
Clinical Markers of Need for Surgery in Orbital Complication of Acute Rhinosinusitis in Children: Overview and Systematic Review
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
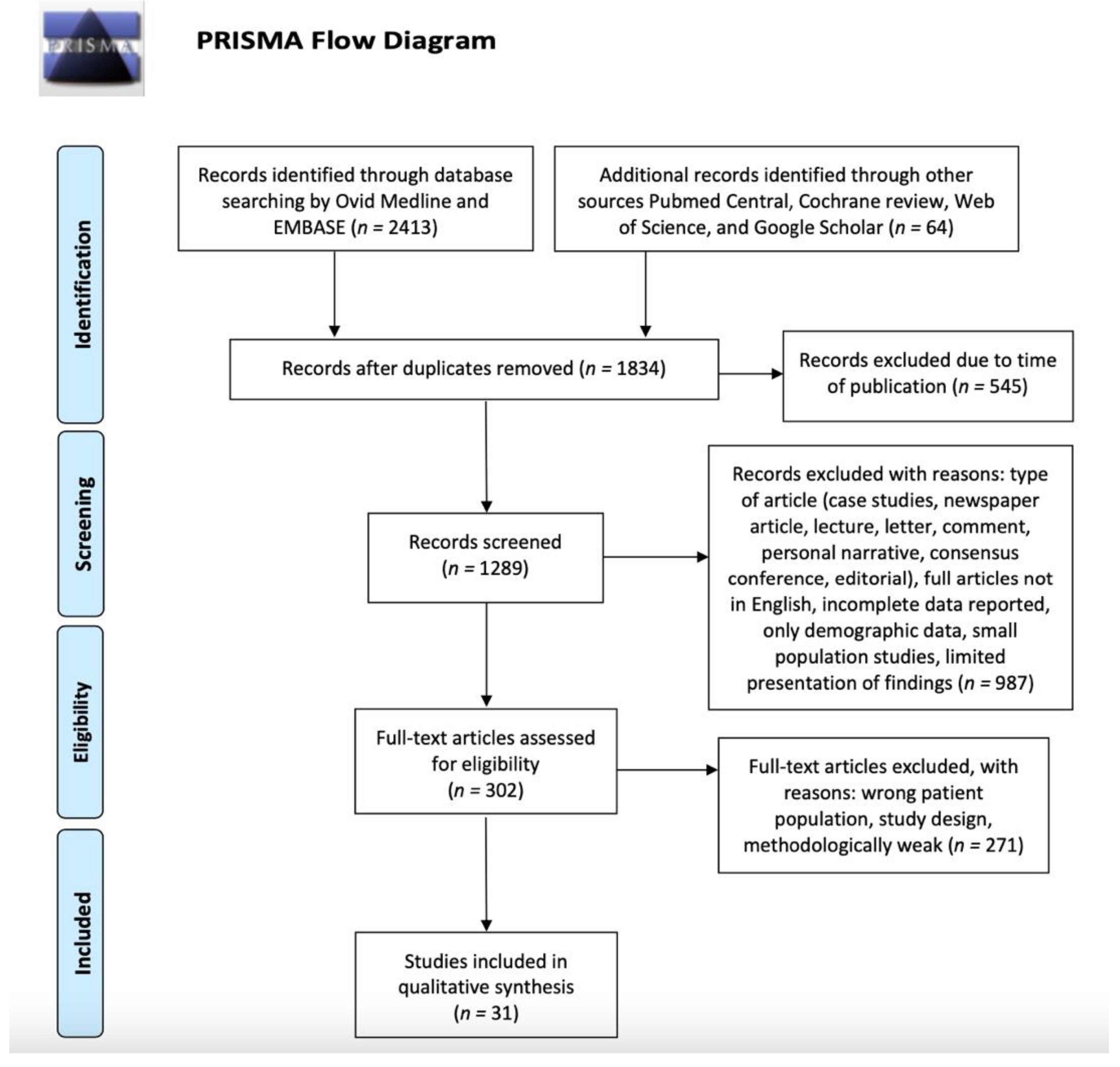
2.1. Search Strategy
2.2. Study Selection
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gill, P.J.; Parkin, P.C.; Begu, N.; Drouin, O.; Foulds, J.; Pound, C.; Quet, J.; Vomiero, G.; Wahi, G.; Sakran, M.; et al. Care and outcomes of Canadian children hospitalised with periorbital and orbital cellulitis: Protocol for a multicentre, retrospective cohort study. BMJ Open 2019, 12, e035206. [Google Scholar] [CrossRef] [PubMed]
- Sciarretta, V.; Demattè, M.; Farneti, P.; Fornaciari, M.; Corsini, I.; Piccin, O.; Saggese, D.; Fernandez, I.J. Management of orbital cellulitis and subperiosteal orbital abscess in pediatric patients: A ten-year review. Int. J. Pediatr. Otorhinolaryngol. 2017, 96, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Jabarin, B.; Eviatar, E.; Israel, O.; Maro, T.; Gavriel, H. Indicators for imaging in periorbital cellulitis secondary to rhinosinusitis. Eur. Arch. Otorhinolaryngol. 2018, 4, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Mahalingam, S.; Hone, R.; Lloyd, G.; Grounds, R.; Shamil, E.; Wong, G.; Al-Lami, A.; Pervez, A.; Rudd, J.; Poon, J.S.; et al. The management of periorbital cellulitis secondary to sinonasal infection: A multicenter prospective study in the United Kingdom. Int. Forum Allergy Rhinol. 2020, 10, 726–737. [Google Scholar] [CrossRef] [PubMed]
- Sedaghat, A.R.; Wilke, C.O.; Cunningham, M.J.; Ishman, S.L. Socioeconomic disparities in the presentation of acute bacterial sinusitis complications in children. Laryngoscope 2014, 124, 1700–1706. [Google Scholar] [CrossRef]
- Villwock, M.R.; Villwock, J.A. Incidence and extent of sinus procedures in treatment of pediatric orbital cellulitis. Int. J. Pediatr. Otorhinolaryngol. 2020, 135, 110086. [Google Scholar] [CrossRef]
- McDermott, S.M.; Onwuka, A.; Elmaraghy, C.; Walz, P.C. Management Patterns in Pediatric Complicated Sinusitis. Otolaryngol. Head Neck Surg. 2020, 4, 814–821. [Google Scholar] [CrossRef]
- Chrobok, V.; Pellant, A.; Mandysová, P.; Mejzlík, J.; Dědková, J.; Čelakovský, P. Rhinogenic Orbital Inflammation—What Has Changed over the Past 50 Years? Acta Med. 2019, 3, 94–98. [Google Scholar] [CrossRef]
- Cohen, N.; Erisson, S.; Anafy, A.; Palnizky-Soffer, G.; Cohen, E.; Capua, C.; Rimon, A.; Grisaru-Soen, G. Clinicians need to consider surgery when presented with some markers for severe paediatric orbital cellulitis. Acta Paediatr. 2020, 109, 1269–1270. [Google Scholar] [CrossRef]
- Dennison, S.H.; Hertting, O.; Bennet, R.; Eriksson, M.; Holmström, M.; Schollin Ask, L.; Lindstrand, A.; Dimitriou, P.; Stjärne, P.; Granath, A. A Swedish population-based study of complications due to acute rhinosinusitis in children 5–18 years old. Int. J. Pediatr. Otorhinolaryngol. 2021, 150, 110866. [Google Scholar] [CrossRef]
- Quintanilla-Dieck, L.; Chinnadurai, S.; Goudy, S.L.; Virgin, F.W. Characteristics of superior orbital subperiosteal abscesses in children. Laryngoscope 2017, 27, 735–740. [Google Scholar] [CrossRef] [PubMed]
- Chandler, J.R.; Langenbrunner, D.J.; Stevens, E.R. The pathogenesis of orbital complications in acute sinusitis. Laryngoscope 1970, 80, 1414–1428. [Google Scholar] [CrossRef] [PubMed]
