



The Presence of Psoriasis, Metabolic Syndrome and Their Combination Increases the Serum Levels of CRP and CD5L but Not sCD200R1 and sTLR2 in Participants
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Groups
2.2. PASI
2.3. Metabolic Syndrome
2.4. Blood Sampling
2.5. Levels of sCR200R1
2.6. Levels of CD5L
2.7. Levels of sTLR2
2.8. Levels of CRP
2.9. Statistical Analysis
3. Results
3.1. Levels of CRP
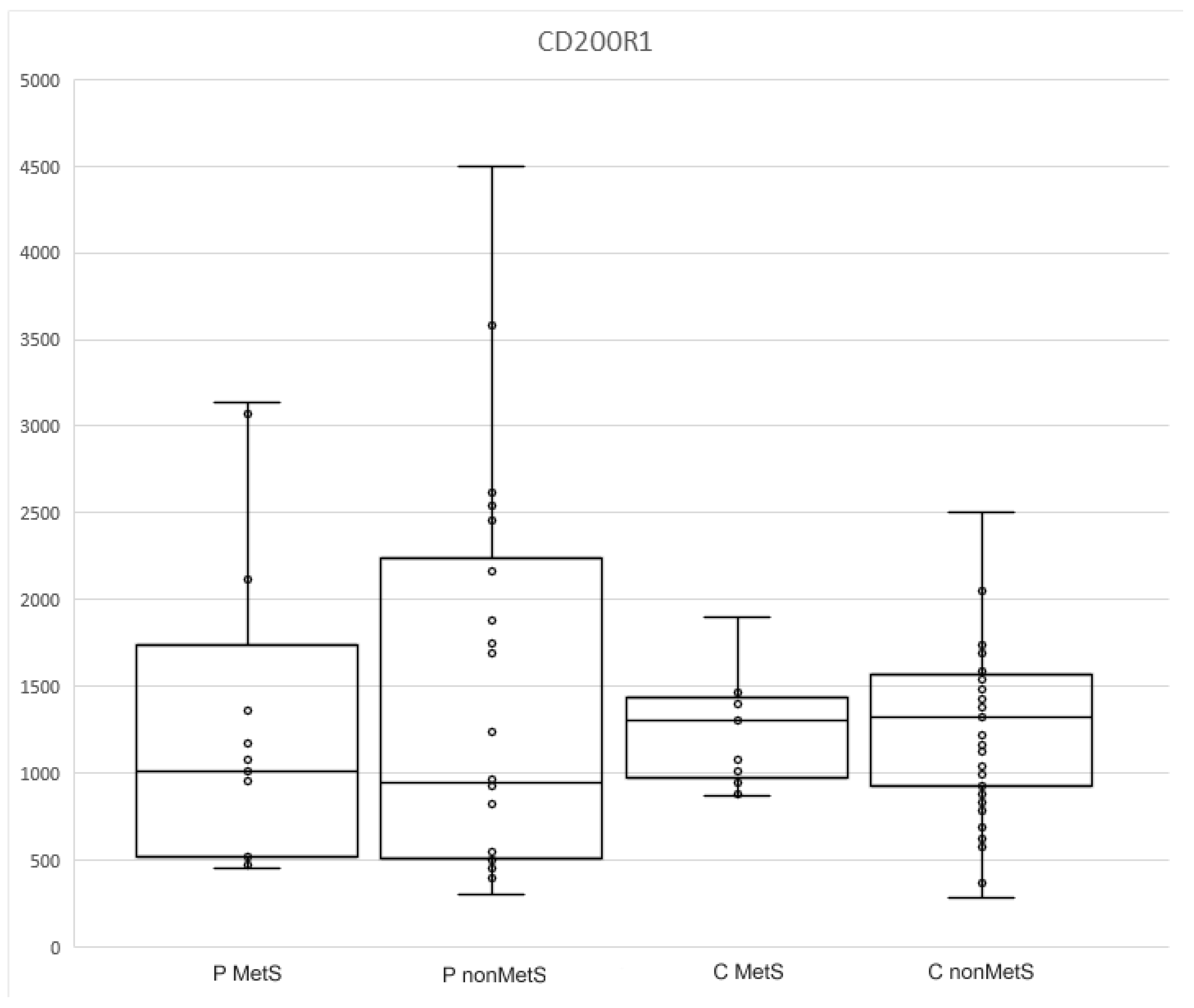
3.2. Levels of sCD200R1
3.3. Levels of CD5L
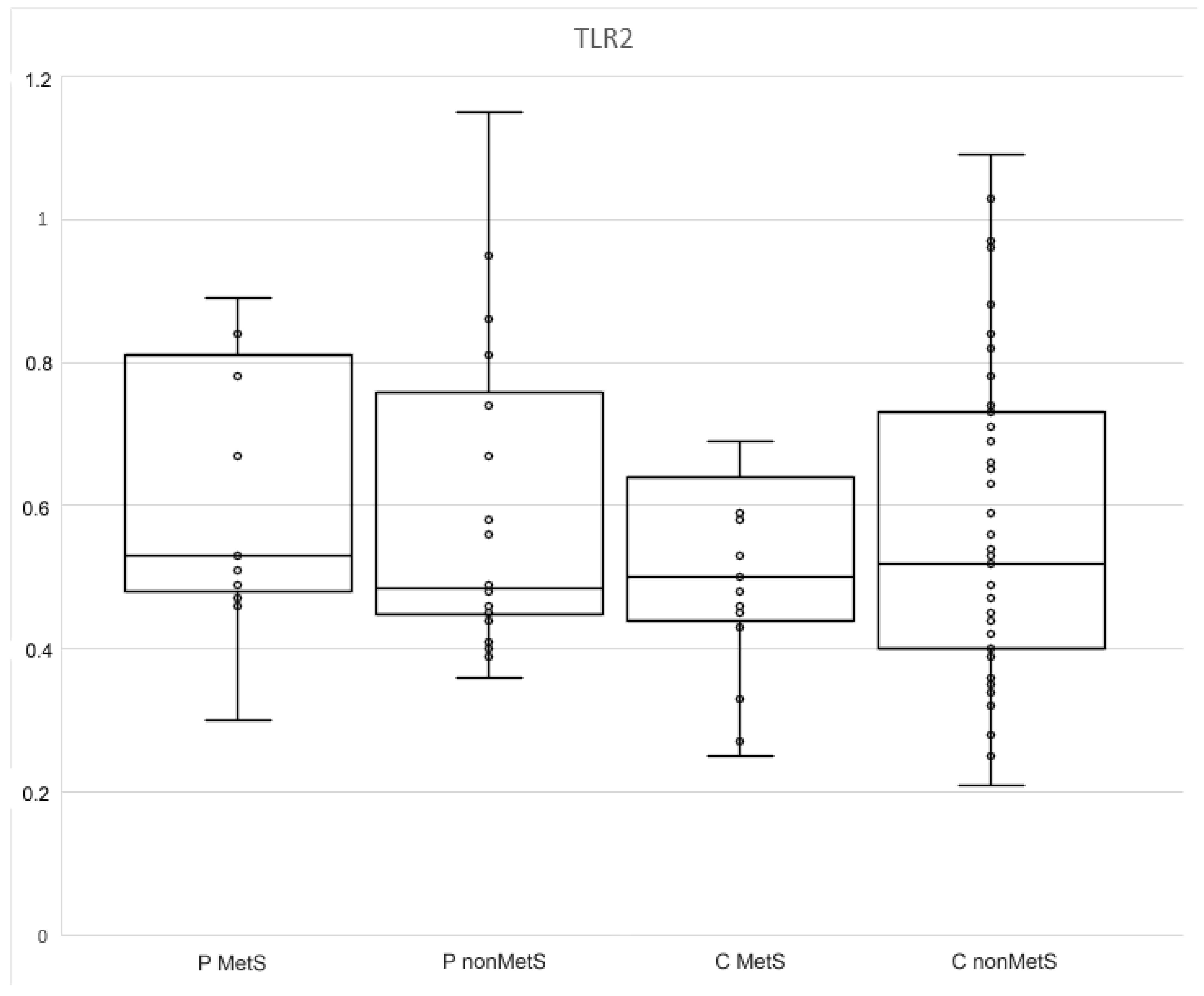
3.4. Levels of sTLR2
3.5. Relationships among Selected Parameters
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vičić, M.; Kaštelan, M.; Brajac, I.; Sotošek, V.; Massari, L.P. Current Concepts of Psoriasis Immunopathogenesis. Int. J. Mol. Sci. 2021, 22, 11574. [Google Scholar] [CrossRef] [PubMed]
- Capon, F. The genetic basis of psoriasis. Int. J. Mol. Sci. 2017, 18, 2526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamiya, K.; Kishimoto, M.; Sugai, J.; Komine, M.; Ohtsuki, M. Risk factors for the development of psoriasis. Int. J. Mol. Sci. 2019, 20, 4347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, B.-X.; Chen, X.-Y.; Ye, L.-R.; Chen, J.-Q.; Zheng, M.; Man, X.-Y. Cutaneous and Systemic Psoriasis: Classifications and Classification for the Distinction. Front Med. 2021, 8, 1820. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, A.K.; Chand Yadav, T.; Khera, H.K.; Mishra, P.; Raghuwanshi, N.; Pruthi, V.; Prasad, R. Insights into interplay of immunopathophysiological events and molecular mechanistic cascades in psoriasis and its associated comorbidities. J. Autoimmun. 2021, 118, 102614. [Google Scholar] [CrossRef]
- Gisondi, P.; Fostini, A.C.; Fossà, I.; Girolomoni, G.; Targher, G. Psoriasis and the metabolic syndrome. Clin. Dermatol. 2018, 36, 21–28. [Google Scholar] [CrossRef]
- Zafar, U.; Khaliq, S.; Ahmad, H.U.; Manzoor, S.; Lone, K.P. Metabolic syndrome: An update on diagnostic criteria, pathogenesis, and genetic links. Hormones 2018, 17, 299–313. [Google Scholar] [CrossRef] [PubMed]
- Fahed, G.; Aoun, L.; Bou Zerdan, M.; Allam, S.; Bou Zerdan, M.; Bouferraa, Y.; Assi, H.I. Metabolic Syndrome: Updates on Pathophysiology and Management in 2021. Int. J. Mol. Sci. 2022, 23, 786. [Google Scholar] [CrossRef]
