| Pilloni et al. 2019 [41] | Yes | Yes | Yes | Yes | Yes | No |
| Rajan et al. 2015 [54] | Unclear | Unclear | Unclear | Yes | Unclear | Unclear |
| Kumar et al. 2014 [55] | Yes | Unclear | Unclear | Unclear | Yes | Unclear |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rojas, M.A.; Marini, L.; Sahrmann, P.; Pilloni, A. Hyaluronic Acid as an Adjunct to Coronally Advanced Flap Procedures for Gingival Recessions: A Systematic Review and Meta—Analysis of Randomized Clinical Trials. J. Pers. Med. 2022, 12, 1539. https://doi.org/10.3390/jpm12091539
Rojas MA, Marini L, Sahrmann P, Pilloni A. Hyaluronic Acid as an Adjunct to Coronally Advanced Flap Procedures for Gingival Recessions: A Systematic Review and Meta—Analysis of Randomized Clinical Trials. Journal of Personalized Medicine. 2022; 12(9):1539. https://doi.org/10.3390/jpm12091539
Chicago/Turabian StyleRojas, Mariana A., Lorenzo Marini, Philipp Sahrmann, and Andrea Pilloni. 2022. "Hyaluronic Acid as an Adjunct to Coronally Advanced Flap Procedures for Gingival Recessions: A Systematic Review and Meta—Analysis of Randomized Clinical Trials" Journal of Personalized Medicine 12, no. 9: 1539. https://doi.org/10.3390/jpm12091539