
Supraglottic Localization of IgG4-Related Disease—Rare and Challenging Equity

 ,
,
Abstract
:1. Introduction
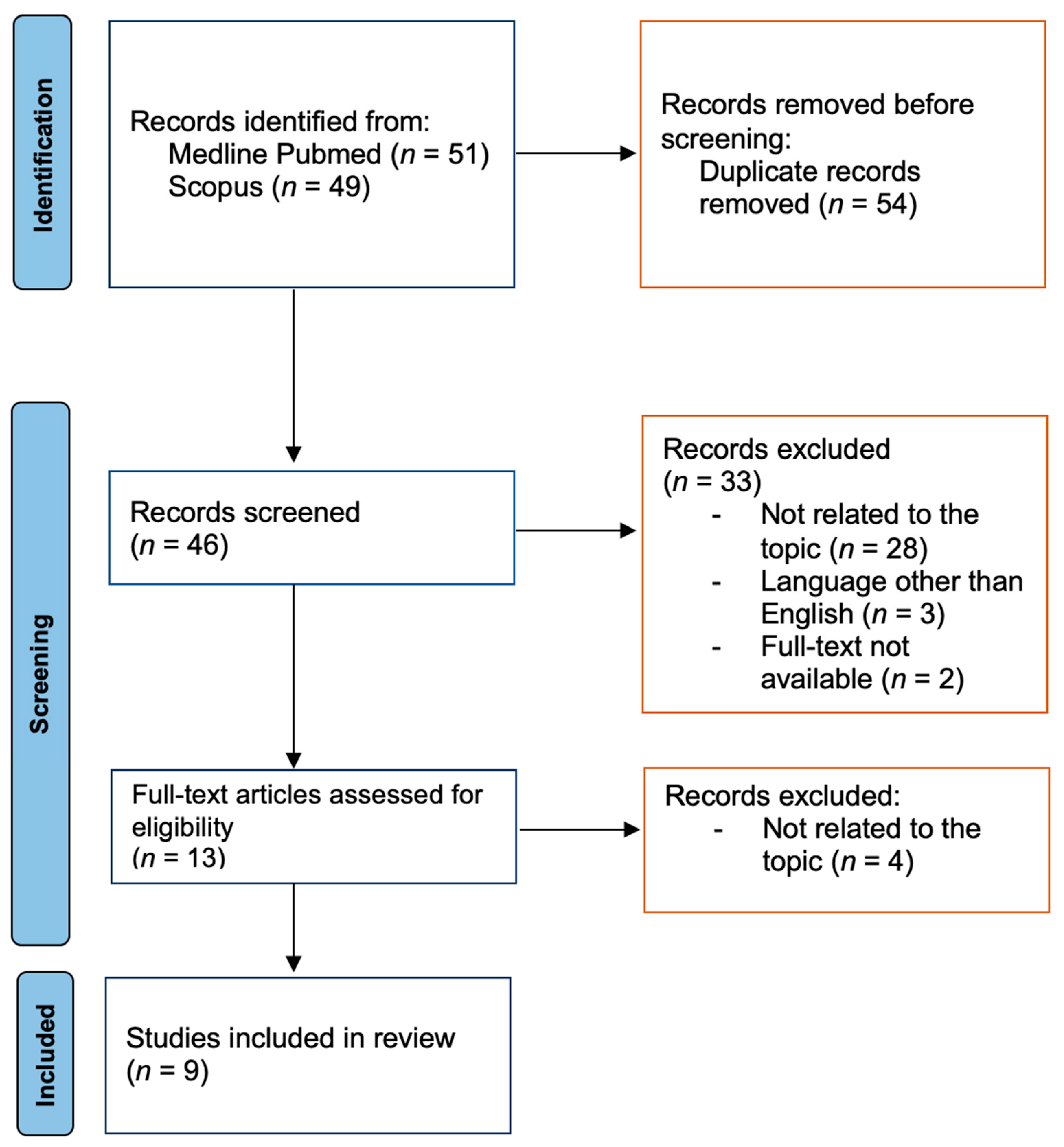
2. Materials and Methods
3. Results
3.1. Overview of Previously Published Case Reports
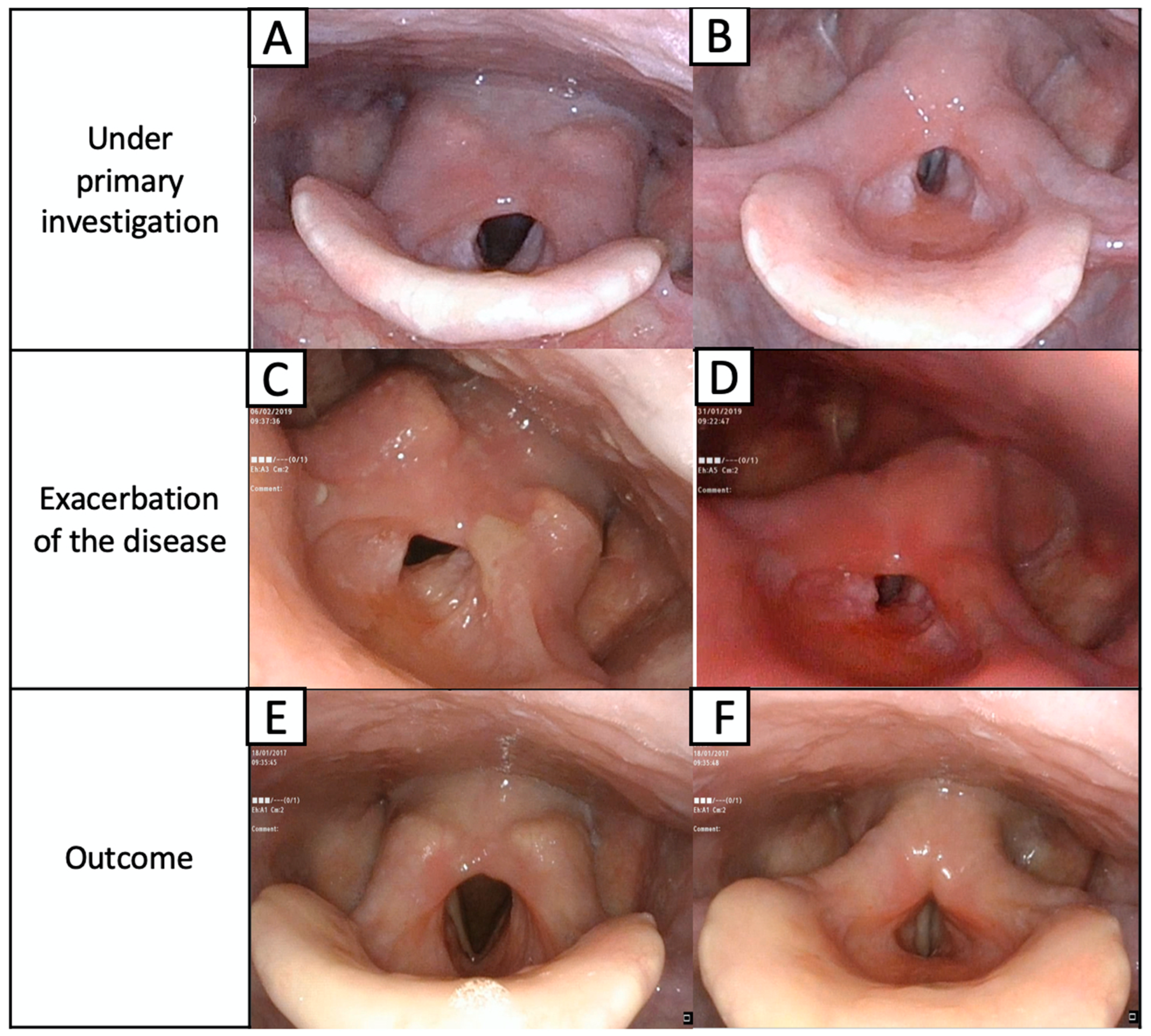
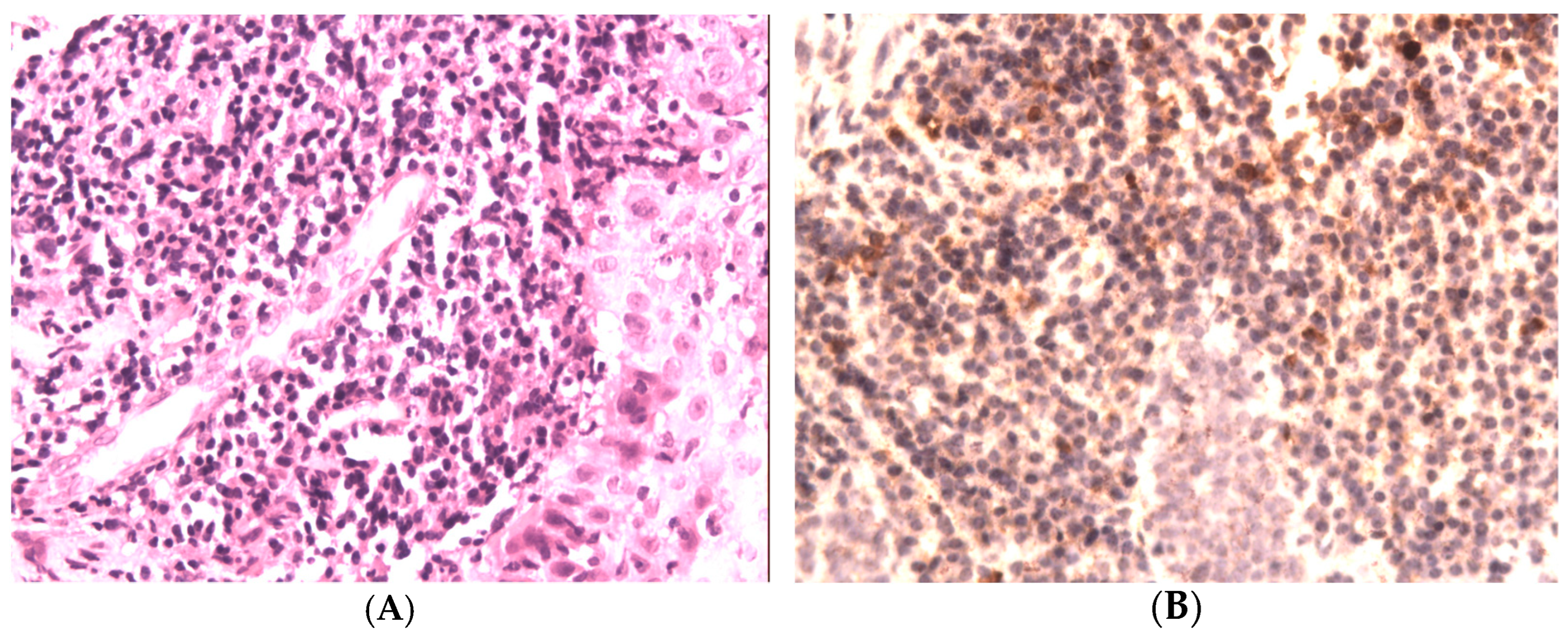
3.2. Case Report of L.G.
4. Discussion
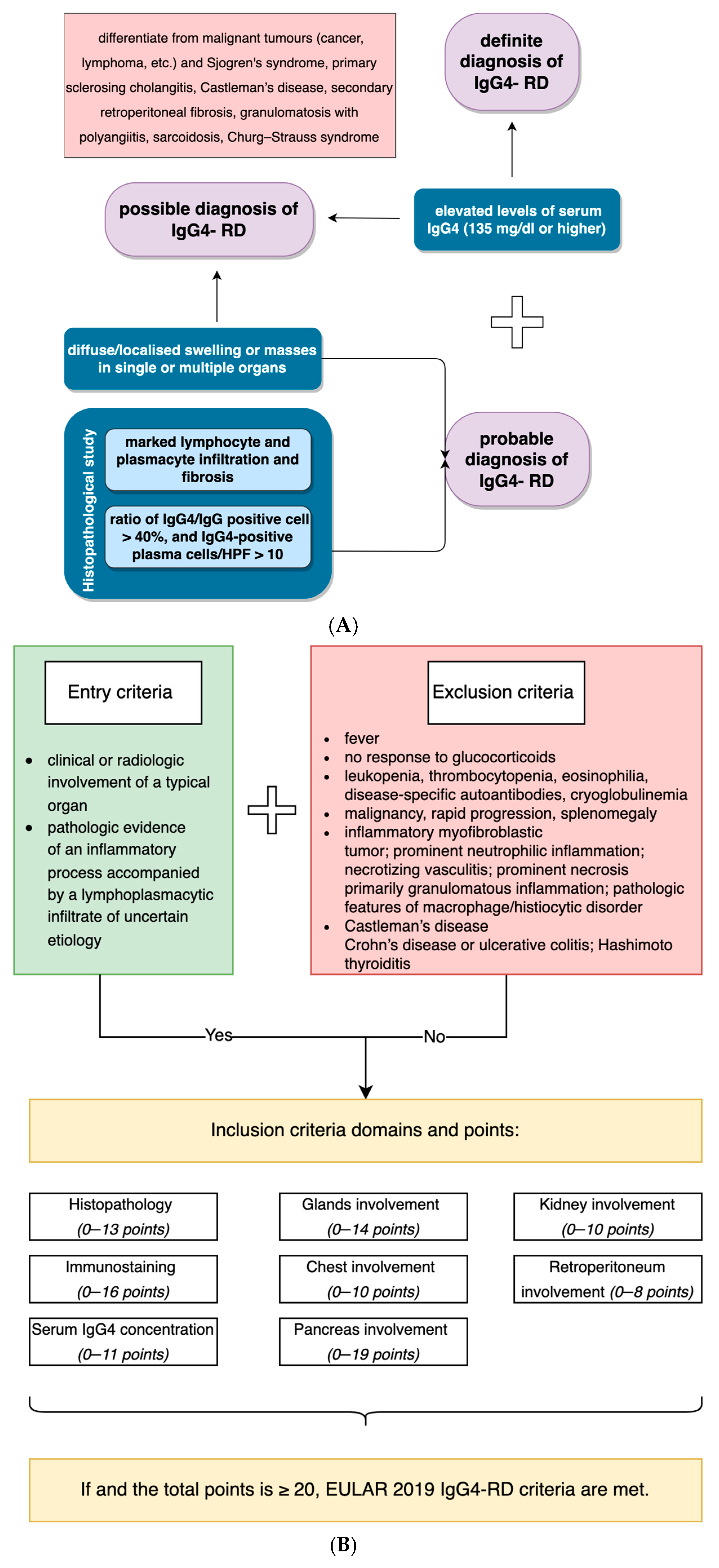
4.1. Diagnosis of IgG4-Related Disease: Comprehensive vs. ACR/EULAR Criteria
4.2. Differential Diagnosis between IgG4-RD and ANCA-Associated Diseases
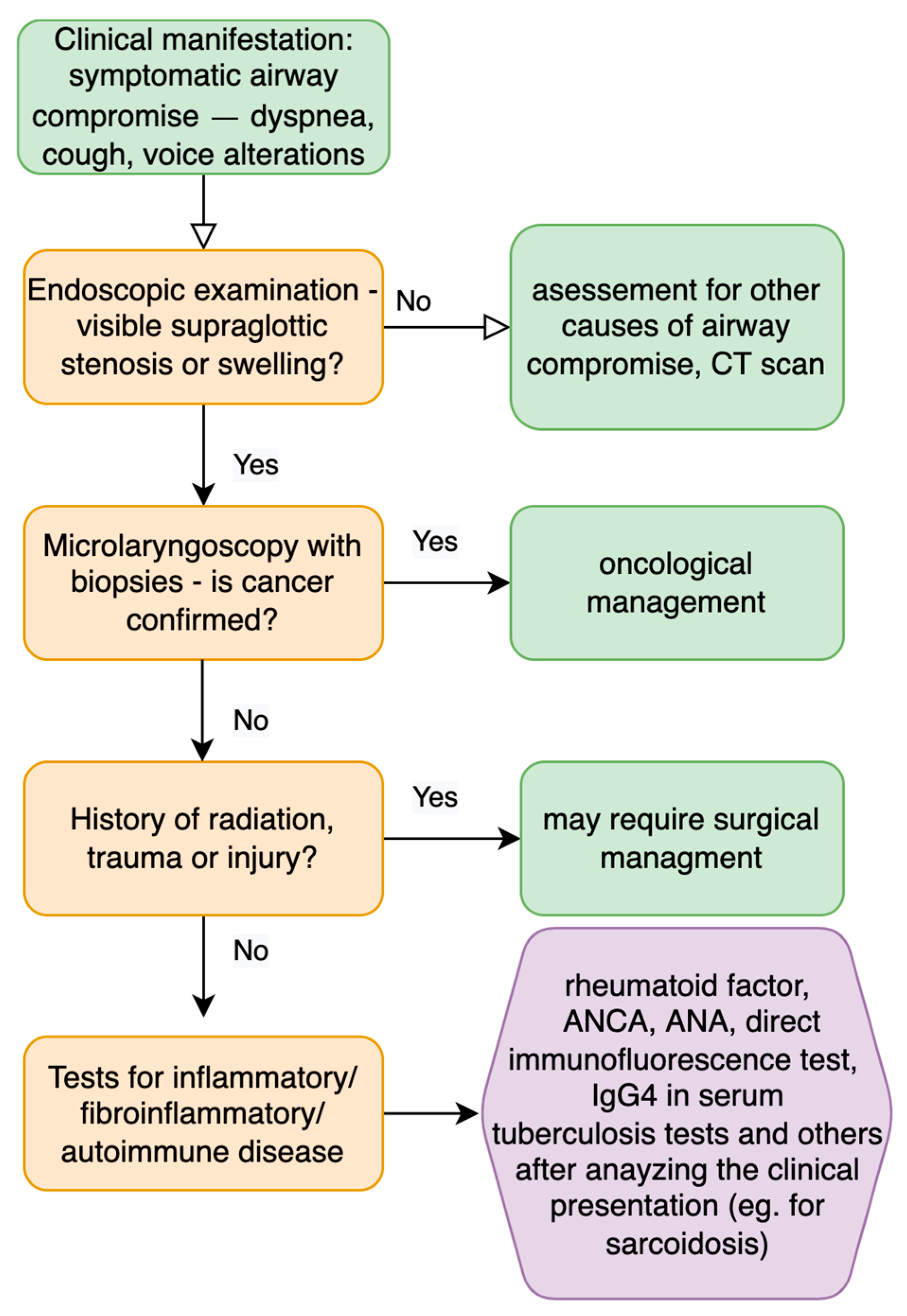
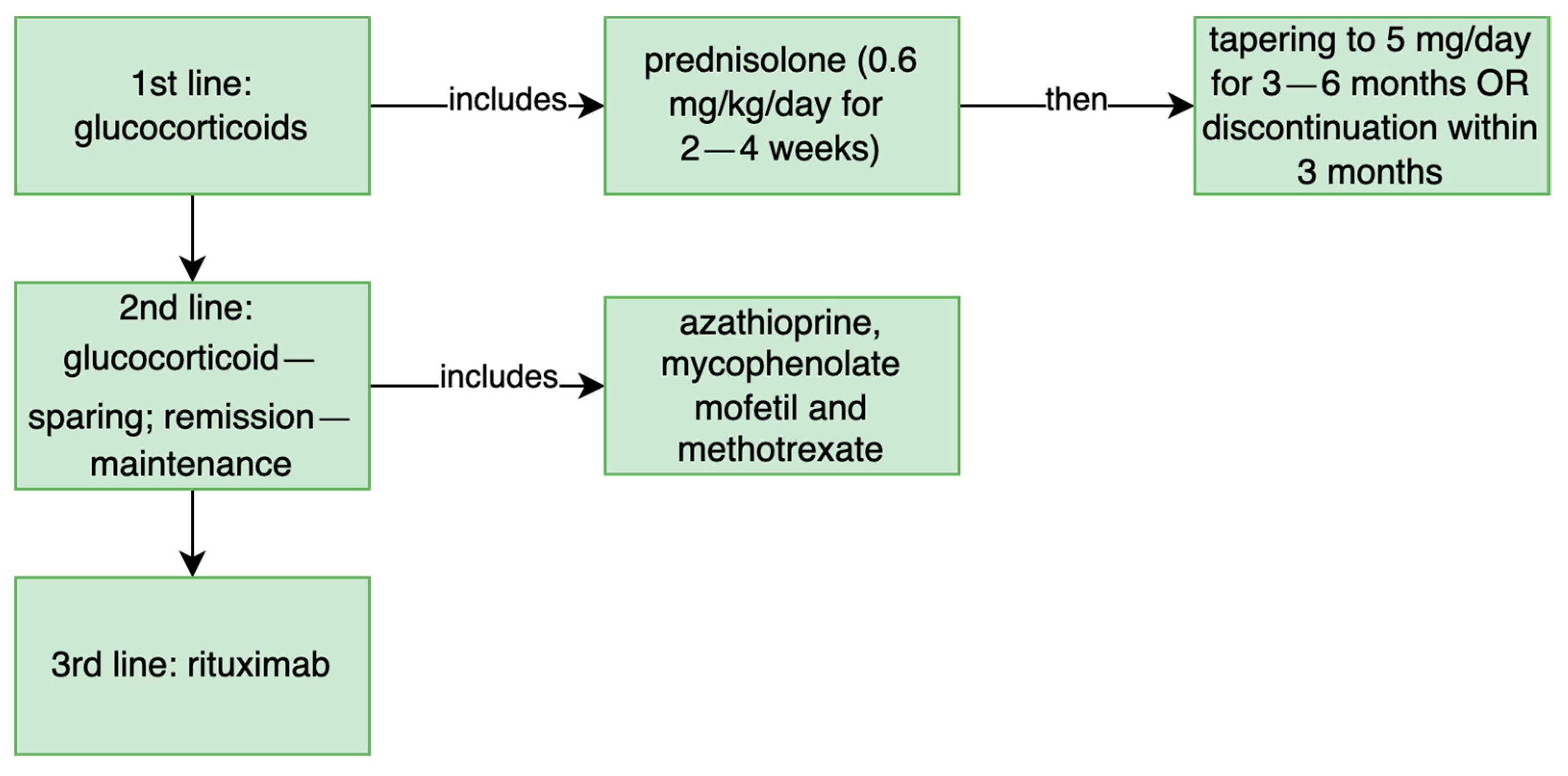
4.3. Management of Supraglottic Stenosis in ENT Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Endoscopic Examination | Treatment/Intervention | Outcome | IgG4 Serum Level and Histopathology | Comprehensive Criteria | EULAR Criteria |
|---|---|---|---|---|---|---|
| Patient L.G.—current case | narrowing of laryngeal inlet; aryepiglottic folds thickening, hypertrophy of posterior commissure; limited mobility of vocal folds | (1) methotrexate (20 mg/week), changed to 150 mg azathioprine daily; prednisone (5 mg/day—starting from glucocorticoids pulses 3 × 1000 mg methylprednisolone, then 30 mg prednisone in descending doses). (2) cyclophosphamide (1 g for every 4 weeks); methylprednisolone (500 mg in pulses for 3 days and then 1 pulse for a month) | (1) poor toleration of methotrexate; after initial improvement stenosis increased; (2) significant improvement | IgG4 serum level >135 mg/dL; IgG4 in 50% of mononuclear cells of massive inflammatory infiltration from the biopsy specimens | definite diagnosis | 15 |
| Matsushima (2019) [8] | diffuse swelling—left arytenoid region, obscuring visualization of the glottis | (1) wide resection with CO2 laser; (2) tracheostomy (3) prednisolone (0.6 mg/kg/day); now 5 mg/day | reduction of tumor size after 2 weeks of treatment | serum IgG4 31 mg/dL; storiform fibrosis; >100 IgG4-positive plasma cells and 50% IgG4/IgG | probable diagnosis | ≥20 |
| Maughan (2020) patient 1: [7] | supraglottic and interarytenoid fibrosis | (1) balloon dilatation and microlaryngoscopy + laser excision + steroid injections; (2) oral prednisolone + azathioprine then switched for methotrexate; (3) laryngotracheal reconstruction | transient relief after 1 and 2 treatment; significant long-term improvement after treatment 3, back to oral intake and work | IgG4 serum level—normal; lymphoplasmocytic infiltrate, fibrosis, IgG4:IgG ratio 80% in biopsy specimens; | probable diagnosis | ≥20 |
| Maughan (2020) patient 2: [7] | supraglottic swelling | (1) balloon dilatation and microlaryngoscopy + laser excision + steroid injections; (2) immunomodulatory treatment then for 30 months patient declined treatment | (1) had to be repeated every 4–6 months (2) patient for 30 months remains in “watch and wait” approach | IgG4 serum level normal; subepithelial lymphoid infiltrate, plasma cells, 20% positive cells for IgG4 (50 IgG+ in high power field); | probable diagnosis | 4 |