- Kahn, C.R.; Wang, G.; Lee, K.Y. Altered adipose tissue and adipocyte function in the pathogenesis of metabolic syndrome. J. Clin. Investig. 2019, 129, 3990–4000. [Google Scholar] [CrossRef]
- Grandl, G.; Wolfrum, C. Hemostasis, endothelial stress, inflammation, and the metabolic syndrome. Semin. Immunopathol. 2018, 40, 215–224. [Google Scholar] [CrossRef]
- Holmannova, D.; Borsky, P.; Borska, L.; Andrys, C.; Hamakova, K.; Rehacek, V.; Svadlakova, T.; Malkova, A.; Beranek, M.; Palicka, V.; et al. Metabolic Syndrome, Clusterin and Elafin in Patients with Psoriasis Vulgaris. Int. J. Mol. Sci. 2020, 21, 5617. [Google Scholar] [CrossRef] [PubMed]
- Holmannova, D.; Borska, L.; Andrys, C.; Borsky, P.; Kremlacek, J.; Hamakova, K.; Rehacek, V.; Malkova, A.; Svadlakova, T.; Palicka, V.; et al. The impact of psoriasis and metabolic syndrome on the systemic inflammation and oxidative damage to nucleic acids. J. Immunol. Res. 2020, 2020, 7352637. [Google Scholar] [CrossRef] [PubMed]
- Holmannova, D.; Borsky, P.; Andrys, C.; Hamakova, K.; Cermakova, E.; Poctova, G.; Fiala, Z.; Smejkalova, J.; Blaha, V.; Borska, L. Chromosomal Aberrations and Oxidative Stress in Psoriatic Patients with and without Metabolic Syndrome. Metabolites 2022, 12, 688. [Google Scholar] [CrossRef] [PubMed]
- Holmannová, D.; Kolácková, M.; Kondélková, K.; Kunes, P.; Krejsek, J.; Andrýs, C. CD200/CD200R paired potent inhibitory molecules regulating immune and inflammatory responses; Part I: CD200/CD200R structure, activation, and function. Acta Med. 2012, 55, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Kotwica-Mojzych, K.; Jodłowska-Jędrych, B.; Mojzych, M. Cd200:Cd200r interactions and their importance in immunoregulation. Int. J. Mol. Sci. 2021, 22, 1602. [Google Scholar] [CrossRef]
- Sanchez-Moral, L.; Ràfols, N.; Martori, C.; Paul, T.; Téllez, É.; Sarrias, M.R. Multifaceted roles of cd5l in infectious and sterile inflammation. Int. J. Mol. Sci. 2021, 22, 4076. [Google Scholar] [CrossRef]
- Weng, D.; Gao, S.; Shen, H.; Yao, S.; Huang, Q.; Zhang, Y.; Huang, W.; Wang, Y.; Zhang, X.; Yin, Y.; et al. CD5L attenuates allergic airway inflammation by expanding CD11chigh alveolar macrophages and inhibiting NLRP3 inflammasome activation via HDAC2. Immunology. 2022, 167, 384–397. [Google Scholar] [CrossRef]
- Wang, C.; Yosef, N.; Gaublomme, J.; Wu, C.; Lee, Y.; Clish, C.B.; Kaminski, J.; Xiao, S.; Zu Horste, G.M.; Pawlak, M.; et al. CD5L/AIM Regulates Lipid Biosynthesis and Restrains Th17 Cell Pathogenicity. Cell 2015, 163, 1413–1427. [Google Scholar] [CrossRef] [Green Version]
