

Patient-Specific Image-Based Computational Fluid Dynamics Analysis of Abdominal Aorta and Branches

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
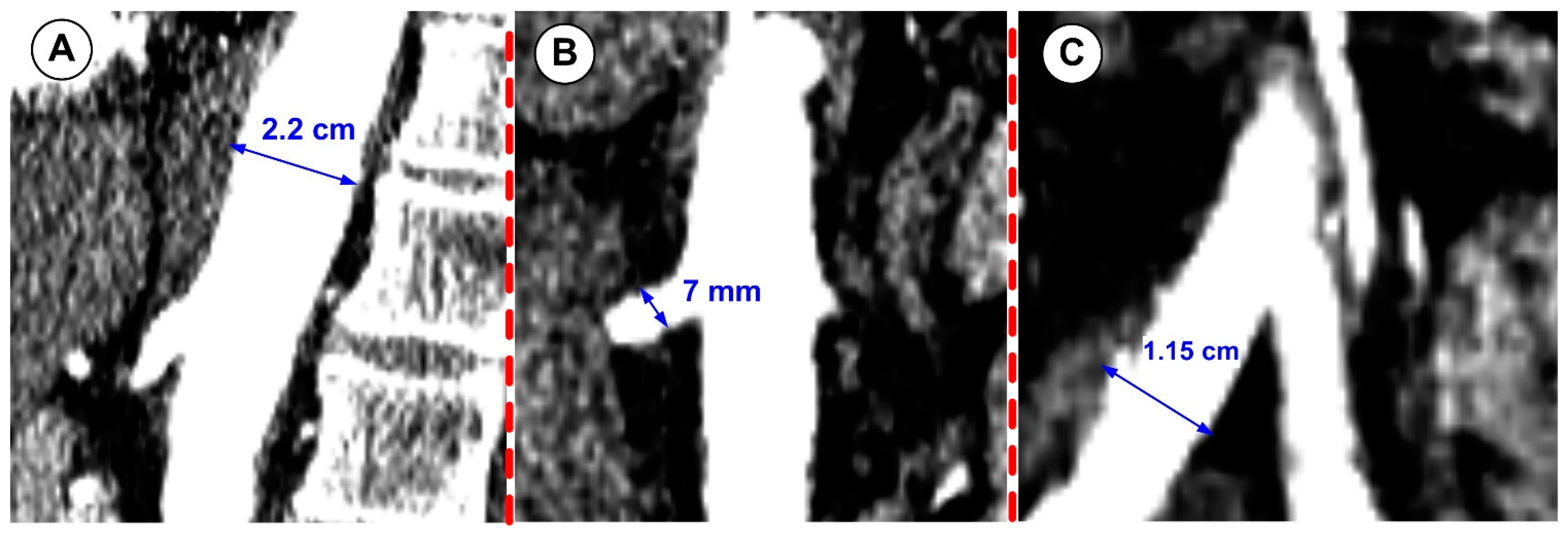
2.1. Image Acquisition
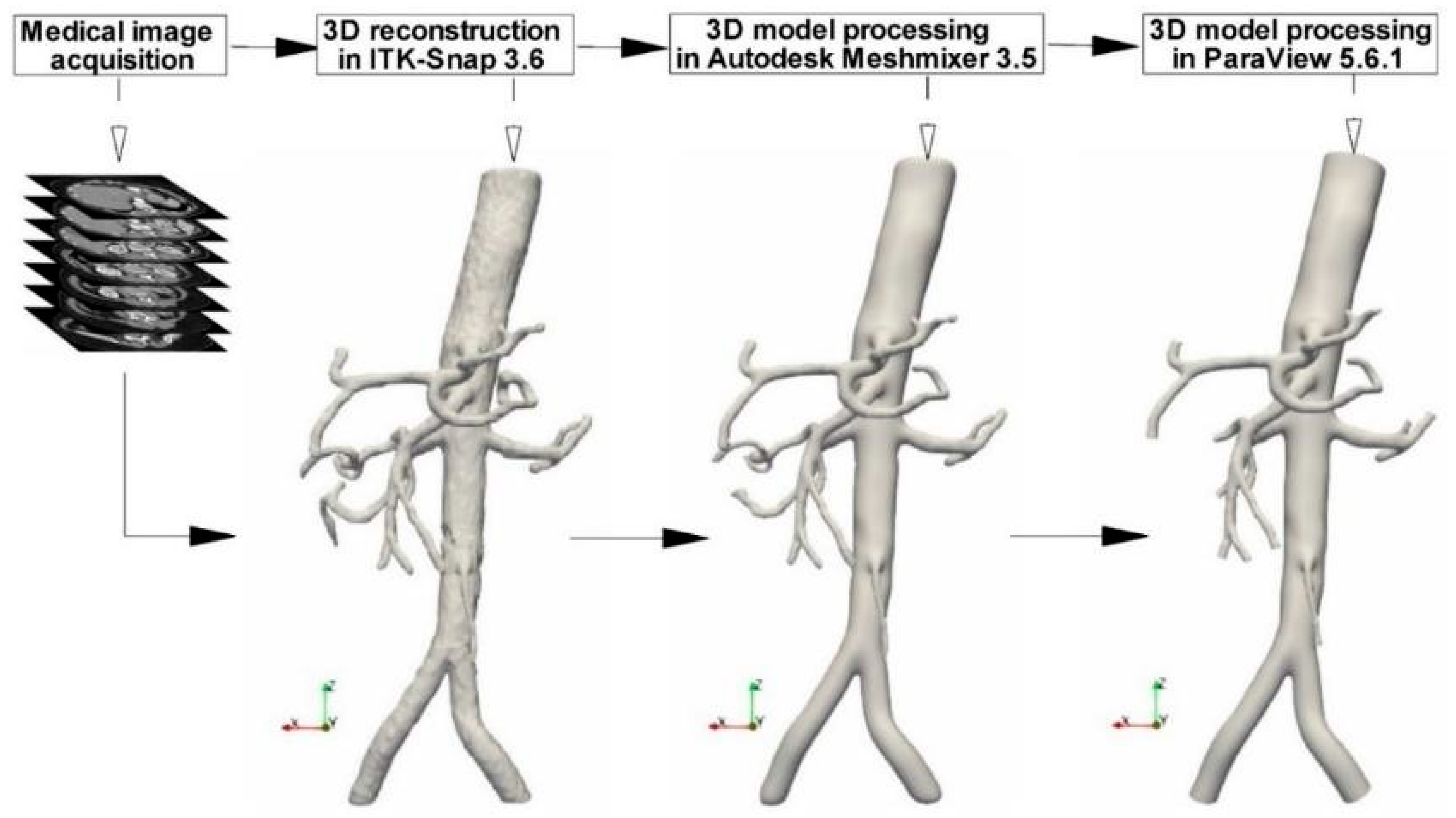
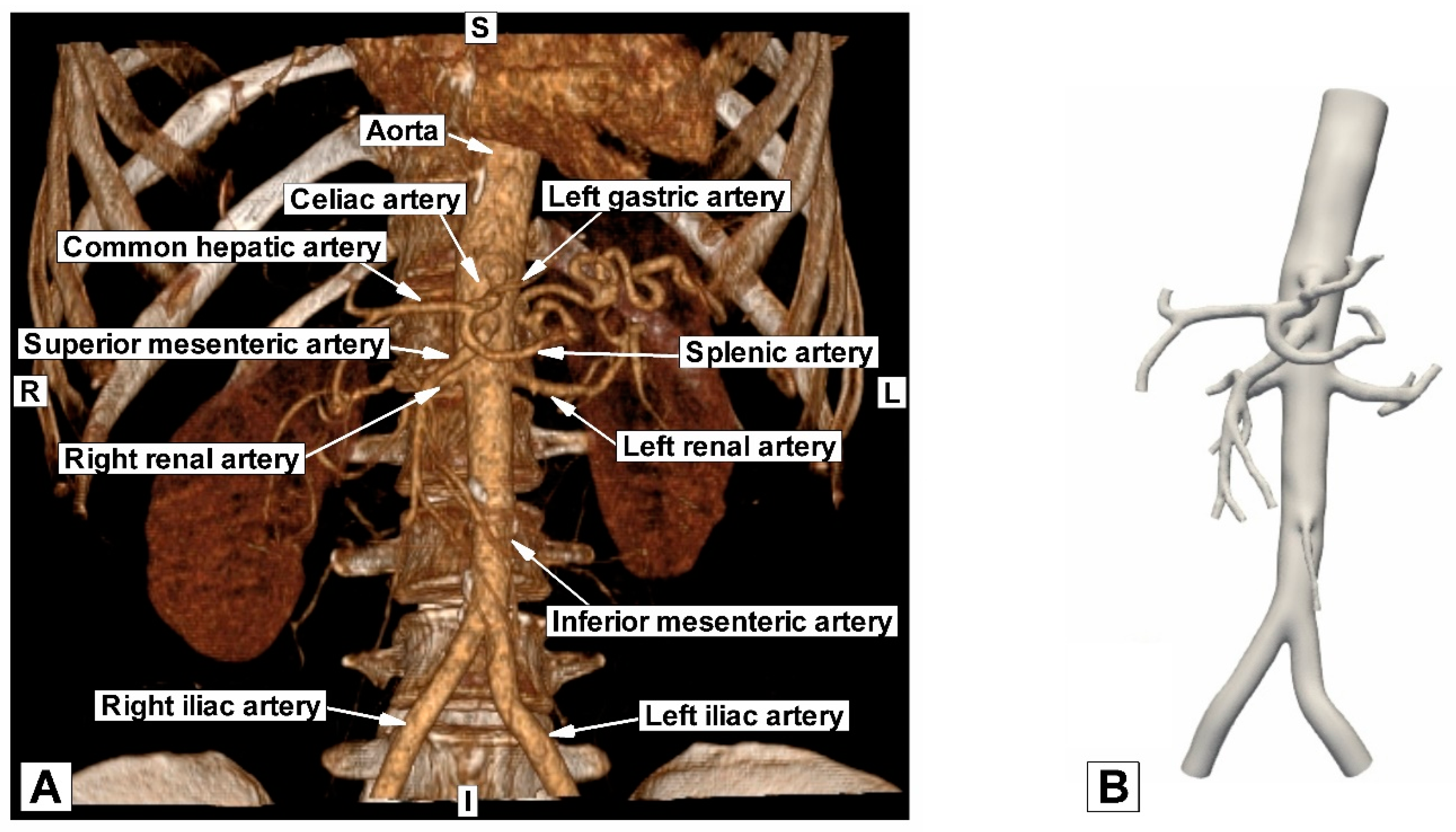
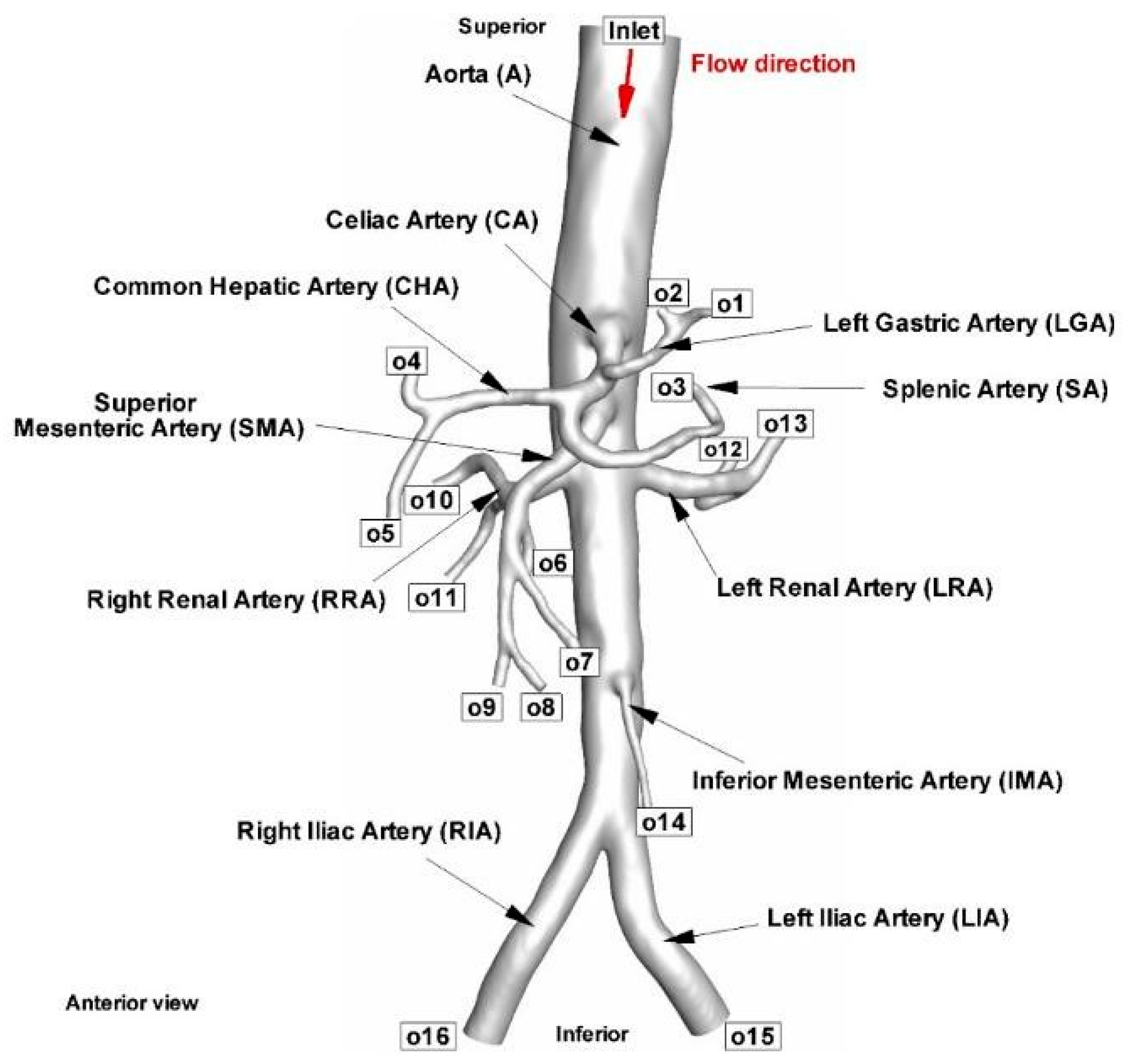
2.2. Geometry Reconstruction
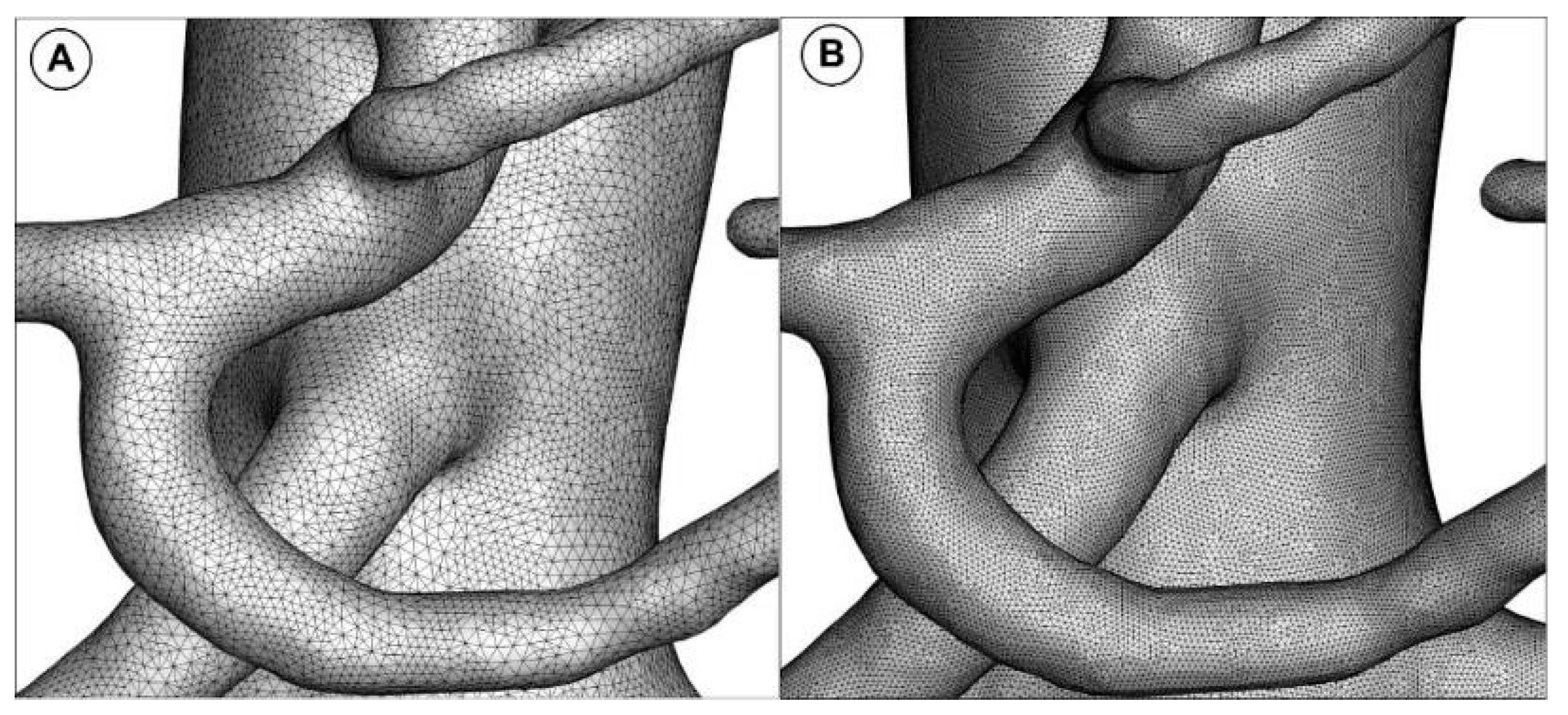
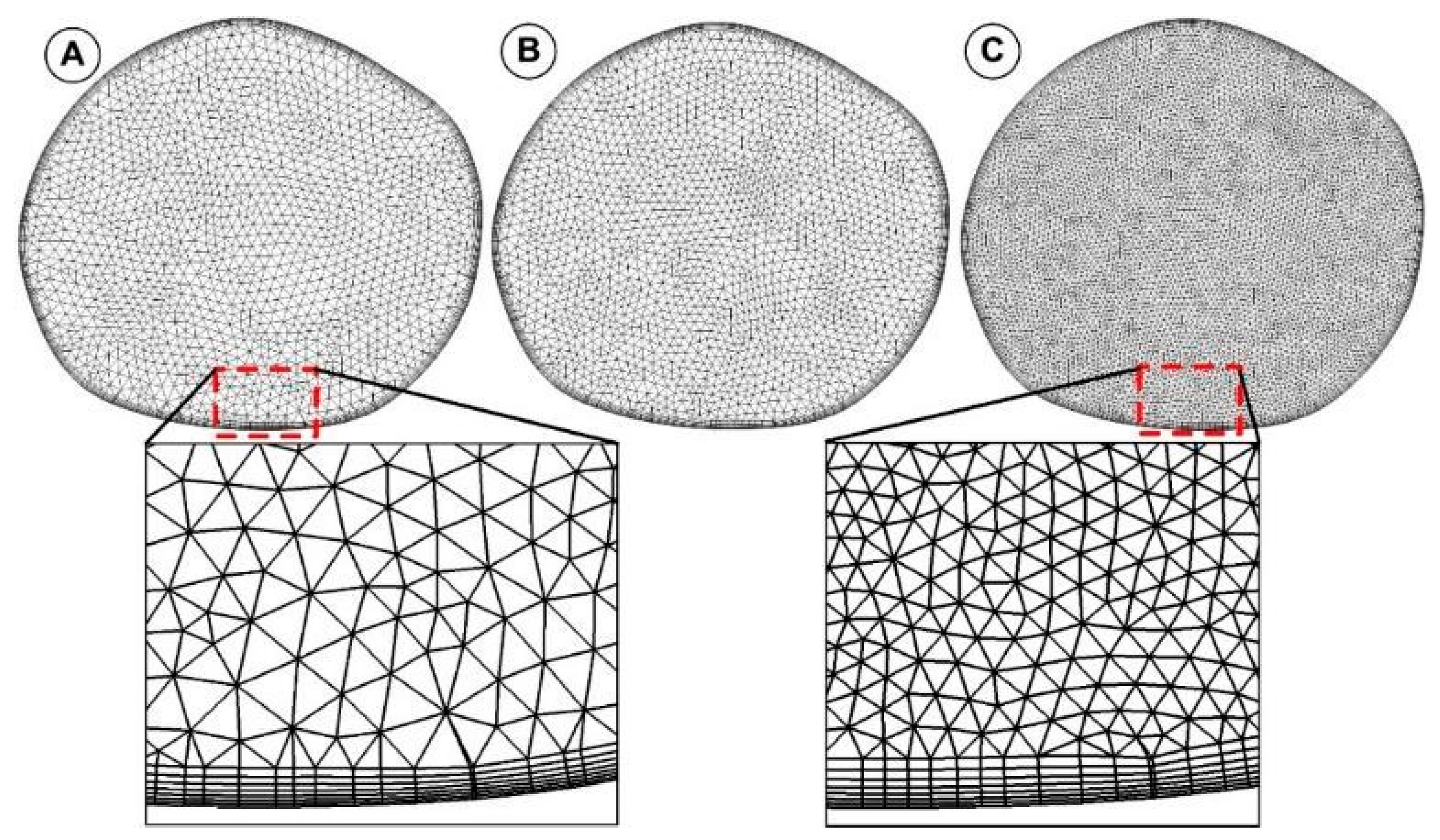
2.3. Geometry Meshing Method
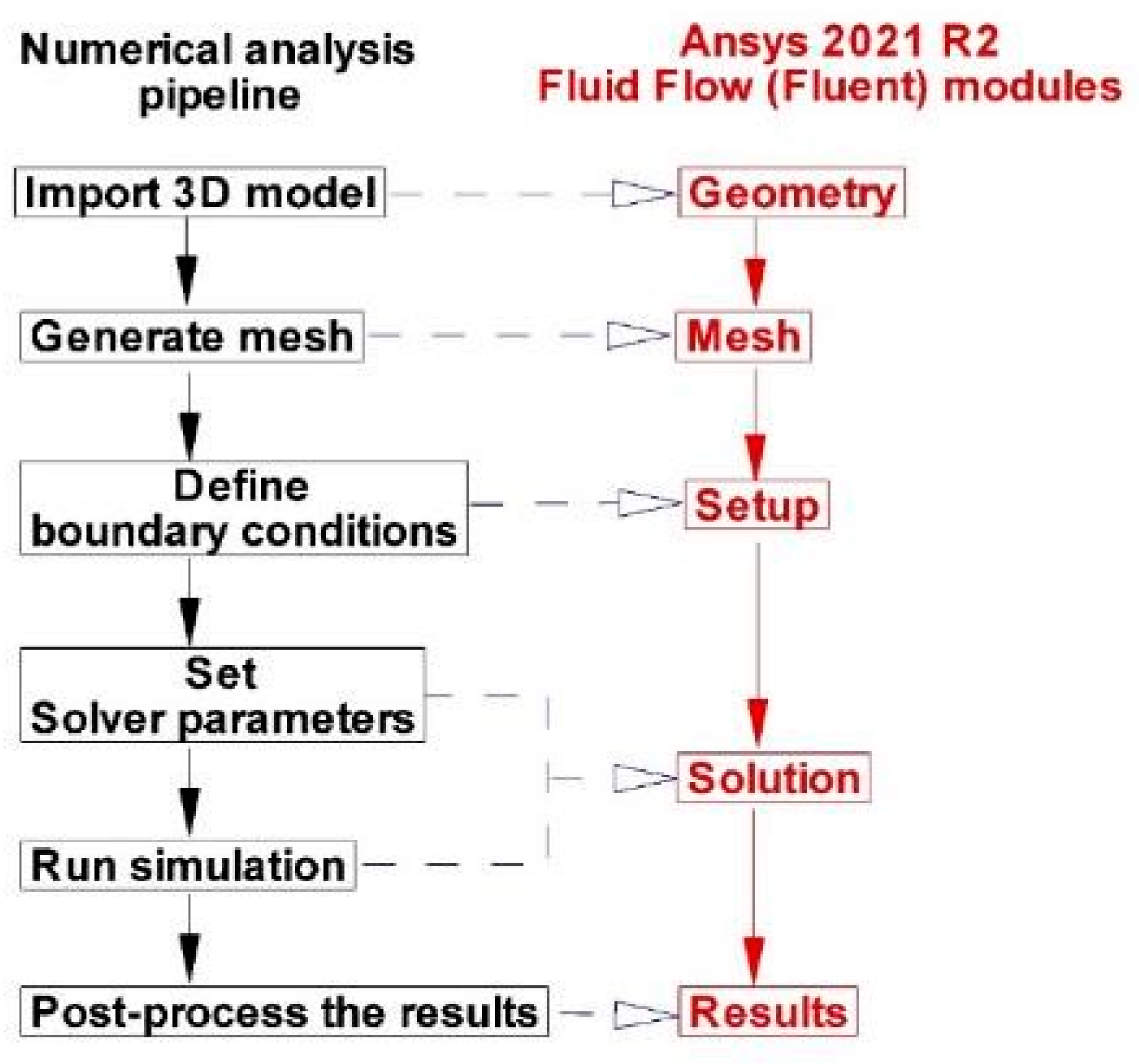
2.4. Computational Fluid Dynamics
2.5. Turbulence Model
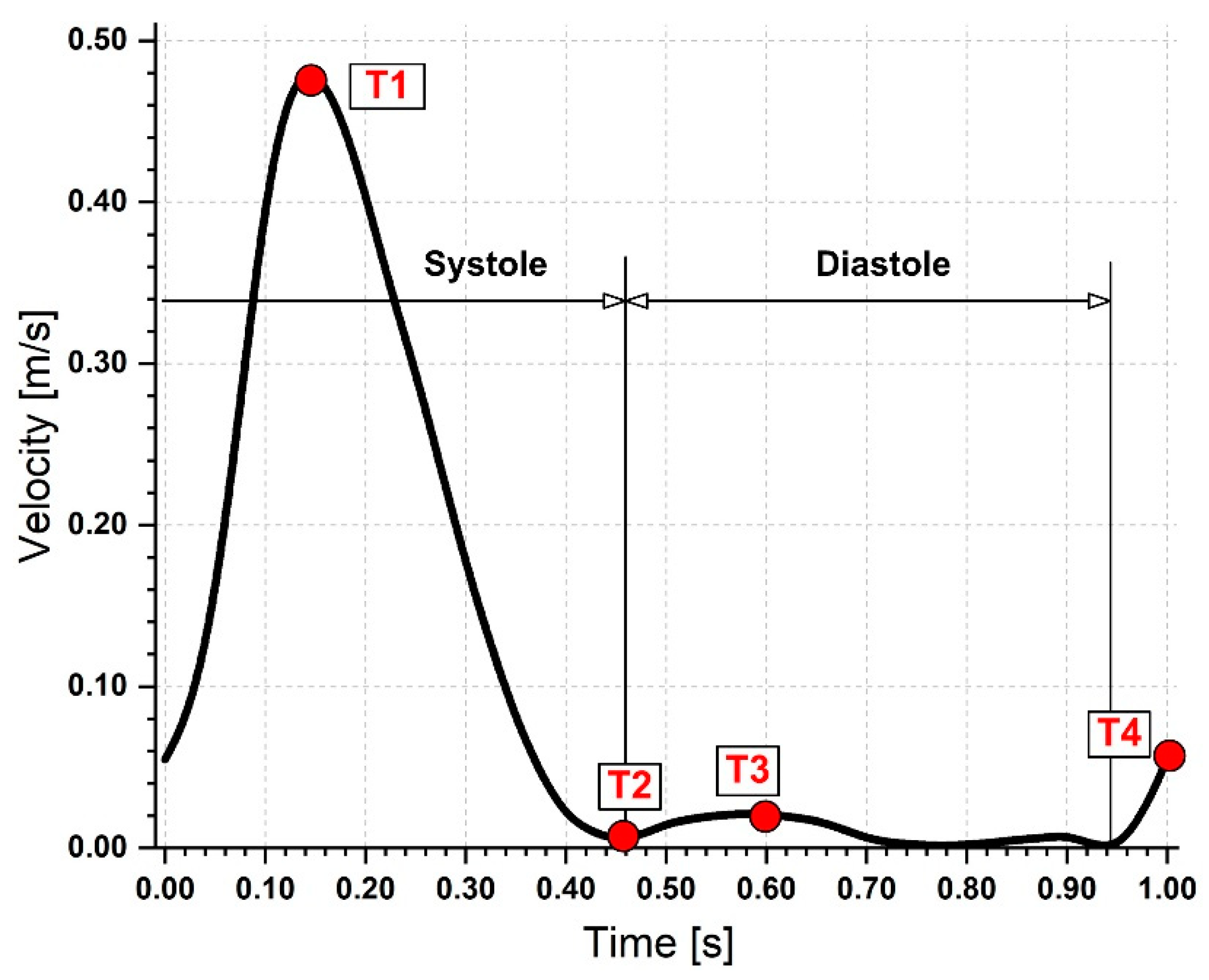
2.6. Boundary Conditions
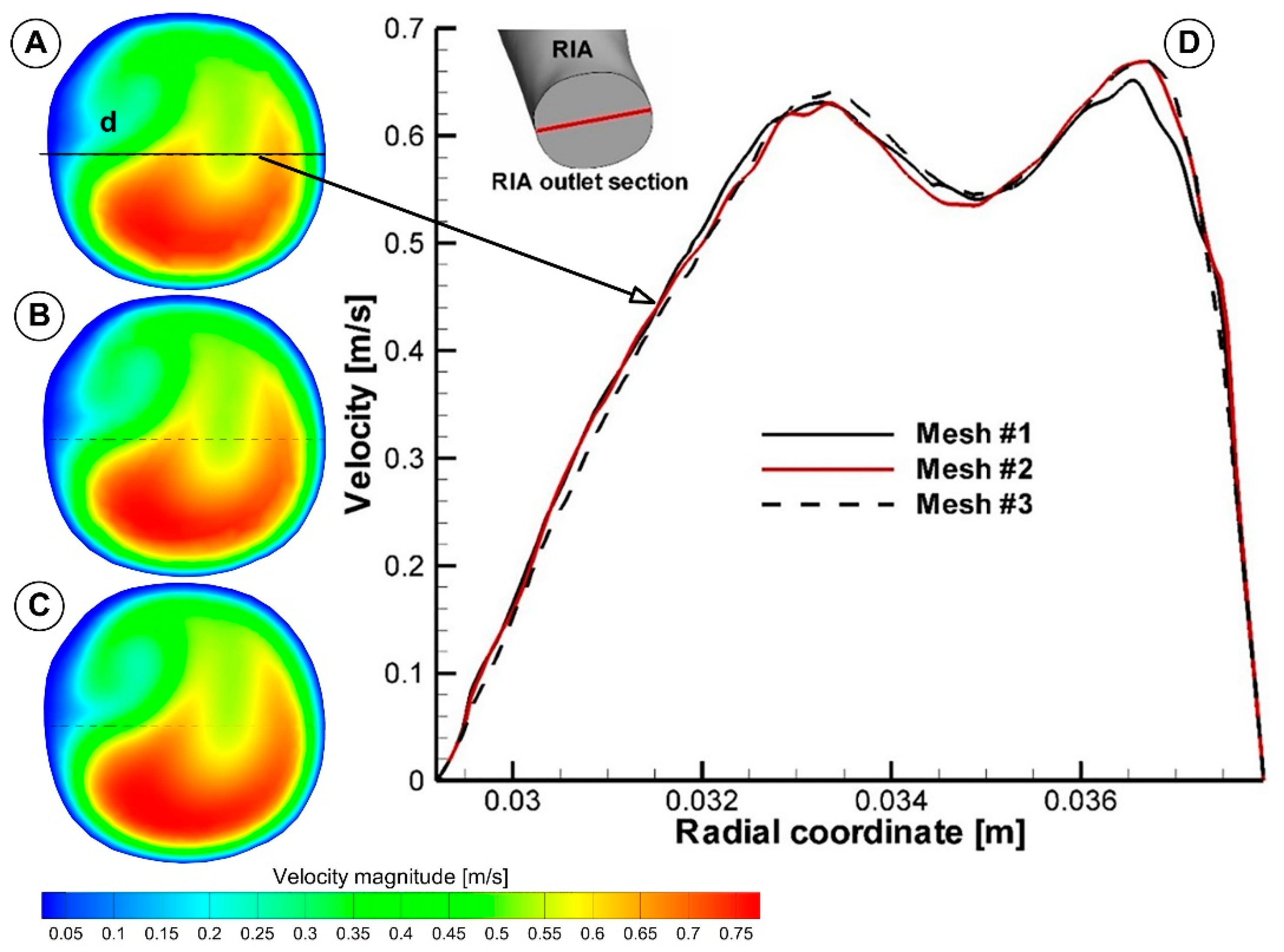
2.7. Grid Independence Study
3. Results
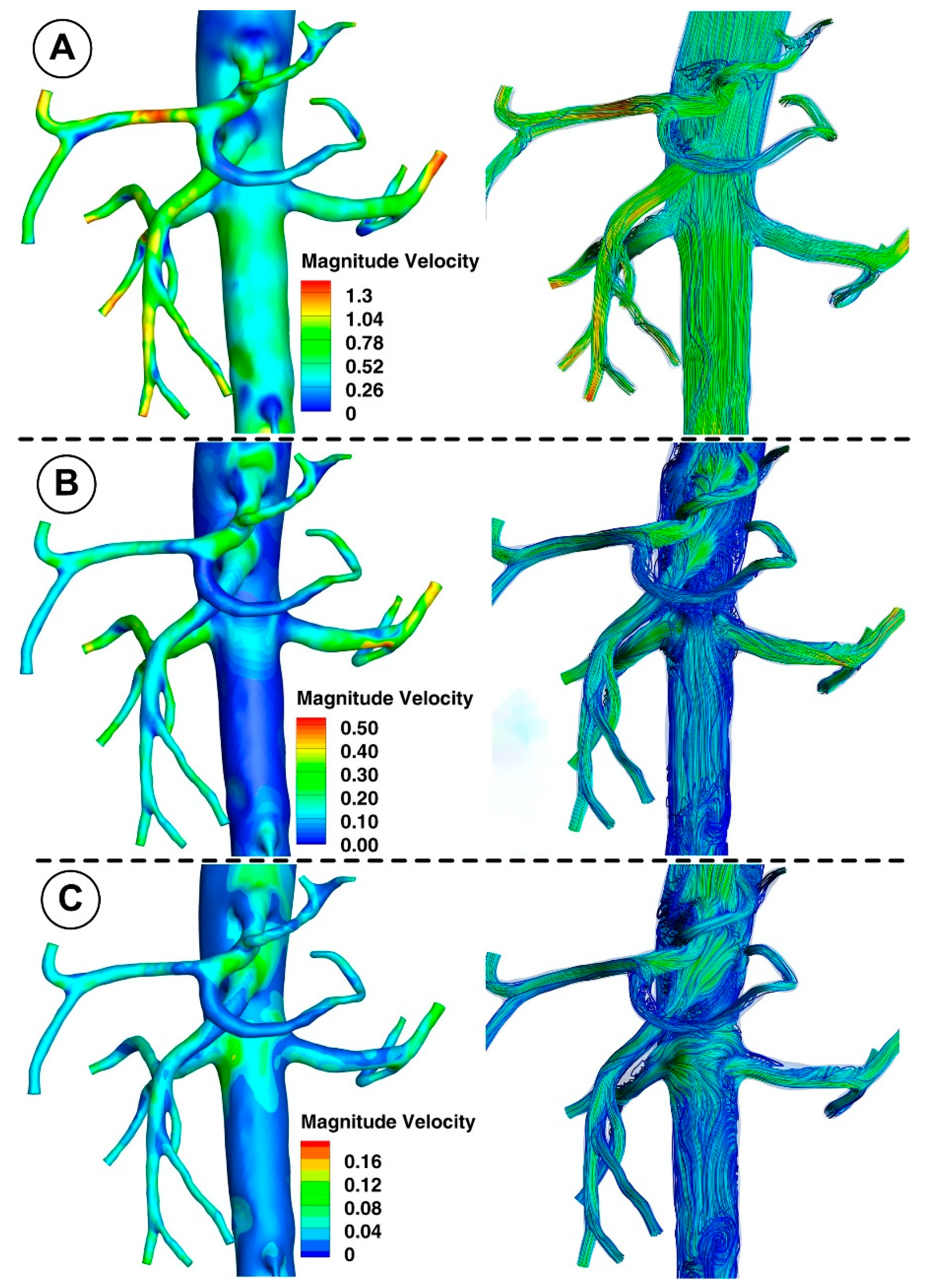
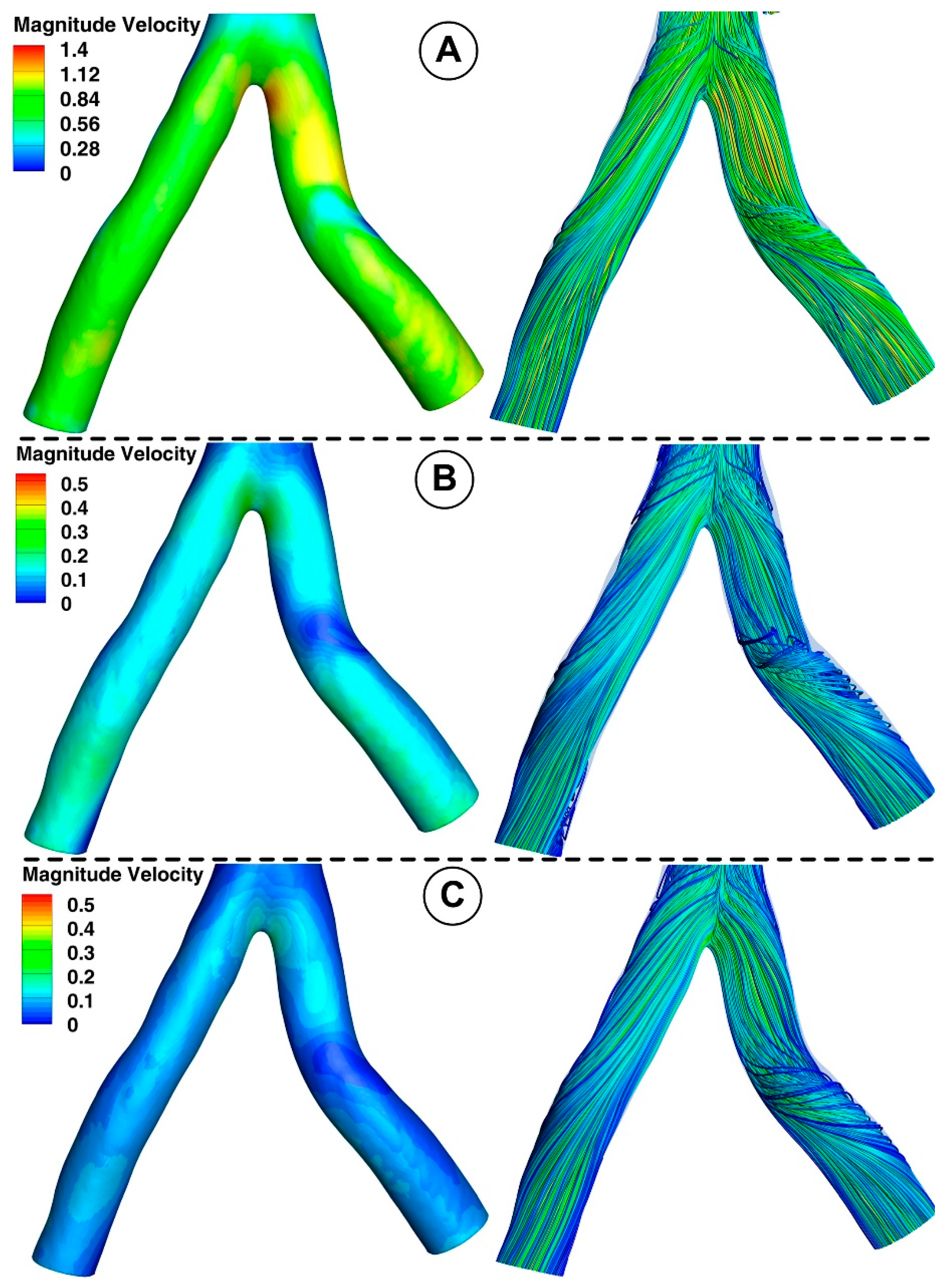
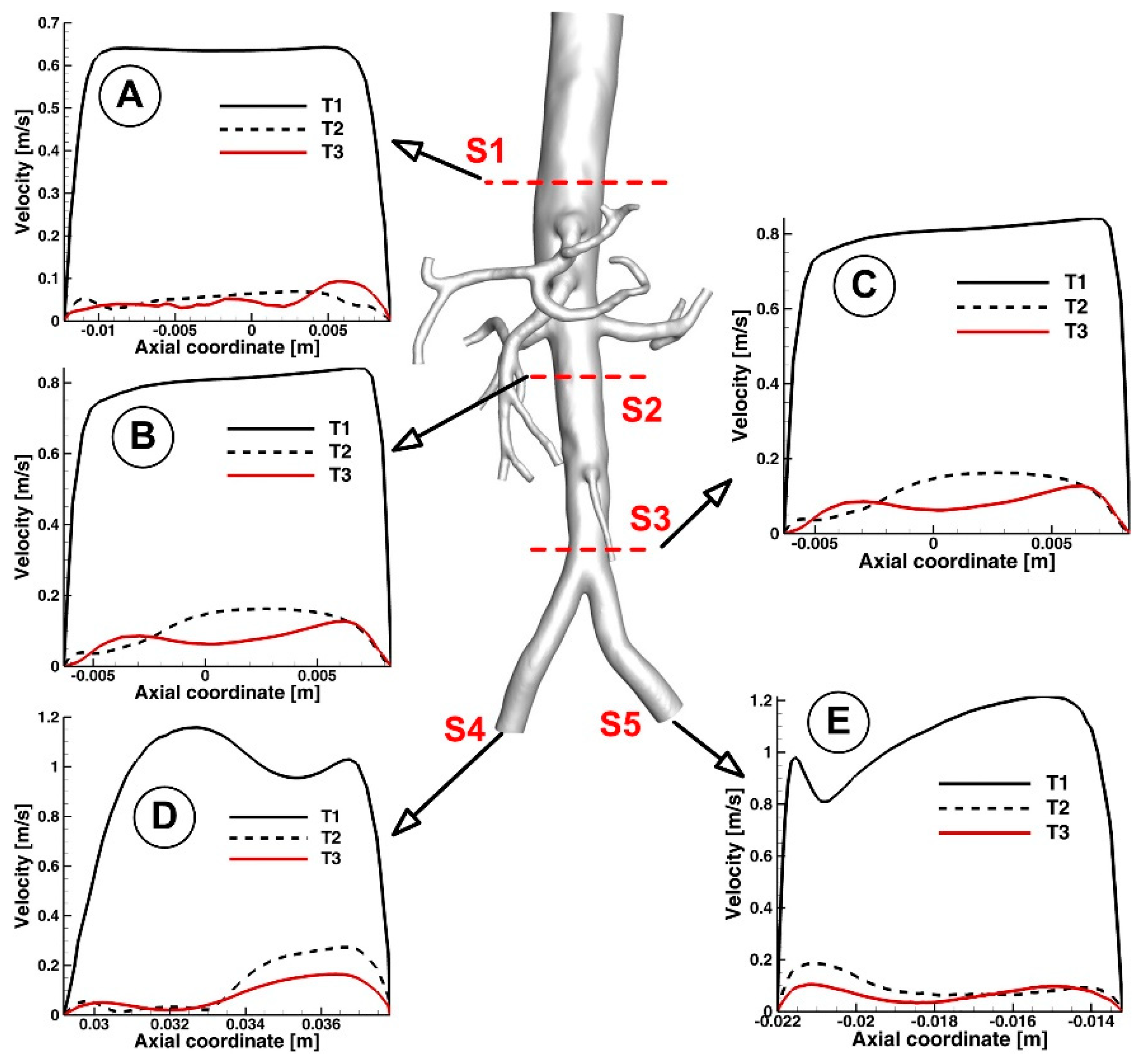
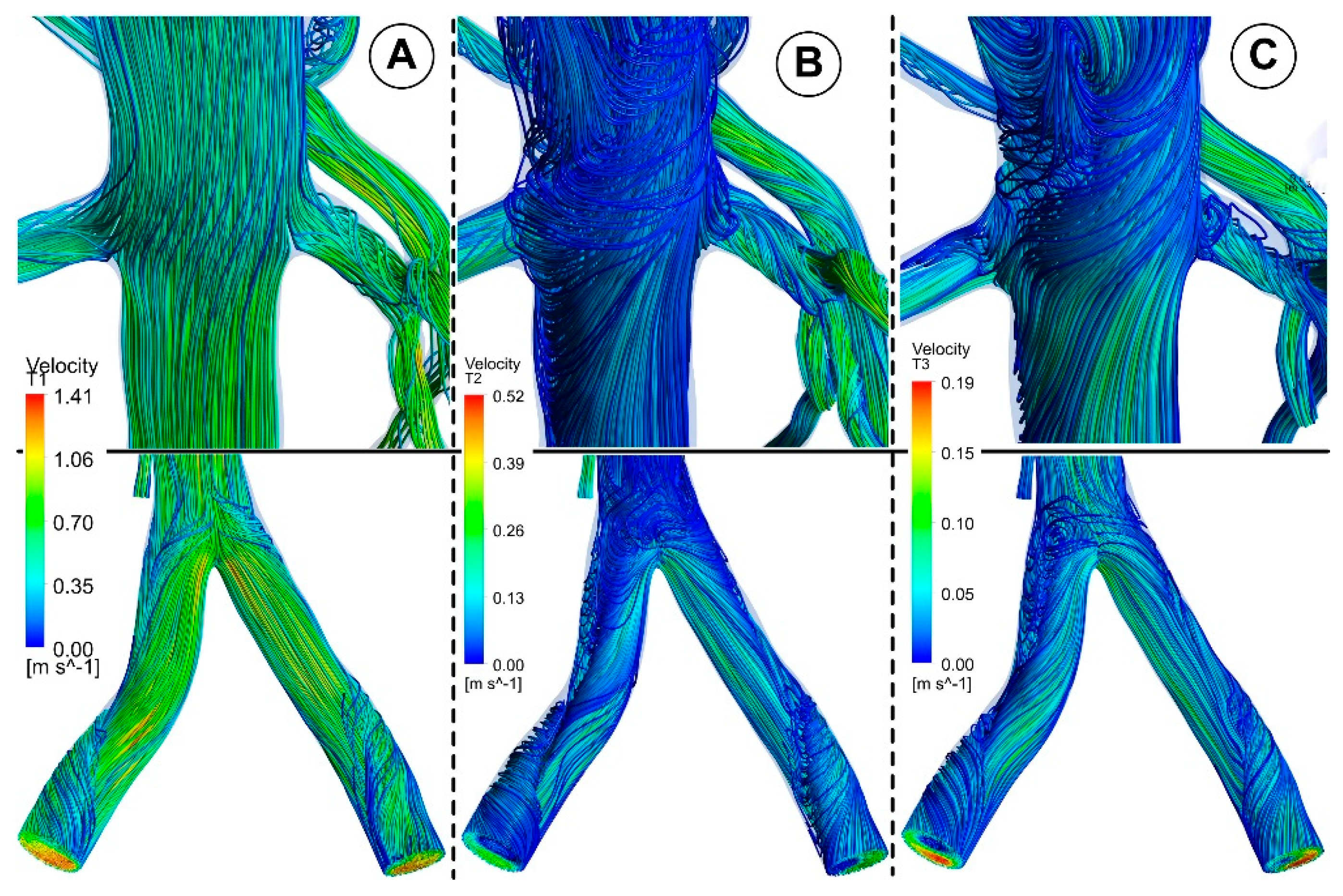
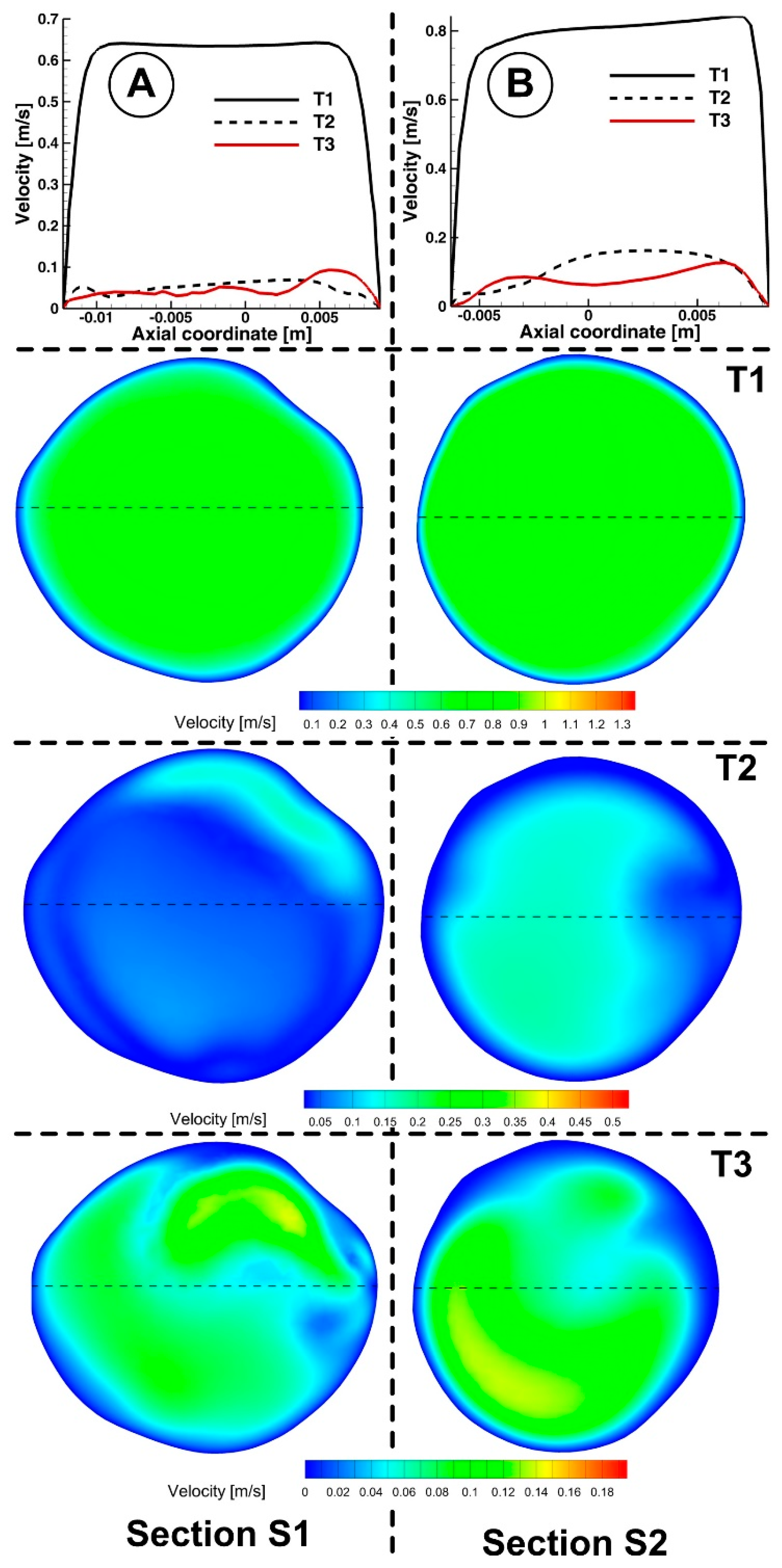
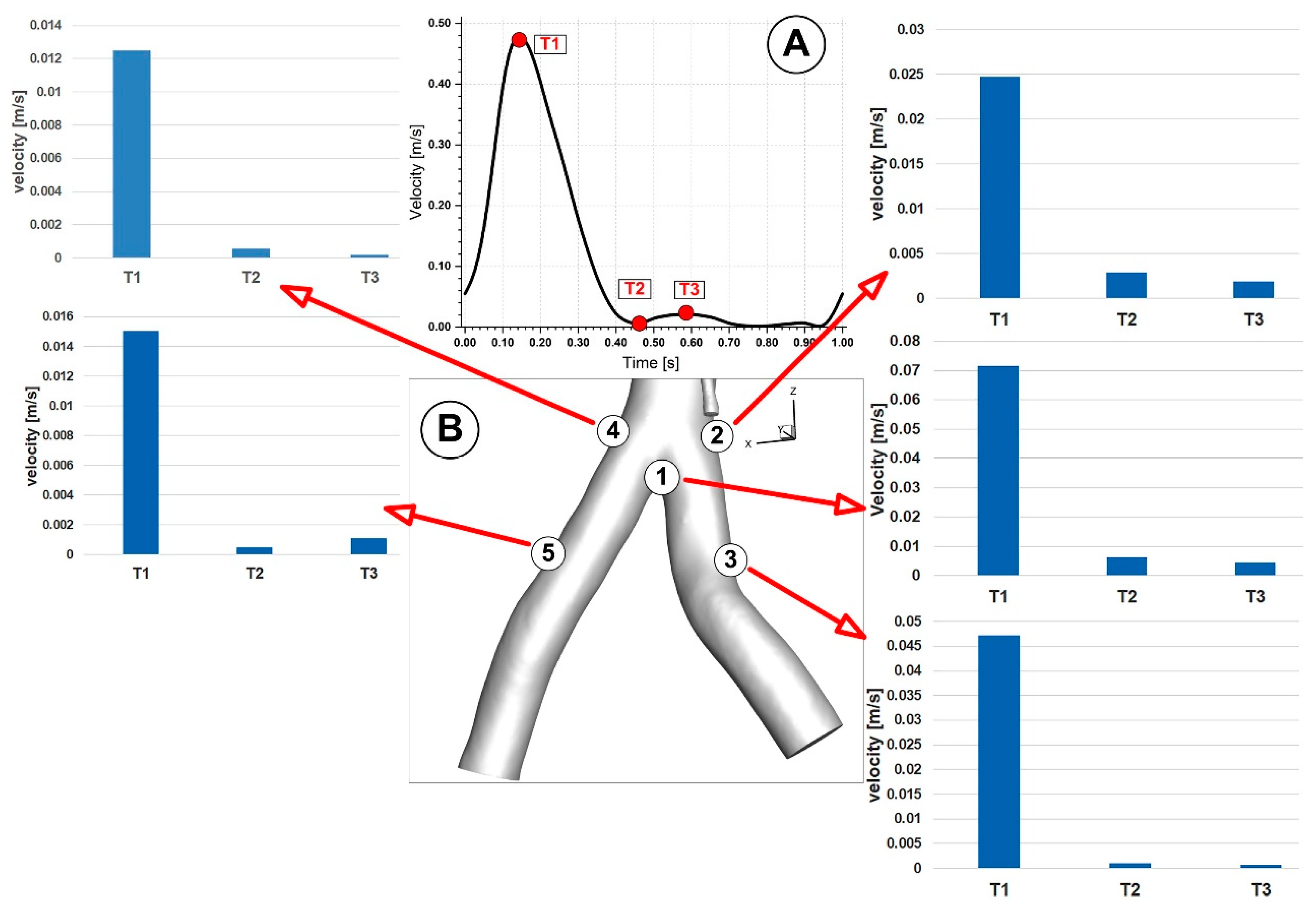
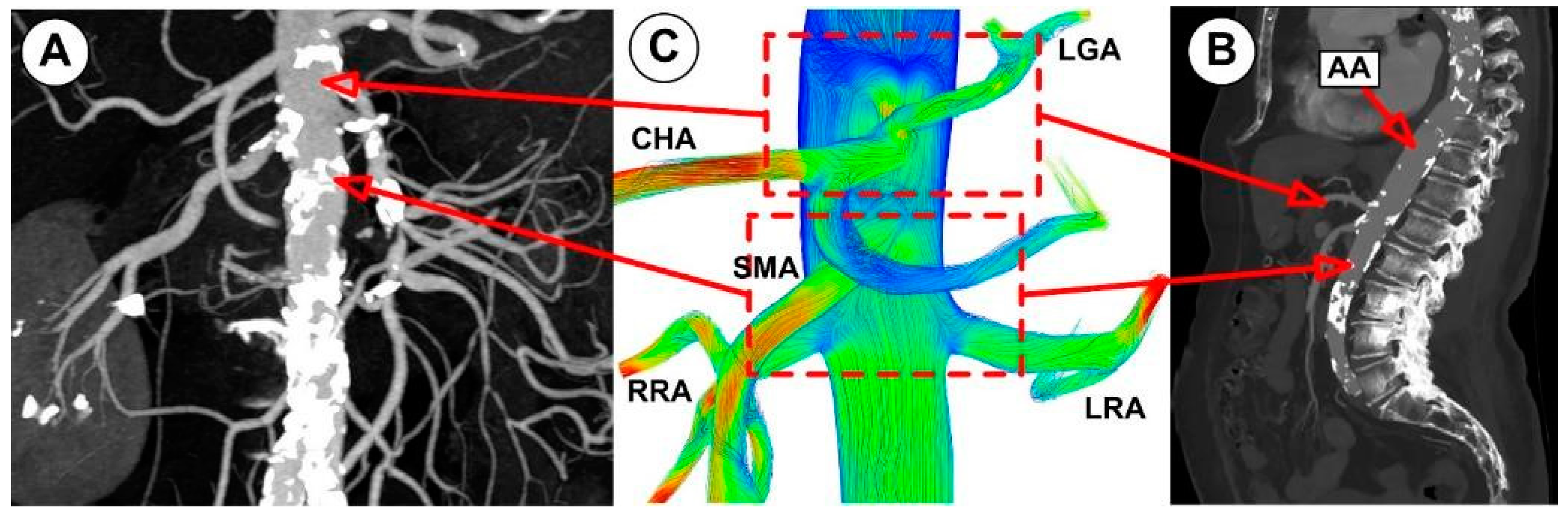
3.1. Velocity Field and Profiles
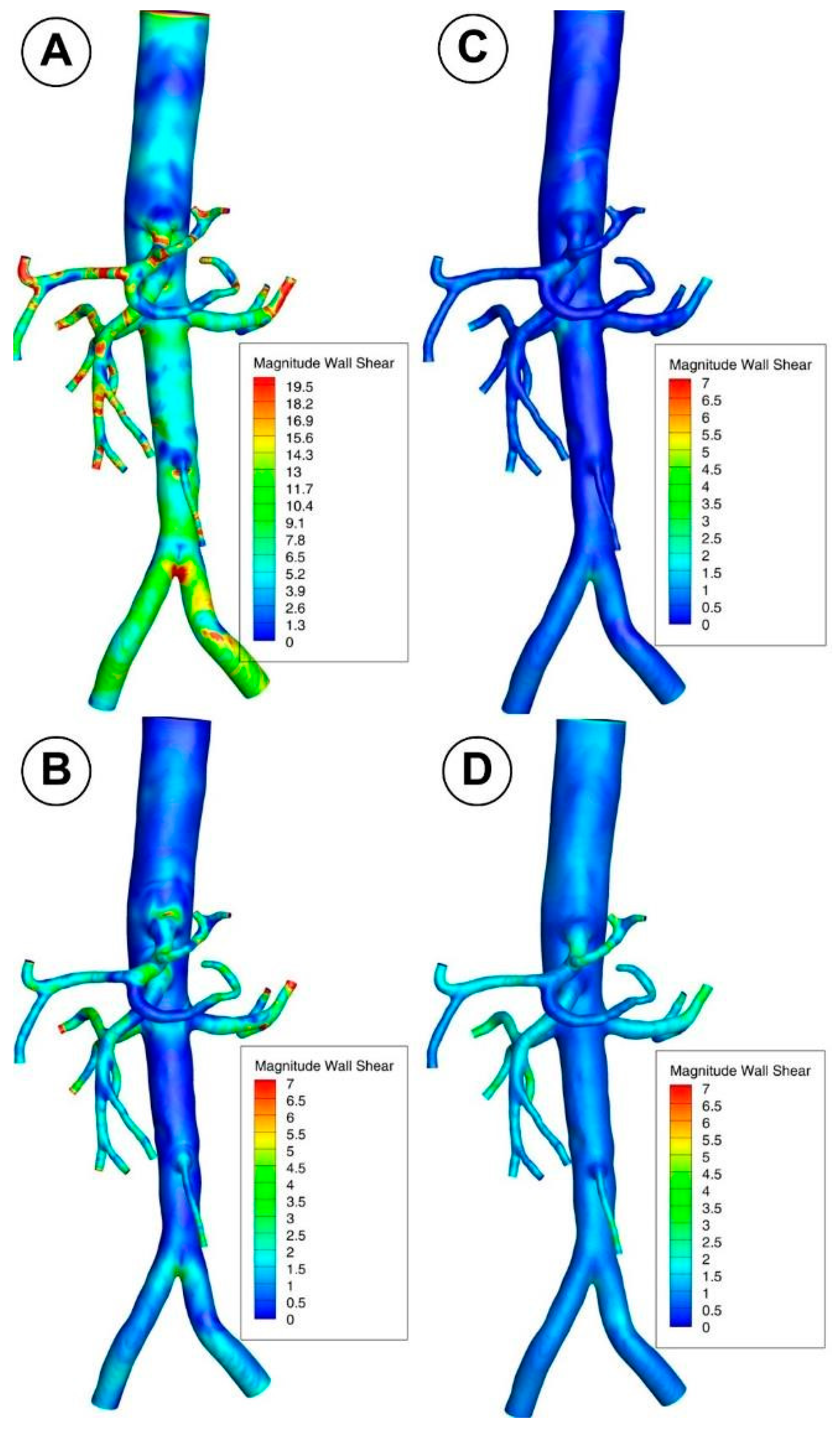
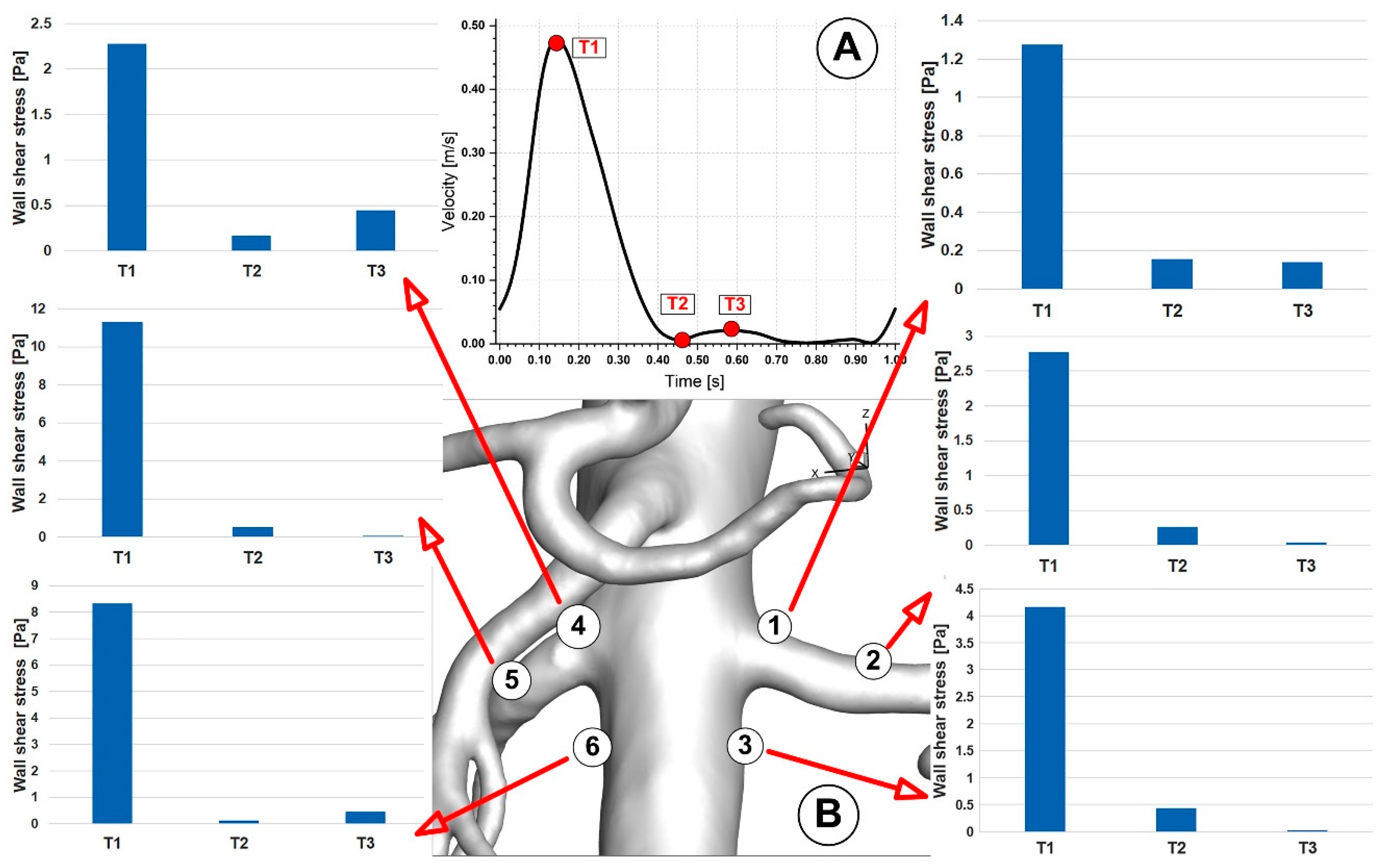
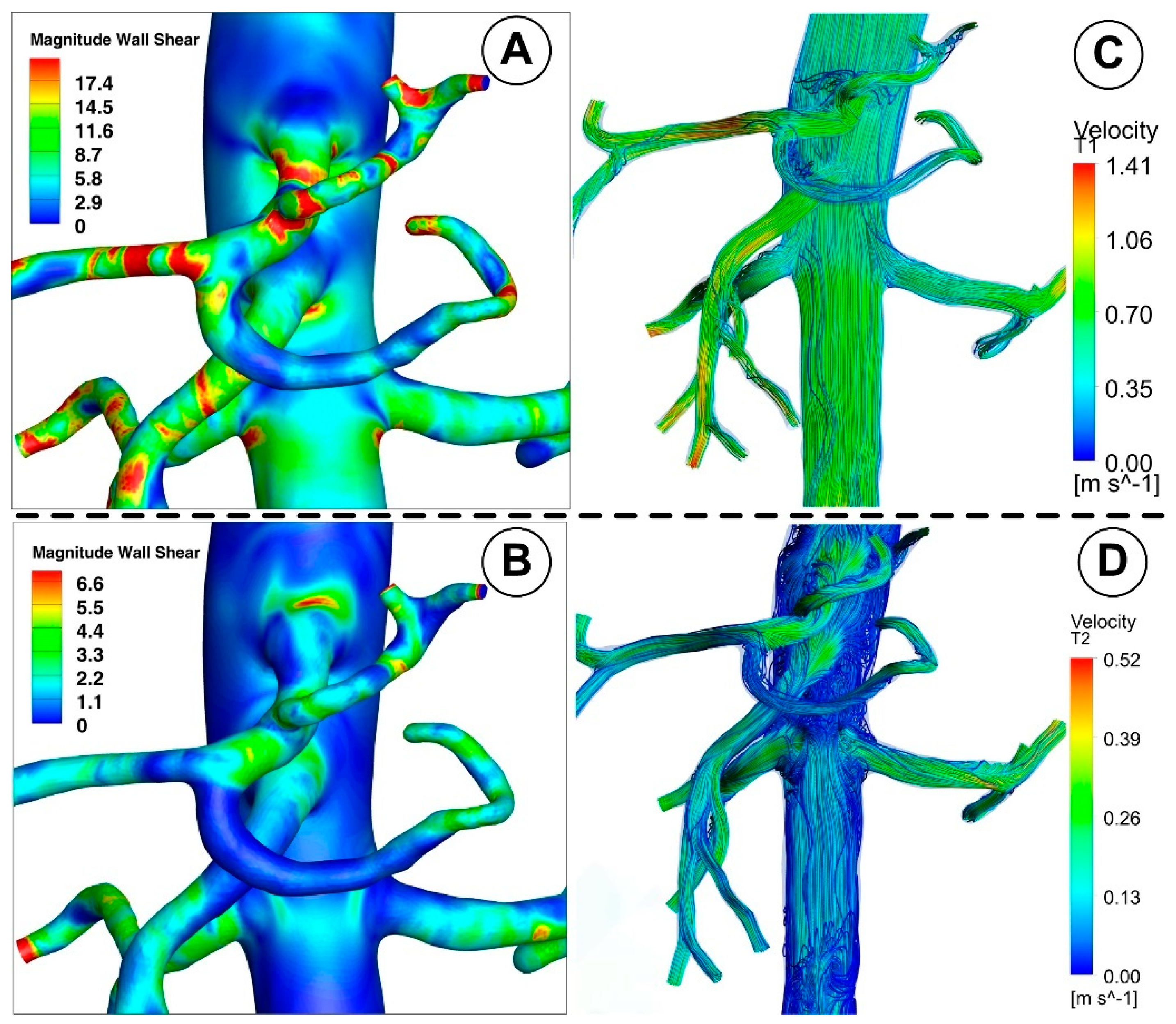
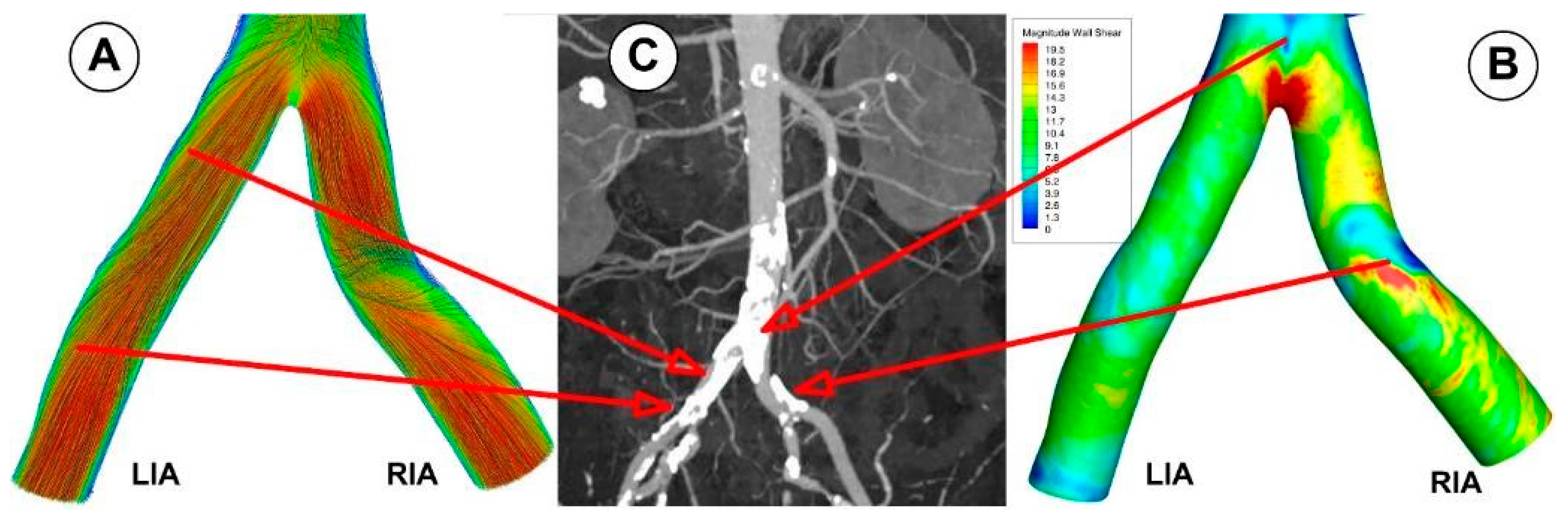
3.2. Wall Shear Stress
4. Discussion
4.1. Velocity Field
4.2. Wall Shear Stress Evolution
4.3. Clinical Relevance
4.4. Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Morris, P.D.; Narracott, A.; von Tengg-Kobligk, H.; Soto, D.A.S.; Hsiao, S.; Lungu, A.; Evans, P.; Bressloff, N.W.; Lawford, P.V.; Hose, D.R.; et al. Computational fluid dynamics modelling in cardiovascular medicine. Heart 2016, 102, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Randles, A.; Frakes, D.H.; Leopold, J.A. Computational Fluid Dynamics and Additive Manufacturing to Diagnose and Treat Cardiovascular Disease. Trends Biotechnol. 2017, 35, 1049–1061. [Google Scholar] [CrossRef] [PubMed]
- Koskinas, K.C.; Chatzizisis, Y.S.; Antoniadis, A.P.; Giannoglou, G.D. Role of Endothelial Shear Stress in Stent Restenosis and Thrombosis: Pathophysiologic Mechanisms and Implications for Clinical Translation. J. Am. Coll. Cardiol. 2012, 59, 1337–1349. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.K.L.; Wang, D.; Ko, J.K.L.; Mazumdar, J.; Le, T.-T.; Ghista, D. Computational medical imaging and hemodynamics framework for functional analysis and assessment of cardiovascular structures. Biomed. Eng. Online 2017, 16, 35. [Google Scholar] [CrossRef] [PubMed]