| Maughan (2020) patient 3: [7] | supraglottic scarring; restricted arytenoid movement bilaterally | balloon dilatation and microlaryngoscopy + laser excision + steroid injections | dilatation repeated every 4 to 6 months; after the diagnosis patient got the prednisolone; however, no further follow up is described | chronic inflammation, fibrosis, IgG serology 0.9 range; ANCA- negative; confirmed on biopsy specimens | probable diagnosis | 13 |
| Hamadani (2016) [9] | mucus in the supraglottis, postcricoid region ulcer, laryngospasm | treatment not described | outcome not described | IgG lymphocytoid plasma-cell infiltrates, with >90% of IgG-positive plasma cells that were IgG4-positive | probable diagnosis | 8 |
| Ferrante (2017) [10] | anterior septal perforation, lateral nasal wall scarring, supraglottis cicatricial narrowing down to 4 mm in diameter | tracheostomy; prednisolone 40 mg/d lowered to 10 mg/d | slow improvement; decannulation after 16 months | 40 IgG4 plasma cells in high-powered field, storiform fibrosis, lymphoplasmatic mucositis | probable diagnosis | ≥20 |
| Reder (2015) patient 1: [11] | lesions on the base of tongue extending to aryepiglottic fold, right vocal process; | (1) laser excision of the lesion; (2) prednisolone 40 mg/day for 2 weeks; (3) rituximab 1 g—2 doses, 2 weeks apart, methylprednisolone 100 mg/day with every rituximab infusion | (1) second excision without long-term improvement; (2) poor toleration of prednisolone; (3) for 2 years patient remains in remission | IgG4 serum level: 196 mg/dL; polypoid squamous mucosa; diffuse storiform fibrosis, dense lymphoplasmacytic infiltrate; 50 IgG4-positive cells per high-power field; IgG4:IgG ratio > 0.50; | definite diagnosis | ≥20 |
| Reder (2015) patient 2: [11] | granular mucosa—base of the tongue and the epiglottis; keratosis, hyperplasia of the aryepiglottic folds, the false and true vocal cords | (1) 2 courses of prednisone 60 mg for 7 days, then 7-day taper; (2) rituximab 1 g—2 doses, 2 weeks apart, methylprednisolone 100 mg/day with every rituximab infusion | (1) “modest” clinical improvement; (2) significant improvement | serum level: 28.6 mg/dL; intense lymphoplasmacytic infiltrate and fibrosis; >100 IgG4-positive plasma cells; | probable diagnosis | ≥20 |
| Reder (2015) patient 3: [11] | ulcerative lesion of the left pharyngeal wall | rituximab 1 g—2 doses, 2 weeks apart, methylprednisolone 100 mg/day with every rituximab infusion | significant improvement; normalization of IgG4 serum concentration; | proliferative squamous mucosa with a lymphoplasmacytic infiltrate and storiform fibrosis; >50 IgG4-positive plasma cells; | probable diagnosis | ≥20 |
| Khoo (2014) [12] | supraglottic papilli- tumor involving the aryepiglottic folds bilaterally | 37.5 mg prednisolone daily for 6 weeks, then 25 mg for 6 weeks with dose reductions to 5 mg | significant improvement visualized in flexible laryngoscopy in 6 and 12 weeks | serum IgG4 level: 154 mg/dL; dense plasmacytoid infiltrate in the subepithelial tissue with lymphocytes; significant staining with IgG4, in some areas with >50 stained cells per high-power field; IgG4:IgG > 40%, | definite diagnosis | ≥20 |