- Sanjurjo, L.; Amézaga, N.; Aran, G.; Naranjo-Gómez, M.; Arias, L.; Armengol, C.; Borràs, F.E.; Sarrias, M.R. The human CD5L/AIM-CD36 axis: A novel autophagy inducer in macrophages that modulates inflammatory responses. Autophagy 2015, 11, 487–502. [Google Scholar] [CrossRef] [Green Version]
- Sanjurjo, L.; Aran, G.; Téllez, É.; Amézaga, N.; Armengol, C.; López, D.; Prats, C.; Sarrias, M.R. CD5L promotes M2 macrophage polarization through autophagy-mediated upregulation of ID3. Front. Immunol. 2018, 9, 480. [Google Scholar] [CrossRef]
- Iwamura, Y.; Mori, M.; Nakashima, K.; Mikami, T.; Murayama, K.; Arai, S.; Miyazaki, T. Apoptosis inhibitor of macrophage (AIM) diminishes lipid droplet-coating proteins leading to lipolysis in adipocytes. Biochem. Biophys. Res. Commun. 2012, 422, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Amézaga, N.; Sanjurjo, L.; Julve, J.; Aran, G.; Pérez-Cabezas, B.; Bastos-Amador, P.; Armengol, C.; Vilella, R. Human scavenger protein AIM increases foam cell formation and CD36-mediated oxLDL uptake. J. Leukoc. Biol. 2014, 95, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Bao, X.; Weng, X.; Bai, X.; Feng, Y.; Huang, J.; Liu, S.; Jia, H.; Yu, B. The protective effect of quercetin on macrophage pyroptosis via TLR2/Myd88/NF-κB and ROS/AMPK pathway. Life Sci. 2022, 291, 120064. [Google Scholar] [CrossRef] [PubMed]
- Langjahr, P.; Díaz-Jiménez, D.; de La Fuente, M.; Rubio, E.; Golenbock, D.; Bronfman, F.C.; Quera, R.; Gonzalez, M.J.; Hermoso, M.A. Metalloproteinase-dependent TLR2 ectodomain shedding is involved in soluble toll-like receptor 2 (sTLR2) production. PLoS ONE 2014, 9, 104624. [Google Scholar] [CrossRef]
- Henrick, B.M.; Yao, X.D.; Taha, A.Y.; Bruce German, J.; Rosenthal, K.L. Insights into soluble Toll-like receptor 2 as a downregulator of virally induced inflammation. Front. Immunol. 2016, 7, 291. [Google Scholar] [CrossRef] [Green Version]
- Salihbegovic, E.M.; Hadzigrahic, N.; Cickusic, A.J. Psoriasis and metabolic syndrome. Med. Arch. 2015, 69, 85–87. [Google Scholar] [CrossRef] [Green Version]
- Borska, L.; Kremlacek, J.; Andrys, C.; Krejsek, J.; Hamakova, K.; Borsky, P.; Palicka, V.; Rehacek, V.; Malkova, A.; Fiala, Z. Systemic inflammation, oxidative damage to nucleic acids, and metabolic syndrome in the pathogenesis of psoriasis. Int. J. Mol. Sci. 2017, 18, 2238. [Google Scholar] [CrossRef] [Green Version]