- Caballero, A.D.; Laín, S. A Review on Computational Fluid Dynamics Modelling in Human Thoracic Aorta. Cardiovasc. Eng. Technol. 2013, 4, 103–130. [Google Scholar] [CrossRef]
- Gijsen, F.J.; Schuurbiers, J.C.; van de Giessen, A.G.; Schaap, M.; van der Steen, A.F.; Wentzel, J.J. 3D reconstruction techniques of human coronary bifurcations for shear stress computations. J. Biomech. 2014, 47, 39–43. [Google Scholar] [CrossRef]
- Lee, D.; Chen, J. Numerical simulation of steady flow fields in a model of abdominal aorta with its peripheral branches. J. Biomech. 2002, 35, 1115–1122. [Google Scholar] [CrossRef]
- Andayesh, M.; Shahidian, A.; Ghassemi, M. Numerical investigation of renal artery hemodynamics based on the physiological response to renal artery stenosis. Biocybern. Biomed. Eng. 2020, 40, 1458–1468. [Google Scholar] [CrossRef]
- Numata, S.; Itatani, K.; Kanda, K.; Doi, K.; Yamazaki, S.; Morimoto, K.; Manabe, K.; Ikemoto, K.; Yaku, H. Blood flow analysis of the aortic arch using computational fluid dynamics. Eur. J. Cardio-Thorac. Surg. 2016, 49, 1578–1585. [Google Scholar] [CrossRef]
- Caballero, A.; Laín, S. Numerical simulation of non-Newtonian blood flow dynamics in human thoracic aorta. Comput. Methods Biomech. Biomed. Eng. 2015, 18, 1200–1216. [Google Scholar] [CrossRef]
- Lin, S.; Han, X.; Bi, Y.; Ju, S.; Gu, L. Fluid-Structure Interaction in Abdominal Aortic Aneurysm: Effect of Modeling Techniques. BioMed Res. Int. 2017, 2017, 7023078. [Google Scholar] [CrossRef] [PubMed]
- Lee, U.; Kwak, H. Analysis of Morphological-Hemodynamic Risk Factors for Aneurysm Rupture Including a Newly Introduced Total Volume Ratio. J. Pers. Med. 2021, 11, 744. [Google Scholar] [CrossRef] [PubMed]
- Martufi, G.; Gasser, T.C. Review: The Role of Biomechanical Modeling in the Rupture Risk Assessment for Abdominal Aortic Aneurysms. J. Biomech. Eng. 2013, 135, 21010. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Chen, R.; Juan, Y.-H.; Li, H.; Wang, J.; Yu, Z.; Liu, H. Clinical validation and assessment of aortic hemodynamics using computational fluid dynamics simulations from computed tomography angiography. Biomed. Eng. Online 2018, 17, 53. [Google Scholar] [CrossRef]
