
Effectiveness of Dupilumab in the Treatment of Patients with Uncontrolled Severe CRSwNP: A “Real-Life” Observational Study in Naïve and Post-Surgical Patients
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Clinical Evaluation
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ottaviano, G.; Cappellesso, R.; Mylonakis, I.; Lionello, M.; Favaretto, N.; Giacomelli, L.; Spoladore, C.; Marchese-Ragona, R.; Marino, F.; Staffieri, A.; et al. Endoglin (CD105) Expression in Sinonasal Polyposis. Eur Arch. Otorhinolaryngol. 2015, 272, 3367–3373. [Google Scholar] [CrossRef] [PubMed]
- Bayar Muluk, N.; Cingi, C.; Scadding, G.K.; Scadding, G. Chronic Rhinosinusitis—Could Phenotyping or Endotyping Aid Therapy? Am. J. Rhinol. Allergy 2019, 33, 83–93. [Google Scholar] [CrossRef] [PubMed]
- de Corso, E.; Bellocchi, G.; de Benedetto, M.; Lombardo, N.; Macchi, A.; Malvezzi, L.; Motta, G.; Pagella, F.; Vicini, C.; Passali, D. Biologics for Severe Uncontrolled Chronic Rhinosinusitis with Nasal Polyps: A Change Management Approach. Consensus of the Joint Committee of Italian Society of Otorhinolaryngology on Biologics in Rhinology. Acta Otorhinolaryngol. Ital. 2022, 42, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinol. J. 2020, 58, 1–464. [Google Scholar] [CrossRef]
- Bachert, C.; Han, J.K.; Wagenmann, M.; Hosemann, W.; Lee, S.E.; Backer, V.; Mullol, J.; Gevaert, P.; Klimek, L.; Prokopakis, E.; et al. EUFOREA Expert Board Meeting on Uncontrolled Severe Chronic Rhinosinusitis with Nasal Polyps (CRSwNP) and Biologics: Definitions and Management. J. Allergy Clin. Immunol. 2021, 147, 29–36. [Google Scholar] [CrossRef]
- Bachert, C.; Han, J.K.; Desrosiers, M.; Hellings, P.W.; Amin, N.; Lee, S.E.; Mullol, J.; Greos, L.S.; Bosso, J.V.; Laidlaw, T.M.; et al. Efficacy and Safety of Dupilumab in Patients with Severe Chronic Rhinosinusitis with Nasal Polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): Results from Two Multicentre, Randomised, Double-Blind, Placebo-Controlled, Parallel-Group Phase 3 Trials. Lancet 2019, 394, 1638–1650. [Google Scholar] [CrossRef]