- Beygi, S.; Lajevardi, V.; Abedini, R. C-reactive protein in psoriasis: A review of the literature. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 700–711. [Google Scholar] [CrossRef]
- Mirhafez, S.R.; Ebrahimi, M.; Saberi-Karimian, M.; Avan, A.; Tayefi, M.; Heidari-Bakavoli, A.; Parizadeh, M.R.; Moohebati, M.; Azarpazhooh, M.R.; Esmaily, H.; et al. Serum high-sensitivity C-reactive protein as a biomarker in patients with metabolic syndrome: Evidence-based study with 7284 subjects. Eur. J. Clin. Nutr. 2016, 70, 1298–1304. [Google Scholar] [CrossRef]
- Kim, T.; Ganocy, S.J.; Antonelli, M.; Einstadter, D.; Ballou, S. Association of CRP with BMI in Males and Females 3–5. Available online: https://acrabstracts.org/abstract/association-of-crp-with-bmi-in-males-and-females/ (accessed on 2 December 2021).
- Zhao, S.C.; Xu, H.; Wang, Y.; Luan, D.; Wu, W.; Ma, L.; Chu, Z.H.; Xu, Y. CD200-CD200R1 signaling pathway regulates neuroinflammation after stroke. Brain Behav. 2020, 10, e01882. [Google Scholar] [CrossRef]
- Holmannova, D.; Kolackova, M.; Mandak, J.; Kunes, P.; Holubcova, Z.; Krejsek, J.; Vlaskova, D.; Andrys, C. Inhibitory CD200R and proapoptotic CD95/CD95L molecules on innate immunity cells are modulated by cardiac surgery. Perfus 2015, 30, 543–555. [Google Scholar] [CrossRef] [PubMed]
- Walker, D.G.; Dalsing-Hernandez, J.E.; Campbell, N.A.; Lue, L.F. Decreased expression of CD200 and CD200 receptor in Alzheimer’s disease: A potential mechanism leading to chronic inflammation. Exp. Neurol. 2009, 215, 5–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Zhao, L.D.; Tong, L.S.; Qian, S.N.; Ren, Y.; Zhang, L.; Ding, X.; Chen, Y.; Wang, Y.X.; Zhang, W.; et al. Aberrant CD200/CD200R1 expression and function in systemic lupus erythematosus contributes to abnormal T-cell responsiveness and dendritic cell activity. Arthritis Res. Ther. 2012, 14, R123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, S.; Hao, B.; Yang, X.F.; Chen, W.Q. Decreased CD200R expression on monocyte-derived macrophages correlates with Th17/Treg imbalance and disease activity in rheumatoid arthritis patients. Inflamm. Res. 2014, 63, 441–450. [Google Scholar] [CrossRef]
