
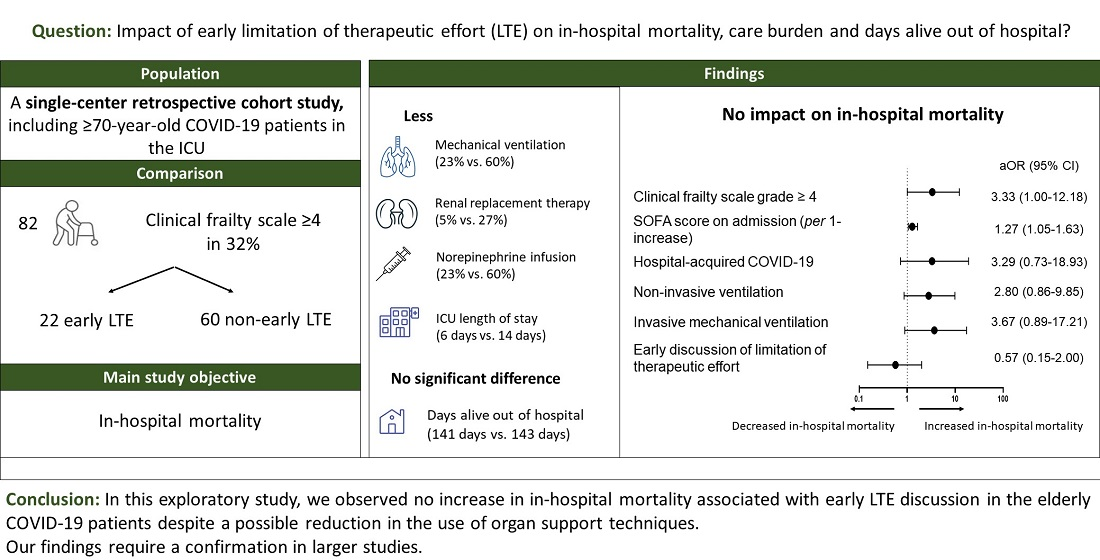
Impact of Early Limitation of Therapeutic Effort in Elderly COVID-19 Patients Admitted to the Intensive Care Unit—A Cohort Study
 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Management and LTE Discussion
2.3. Study Objectives
2.4. Data Collection and Parameter Definitions
2.5. Statistical Analysis
3. Results
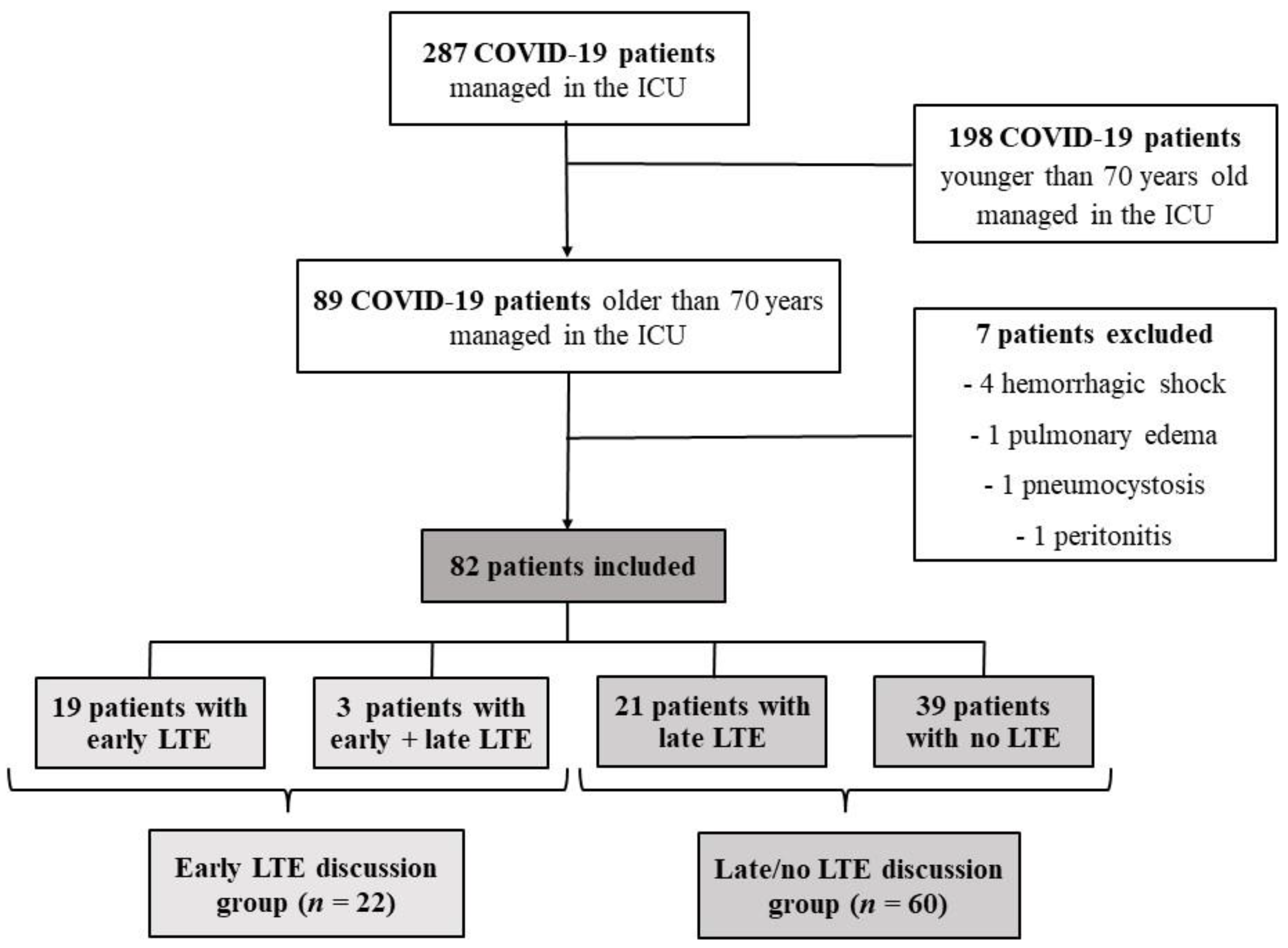
3.1. Patient Description
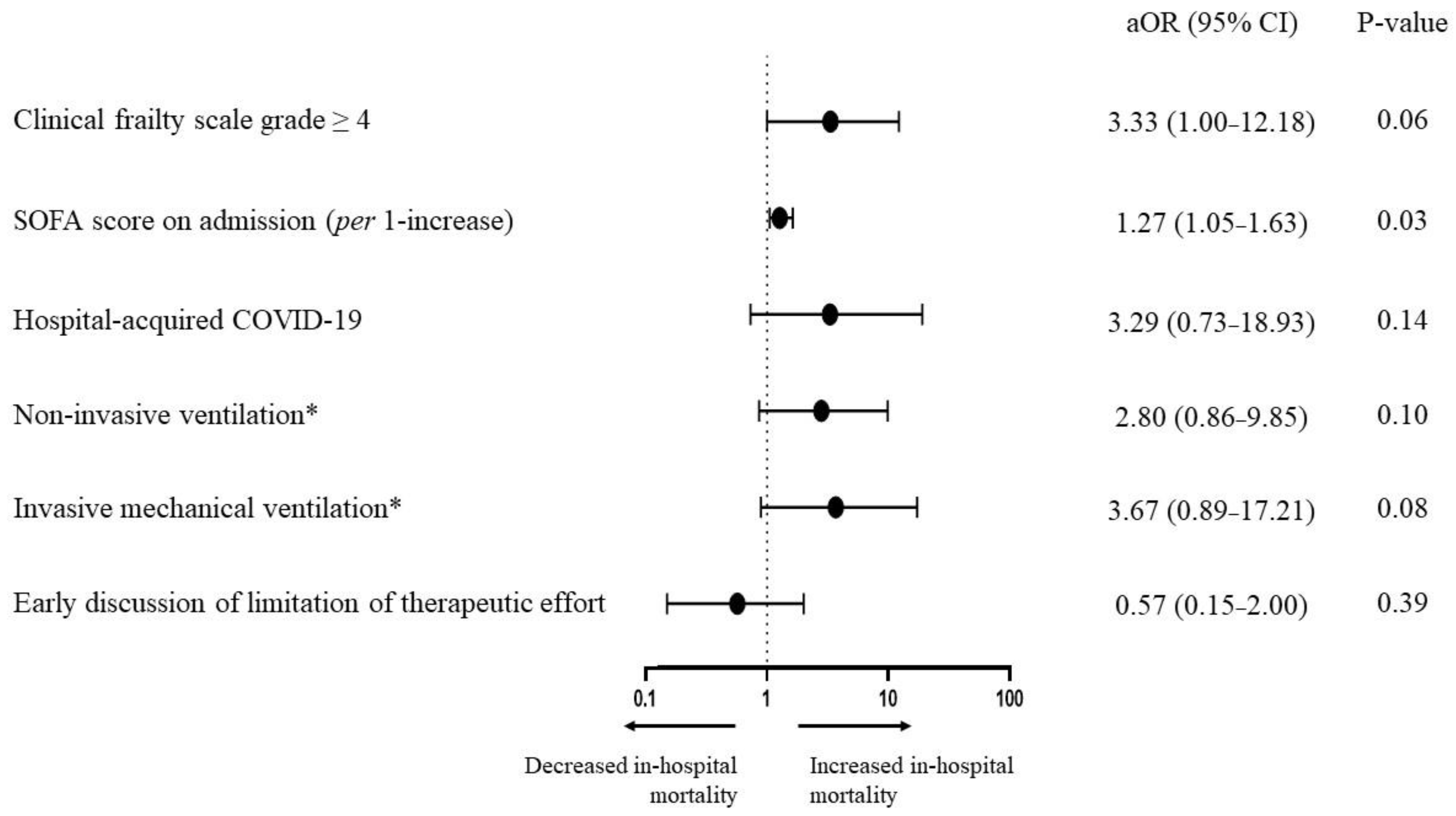
3.2. Prognostic Factors of In-Hospital Death
3.3. Characteristics of Patients with Early LTE Discussion
3.4. Impact of LTE Discussion on Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guidet, B.; Vallet, H.; Boddaert, J.; de Lange, D.W.; Morandi, A.; Leblanc, G.; Artigas, A.; Flaatten, H. Caring for the Critically Ill Patients over 80: A Narrative Review. Ann. Intensive Care 2018, 8, 114. [Google Scholar] [CrossRef] [PubMed]
- Correia, I.; Simas, Â.; Chaves, S.; Paixão, A.I.; Catarino, A.; Gonçalves-Pereira, J. The PALliative MUlticenter Study in Intensive Care (PalMuSIC). Results From a Multicenter Study Addressing Frailty and Palliative Care Interventions in Intensive Care Units in Portugal. J. Palliat. Care 2022, 37, 552–561. [Google Scholar] [CrossRef] [PubMed]
- Sprung, C.L.; Ricou, B.; Hartog, C.S.; Maia, P.; Mentzelopoulos, S.D.; Weiss, M.; Levin, P.D.; Galarza, L.; de la Guardia, V.; Schefold, J.C.; et al. Changes in End-of-Life Practices in European Intensive Care Units From 1999 to 2016. JAMA 2019, 322, 1692–1704. [Google Scholar] [CrossRef] [PubMed]
- Avidan, A.; Sprung, C.L.; Schefold, J.C.; Ricou, B.; Hartog, C.S.; Nates, J.L.; Jaschinski, U.; Lobo, S.M.; Joynt, G.M.; Lesieur, O.; et al. Variations in End-of-Life Practices in Intensive Care Units Worldwide (Ethicus-2): A Prospective Observational Study. Lancet Respir. Med. 2021, 9, 1101–1110. [Google Scholar] [CrossRef]