- Jiramongkolchai, P.; Lander, D.P.; Kallogjeri, D.; Olsen, M.A.; Keller, M.; Schneider, J.S.; Lee, J.J.; Jiramongkolchai, K.; Piccirillo, J.F. Trend of surgery for orbital cellulitis: An analysis of state inpatient databases. Laryngoscope 2020, 130, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Bedwell, J.; Bauman, N.M. Management of pediatric orbital cellulitis and abscess. Curr. Opin. Otolaryngol. Head Neck Surg. 2011, 19, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; the PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Lahmini, W.; Oumou, M.; Bourrous, M. Management of periorbital cellulitis at the Pediatric Emergency Department: A ten years study. J. Français D’ophtalmol. 2022, 45, 166–172. [Google Scholar] [CrossRef]
- Presutti, L.; Lucidi, D.; Spagnolo, F.; Molinari, G.; Piccinini, S.; Alican-dri-Ciufelli, M. Surgical multidisciplinary approach of orbital complications of sinonasal inflammatory disorders. Acta Otorhinolaryngol. Ital. 2021, 41, S108–S115. [Google Scholar] [CrossRef]
- Bülbül, L.; Sağlam, N.O.; Elitok, G.K.; Yazici, Z.M.; Hatipoglu, N.; Hatipoğlu, S.; Palabiyik, F.B.; Yigit, U.; Demir, M.; Bülbül, A. Preseptal and Orbital Cellulitis: Analysis of Clinical, Laboratory and Imaging Findings of 123 Pediatric Cases from Turkey. Pediatr. Infect. Dis. J. 2022, 41, 97–101. [Google Scholar] [CrossRef]
- Turhal, G.; Göde, S.; Sezgin, B.; Kaya, I.; Bozan, A.; Midilli, R.; Karcı, B. Orbital complications of pediatric rhinosinusitis: A single institution report. Turk. J. Pediatrics 2020, 62, 533–540. [Google Scholar] [CrossRef]
- Mabrouk, A.B.; Wannes, S.; Hasnaoui, M.; Werdani, A.; Hamida, N.B.; Jerbi, S.; Driss, N.; Mahjoub, B. Orbital complication of acute ethmoiditis: A Tunisian paediatric cross sectional study. Am. J. Otolaryngol. 2020, 41, 102320. [Google Scholar] [CrossRef]
- Santos, J.C.; Pinto, S.; Ferreira, S.; Maia, C.; Alves, S.; da Silva, V. Pediatric preseptal and orbital cellulitis: A 10-year experience. Int. J. Pediatr. Otorhinolaryngol. 2019, 120, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Tzelnick, S.; Soudry, E.; Raveh, E.; Gilony, D. Recurrent periorbital cellulitis associated with rhinosinusitis in children: Characteristics, course of disease, and management paradigm. Pediatr. Otorhinolaryngol. 2019, 121, 26–28. [Google Scholar] [CrossRef] [PubMed]
- Sansa-Perna, A.; Gras-Cabrerizo, J.R.; Montserrat-Gili, J.R. Our experience in the management of orbital complications in acute rhinosinusitis. Acta Otorrinolaringol. 2020, 71, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Hultman Dennison, S.; Schollin Ask, L.; Eriksson, M.; Granath, A.; Hertting, O.; Bennet, R.; Lindstrand, A.; Masaba, P.; Dimitriou, P.; Stjärne, P. Serious complications due to acute rhinosinusitis in children up to five years old in Stockholm, Sweden—Still a challenge in the pneumococcal conjugate vaccine era. Int. J. Pediatr. Otorhinolaryngol. 2019, 121, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Schollin Ask, L.; Hultman Dennison, S.; Stjärne, P.; Granath, A.; Srivastava, S.; Eriksson, M.; Lindstrand, A.; Ryd Rinder, M. Most preschool children hospitalised for acute rhinosinusitis had orbital complications, more common in the youngest and among boys. Acta Paediatr. 2017, 106, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Wan, Y.; Shi, G.; Wang, H. Treatment of Orbital Complications Following Acute Rhinosinusitis in Children. Balkan Med. J. 2016, 33, 401–406. [Google Scholar] [CrossRef]