- Elshal, M.F.; Aldahlawi, A.M.; Saadah, O.I.; McCoy, J.P. Reduced dendritic cells expressing CD200R1 in children with inflammatory bowel disease: Correlation with Th17 and regulatory T cells. Int. J. Mol. Sci. 2015, 16, 28998–29010. [Google Scholar] [CrossRef] [Green Version]
- Bories, G.; Caiazzo, R.; Derudas, B.; Copin, C.; Raverdy, V.; Pigeyre, M.; Pattou, F.; Staels, B.; Chinetti-Gbaguidi, G. Impaired alternative macrophage differentiation of peripheral blood mononuclear cells from obese subjects. Diabetes Vasc. Dis. Res. 2012, 9, 189–195. [Google Scholar] [CrossRef] [Green Version]
- Ismail, A.A.; Donia, H.M.; Ghatesh, H.M.; Farid, C.I. CD200/CD200 receptor axis in psoriasis vulgaris. PLoS ONE 2020, 15, e0230621. [Google Scholar] [CrossRef] [Green Version]
- Linley, H.; Jaigirdar, S.; Mohamed, K.; Griffiths, C.E.; Saunders, A. Reduced cutaneous CD200:CD200R1 signaling in psoriasis enhances neutrophil recruitment to skin. Immunity Inflamm. Dis. 2022, 10, e648. [Google Scholar] [CrossRef]
- Taskin, I.I.; Kandemir, S.I.; Nas, K.; Dagli, A.Z. Serum Level of ADAMTS4 and ADAMTS8 in Patients with Psoriatic Arthritis. Erciyes Med. J. 2020, 43, 20–25. [Google Scholar] [CrossRef]
- Berg, G.; Miksztowicz, V. Metalloproteinases in the pathogenesis and progression of metabolic syndrome: Potential targets for improved outcomes. Met. Med. 2015, 2, 51. [Google Scholar] [CrossRef]
- Akman-Karakaş, A.; Yalcin, A.D.; Koç, S.; Gumuslu, S.; Şenol, Y.Y.; Özkesici, B.; Genç, G.E.; Ergun, E.; Ongut, G.; Yilmaz, E.; et al. There might be a role for CD200 in the pathogenesis of autoimmune and inflammatory skin disorders. Med. Sci. Monit. 2013, 19, 888–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanjurjo, L.; Aran, G.; Roher, N.; Valledor, A.F.; Sarrias, M.-R. AIM/CD5L: A key protein in the control of immune homeostasis and inflammatory disease. J. Leukoc. Biol. 2015, 98, 173–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurokaw, J.; Nagano, H.; Ohara, O.; Kubota, N.; Kadowaki, T.; Arai, S.; Miyazaki, T. Apoptosis inhibitor of macrophage (AIM) is required for obesity-associated recruitment of inflammatory macrophages into adipose tissue. Proc. Natl. Acad. Sci. USA 2011, 108, 12072–12077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shoji, S.; Uchida, K.; Inoue, G.; Takata, K.; Mukai, M.; Aikawa, J.; Iwase, D.; Takano, S.; Sekiguchi, H.; Takaso, M. Increase in CD5L expression in the synovial membrane of knee osteoarthritis patients with obesity. Cent. Eur. J. Immunol. 2021, 46, 231–235. [Google Scholar] [CrossRef]