- van der Lans, R.J.L.; Fokkens, W.J.; Adriaensen, G.F.J.P.M.; Hoven, D.R.; Drubbel, J.J.; Reitsma, S. Real-life Observational Cohort Verifies High Efficacy of Dupilumab for Chronic Rhinosinusitis with Nasal Polyps. Allergy 2022, 77, 670–674. [Google Scholar] [CrossRef]
- de Corso, E.; Settimi, S.; Montuori, C.; Corbò, M.; Passali, G.C.; Porru, D.P.; lo Verde, S.; Spanu, C.; Penazzi, D.; di Bella, G.A.; et al. Effectiveness of Dupilumab in the Treatment of Patients with Severe Uncontrolled CRSwNP: A “Real-Life” Observational Study in the First Year of Treatment. J. Clin. Med. 2022, 11, 2684. [Google Scholar] [CrossRef]
- Gevaert, P.; Calus, L.; van Zele, T.; Blomme, K.; de Ruyck, N.; Bauters, W.; Hellings, P.; de Bacquer, D.; Brusselle, G.; van Cauwenberge, P.; et al. Omalizumab Is Effective In Allergic And Non-Allergic Patients With Nasal Polyps And Asthma. J. Allergy Clin. Immunol. 2012, 129, AB69. [Google Scholar] [CrossRef]
- Ottaviano, G.; Zuccarello, D.; Frasson, G.; Scarpa, B.; Nardello, E.; Foresta, C.; Marioni, G.; Staffieri, A. Olfactory Sensitivity and Sexual Desire in Young Adult and Elderly Men: An Introductory Investigation. Am. J. Rhinol. Allergy 2013, 27, 157–161. [Google Scholar] [CrossRef]
- Rimmer, J.; Hellings, P.; Lund, V.J.; Alobid, I.; Beale, T.; Dassi, C.; Douglas, R.; Hopkins, C.; Klimek, L.; Landis, B.; et al. European Position Paper on Diagnostic Tools in Rhinology. Rhinol. J. 2019, 57, 1–41. [Google Scholar] [CrossRef] [PubMed]
- Huvanandana, J.; Nguyen, C.D.; Foster, J.M.; Frey, U.; Reddel, H.K.; Thamrin, C. Novel Methods of Measuring Adherence Patterns Reveal Adherence Phenotypes with Distinct Asthma Outcomes. Ann. Am. Thorac. Soc. 2022, 19, 933–942. [Google Scholar] [CrossRef]