- Gray, R.A.; Pathmanathan, P. Patient-Specific Cardiovascular Computational Modeling: Diversity of Personalization and Challenges. J. Cardiovasc. Transl. Res. 2018, 11, 80–88. [Google Scholar] [CrossRef]
- Carvalho, V.; Carneiro, F.; Ferreira, A.C.; Gama, V.; Teixeira, J.C.; Teixeira, S. Numerical Study of the Unsteady Flow in Simplified and Realistic Iliac Bifurcation Models. Fluids 2021, 6, 284. [Google Scholar] [CrossRef]
- Eslami, P.; Hartman, E.M.J.; Albaghadai, M.; Karady, J.; Jin, Z.; Thondapu, V.; Cefalo, N.V.; Lu, M.T.; Coskun, A.; Stone, P.H.; et al. Validation of Wall Shear Stress Assessment in Non-invasive Coronary CTA versus Invasive Imaging: A Patient-Specific Computational Study. Ann. Biomed. Eng. 2020, 49, 1151–1168. [Google Scholar] [CrossRef]
- Polanczyk, A.; Podgorski, M.; Wozniak, T.; Stefanczyk, L.; Strzelecki, M. Computational Fluid Dynamics as an Engineering Tool for the Reconstruction of Hemodynamics after Carotid Artery Stenosis Operation: A Case Study. Medicina 2018, 54, 42. [Google Scholar] [CrossRef]
- Fry, D.L. Acute Vascular Endothelial Changes Associated with Increased Blood Velocity Gradients. Circ. Res. 1968, 22, 165–197. [Google Scholar] [CrossRef]
- Ling, S.C.; Atabek, H.B.; Fry, D.L.; Patel, D.J.; Janicki, J.S. Application of Heated-Film Velocity and Shear Probes to Hemodynamic Studies. Circ. Res. 1968, 23, 789–801. [Google Scholar] [CrossRef] [Green Version]
- Caro, C.G.; Fitz-Gerald, J.M.; Schroter, R.C. Atheroma and arterial wall shear—Observation, correlation and proposal of a shear dependent mass transfer mechanism for atherogenesis. Proc. R. Soc. Lond. Ser. B Biol. Sci. 1971, 177, 109–133. [Google Scholar] [CrossRef]
- Zhang, W.; Liu, J.; Yan, Q.; Liu, J.; Hong, H.; Mao, L. Computational haemodynamic analysis of left pulmonary artery angulation effects on pulmonary blood flow. Interact. Cardiovasc. Thorac. Surg. 2016, 23, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Chiastra, C.; Gallo, D.; Tasso, P.; Iannaccone, F.; Migliavacca, F.; Wentzel, J.J.; Morbiducci, U. Healthy and diseased coronary bifurcation geometries influence near-wall and intravascular flow: A computational exploration of the hemodynamic risk. J. Biomech. 2017, 58, 79–88. [Google Scholar] [CrossRef]
- Polanczyk, A.; Klinger, M.; Nanobachvili, J.; Huk, I.; Neumayer, C. Artificial Circulatory Model for Analysis of Human and Artificial Vessels. Appl. Sci. 2018, 8, 1017. [Google Scholar] [CrossRef]