- Lai, X.; Xiang, Y.; Zou, L.; Li, Y.; Zhang, L. Elevation of serum CD5L concentration is correlated with disease activity in patients with systemic lupus erythematosus. Int. Immunopharmacol. 2018, 63, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, L.; Henderson, R.D.; McCombe, P.A.; Lee, A. Levels of clusterin, CD5L, ficolin-3, and gelsolin in ALS patients and controls. Amyotroph Lateral Scler Front. Degener. 2020, 21, 631–634. [Google Scholar] [CrossRef]
- Bárcena, C.; Aran, G.; Perea, L.; Sanjurjo, L.; Téllez, É.; Oncins, A.; Masnou, H.; Serra, I.; García-Gallo, M.; Kremer, L.; et al. CD5L is a pleiotropic player in liver fibrosis controlling damage, fibrosis and immune cell content. EBioMedicine 2019, 43, 513–524. [Google Scholar] [CrossRef] [Green Version]
- Castelblanco, E.; Sarrias, M.R.; Betriu, À.; Soldevila, B.; Barranco-Altirriba, M.; Franch-Nadal, J.; Valdivielso, J.M.; Bermudez-Lopez, M.; Groop, P.H.; Fernández, E.; et al. Circulating CD5L is associated with cardiovascular events and all-cause mortality in individuals with chronic kidney disease. Aging 2021, 13, 22690–22709. [Google Scholar] [CrossRef]
- Cheng, Q.; Lai, X.; Yang, L.; Yang, H.; Luo, Y. Serum CD5L predicts acute lung parenchymal injury and acute respiratory distress syndrome in trauma patients. Medicine 2021, 100, e27219. [Google Scholar] [CrossRef]
- Cretu, D.; Prassas, I.; Saraon, P.; Prassas, I.; Cretu, D. Identification of psoriatic arthritis mediators in synovial fluid by quantitative mass spectrometry. Clin. Proteom. 2014, 11, 27. [Google Scholar] [CrossRef]
- Cretu, D.; Gao, L.; Liang, K.; Soosaipillai, A.; Diamandis, E.P.; Chandran, V. Differentiating Psoriatic Arthritis from Psoriasis Without Psoriatic Arthritis Using Novel Serum Biomarkers. Arthritis Care Res. 2018, 70, 454–461. [Google Scholar] [CrossRef] [Green Version]
- Fraser, S.D.; Crooks, M.G.; Kaye, P.M.; Hart, S.P. Distinct immune regulatory receptor profiles linked to altered monocyte subsets in sarcoidosis. ERJ Open Res. 2021, 7. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, P.; Bouchard, B. The impact of aging on adipose function and adipokine synthesis. Front. Endocrinol. 2019, 10, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kondelkova, K.; Krejsek, J.; Borska, L.; Fiala, Z.; Hamakova, K.; Ettler, K.; Andrys, C. Membrane and soluble Toll-like receptor 2 in patients with psoriasis treated by Goeckerman therapy. Int. J. Dermatol. 2014, 53, e512–e517. [Google Scholar] [CrossRef] [PubMed]