- Azoulay, É.; Beloucif, S.; Guidet, B.; Pateron, D.; Vivien, B.; Le Dorze, M. Admission Decisions to Intensive Care Units in the Context of the Major COVID-19 Outbreak: Local Guidance from the COVID-19 Paris-Region Area. Crit. Care Lond. Engl. 2020, 24, 293. [Google Scholar] [CrossRef]
- Fagard, K.; Gielen, E.; Deschodt, M.; Devriendt, E.; Flamaing, J. Risk Factors for Severe COVID-19 Disease and Death in Patients Aged 70 and over: A Retrospective Observational Cohort Study. Acta Clin. Belg. 2022, 77, 487–494. [Google Scholar] [CrossRef]
- Guillon, A.; Laurent, E.; Godillon, L.; Kimmoun, A.; Grammatico-Guillon, L. Long-Term Mortality of Elderly Patients after Intensive Care Unit Admission for COVID-19. Intensive Care Med. 2021, 47, 710–712. [Google Scholar] [CrossRef]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated With Mortality Among Patients With COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef]
- Grasselli, G.; Scaravilli, V.; Mangioni, D.; Scudeller, L.; Alagna, L.; Bartoletti, M.; Bellani, G.; Biagioni, E.; Bonfanti, P.; Bottino, N.; et al. Hospital-Acquired Infections in Critically-Ill COVID-19 Patients. Chest 2021, 160, 454–465. [Google Scholar] [CrossRef]
- Dres, M.; Hajage, D.; Lebbah, S.; Kimmoun, A.; Pham, T.; Béduneau, G.; Combes, A.; Mercat, A.; Guidet, B.; Demoule, A.; et al. Characteristics, Management, and Prognosis of Elderly Patients with COVID-19 Admitted in the ICU during the First Wave: Insights from the COVID-ICU Study: Prognosis of COVID-19 Elderly Critically Ill Patients in the ICU. Ann. Intensive Care 2021, 11, 77. [Google Scholar] [CrossRef]
- Jung, C.; Flaatten, H.; Fjølner, J.; Bruno, R.R.; Wernly, B.; Artigas, A.; Bollen Pinto, B.; Schefold, J.C.; Wolff, G.; Kelm, M.; et al. The Impact of Frailty on Survival in Elderly Intensive Care Patients with COVID-19: The COVIP Study. Crit. Care Lond. Engl. 2021, 25, 149. [Google Scholar] [CrossRef]