- Ottaviano, G.; Pendolino, A.L.; Nardello, E.; Maculan, P.; Martini, A.; Russo, M.; Lund, V.J. Peak Nasal Inspiratory Flow Measurement and Visual Analogue Scale in a Large Adult Population. Clin. Otolaryngol. 2019, 44, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Hummel, T.; Whitcroft, K.L.; Andrews, P.; Altundag, A.; Cinghi, C.; Costanzo, R.M.; Damm, M.; Frasnelli, J.; Gudziol, H.; Gupta, N.; et al. Position Paper on Olfactory Dysfunction. Rhinol. J. 2017, 54, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Ottaviano, G.; Marioni, G.; Giacomelli, L.; la Torre, F.B.; Staffieri, C.; Marchese-Ragona, R.; Staffieri, A. Smoking and Chronic Rhinitis: Effects of Nasal Irrigations with Sulfurous-Arsenical-Ferruginous Thermal Water: A Prospective, Randomized, Double-Blind Study. Am. J. Otolaryngol. 2012, 33, 657–662. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Bordin, A.; Mucignat-Caretta, C.; Gaudioso, P.; Pendolino, A.L.; Leoni, D.; Scarpa, B.; Andrews, P.J.; Cattelan, A.M.; Antonini, A.; Nicolai, P.; et al. Comparison of Self-Reported Symptoms and Psychophysical Tests in Coronavirus Disease 2019 (COVID-19) Subjects Experiencing Long-Term Olfactory Dysfunction: A 6-Month Follow-up Study. Int. Forum Allergy Rhinol. 2021, 11, 1592–1595. [Google Scholar] [CrossRef]
- Pendolino, A.L.; Scarpa, B.; Ottaviano, G. Relationship Between Nasal Cycle, Nasal Symptoms and Nasal Cytology. Am. J. Rhinol. Allergy 2019, 33, 644–649. [Google Scholar] [CrossRef]
- Pendolino, A.L.; Nardello, E.; Lund, V.J.; Maculan, P.; Scarpa, B.; Martini, A.; Ottaviano, G. Comparison between Unilateral PNIF and Rhinomanometry in the Evaluation of Nasal Cycle. Rhinology 2018, 56, 122–126. [Google Scholar] [CrossRef]
- Marioni, G.; Ottaviano, G.; Staffieri, A.; Zaccaria, M.; Lund, V.J.; Tognazza, E.; Coles, S.; Pavan, P.; Brugin, E.; Ermolao, A. Nasal Functional Modifications after Physical Exercise: Olfactory Threshold and Peak Nasal Inspiratory Flow. Rhinol. J. 2010, 48, 277–280. [Google Scholar] [CrossRef]
- Ottaviano, G.; Lund, V.; Nardello, E.; Scarpa, B.; Frasson, G.; Staffieri, A.; Scadding, G. Comparison between Unilateral PNIF and Rhinomanometry in Healthy and Obstructed Noses. Rhinol. J. 2014, 52, 25–30. [Google Scholar] [CrossRef]