- Zaharieva, E.; Velikova, T.; Tsakova, A.; Kamenov, Z. Reduced soluble Toll-like receptors 2 in type 2 diabetes. Arch. Physiol. Biochem. 2018, 124, 326–329. [Google Scholar] [CrossRef] [PubMed]
- Houssen, M.E.; El-Mahdy, R.H.; Shahin, D.A. Serum soluble toll-like receptor 2: A novel biomarker for systemic lupus erythematosus disease activity and lupus-related cardiovascular dysfunction. Int. J. Rheum. Dis. 2016, 19, 685–692. [Google Scholar] [CrossRef]
- Holst, B.; Szakmany, T.; Raby, A.-C.; Hamlyn, V.; Durno, V.; Hall, J.E.; Labeta, M.O. Soluble Toll-like receptor 2 is a biomarker for sepsis in critically ill patients with multi-organ failure within 12 h of ICU admission. Intensive Care Med. Exp. 2017, 5, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Ten Oever, J.; Kox, M.; van de Veerdonk, F.L.; Mothapo, K.M.; Slavcovici, A.; Jansen, T.L.; Tweehuysen, L.; Giamarellos-Bourboulis, E.J.; Schneeberger, P.M.; Wever, P.C.; et al. The discriminative capacity of soluble Toll-like receptor (sTLR)2 and sTLR4 in inflammatory diseases. BMC Immunol. 2014, 15, 55. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Controls (n = 64; Median, Q1–Q3/Numbers) | Patients (n = 43; Median, Q1–Q3/Numbers) | |
|---|---|---|
| Age (years) | 43 (31–57) | 50 (34.5–57.8) |
| nonMetS | 49 (77.8%) | 28 (65.1%) |
| MetS | 15 (22.2%) | 15 (34.9%) |
| nonSmokers | 54 (84.4%) | 19 (44.2%) |
| Smokers | 10 (15.6%) | 24 (55.8%) |
| Sex | 34 men (53.1%), 30 women (46.9%) | 18 men (41.9%), 25 women (58.1%) |
| BMI | Median | Q1 | Q3 | p Value |
|---|---|---|---|---|
| Controls (C; n= 64) | 25.7 | 23.6 | 28.7 | p < 0.005 |
| Patients (P; n = 43) | 29.3 | 24.3 | 32.5 | |
| C nonMetS (n = 49) | 25.4 | 23.7 | 28.4 | NS |
| C MetS (n = 15) | 28.4 | 23.2 | 30.6 | |
| P nonMetS (n = 28) | 25.3 | 20.3 | 30.8 | p < 0.001 |
| P MetS (n = 15) | 32.2 | 30.1 | 36.1 |
| PASI | Median | Q1 | Q3 | p Value |
|---|---|---|---|---|
| P nonMetS (n = 28) | 19.4 | 15.6 | 26.6 | NS |
| P MetS (n = 15) | 18 | 13.7 | 25.8 |
| Parameters | Median (Q1–Q3) | p Value |
|---|---|---|
| CRP | ||
| Controls | 2.48 (2.1–3.41) | p < 0.05 |
| Patients | 3.43 (2.28–5.14) | |
| sCD200R1 (pg/mL) | ||
| Controls | 1314.5 (945–1567) | NS |