- Rudloe, T.F.; Harper, M.B.; Prabhu, S.P.; Rahbar, R.; Vanderveen, D.; Kimia, A.A. Acute periorbital infections: Who needs emergent imaging? Pediatrics 2010, 125, e719–e726. [Google Scholar] [CrossRef]
- Deutschmann, M.W.; Livingstone, D.; Cho, J.J.; Vanderkooi, O.G.; Brookes, J.T. The significance of Streptococcus anginosus group in intracranial complications of pediatric rhinosinusitis. JAMA Otolaryngol. Head Neck Surg. 2013, 139, 157–160. [Google Scholar] [CrossRef]
- Todman, M.S.; Enzer, Y.R. Medical management versus surgical intervention of pediatric orbital cellulitis: The importance of subperiosteal abscess volume as a new criterion. Ophthalmic Plast. Reconstr. Surg. 2011, 27, 255–259. [Google Scholar] [CrossRef]
- McCoy, J.L.; Dixit, R.; Dohar, J.E.; Tobey, A.B.J. Pediatric subperiosteal orbital abscess characterization and prediction of size, location, and management. Pediatr. Otorhinolaryngol. 2021, 144, 110693. [Google Scholar] [CrossRef]
- Torretta, S.; Guastella, C.; Marchisio, P.; Marom, T.; Bosis, S.; Ibba, T.; Drago, L.; Pignataro, L. Sinonasal-Related Orbital Infections in Children: A Clinical and Therapeutic Overview. J. Clin. Med. 2019, 8, 101. [Google Scholar] [CrossRef] [PubMed]
- Rahbar, R.; Robson, C.D.; Petersen, R.A.; DiCanzio, J.; Rosbe, K.W.; McGill, T.J.; Healy, G.B. Management of orbital subperiosteal abscess in children. Arch. Otolaryngol. Head Neck Surg. 2001, 127, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Sorotzky, M.; Shahar-Nissan, K.; Shack, A.R.; Berant, R.; Weiser, G.; Berliner, E.; Heiman, E. Management of intraorbital infections in the pediatric emergency department. Eur. J. Pediatr. 2022, 181, 2741–2746. [Google Scholar] [CrossRef] [PubMed]
- Tritt, A.; Kay-Rivest, E.; Paradis, T.; Duval, M. Daily outpatient intravenous antibiotic therapy for the management of paediatric periorbital cellulitis, a retrospective case series. Clin. Otolaryngol. 2019, 44, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Shifman, N.T.; Krause, I.; Dotan, G.; Gilony, D.; Bilavsky, E. Orbital Cellulitis in a Pediatric Population—Experience from a Tertiary Center. Indian. Pediatr. 2022, 59, 35–37. [Google Scholar] [CrossRef] [PubMed]
- Anosike, B.I.; Ganapathy, V.; Nakamura, M.M. Epidemiology and Management of Orbital Cellulitis in Children. J. Pediatric Infect. Dis. Soc. 2022, 11, 214–220. [Google Scholar] [CrossRef]
- Cürebal, B.; Şahin, A.; Dalgıç, N. Preseptal Cellulitis in Children: A Single-Center Experience. SiSli Etfal Häst. Tip Bulteni/Med Bull. Sisli Hosp. 2019, 53, 409–412. [Google Scholar] [CrossRef]
- Martins, M.; Martins, S.P.; Pinto-Moura, C.; Leal, V.; Spratley, J. Management of post-septal complications of acute rhinosinuitis in children: A 14-year experience in a tertiary hospital. Int. J. Pediatr. Otorhinolaryngol. 2021, 151, 110925. [Google Scholar] [CrossRef]
- Gavriel, H.; Yeheskeli, E.; Aviram, E.; Yehoshua, L.; Eviatar, E. Dimension of Subperiosteal Orbital Abscess as an Indication for Surgical Management in Children. Otolaryngol.-Head Neck Surg. 2011, 145, 823–827. [Google Scholar] [CrossRef]


{kind=link}
| Authors (Years) | Type of Study | Patients (n) | Methods | Results | Clinical Markers of Need for Surgery |
|---|---|---|---|---|---|