| Jordan (2018) [15] | surgically absent palatine tonsils, enlarged lingual tonsils, thickened epiglottis and arytenoids, fullness in the piriform sinuses, supraglottis thickening | high-dose steroids and rituximab | stabilization of disease for 18 months; reduction of laryngeal findings | increased number of IgG4- positive cells with IgG/IgG4 ratio of 40% to 50% | probable diagnosis | 7 |
| Syed (2020) [21] | gross inflammation of the epiglottis and vocal cord dysfunction, | (1) azithromycin albuterol inhaler, histamine-2 receptor antagonist, proton pump inhibitor (PPI) (2) rituximab | (1) no effects; (2) resolution of symptoms | IgG4 serum level 29 mg/dL; patient previously diagnosed with IgG4-RD; PET scan showed increased uptake in the larynx and thoracic aorta; | definite diagnosis | ≥20 |
| Hill (2020) [13] | right arytenoid extending into the aryepiglottic fold, limiting the mobility of the right vocal fold | (1) doxycycline; (2) prednisone orally | (1) no effects; (2) resolution of symptoms | IgG4 serum level 133.6 mg/dL, inflammatory infiltrate and an increased plasma cell component | definite diagnosis | ≥20 |
References
- Umehara, H.; Okazaki, K.; Nakamura, T.; Satoh-Nakamura, T.; Nakajima, A.; Kawano, M.; Mimori, T.; Chiba, T. Current approach to the diagnosis of IgG4-related disease—Combination of comprehensive diagnostic and organ-specific criteria. Mod. Rheumatol. 2017, 27, 381–391. [Google Scholar] [CrossRef]
- Stone, J.H.; Zen, Y.; Deshpande, V. IgG4-related disease. N. Engl. J. Med. 2012, 366, 539–551. [Google Scholar] [CrossRef]
- Moura, M.C.; Gripaldo, R.; Baqir, M.; Ryu, J.H. Thoracic Involvement in IgG4-Related Disease. Semin. Respir. Crit. Care Med. 2020, 41, 202–213. [Google Scholar] [CrossRef]
- Stone, J.H.; Khosroshahi, A.; Deshpande, V.; Chan, J.K.C.; Heathcote, J.G.; Aalberse, R.; Azumi, A.; Bloch, D.; Brugge, W.R.; Carruthers, M.N.; et al. Recommendations for the nomenclature of IgG4-related disease and its individual organ system manifestations. Arthritis Care Res. 2012, 64, 3061–3067. [Google Scholar] [CrossRef]
- Ebbo, M.; Daniel, L.; Pavic, M.; Sève, P.; Hamidou, M.; Andres, E.; Burtey, S.; Chiche, L.; Serratrice, J.; Longy-Boursier, M.; et al. IgG4-Related Systemic Disease: Features and treatment response in a French cohort: Results of a multicenter registry. Medicine 2012, 91, 49–56. [Google Scholar] [CrossRef]
- Nair, S.; Nilakantan, A.; Sood, A.; Gupta, A.; Gupta, A. Challenges in the Management of Laryngeal Stenosis. Indian J. Otolaryngol. Head Neck Surg. 2015, 68, 294–299. [Google Scholar] [CrossRef] [Green Version]
- Maughan, E.F.; Michaels, J.; Miller, B.; Weir, J.; Salama, A.; Warner, E.; Ghufoor, K.; Sandhu, G.; Al Yaghchi, C. Primary Immunoglobulin G4-Related Laryngeal Disease: A Case Series and Review of Literature. Clin. Med. Insights Case Rep. 2020, 13, 1179547620960197. [Google Scholar] [CrossRef]
- Matsushima, K.; Ohira, S.; Matsui, H.; Fukuo, A.; Honma, N.; Wada, K.; Matsuura, K. IgG4-related disease with pseudotumor formation in the larynx. Auris Nasus Larynx 2019, 47, 305–308. [Google Scholar] [CrossRef]
- Hamadani, S.; Wang, B.; Gupta, S. P222 IGG4 related disease presenting as post cricoid ulcer of the larynx. Ann. Allergy Asthma Immunol. 2016, 117, S88. [Google Scholar] [CrossRef]
- Ferrante, S.S.; Wang, L.; Kurant, D.; Daniero, J. Laryngeal Immunoglobulin G4-Related Disease Resulting in Severe Airway Obstruction. JAMA Otolaryngol. Neck Surg. 2017, 143, 426–427. [Google Scholar] [CrossRef]