- Azoulay, E.; Metnitz, B.; Sprung, C.L.; Timsit, J.-F.; Lemaire, F.; Bauer, P.; Schlemmer, B.; Moreno, R.; Metnitz, P. SAPS 3 investigators End-of-Life Practices in 282 Intensive Care Units: Data from the SAPS 3 Database. Intensive Care Med. 2009, 35, 623–630. [Google Scholar] [CrossRef]
- Sprung, C.L.; Artigas, A.; Kesecioglu, J.; Pezzi, A.; Wiis, J.; Pirracchio, R.; Baras, M.; Edbrooke, D.L.; Pesenti, A.; Bakker, J.; et al. The Eldicus Prospective, Observational Study of Triage Decision Making in European Intensive Care Units. Part II: Intensive Care Benefit for the Elderly. Crit. Care Med. 2012, 40, 132–138. [Google Scholar] [CrossRef]
- Sprung, C.L.; Cohen, S.L.; Sjokvist, P.; Baras, M.; Bulow, H.-H.; Hovilehto, S.; Ledoux, D.; Lippert, A.; Maia, P.; Phelan, D.; et al. End-of-Life Practices in European Intensive Care Units: The Ethicus Study. JAMA 2003, 290, 790–797. [Google Scholar] [CrossRef]
- ARDS Definition Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar]
- Fan, E.; Del Sorbo, L.; Goligher, E.C.; Hodgson, C.L.; Munshi, L.; Walkey, A.J.; Adhikari, N.K.J.; Amato, M.B.P.; Branson, R.; Brower, R.G.; et al. An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2017, 195, 1253–1263. [Google Scholar] [CrossRef]
- Guérin, C.; Reignier, J.; Richard, J.-C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone Positioning in Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef]
- Villar, J.; Ferrando, C.; Martínez, D.; Ambrós, A.; Muñoz, T.; Soler, J.A.; Aguilar, G.; Alba, F.; González-Higueras, E.; Conesa, L.A.; et al. Dexamethasone Treatment for the Acute Respiratory Distress Syndrome: A Multicentre, Randomised Controlled Trial. Lancet Respir. Med. 2020, 8, 267–276. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar]