- Polanczyk, A.; Piechota-Polanczyk, A.; Stefańczyk, L.; Strzelecki, M. Spatial Configuration of Abdominal Aortic Aneurysm Analysis as a Useful Tool for the Estimation of Stent-Graft Migration. Diagnostics 2020, 10, 737. [Google Scholar] [CrossRef]
- Polanczyk, A.; Piechota-Polanczyk, A.; Domenig, C.; Nanobachvili, J.; Huk, I.; Neumayer, C. Computational Fluid Dynamic Accuracy in Mimicking Changes in Blood Hemodynamics in Patients with Acute Type IIIb Aortic Dissection Treated with TEVAR. Appl. Sci. 2018, 8, 1309. [Google Scholar] [CrossRef]
- Totorean, A.F.; Bernad, S.I.; Ciocan, T.; Totorean, I.C.; Bernad, E.S. Computational Fluid Dynamics Applications in Cardiovascular Medicine-from Medical Image-Based Modeling to Simulation: Numerical Analysis of Blood Flow in Abdominal Aorta. In Advances in Fluid Mechanics Modelling and Simulations; Zeidan, D., Zhang, L.T., Goncalves Da Silva, E., Merker, J., Eds.; Springer: Singapore, 2022; pp. 1–42. [Google Scholar] [CrossRef]
- Ippolito, D.; Franzesi, C.T.; Fior, D.; Bonaffini, P.A.; Minutolo, O.; Sironi, S. Low kV settings CT angiography (CTA) with low dose contrast medium volume protocol in the assessment of thoracic and abdominal aorta disease: A feasibility study. Br. J. Radiol. 2015, 88, 20140140. [Google Scholar] [CrossRef]
- Mix, J.; Pitta, S.R.; Schwartz, J.P.; Tuchek, J.; Dieter, R.S.; Freeman, M.B. Abdominal Aorta. In Peripheral Arterial Disease; Dieter, R.S., Dieter, R.A., Jr., Dieter, R.A., III, Eds.; McGraw Hill: New York, NY, USA, 2009; ISBN 978-0071481793. [Google Scholar]
- Michalinos, A.; Goutas, N.; Spiliopoulou, C.; Nikiteas, N.; Skandalakis, P.; Gorgoulis, V.; Troupis, T. A study concerning morphometry of abdominal aorta branches and abdominal viscera: Relations and correlation. Folia Morphol. 2016, 75, 60–75. [Google Scholar] [CrossRef]
- Moin, P.; Mahesh, K. Direct Numerical Simulation: A Tool in Turbulence Research. Annu. Rev. Fluid Mech. 1998, 30, 539–578. [Google Scholar] [CrossRef] [Green Version]
- Mahalingam, A.; Gawandalkar, U.U.; Kini, G.; Buradi, A.; Araki, T.; Ikeda, N.; Nicolaides, A.; Laird, J.R.; Saba, L.; Suri, J.S. Numerical analysis of the effect of turbulence transition on the hemodynamic parameters in human coronary arteries. Cardiovasc. Diagn. Ther. 2016, 6, 208–220. [Google Scholar] [CrossRef]
- ANSYS. Ansys Fluent Tutorial Guide, 2021 R1; ANSYS Inc.: Pittsburgh, PA, USA, 2021. [Google Scholar]