- Oleszkiewicz, A.; Schriever, V.A.; Croy, I.; Hähner, A.; Hummel, T. Updated Sniffin’ Sticks Normative Data Based on an Extended Sample of 9139 Subjects. Eur. Arch. Oto-Rhino-Laryngol. 2019, 276, 719–728. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, C.; Lund, V. Does Time from Previous Surgery Predict Subsequent Treatment Failure in Chronic Rhinosinusitis with Nasal Polyps? Rhinology 2021, 59, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Saunders, M.W.; Wheatley, A.H.; George, S.J.; Lai, T.; Birchall, M.A. Do Corticosteroids Induce Apoptosis in Nasal Polyp Inflammatory Cells? In Vivo and in Vitro Studies. Laryngoscope 1999, 109, 785–790. [Google Scholar] [CrossRef] [PubMed]
- Pendolino, A.L.; Scadding, G.K.; Scarpa, B.; Andrews, P.J. A Retrospective Study on Long-Term Efficacy of Intranasal Lysine-Aspirin in Controlling NSAID-Exacerbated Respiratory Disease. Eur. Arch. Oto-Rhino-Laryngol. 2022, 279, 2473–2484. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-K.; Lim, H.-S.; Eun, K.M.; Seo, Y.; Kim, J.K.; Kim, Y.S.; Kim, M.-K.; Jin, S.; Han, S.C.; Kim, D.W. Subepithelial Neutrophil Infiltration as a Predictor of the Surgical Outcome of Chronic Rhinosinusitis with Nasal Polyps. Rhinol. J. 2021, 59, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.K.; Kim, J.Y.; Han, Y.E.; Kim, J.K.; Lim, H.S.; Eun, K.M.; Yang, S.K.; Kim, D.W. Elastase-Positive Neutrophils Are Associated With Refractoriness of Chronic Rhinosinusitis With Nasal Polyps in an Asian Population. Allergy Asthma Immunol. Res. 2020, 12, 42–55. [Google Scholar] [CrossRef]
- Delemarre, T.; Bochner, B.S.; Simon, H.-U.; Bachert, C. Rethinking Neutrophils and Eosinophils in Chronic Rhinosinusitis. J. Allergy Clin. Immunol. 2021, 148, 327–335. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All n = 47 | Post-Surgical n = 33 | Naïve n = 14 | p | |
|---|---|---|---|---|