- LOI N° 2016-87 Du 2 Février 2016 Créant de Nouveaux Droits En Faveur Des Malades et Des Personnes En Fin de Vie (1); 2016; Légifrance. Available online: https://www.legifrance.gouv.fr/eli/loi/2016/2/2/AFSX1507642L/jo/texte (accessed on 7 September 2022).
- Cook, D.; Rocker, G. Dying with Dignity in the Intensive Care Unit. N. Engl. J. Med. 2014, 370, 2506–2514. [Google Scholar] [CrossRef]
- Lesieur, O.; Leloup, M.; Gonzalez, F.; Mamzer, M.-F. EPILAT study group Withholding or Withdrawal of Treatment under French Rules: A Study Performed in 43 Intensive Care Units. Ann. Intensive Care 2015, 5, 15. [Google Scholar] [CrossRef]
- Pan, F.; Ye, T.; Sun, P.; Gui, S.; Liang, B.; Li, L.; Zheng, D.; Wang, J.; Hesketh, R.L.; Yang, L.; et al. Time Course of Lung Changes at Chest CT during Recovery Coronavirus Disease 2019 (COVID-19). Radiology 2020, 295, 715–721. [Google Scholar] [CrossRef] [Green Version]
- Juma, S.; Taabazuing, M.-M.; Montero-Odasso, M. Clinical Frailty Scale in an Acute Medicine Unit: A Simple Tool That Predicts Length of Stay. Can. Geriatr. J. CGJ 2016, 19, 34–39. [Google Scholar] [CrossRef]
- Schneeweiss, S.; Wang, P.S.; Avorn, J.; Glynn, R.J. Improved Comorbidity Adjustment for Predicting Mortality in Medicare Populations. Health Serv. Res. 2003, 38, 1103–1120. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-Related Organ Failure Assessment) Score to Describe Organ Dysfunction/Failure. On Behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Kellum, J.A.; Levin, N.; Bouman, C.; Lameire, N. Developing a Consensus Classification System for Acute Renal Failure. Curr. Opin. Crit. Care 2002, 8, 509–514. [Google Scholar] [CrossRef]