- Reder, L.; Della-Torre, E.; Stone, J.H.; Mori, M.; Song, P. Clinical Manifestations of IgG4-Related Disease in the Pharynx. Ann. Otol. Rhinol. Laryngol. 2014, 124, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Khoo, J.F.; Batt, M.; Stimpson, P.; Safdar, A. Supraglottic immunoglobulin-G4 related plasma cell granuloma: Case report and literature review. Head Neck 2014, 36, E57–E59. [Google Scholar] [CrossRef]
- Hill, R.; Baiyee, D.; Rivero, A. Indolent Laryngeal Mass Causing Progressive Dysphagia. JAMA Otolaryngol. Neck Surg. 2020, 146, 298. [Google Scholar] [CrossRef]
- Syed, A.S.; E Colombo, R.; Syed, B.S.; Henning, P.M. Treatment-resistant cough: A rare manifestation of IgG4-related disease involving the larynx. BMJ Case Rep. 2020, 13, e237614. [Google Scholar] [CrossRef]
- Jordan, V.A.; Hernandez, L.P.H.; Cofer, S.A.; Roby, B.B. Pediatric Laryngeal Expression and Surgical Treatment of IgG4-Related Disease. JAMA Otolaryngol. Neck Surg. 2018, 144, 1183. [Google Scholar] [CrossRef]
- Umehara, H.; Okazaki, K.; Masaki, Y.; Kawano, M.; Yamamoto, M.; Saeki, T.; Matsui, S.; Yoshino, T.; Nakamura, S.; Kawa, S.; et al. Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD), 2011. Mod. Rheumatol. 2012, 22, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Wallace, Z.S.; Naden, F.R.P.; Chari, S.; Choi, H.; Della-Torre, E.; Dicaire, J.; Hart, P.A.; Inoue, M.D.; Khosroshahi, A.; Kubota, K.; et al. The 2019 American College of Rheumatology/European League Against Rheumatism Classification Criteria for IgG4-Related Disease. Arthritis Rheumatol. 2019, 72, 7–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar]
- Wallace, Z.S.; Zhang, Y.; A Perugino, C.; Naden, R.; Choi, H.K.; Stone, J.H. Clinical phenotypes of IgG4-related disease: An analysis of two international cross-sectional cohorts. Ann. Rheum. Dis. 2019, 78, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Völker, H.-U.; Scheich, M.; Zettl, A.; Hagen, R.; Müller-Hermelink, H.K.; Gattenlöhner, S. Laryngeal inflammatory myofibroblastic tumors: Different clinical appearance and histomorphologic presentation of one entity. Head Neck 2009, 32, 1573–1578. [Google Scholar] [CrossRef]
- Kamisawa, T.; Okazaki, K. Diagnosis and Treatment of IgG4-Related Disease. Poxviruses 2016, 401, 19–33. [Google Scholar] [CrossRef]
- Carruthers, M.N.; Khosroshahi, A.; Augustin, T.; Deshpande, V.; Stone, J.H. The diagnostic utility of serum IgG4 concentrations in IgG4-related disease. Ann. Rheum. Dis. 2014, 74, 14–18. [Google Scholar] [CrossRef] [Green Version]
- Peters, R.J.R.; Martin, H.; Virdee, A.; Fryer, E.; Bungay, H.; Rodriguez-Justo, M.; Chouhan, M.; Barnes, E.; Webster, G.; Culver, E.L. Correspondence on ‘The 2019 American College of Rheumatology/European League Against Rheumatism Classification Criteria for IgG4-Related Disease’. Ann. Rheum. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Cheuk, W.; Chan, J.K. Lymphadenopathy of IgG4-related disease: An underdiagnosed and overdiagnosed entity. Semin. Diagn. Pathol. 2012, 29, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Danlos, F.-X.; Rossi, G.M.; Blockmans, D.; Emmi, G.; Kronbichler, A.; Durupt, S.; Maynard, C.; Luca, L.; Garrouste, C.; Lioger, B.; et al. Antineutrophil cytoplasmic antibody-associated vasculitides and IgG4-related disease: A new overlap syndrome. Autoimmun. Rev. 2017, 16, 1036–1043. [Google Scholar] [CrossRef] [PubMed]