| Age, mean (SD), yr | 51.8 (13.5) | 53.6 (10.5) | 47.6 (18.5) | 0.42 |
| Asthma, n (%) | 25 (53.2) | 17 (51.5) | 8 (57.1) | 1 |
| Smokers, n (%) | 6 (12.8) | 3 (9.1) | 3 (21.4) | 0.35 |
| NSAIDs intolerance (%) | 9 (19.1) | 7 (21.2) | 2 (14.3) | 0.70 |
| Lund–Mackay score | 16.3 (4.2) | 16.33 (3.82) | 16.23 (5.26) | 0.93 |
| VAS-NO, mean (SD) | 7.62 (2.45) | 7.24 (2.66) | 8.50 (1.65) | 0.13 |
| VAS-smell, mean (SD) | 8.41 (2.53) | 8.47 (2.59) | 8.29 (2.46) | 0.63 |
| SNOT-22, mean (SD) | 58.83 (21.53) | 59.18 (23.71) | 58.00 (15.97) | 0.72 |
| NCS, mean (SD) | 2.47 (0.73) | 2.39 (0.67) | 2.64 (0.84) | 0.09 |
| ACT, mean (SD) | 9.9 (10.11) | 9.92 (9.98) | 10 (10.96) | 0.97 |
| NPS, mean (SD) | 5.51 (1.40) | 5.33 (1.57) | 5.93 (0.73) | 0.42 |
| PNIF, mean (SD) | 128.89 (64.29) | 139.52 (63.39) | 105.36 (62.03) | 0.07 |
| SSIT, mean (SD) | 6.1 (2.7) | 6.0 (2.7) | 6.4 (2.8) | 0.64 |
| Blood eosinophilia, mean (SD) | 0.51(0.29) | 0.49 (0.30) | 0.54 (0.27) | 0.61 |
| Eosinophils cytology, mean (SD) | 2.67 (4.91) | 2.04 (3.87) | 4.3 (6.93) | 0.53 |
| Neutrophils cytology, mean (SD) | 43.83 (66.37) | 54.27 (74.88) | 36.7 (20.61) | 0.07 |
| OCS courses/last y, mean (SD) | 2.6 (2.31) | 2.19 (1.74) | 3.5 (3.13) | 0.09 |
| T1 vs. T0 | T3 vs. T1 | T6 vs. T3 | T9 vs. T6 | T12 vs. T9 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Difference | p | Difference | p | Difference | p | Difference | p | Difference | p | |
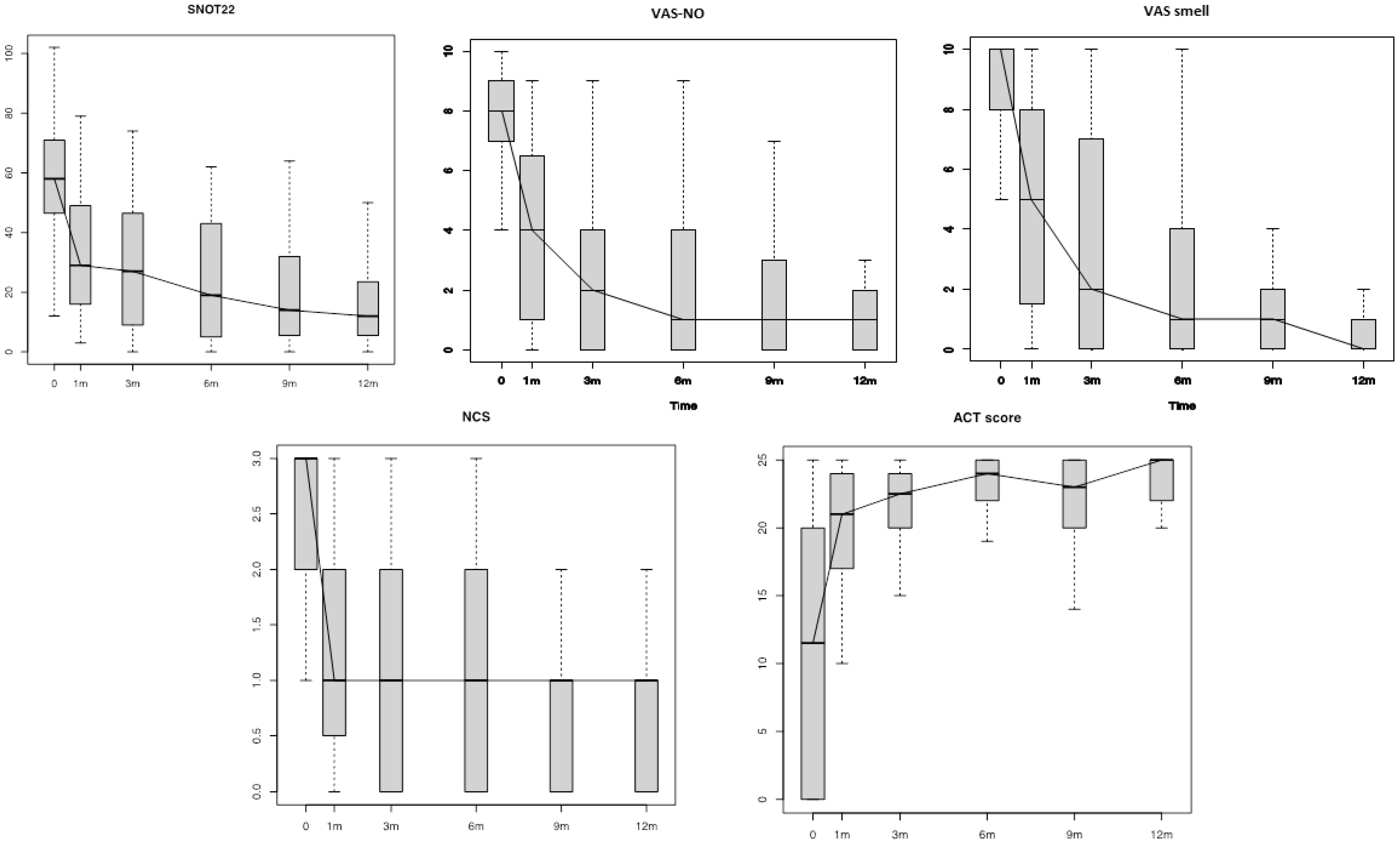
| VAS-NO | −4.00 | <0.01 | −1.23 | <0.01 | 0.11 | 0.82 | −0.11 | 0.50 | 0.17 | 0.15 |
| VAS-smell | −3.66 | <0.01 | −1.52 | <0.01 | −0.50 | 0.34 | −0.48 | 0.05 | −0.22 | 0.24 |
| SNOT22 | −27.17 | <0.01 | −4.95 | 0.02 | −0.26 | 0.01 | −3.64 | 0.89 | 0.32 | 0.92 |
| NCS | −1.07 | <0.01 | −0.47 | <0.01 | −0.12 | 0.30 | 0.07 | 0.53 | 0.00 | 1.00 |
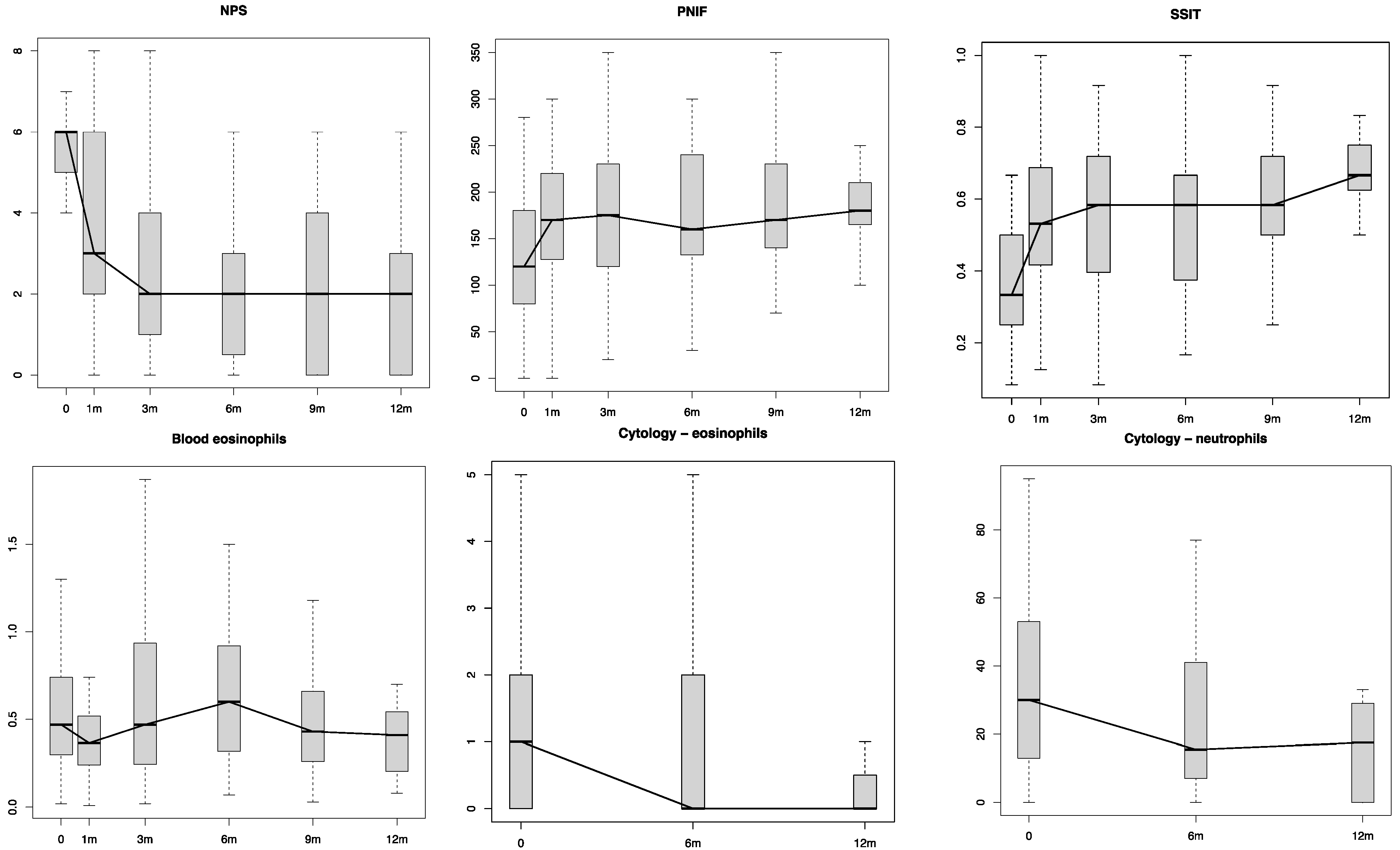
| NPS | −1.98 | <0.01 | −0.74 | <0.01 | −0.34 | 0.18 | 0.07 | 0.86 | −0.65 | 0.08 |
| PNIF | 39.56 | <0.01 | 3.98 | 0.82 | −3.14 | 0.98 | 4.48 | 0.51 | −1.84 | 0.91 |