- López Camps, V.; García García, M.A.; Martín Delgado, M.C.; Añón Elizalde, J.M.; Masnou Burrallo, N.; Rubio Sanchiz, O.; Estella García, A.; Monzón Marín, J.L. el Grupo de Trabajo de Bioética de la Sociedad Española de Medicina Intensiva Crítica y Unidades Coronarias National Survey on the Indicators of Quality in Bioethics of the SEMICYUC in the Departments of Intensive Care Medicine in Spain. Med. Intensiva 2017, 41, 523–531. [Google Scholar] [CrossRef]
- Curtis, J.R.; Vincent, J.-L. Ethics and End-of-Life Care for Adults in the Intensive Care Unit. Lancet Lond. Engl. 2010, 376, 1347–1353. [Google Scholar] [CrossRef]
- Detering, K.M.; Hancock, A.D.; Reade, M.C.; Silvester, W. The Impact of Advance Care Planning on End of Life Care in Elderly Patients: Randomised Controlled Trial. BMJ 2010, 340, c1345. [Google Scholar] [CrossRef]
- Prokopová, T.; Hudec, J.; Vrbica, K.; Stašek, J.; Pokorná, A.; Štourač, P.; Rusinová, K.; Kerpnerová, P.; Štěpánová, R.; Svobodník, A.; et al. Palliative Care Practice and Moral Distress during COVID-19 Pandemic (PEOpLE-C19 Study): A National, Cross-Sectional Study in Intensive Care Units in the Czech Republic. Crit. Care 2022, 26, 1–14. [Google Scholar] [CrossRef]
- Rubio, O.; Arnau, A.; Cano, S.; Subirà, C.; Balerdi, B.; Perea, M.E.; Fernández-Vivas, M.; Barber, M.; Llamas, N.; Altaba, S.; et al. Limitation of Life Support Techniques at Admission to the Intensive Care Unit: A Multicenter Prospective Cohort Study. J. Intensive Care 2018, 6, 24. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Overall (n = 82) | Non-Early LTE Discussion (n = 60) | Early LTE Discussion (n = 22) | p-Value | |
|---|---|---|---|---|
| Demographics | ||||
| Age, years | 78 (74–82) | 77 (73–79) | 83 (78–85) | <0.001 |
| Age > 80 years | 28 (34) | 13 (22) | 15 (68) | <0.001 |
| Male gender | 59 (72.0) | 43 (71.7) | 16 (72.7) | 1 |
| Body mass index, kg·m−2 | 27.1 (24.0–30.6) | 27.7 (24.2–31.0) | 25.2 (23.4–28.9) | 0.46 |