- Erden, A.; Bolek, E.C.; Yardimci, K.G.; Kilic, L.; Bilgen, S.A.; Karadag, O. Do ANCA-associated vasculitides and IgG4-related disease really overlap or not? Int. J. Rheum. Dis. 2019, 22, 1926–1932. [Google Scholar] [CrossRef] [PubMed]
- Jennette, J.C.; Falk, R.J.; Bacon, P.A.; Basu, N.; Cid, M.C.; Ferrario, F.; Flores-Suarez, L.F.; Gross, W.L.; Guillevin, L.; Hagen, E.C.; et al. 2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Care Res. 2012, 65, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Bloch, D.A.; Michel, B.A.; Hunder, G.G.; McShane, D.J.; Arend, W.P.; Do, L.H.C.; Edworthy, S.M.; Fauci, A.S.; Fries, J.F.; Leavitt, R.Y.; et al. The American College of Rheumatology 1990 criteria for the classification of vasculitis: Patients and methods. Arthritis Care Res. 1990, 33, 1068–1073. [Google Scholar] [CrossRef] [PubMed]
- Wojciechowska, J.; Krajewski, W.; Krajewski, P.; Kręcicki, T. Granulomatosis with Polyangiitis in Otolaryngologist Practice: A Review of Current Knowledge. Clin. Exp. Otorhinolaryngol. 2016, 9, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Holle, J.U.; Gross, W.L.; Holl-Ulrich, K.; Ambrosch, P.; Noelle, B.; Both, M.; Csernok, E.; Moosig, F.; Schinke, S.; Reinhold-Keller, E. Prospective long-term follow-up of patients with localised Wegener’s granulomatosis: Does it occur as persistent disease stage? Ann. Rheum. Dis. 2010, 69, 1934–1939. [Google Scholar] [CrossRef]
- Knopf, A.; Chaker, A.; Stark, T.; Hofauer, B.; Lahmer, T.; Thürmel, K.; Bas, M. Clinical aspects of granulomatosis with polyangiitis affecting the head and neck. Eur. Arch. Oto-Rhino-Laryngol. 2015, 272, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Al-Ammar, A.Y.; Yasin, S.S.; Al-Muhsen, S.Z.; Al-Saadi, M.M.; Al-Sohaibani, M.O. A laryngeal presentation of Churg--Strauss syndrome in childhood. Ann. Saudi Med. 2009, 29, 142–145. [Google Scholar] [CrossRef] [Green Version]
- Masi, A.T.; Hunder, G.G.; Lie, J.T.; Michel, B.A.; Bloch, D.A.; Arend, W.P.; Do, L.H.C.; Edworthy, S.M.; Fauci, A.S.; Leavitt, R.Y.; et al. The American College of Rheumatology 1990 criteria for the classification of churg-strauss syndrome (allergic granulomatosis and angiitis). Arthritis Care Res. 1990, 33, 1094–1100. [Google Scholar] [CrossRef] [PubMed]
- Suárez, L.F.F.; Alba, M.A.; Tona, G. Severe microscopic polyangiitis with unilateral vocal cord paralysis as initial manifestation. Colomb. Medica 2017, 48, 32–34. [Google Scholar] [CrossRef]
- Greco, A.; De Virgilio, A.; Rizzo, M.I.; Gallo, A.; Magliulo, G.; Fusconi, M.; Ruoppolo, G.; Tombolini, M.; Turchetta, R.; de Vincentiis, M. Microscopic polyangiitis: Advances in diagnostic and therapeutic approaches. Autoimmun. Rev. 2015, 14, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.Y.; Keogh, K.A.; Lewis, J.E.; Ryu, J.H.; Cornell, L.D.; Garrity, J.A.; Yi, E.S. IgG4-positive plasma cells in granulomatosis with polyangiitis (Wegener’s): A clinicopathologic and immunohistochemical study on 43 granulomatosis with polyangiitis and 20 control cases. Hum. Pathol. 2013, 44, 2432–2437. [Google Scholar] [CrossRef] [PubMed]