| SSIT | 0.18 | <0.01 | 0.01 | 0.90 | 0.01 | 0.58 | 0.02 | 1.00 | 0.01 | 0.75 |
| Blood eosinophilia | −0.06 | 0.16 | 0.01 | 0.82 | 0.10 | 0.46 | −0.10 | 0.32 | −0.09 | 0.05 |
| T1 vs. T0 | - | T6 vs. T1 | - | T12 vs. T6 | ||||||
| Eosinophils cytology | −1.91 | 0.06 | - | - | −0.69 | 0.34 | - | - | 2.80 | 0.37 |
| Neutrophils cytology | −21.03 | 0.01 | - | - | 32.44 | 0.67 | - | - | −40.20 | 0.10 |
| T0 | T1 | T3 | T6 | T9 | T12 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| corr | p | corr | p | corr | p | corr | p | corr | p | corr | p | |
| PNIF vs. VAS−NO | −0.15 | 0.32 | −0.42 | 0.003 | −0.51 | <0.001 | −0.34 | 0.043 | −0.34 | 0.07 | −0.34 | 0.15 |
| SSIT vs. VAS−smell | −0.31 | 0.04 | −0.26 | 0.08 | −0.36 | 0.017 | −0.52 | 0.002 | −0.10 | 0.61 | 0.15 | 0.54 |
| NPS vs. SNOT22 | −0.30 | 0.06 | −0.08 | 0.63 | −0.05 | 0.73 | −0.13 | 0.46 | −0.37 | 0.06 | −0.22 | 0.37 |
| NPS vs. SSIT | −0.36 | 0.02 | −0.11 | 0.47 | −0.25 | 0.10 | −0.20 | 0.27 | 0.05 | 0.81 | 0.04 | 0.86 |
| NPS vs. PNIF | 0.05 | 0.76 | 0.01 | 0.95 | 0.08 | 0.59 | 0.01 | 0.96 | −0.11 | 0.57 | −0.28 | 0.26 |
| Blood eosinophilia vs. eosinophils cytology | 0.17 | 0.37 | 0.27 | 0.21 | - | - | −0.49 | 0.11 | - | - | 0.87 | 0.06 |
| T1 vs. T0 | T3 vs. T1 | T6 vs. T3 | T9 vs. T6 | T12 vs. T9 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Difference | p | Difference | p | Difference | p | Difference | p | Difference | p | ||||||
| Naive | Surg. | Naive | Surg. | Naive | Surg. | Naive | Surg. | Naive | Surg. | ||||||
| VAS−NO | −4.00 | −4.00 | 0.91 | −1.38 | −1.16 | 0.66 | −0.20 | 0.24 | 0.77 | 0.22 | −0.26 | 0.29 | 0.12 | 0.20 | 0.73 |
| VAS−smell | −3.71 | −3.64 | 0.87 | −2.38 | −1.15 | 0.36 | 0.20 | −0.79 | 0.56 | −0.44 | −0.50 | 0.98 | 0.12 | −0.50 | 0.07 |
| SNOT−22 | −23.36 | −28.84 | 0.46 | −7.46 | −3.87 | 0.62 | 7.00 | −3.29 | 0.82 | −8.56 | −1.32 | 0.43 | −1.12 | 1.36 | 0.11 |
| NCS | −0.85 | −1.17 | 0.31 | −0.58 | −0.43 | 0.01 | −0.30 | −0.04 | 0.32 | 0.22 | 0.00 | 0.34 | 0.25 | −0.20 | 0.06 |