- Jin, S.; Oshinski, J.; Giddens, D.P. Effects of Wall Motion and Compliance on Flow Patterns in the Ascending Aorta. J. Biomech. Eng. 2003, 125, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Banks, J.; Bressloff, N.W. Turbulence Modeling in Three-Dimensional Stenosed Arterial Bifurcations. J. Biomech. Eng. 2007, 129, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Totorean, A.F.; Hudrea, C.I.; Bosioc, A.I.; Bernad, S.I. Flow field evolution in stented versus stenosed coronary artery. Proc. Rom. Acad. Ser. A-Math. Phys. 2017, 18, 248–255. [Google Scholar]
- Bernad, S.I.; Totorean, A.; Bosioc, A.; Stanciu, R.; Bernad, E.S. Numerical investigation of Dean vortices in a curved pipe. In Proceedings of the 11th International Conference of Numerical Analysis and Applied Mathematics 2013, ICNAAM 2013, Rhodes, Greece, 21–27 September 2013; Volume 1558, pp. 172–175. [Google Scholar] [CrossRef]
- Varghese, S.S.; Frankel, S.H. Numerical Modeling of Pulsatile Turbulent Flow in Stenotic Vessels. J. Biomech. Eng. 2003, 125, 445–460. [Google Scholar] [CrossRef]
- Tan, F.P.P.; Soloperto, G.; Bashford, S.; Wood, N.B.; Thom, S.; Hughes, A.; Xu, X.Y. Analysis of Flow Disturbance in a Stenosed Carotid Artery Bifurcation Using Two-Equation Transitional and Turbulence Models. J. Biomech. Eng. 2008, 130, 61008. [Google Scholar] [CrossRef]
- Totorean, A.F.; Bosioc, A.I.; Bernad, S.I.; Susan-Resiga, R. Identification and visualization of the vortices in bypass graft flow. Proc. Rom. Acad. Ser. A-Math. Phys. 2014, 15, 52–59. [Google Scholar]
- Liu, X.; Fan, Y.; Deng, X.; Zhan, F. Effect of non-Newtonian and pulsatile blood flow on mass transport in the human aorta. J. Biomech. 2011, 44, 1123–1131. [Google Scholar] [CrossRef]
- Johnson, D.A.; Naik, U.P.; Beris, A.N. Efficient implementation of the proper outlet flow conditions in blood flow simulations through asymmetric arterial bifurcations. Int. J. Numer. Methods Fluids 2010, 66, 1383–1408. [Google Scholar] [CrossRef]
- Perktold, K.; Resch, M.; Florian, H. Pulsatile Non-Newtonian Flow Characteristics in a Three-Dimensional Human Carotid Bifurcation Model. J. Biomech. Eng. 1991, 113, 464–475. [Google Scholar] [CrossRef]
- Anor, T.; Grinberg, L.; Baek, H.; Madsen, J.R.; Jayaraman, M.V.; Karniadakis, G.E. Modeling of blood fow in arterial trees. Wiley Interdiscip. Rev. Syst. Biol. Med. 2010, 2, 612–623. [Google Scholar] [CrossRef]