| Clinical frailty scale | 3 (2–4) | 3 (2–3) | 4 (3–6) | 0.004 |
| Clinical frailty scale ≥4 | 26 (32) | 15 (25) | 11 (50) | 0.048 |
| Comorbidities | ||||
| Hypertension | 56 (68) | 43 (72) | 13 (59) | 0.30 |
| Ischemic cardiomyopathy | 14 (17) | 10 (17) | 4 (18) | 1 |
| Chronic heart failure | 11 (13) | 6 (10) | 5 (23) | 0.16 |
| Chronic kidney disease | 15 (18) | 13 (22) | 2 (9) | 0.33 |
| Peripheral arterial disease | 5 (6) | 2 (3) | 3 (14) | 0.12 |
| Cerebrovascular disease | 6 (7) | 5 (8) | 1 (5) | 1 |
| COPD | 7 (9) | 5 (8) | 2 (9) | 1 |
| Diabetes mellitus | 31 (38) | 27 (45) | 4 (18) | 0.04 |
| End organ damage | 18 (22) | 16 (59) | 2 (50) | 1 |
| Connective tissue disease | 2 (2) | 1 (2) | 1 (5) | 0.47 |
| Gastro-intestinal peptic ulcer | 2 (2) | 2 (3) | 0 (0) | 1 |
| Cancer | 10 (12) | 5 (8) | 5 (23) | 0.12 |
| Metastasis | 2 (8) | 1 (2) | 1 (5) | 1 |
| Atrial fibrillation | 11 (13) | 5 (8.3) | 6 (27) | 0.06 |
| Charlson comorbidity index | 5 (4–6) | 4 (4–6) | 6 (4–6) | 0.03 |
| Charlson index null besides age | 24 (29) | 17 (28) | 7 (32) | 0.79 |
| Disease history and severity on ICU admission | ||||
| Hospitalization for COVID-19 | 67 (82) | 54 (90) | 13 (59) | 0.003 |
| Symptom onset to ICU, days | 8 (6–12) | 8 (6–12) | 9 (7–13) | 0.39 |
| Hospital to ICU admission, days | 2 (0–4) | 2 (0–4) | 2 (0–6) | 0.68 |
| Hospital-acquired COVID-19 | 15 (18) | 6 (10) | 9 (41) | 0.003 |
| Hospital to ICU admission, days | 20 (17–45) | 21 (19–37) | 20 (15–48) | 0.91 |
| Plasma D-dimer, mg/L | 1.58 (0.97–3.14) | 1.91 (1.10–3.48) | 1.28 (0.70–2.26) | 0.07 |
| Serum albumin, g/L | 26.3 (23.1–28.5) | 25.7 (23.0, 27.7) | 28.0 (25.8, 28.8) | 0.09 |
| CT-scan severity category | 4 (3–4) | 4 (3–4) | 4 (3–4) | 0.88 |
| CT-scan severity (categories 4 to 5) | 37/57 (65) | 29/44 (66) | 8/13 (62) | 0.75 |