| NPS | −1.21 | −2.32 | 0.07 | −1.38 | −0.47 | 0.07 | 1.20 | −0.44 | 0.29 | 0.11 | 0.05 | 0.39 | −1.29 | −0.20 | 0.15 |
| PNIF | 42.86 | 38.06 | 0.65 | 2.31 | 4.68 | 0.87 | −17.50 | 2.60 | 0.37 | 31.67 | −7.75 | 0.36 | −14.38 | 0.20 | 0.53 |
| SSIT | 0.23 | 0.16 | 0.26 | 0.04 | 0.01 | 1.00 | −0.02 | 0.02 | 0.58 | 0.01 | 0.02 | 0.73 | 0.05 | −0.01 | <0.01 |
| Blood eosinophilia | −0.04 | −0.07 | 1.00 | −0.03 | 0.03 | 0.66 | 0.29 | 0.01 | 0.19 | −0.50 | 0.03 | 0.04 | −0.07 | −0.11 | 1.00 |
| Eosinophils cytology | −3.60 | −1.21 | 0.37 | 0.00 | −1.10 | 0.46 | 0.50 | 4.33 | 1.00 | −3.60 | −1.21 | 0.37 | 0.00 | −1.10 | 0.46 |
| Neutrophils cytology | −3.10 | −28.50 | 0.07 | −7.50 | 56.40 | 0.30 | −9.50 | −60.67 | 0.40 | −3.10 | −28.50 | 0.07 | −7.50 | 56.40 | 0.30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ottaviano, G.; Saccardo, T.; Roccuzzo, G.; Bernardi, R.; Chicco, A.D.; Pendolino, A.L.; Scarpa, B.; Mairani, E.; Nicolai, P. Effectiveness of Dupilumab in the Treatment of Patients with Uncontrolled Severe CRSwNP: A “Real-Life” Observational Study in Naïve and Post-Surgical Patients. J. Pers. Med. 2022, 12, 1526. https://doi.org/10.3390/jpm12091526
Ottaviano G, Saccardo T, Roccuzzo G, Bernardi R, Chicco AD, Pendolino AL, Scarpa B, Mairani E, Nicolai P. Effectiveness of Dupilumab in the Treatment of Patients with Uncontrolled Severe CRSwNP: A “Real-Life” Observational Study in Naïve and Post-Surgical Patients. Journal of Personalized Medicine. 2022; 12(9):1526. https://doi.org/10.3390/jpm12091526
Chicago/Turabian StyleOttaviano, Giancarlo, Tommaso Saccardo, Giuseppe Roccuzzo, Riccardo Bernardi, Alessandra Di Chicco, Alfonso Luca Pendolino, Bruno Scarpa, Edoardo Mairani, and Piero Nicolai. 2022. "Effectiveness of Dupilumab in the Treatment of Patients with Uncontrolled Severe CRSwNP: A “Real-Life” Observational Study in Naïve and Post-Surgical Patients" Journal of Personalized Medicine 12, no. 9: 1526. https://doi.org/10.3390/jpm12091526