- Madhavan, S.; Kemmerling, E.M.C. The effect of inlet and outlet boundary conditions in image-based CFD modeling of aortic flow. Biomed. Eng. Online 2018, 17, 66. [Google Scholar] [CrossRef] [PubMed]
- Ku, D.N. Blood Flow in Arteries. Annu. Rev. Fluid Mech. 1997, 29, 399–434. [Google Scholar] [CrossRef]
- Moore, J.E., Jr.; Ku, D.N.; Zarin, C.K.; Glagov, S. Pulsatile flow visualization in the abdominal aorta under differing physiologic conditions: Implications for increased susceptibility to Atherosclerosis. J. Biomech. Eng. 1992, 114, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Moore, J., Jr.; Ku, D.N. Pulsatile Velocity Measurements in a Model of the Human Abdominal Aorta Under Simulated Exercise and Postprandial Conditions. J. Biomech. Eng. 1994, 116, 107–111. [Google Scholar] [CrossRef]
- Taylor, C.A.; Hughes, T.J.; Zarins, C.K. Effect of exercise on hemodynamic conditions in the abdominal aorta. J. Vasc. Surg. 1999, 29, 1077–1089. [Google Scholar] [CrossRef]
- Walburn, F.J.; Stein, P.D. Velocity profiles in symmetrically branched tubes simulating the aortic bifurcation. J. Biomech. 1981, 14, 601–611. [Google Scholar] [CrossRef]
- Farnoush, A.; Avolio, A.; Qian, Y. Effect of Bifurcation Angle Configuration and Ratio of Daughter Diameters on Hemodynamics of Bifurcation Aneurysms. Am. J. Neuroradiol. 2012, 34, 391–396. [Google Scholar] [CrossRef]
- Cunningham, K.S.; Gotlieb, A.I. The role of shear stress in the pathogenesis of atherosclerosis. Lab. Investig. 2004, 85, 9–23. [Google Scholar] [CrossRef]
- Shahcheraghi, N.; Dwyer, H.A.; Cheer, A.Y.; Barakat, A.I.; Rutaganira, T. Unsteady and Three-Dimensional Simulation of Blood Flow in the Human Aortic Arch. J. Biomech. Eng. 2002, 124, 378–387. [Google Scholar] [CrossRef]
- Mostbeck, G.H.; Dulce, M.C.; Caputo, G.R.; Proctor, E.; Higgins, C.B. Flow pattern analysis in the abdominal aorta with velocity encoded cine MR imaging. J. Magn. Reson. Imaging 1993, 3, 617–623. [Google Scholar] [CrossRef]
- Malek, A.M.; Alper, S.L.; Izumo, S. Hemodynamic Shear Stress and Its Role in Atherosclerosis. JAMA 1999, 282, 2035–2042. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.-J.; Liu, C.-A.; Huang, B.; Tseng, A.H.; Wang, D.L. Shear-induced endothelial mechanotransduction: The interplay between reactive oxygen species (ROS) and nitric oxide (NO) and the pathophysiological implications. J. Biomed. Sci. 2014, 21, 3. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.-S.J.; Haga, J.H.; Chien, S. Molecular basis of the effects of shear stress on vascular endothelial cells. J. Biomech. 2005, 38, 1949–1971. [Google Scholar] [CrossRef]