| Choen, 2019 [9] | RCS | 76 | 2 groups (<9/>9 years) and treatment strategy. | Conservative treatment of just antibiotics was administered to 76% of the cohort, with abscess drainage for the remainder. | Impaired vision, ophthalmoplegia, >9 years, no pansinusitis, proptosis, air bubbles in the subperiosteal space or in the intraconal space, elevated CRP, and hemodynamic compromise. |
| Bülbül, 2022 [18] | R | 123 | Findings of preseptal and orbital cellulitis groups were compared. The risk factors for the development of orbital involvement were analyzed. | Rhinosinusitis was the most common predisposing factor in the development of preseptal cellulitis and orbital cellulitis. Orbital involvement was present in 9.8% of the patients. | High CRP value could be used to predict orbital involvement. |
| Chrobok, 2019 [8] | R | 292 | Patients treated before functional endonasal surgery vs. patients treated by functional endonasal surgery as standard surgical method. | Most patients were treated conservatively; surgery was indicated in 1/3. Endoscopic endonasal approach. | SPOA and OA, impaired visual acuity, progression of local and systemic signs and symptoms despite adequate conservative management for more than 24 h, or no local improvement after 48/72 h of antibiotic therapy. |
| Quintanilla-Dieck, 2016 [11] | RCS | 52 |
Imaging characteristics and treatment between superior and medial subperiosteal abscess |
Superior subperiosteal abscess may present with more advanced disease, leading to a higher rate of characteristics such as proptosis, hypoglobus, and intraorbital air. |
SPOA with proptosis, hypoglobus, and intraorbital air factors predispose to surgical drainage. Abscess volume is the most predictive of surgery (>0.67 mL). |
| Jiramongkolchai, 2020 [13] | R | 10,148 children and adults | Trend of surgery over time and patient- and hospital-level factors associated with surgery from state inpatient databases | 13% of children admitted for orbital cellulitis underwent surgery | >9 years, ophthalmologic comorbidities, and conjunctival edema |
| McDermot, 2020 [7] | Case series with charts review | 168 | Demographics, disease characteristics, in-hospital management, and outcomes were recorded and analyzed | 49% surgery and 36% medical therapy followed by surgery. 83% of Chandler III received surgery | Chandler III and SPOA |
| Sciarretta, 2017 [2] | R | 57 | Data collection | Medical management was the main treatment for both preseptal and postseptal OC | SPOA |
| Thural, 2017 [19] | R | 55 | Data collection | Hospitalization in SPOA was higher than PSC. Conservative therapy was an effective method for PSC and most cases of OC | Nonresponsive to medical treatment within 48 h, ophthalmoplegia, and reduction in the visual acuity. |
| Mabrouk, 2020 [20] | CSS | 39 | Chandler I and II vs. Chandler III, IV, and V subgroups | Fever, exophthalmos, ophthalmoplegia, positive CRP, age, and white blood cells count were not associated with more severe lesions in the CT scan. | Orbital abscess |
| Caldeira Santos, 2019 [21] | R | 122 | Data collection | Fever, photophobia, ocular pain, painful eye movements, proptosis, rhinorrhea, and vison impairment were related with OC. Leukocytosis was present in 34.4% with OC. | Visual acuity, grade of proptosis, limitation and pain with eye movements, pupillary reflex, and neurologic exam. |