- Drobysheva, A.; Fuller, J.; Pfeifer, C.M.; Rakheja, D. Orbital Granulomatosis with Polyangiitis Mimicking IgG4-Related Disease in a 12-Year-Old Male. Int. J. Surg. Pathol. 2018, 26, 453–458. [Google Scholar] [CrossRef]
- Hamano, H.; Kawa, S.; Horiuchi, A.; Unno, H.; Furuya, N.; Akamatsu, T.; Fukushima, M.; Nikaido, T.; Nakayama, K.; Usuda, N.; et al. High Serum IgG4 Concentrations in Patients with Sclerosing Pancreatitis. N. Engl. J. Med. 2001, 344, 732–738. [Google Scholar] [CrossRef]
- Ebbo, M.; Grados, A.; Bernit, E.; Vély, F.; Boucraut, J.; Harlé, J.-R.; Daniel, L.; Schleinitz, N. Pathologies Associated with Serum IgG4 Elevation. Int. J. Rheumatol. 2012, 2012, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Deshpande, V.; Zen, Y.; Chan, J.K.; E Yi, E.; Sato, Y.; Yoshino, T.; Klöppel, G.; Heathcote, J.G.; Khosroshahi, A.; A Ferry, J.; et al. Consensus statement on the pathology of IgG4-related disease. Mod. Pathol. 2012, 25, 1181–1192. [Google Scholar] [CrossRef] [Green Version]
- Yates, M.; A Watts, R.; Bajema, I.M.; Cid, M.C.; Crestani, B.; Hauser, T.; Hellmich, B.; Holle, J.U.; Laudien, M.; Little, M.; et al. EULAR/ERA-EDTA recommendations for the management of ANCA-associated vasculitis. Ann. Rheum. Dis. 2016, 75, 1583–1594. [Google Scholar] [CrossRef] [Green Version]
- Faz-Muñoz, D.; Hinojosa-Azaola, A.; Mejía-Vilet, J.M.; Uribe-Uribe, N.O.; Rull-Gabayet, M.; Muñoz-Castañeda, W.R.; Vargas-Parra, N.J.; Martín-Nares, E. ANCA-associated vasculitis and IgG4-related disease overlap syndrome: A case report and literature review. Immunol. Res. 2022, 70, 550–559. [Google Scholar] [CrossRef] [PubMed]
- Yunyun, F.; Yu, C.; Panpan, Z.; Hua, C.; Di, W.; Lidan, Z.; Linyi, P.; Li, W.; Qingjun, W.; Xuan, Z.; et al. Efficacy of Cyclophosphamide treatment for immunoglobulin G4-related disease with addition of glucocorticoids. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Colliard, A.; Ishii, A.; De Sandre, C.; Gorostidi, F.; Sandu, K. Decoding supraglottic stenosis. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Krishna, P.D.; Malone, J.P. Isolated adult supraglottic stenosis: Surgical treatment and possible etiologies. Am. J. Otolaryngol. 2006, 27, 355–357. [Google Scholar] [CrossRef]
- Gallo, A.; Pagliuca, G.; Greco, A.; Martellucci, S.; Mascelli, A.; Fusconi, M.; De Vincentiis, M. Laryngotracheal stenosis treated with multiple surgeries: Experience, results and prognostic factors in 70 patients. Acta Otorhinolaryngol. Ital. Organo Uff. Soc. Ital. Otorinolaringol. Chir. Cerv.-Facc. 2012. [Google Scholar]
- Herrington, H.C.; Weber, S.M.; Andersen, P.E. Modern Management of Laryngotracheal Stenosis. Laryngoscope 2006, 116, 1553–1557. [Google Scholar] [CrossRef] [PubMed]
- Stevens, M.S.; Chang, A.; Simpson, C.B. Supraglottic Stenosis: Etiology and Treatment of a Rare Condition. Ann. Otol. Rhinol. Laryngol. 2013, 122, 205–209. [Google Scholar] [CrossRef]
- Daniero, J.J. Expanding perspectives in airway stenosis. JAMA Otolaryngol. Head Neck Surg. 2017, 143, 505–506. [Google Scholar] [CrossRef] [PubMed]