- Nerem, R.M.; Rumbergerjr, J.A.; Gross, D.R.; Hamlin, R.L.; Geiger, G.L. Hot-Film Anemometer Velocity Measurements of Arterial Blood Flow in Horses. Circ. Res. 1974, 34, 193–203. [Google Scholar] [CrossRef]
- Bernad, S.I.; Susan-Resiga, D.; Bernad, E.S. Hemodynamic Effects on Particle Targeting in the Arterial Bifurcation for Different Magnet Positions. Molecules 2019, 24, 2509. [Google Scholar] [CrossRef] [PubMed]
- Bernad, S.I.; Susan-Resiga, D.; Vekas, L.; Bernad, E.S. Drug targeting investigation in the critical region of the arterial bypass graft. J. Magn. Magn. Mater. 2019, 475, 14–23. [Google Scholar] [CrossRef]
- Bonfanti, M.; Franzetti, G.; Maritati, G.; Homer-Vanniasinkam, S.; Balabani, S.; Díaz-Zuccarini, V. Patient-specific haemodynamic simulations of complex aortic dissections informed by commonly available clinical datasets. Med. Eng. Phys. 2019, 71, 45–55. [Google Scholar] [CrossRef]
- Carreau, P.J. Rheological Equations from Molecular Network Theories. Trans. Soc. Rheol. 1972, 16, 99–127. [Google Scholar] [CrossRef]
- Shad, R.; Kaiser, A.D.; Kong, S.; Fong, R.; Quach, N.; Bowles, C.; Kasinpila, P.; Shudo, Y.; Teuteberg, J.; Woo, Y.J.; et al. Patient-Specific Computational Fluid Dynamics Reveal Localized Flow Patterns Predictive of Post–Left Ventricular Assist Device Aortic Incompetence. Circ. Heart Fail. 2021, 14, e008034. [Google Scholar] [CrossRef]
- Bernad, S.I.; Craciunescu, I.; Sandhu, G.S.; Dragomir-Daescu, D.; Tombacz, E.; Vekas, L.; Turcu, R. Fluid targeted delivery of functionalized magnetoresponsive nanocomposite particles to a ferromagnetic stent. J. Magn. Magn. Mater. 2021, 519, 167489. [Google Scholar] [CrossRef]
- Motaghedifar, M.R.; Fakhar, A.; Tabatabaei, H.; Mazochi, M. The effect of pharmaceutical nanoparticles and atherosclerosis in aorta artery on the instable blood velocity based on numerical method. Int. J. Numer. Methods Biomed. Eng. 2021, 38, e3568. [Google Scholar] [CrossRef] [PubMed]
- Taebi, A. Deep Learning for Computational Hemodynamics: A Brief Review of Recent Advances. Fluids 2022, 7, 197. [Google Scholar] [CrossRef]





