| Tzelnick, 2019 [22] | R | 14 | Data collection | Patients responded well to intravenous antibiotics, both during the primary and recurrent events. Surgery in patients failing conservative treatment or presenting with abscess formation. | Patients failing conservative treatment or presenting with abscess formation |
| Sansa-Perna, 2020 [23] | R | 21 children and adults | Data collection | A CT scan was performed in all patients and the cases of subperiosteal or orbital abscess were treated surgically | Subperiosteal or orbital abscesses |
| Dennison 2019 [24] | R | 215 | Data collection | Postseptal OC occurred in 29 cases (13.5%) and surgery was necessary in 9 (4.2%). | Orbital complications |
| Ask, 2016 [25] | R | 213 | Data collection | CT scans were performed to deterioration of, or lack of improvement of status and/or symptoms and severity of the symptoms | CT verified postseptal complications and only one child needed surgery. |
| Wan, 2016 [26] | R | 31 | Data collection | 16 patients were cured by conservative therapy and 15 patients by ESS. | No improvement after 48 h, orbital SPA, motility disorders of eyeball, or decreased vision |
| Rudloe, 2010 [27] | R | 918 | Data collection | Proptosis and/or pain or limitation of extraocular movements were at high risk for intraorbital abscesses, yet many did not have these predictors. | Orbital abscess, absolute neutrophil count—ANC of 10,000 cells/L, periorbital Edema, <3 years, previous antibiotic use, and Chandler III score or higher |
| Deutschman, 2013 [28] | RCS | 50 |
medical records identified patients |
Infection by the S. Anginosus were more severe and likely to require neurosurgical intervention with development of long-term neurologic deficits. | S. Anginosus infection |
| Todmann, 2011 [29] | R | 29 | Chart review |
27.6% surgery and 72.4% medical therapy. The mean volume of abscesses needing surgery were larger. | Multiple foci of bacteria, >9 years, immunodeficiency, no improvement > 48 h after parenteral antibiotic treatment, SPA, and orbital cellulitis |
| McCoy, 2012 [30] | R | 108 | Data collection | With an abscess volume of 0.510 cm3, there was a sensitivity of 71.2% and a specificity of 84.4% for needing surgical drainage | Abscess size of 0.510 cm3 or larger |
| Rahbar, 2001 [32] | R | 19 | CT scans were reviewed | Probability of surgery was 92% for 2 mm of proptosis | Proptosis |
| Sorotzki, 2022 [33] | RCS | 95 | CT timing and results | Having three or more high-risk presenting symptoms was associated with a greater likelihood of surgical intervention | Number and severity of presenting complaints |
| Tritt, 2018 [34] | R | 66 |
Number of days of intravenous antibiotics, complications, and need for admission. | 2 children developed complications and one child underwent surgery. | Phlegmon and cellulitis despite intravenous antibiotics |
| Shifman, 2022 [35] | R | 94 | Clinical, laboratory and radiology characteristics, management, microbiological data, and outcomes were collected. | Children aged older than 9 years presented with markedly elevated inflammatory markers, i.e., leukocytosis and CRP. | Severe ocular presentation |
| Anosike, 2022 [36] | RCS | 220 | charts for demographic characteristics, clinical features, management, and outcomes | Although MRSA was rare, empiric vancomycin use was high. Treatment failure was uncommon in patients who received ≤ 2 weeks of therapy, suggesting that shorter durations are adequate in some patients. | >5 years of age proptosis, diplopia, or an SPOA ≥ 20 mm. |