| Study | Sex, Age | Symptoms | Co-Morbidities | Disease Location | Endoscopic Examination | Treatment/Intervention | Outcome | IgG4 Serum Level and Histopathology | Comprehensive Criteria | EULAR Criteria |
|---|---|---|---|---|---|---|---|---|---|---|
| Patient L.G.—current case | F, 72 | dyspnea at rest, cough, globus symptoms | hypothyroidism, glaucoma | supraglottic region | laryngeal inlet narrowing; hypertrophy; limited mobility of vocal folds | (1) methotrexate changed to azathioprine; prednisone; (2) cyclophosphamide; methylprednisolone | (1) poor toleration of methotrexate; stenosis progressed; (2) significant improvement | SL > 135 mg/dL; IgG4 in 50% of mononuclear cells | D | 15 |
| Matsushima (2019) [8] | M, 50 | dyspnea; snoring | cerebral infarction, retroperitoneal fibrosis | left arytenoid region | diffuse swelling | (1) CO2 laser resection and tracheostomy; (2) prednisolone | 1 and 2: improvement | SL 31 mg/dL; storiform fibrosis; >100 IgG4+ plasma cells; 50% IgG4:IgG | P | ≥20 |
| Maughan (2020) patient 1: [7] | F, 52 | dyspnea; biphasic stridor | not reported | supraglottic, region | visible fibrosis | (1) balloon dilatation, excision, steroids; (2) prednisolone, azathioprine changed to methotrexate; (3) laryngotracheal reconstruction | transient relief after 1 and 2; (3) improvement | SL—normal; lymphoplasmocytic infiltrate, fibrosis, IgG4:IgG 80% | P | ≥20 |
| Maughan (2020) patient 2: [7] | M, 76 | dysphagia, dysphonia | asbestos exposure, hypothyroidism, gastritis, H. pylori infection | supraglottic region | swelling | (1) balloon dilatation, laser excision, steroids; (2) immunomodulatory treatment | (1) repeated every 4–6 months (2) improvement | SL—normal; lymphoid infiltrate, plasma cells, 20% IgG4+ cells (50 IgG+ in HPF); | P | 4 |
| Maughan (2020) patient 3: [7] | M, 49 | dysphonia; inspratory stridor | GI reflux, allergic rhinitis | supraglottic region | scarring, restricted arytenoid movement bilaterally | (1) balloon dilatation, laser excision, steroid injections; (2) prednisolone | (1) repeated dilatations; (2) follow up not described | SL—0.9 range; inflammation, fibrosis, ANCA- negative; | P | 13 |
| Hamadani (2016) [9] | F, 54 | dysphagia, odynophagia, weight loss; dysphonia; | rheumatoid arthritis, liver cirrhosis, portal hypertension, | supraglottic, postcricoid region | visible mucus, postcricoid ulcer, laryngospasm | not described | not described | IgG lymphocytoid plasma-cell infiltrates, >90% IgG+ plasma cells | P | 8 |
| Ferrante (2017) [10] | F, 70 | stridor, dyspnea at rest, dysphonia, dysphagia | Sjögren’s syndrome, rheumatoid arthritis, Felty syndrome, COPD | supraglottic region; nasopharynx; | anterior septal perforation, nasal wall scarring, supraglottic stenosis | tracheostomy; prednisolone | slow improvement; decannulation after 16 months | 40 IgG4 plasma cells HPF, storiform fibrosis, lymphoplasmatic mucositis | P | ≥20 |
| Reder (2015) patient 1: [11] | M, 58 | throat discomfort, dysphonia | semicircular canal dehiscence | supraglottis, right vocal process, aryepiglottic fold | visible lesions | (1) laser excision; (2) prednisolone; (3) rituximab, methylprednisolone | (1) no long-term improvement; (2) poor toleration; (3) remission | Sl—196 mg/dL; storiform fibrosis, lymphoplasmacytic infiltrate; 50 IgG4+ cells per HPF; IgG4:IgG > 0.50; | D | ≥20 |