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Artery | Diameter Measured in the Paper [mm] | Diameter Mentioned in References [mm] | References |
|---|---|---|---|
| Aorta (inlet section) | 22.00 | 14–30 | [29] |
| Celiac artery | 7.16 | 8.57 ± 1.57 | [30] |
| Superior mesenteric artery | 7.84 | 8.35 ± 1.60 | [30] |
| Left renal artery | 7.12 | 7.03 ± 1.40 | [30] |
| Right renal artery | 7.00 | 7.13 ± 1.20 | [30] |
| Inferior mesenteric artery | 4.04 | 4.21 ± 1.20 | [30] |
| Left iliac artery | 11.00 | 11.77 ± 2.20 | [30] |
| Right iliac artery | 10.90 | 12.23 ± 2.40 | [30] |
| Mesh | Number of Nodes (Total) | Number of Elements (Total) | Number of the Nodes Inlet Section | Number of Elements (Inlet Section) |
|---|---|---|---|---|
| Coarse (mesh#1) | 1,011,403 | 2,885,022 | 3156 | 4582 |
| Medium (mesh#2) | 1,951,507 | 6,566,740 | 4154 | 6386 |
| Fine (mesh#3) | 3,479,629 | 9,558,980 | 8072 | 13,784 |
| Cross-Section | Flow Rate [L/min] | Percentage Distribution [%] |
|---|---|---|
| Inlet | 5.644 | 100 |
| o1 | 0.043 | 0.76 |
| o2 | 0.071 | 1.25 |
| o3 | 0.076 | 1.35 |
| o4 | 0.153 | 2.72 |
| o5 | 0.092 | 1.63 |
| o6 | 0.101 | 1.78 |
| o7 | 0.077 | 1.37 |
| o8 | 0.057 | 1.01 |
| o9 | 0.133 | 2.35 |
| o10 | 0.175 | 3.10 |
| o11 | 0.102 | 1.82 |
| o12 | 0.063 | 1.11 |
| o13 | 0.237 | 4.20 |
| o14 | 0.045 | 0.80 |
| o15 | 2.228 | 39.48 |
| o16 | 1.991 | 35.28 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Totorean, A.-F.; Totorean, I.-C.; Bernad, S.I.; Ciocan, T.; Malita, D.C.; Gaita, D.; Bernad, E.S. Patient-Specific Image-Based Computational Fluid Dynamics Analysis of Abdominal Aorta and Branches. J. Pers. Med. 2022, 12, 1502. https://doi.org/10.3390/jpm12091502
Totorean A-F, Totorean I-C, Bernad SI, Ciocan T, Malita DC, Gaita D, Bernad ES. Patient-Specific Image-Based Computational Fluid Dynamics Analysis of Abdominal Aorta and Branches. Journal of Personalized Medicine. 2022; 12(9):1502. https://doi.org/10.3390/jpm12091502
Chicago/Turabian StyleTotorean, Alin-Florin, Iuliana-Claudia Totorean, Sandor Ianos Bernad, Tiberiu Ciocan, Daniel Claudiu Malita, Dan Gaita, and Elena Silvia Bernad. 2022. "Patient-Specific Image-Based Computational Fluid Dynamics Analysis of Abdominal Aorta and Branches" Journal of Personalized Medicine 12, no. 9: 1502. https://doi.org/10.3390/jpm12091502