| Patients | 966 (506–2164) | |
| CD5L (ng/mL) | ||
| Controls | 1318.8 (928–1937.2) | NS |
| Patients | 1675.9 (1178–2175.8) | |
| sTLR2 (ng/mL) | ||
| Controls | 0.52 (0.41–0.73) | NS |
| Patients | 0.53 (0.45–0.81) | |
| Parameters | Median | Q1 | Q3 | p Value |
|---|---|---|---|---|
| CRP | ||||
| C MetS n = 15 | 2.77 | 1.92 | 4.04 | NS |
| C nonMetS n = 49 | 2.35 | 2.1 | 3.38 | |
| P MetS = 15 | 4.96 | 3.49 | 6.27 | p < 0.01 |
| P nonMetS n = 28 | 2.68 | 1.95 | 4.53 | |
| C MetS n = 15 | 2.77 | 1.92 | 4.04 | p < 0.05 |
| P MetS = 15 | 4.96 | 3.49 | 6.27 | |
| sCD200R1 (pg/mL) | ||||
| C MetS | 1305 | 945 | 1460 | NS |
| C nonMets | 1321 | 913 | 1575 | |
| P MetS | 1011 | 521 | 2120 | NS |
| P nonMetS | 947 | 505.25 | 2384.5 | |
| CD5L (ng/mL) | ||||
| C MetS | 1207.1 | 686 | 1937.2 | NS |
| C nonMetS | 1319.8 | 1013.3 | 1951.3 | |
| P MetS | 1915 | 1244 | 2704 | p < 0.02 |
| P nonMetS | 1400.5 | 1008.5 | 2040 | |
| C MetS | 1207.1 | 686 | 1937.2 | p < 0.08 |
| P MetS | 1915 | 1244 | 2704 | |
| sTLR2 (ng/mL) | ||||
| C MetS | 0.5 | 0.43 | 0.69 | NS |
| C nonMetS | 0.52 | 0.4 | 0.74 | |
| P MetS | 0.53 | 0.47 | 0.84 | NS |
| P nonMetS | 0.49 | 0.45 | 0.8 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holmannova, D.; Borsky, P.; Andrys, C.; Krejsek, J.; Cermakova, E.; Fiala, Z.; Hamakova, K.; Svadlakova, T.; Parova, H.; Rehacek, V.; et al. The Presence of Psoriasis, Metabolic Syndrome and Their Combination Increases the Serum Levels of CRP and CD5L but Not sCD200R1 and sTLR2 in Participants. J. Pers. Med. 2022, 12, 1965. https://doi.org/10.3390/jpm12121965
Holmannova D, Borsky P, Andrys C, Krejsek J, Cermakova E, Fiala Z, Hamakova K, Svadlakova T, Parova H, Rehacek V, et al. The Presence of Psoriasis, Metabolic Syndrome and Their Combination Increases the Serum Levels of CRP and CD5L but Not sCD200R1 and sTLR2 in Participants. Journal of Personalized Medicine. 2022; 12(12):1965. https://doi.org/10.3390/jpm12121965
Chicago/Turabian StyleHolmannova, Drahomira, Pavel Borsky, Ctirad Andrys, Jan Krejsek, Eva Cermakova, Zdenek Fiala, Kvetoslava Hamakova, Tereza Svadlakova, Helena Parova, Vit Rehacek, and et al. 2022. "The Presence of Psoriasis, Metabolic Syndrome and Their Combination Increases the Serum Levels of CRP and CD5L but Not sCD200R1 and sTLR2 in Participants" Journal of Personalized Medicine 12, no. 12: 1965. https://doi.org/10.3390/jpm12121965