| Reder (2015) patient 2: [11] | M, 62 | cough, dysphagia, dysphonia | primary scleros- ing cholangitis, ulcerative colitis, and colorectal cancer | supraglottic region | granular mucosa, keratosis, hyperplasia | (1) prednisone; (2) rituximab, methylprednisolone | (1) “modest” clinical improvement; (2) significant improvement | SL—28.6 mg/dL; lymphoplasmacytic infiltrate and fibrosis; >100 IgG4+ cells; | P | ≥20 |
| Reder (2015) patient 3: [11] | F, 50 | throat discomfort | hypertension and GI reflux disease | supraglottic region | ulcerative lesion of the left pharyngeal wall | Rituximab, methylprednisolone | significant improvement; normalization of IgG4 serum concentration; | lymphoplasmacytic infiltrate, storiform fibrosis; >50 IgG4+ plasma cells; | P | ≥20 |
| Khoo (2014) [12] | M, 62 | cough, dysphagia, odynophagia, dysphonia, otalgia, | not reported | supraglottic region, aryepiglottic folds | supraglottic papilli- tumor involving the aryepiglottic folds bilaterally | prednisolone | significant improvement visualized in flexible laryngoscopy at 6 and 12 weeks | SL—154 mg/dL; plasmacytoid infiltrate; >50 IgG4+ cells per HPF; IgG4:IgG > 40%, | D | ≥20 |
| Jordan (2018) [15] | F, pediatric patient | dysphonia, globus symptoms, dysphagia | patient without comorbidities | epiglottis, arytenoids | thickening of tissues | rituximab, high-dose steroids | stabilization of disease for 18 months; reduction of laryngeal findings | increased number of IgG4+ cells with IgG:IgG4 40% to 50% | P | 7 |
| Syed (2020) [14] | M, 69 | cough, dysphonia and dyspnea | multivessel coronary artery disease, lacunar cerebrovascular accident, hypertension, hyperlipidemia, benign prostatic hyperplasia | lacrimal gland, pancreas, epiglottis, vocal cord | epiglottic inflammation, vocal cord dysfunction, | (1) azithromycin, albuterol, histamine-2 receptor antagonist, PPI; (2) rituximab | (1) no effects; (2) improvement | SL—29 mg/dL; previous IgG4-RD diagnosis | D | ≥20 |
| Hill (2020) [13] | M, 29 | odynophagia, dysphonia, dysphagia | reactive airway disease | arytenoid, aryepiglottic fold | limited mobility of the vocal fold | (1) doxycycline; (2) prednisone | (1) no effects; (2) improvement | Sl—133.6 mg/dL, inflammatory infiltrate, increased plasma cell component | D | ≥20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barańska, M.; Makowska, J.; Wągrowska-Danilewicz, M.; Pietruszewska, W. Supraglottic Localization of IgG4-Related Disease—Rare and Challenging Equity. J. Pers. Med. 2022, 12, 1223. https://doi.org/10.3390/jpm12081223
Barańska M, Makowska J, Wągrowska-Danilewicz M, Pietruszewska W. Supraglottic Localization of IgG4-Related Disease—Rare and Challenging Equity. Journal of Personalized Medicine. 2022; 12(8):1223. https://doi.org/10.3390/jpm12081223
Chicago/Turabian StyleBarańska, Magda, Joanna Makowska, Małgorzata Wągrowska-Danilewicz, and Wioletta Pietruszewska. 2022. "Supraglottic Localization of IgG4-Related Disease—Rare and Challenging Equity" Journal of Personalized Medicine 12, no. 8: 1223. https://doi.org/10.3390/jpm12081223