| Villwock, 2020 [6] | KID | 15,260 | Frequency of sinus procedures in relation to pediatric age cohort were noted (<8 years vs. 9–20 years). | Sinus surgery in 7.2% of cases—with patients over 8 years having a 2.8-fold increase compared to younger patients. | Presence of cellulitis/abscess of the face was the strongest predictor of multiple sinus procedures |
| Jabarin, 2018 [3] | RCS | 123 | Age, gender, symptoms, physical findings, white blood, CRP levels, CT findings, treatment before and during admission, and surgical treatment | 53 had SPOA | Proptosis and ophthalmoplegia, higher neutrophil count, older age, and a malignant disease progression necessitating broad-spectrum antibiotic use are reliable predictors of an orbital abscess. |
| Dannison, 2021 [10] | RCS | 310 | Age, gender, date of admittance, presence of redness and/or swelling around the eye, maximum CRP level, WBC, radiology results, surgery, and number of days with IV antibiotics. | 1.3 surgeries per 100,000 per year. The percentage of admitted children that had surgery increased with age. | Not found |
| Cürebal, 2019 [37] | R | 29 | Age, gender, length of hospitalization, admission complaint, clinical features, complete blood count, CRP, radiology findings, blood culture results, antibiotic use and duration, and prognosis. | An accurate clinical approach and rapid treatment can prevent the spread of infection and avoid serious complications. | Orbital involvement, such as pain in eye movements, and proptosis. |
| Mahalingam, 2020 [4] | P | 143 children and adults | Data collection | 16.7% of children required surgery; ceftriaxone–metronidazole was associated with reduction in N of patients requiring surgery. | Chandler III and IV |
| Martins, 2021 [38] | R | 55 | Data collection | 60% was treated medically and 40% required surgery. 12.73% developed complications. Higher ANC was found in patients with subperiosteal abscess. | Not found |
| Gavriel, 2011 [39] | R | 95 | Clinical and radiological parameters | Statistically significant larger abscesses in the surgically treated group were noted | Significant or progressing ocular findings, failure to improve after 48 h of medical therapy, together with an abscess volume of more than 0.5 mL, a length greater than 17 mm, and a width greater than 4.5 mm, should be strongly considered to have surgical drainage. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cantone, E.; Piro, E.; De Corso, E.; Di Nola, C.; Settimi, S.; Grimaldi, G.; Motta, G. Clinical Markers of Need for Surgery in Orbital Complication of Acute Rhinosinusitis in Children: Overview and Systematic Review. J. Pers. Med. 2022, 12, 1527. https://doi.org/10.3390/jpm12091527
Cantone E, Piro E, De Corso E, Di Nola C, Settimi S, Grimaldi G, Motta G. Clinical Markers of Need for Surgery in Orbital Complication of Acute Rhinosinusitis in Children: Overview and Systematic Review. Journal of Personalized Medicine. 2022; 12(9):1527. https://doi.org/10.3390/jpm12091527
Chicago/Turabian StyleCantone, Elena, Eva Piro, Eugenio De Corso, Claudio Di Nola, Stefano Settimi, Giusi Grimaldi, and Gaetano Motta. 2022. "Clinical Markers of Need for Surgery in Orbital Complication of Acute Rhinosinusitis in Children: Overview and Systematic Review" Journal of Personalized Medicine 12, no. 9: 1527. https://doi.org/10.3390/jpm12091527