| SOFA score | 4 (3–6) | 4 (3–6) | 4 (4–5) | 0.55 |
| Admission during first wave | 26 (32) | 18 (30) | 8 (36) | 0.60 |
| Respiratory support during the first hours | ||||
| Oxygen supply modalities | 0.05 | |||
| HFNO/conventional oxygen | 43 (52) | 33 (55) | 10 (46) | |
| Non-invasive ventilation | 22 (27) | 12 (20) | 10 (46) | |
| Invasive ventilation | 17 (21) | 15 (25) | 2 (9) | |
| PaO2/FiO2 ratio, mmHg | 114 (80–181) | 119 (91–192) | 100 (61–140) | 0.08 |
| Overall | Non-Early LTE Discussion | Early LTE Discussion | p-Value | |
|---|---|---|---|---|
| (n = 82) | (n = 60) | (n = 22) | ||
| Ventilation management | ||||
| Non-invasive ventilation | 36 (44) | 23 (38) | 13 (59) | 0.13 |
| Invasive mechanical ventilation | 44 (54) | 39 (65) | 5 (23) | 0.001 |
| Duration, days | 15.5 (9.0–25.8) | 16.0 (9.0–28.0) | 11.0 (11.0–13.0) | 0.33 |
| Prone positioning | 32/44 (73) | 29/39 (74) | 3/5 (60) | 0.60 |
| Nitric oxide | 13/44 (30) | 11/39 (28) | 2/5 (40) | 0.62 |
| Almitrine infusion | 3/44 (7) | 2/39 (6) | 1/5 (9) | 1 |
| ECMO | 1 (1) | 1 (2) | 0 (0) | 1 |
| Anti-COVID-19 therapies | ||||
| Dexamethasone | 68 (83) | 51 (85) | 17 (77) | 0.51 |
| 6 mg/day dose regimen | 54 (79) | 40 (78) | 14 (82) | 1 |
| 20 mg/day dose regimen | 28 (41) | 21 (41) | 7 (41) | 1 |
| Tocilizumab | 8 (10) | 4 (7) | 4 (18) | 0.20 |
| Critical care complications and outcome | ||||
| Acute kidney injury | 52 (63) | 40 (67) | 12 (55) | 0.44 |
| KDIGO-3 | 30 (37) | 25 (42) | 5 (23) | 0.13 |
| Renal replacement therapy | 17 (21) | 16 (27) | 1 (5) | 0.03 |
| Norepinephrine infusion | 41 (50) | 36 (60) | 5 (23) | 0.005 |
| Norepinephrine > 0.5 µg/kg/min | 23 (55) | 21 (58) | 2 (33) | 0.38 |
| Alive out of ICU | 38 (46) | 28 (47) | 10 (46) | 1 |
| ICU length of stay, days | 12 (6–21) | 14 (7–24) | 6 (2–12) | 0.001 |
| Alive out of hospital | 37 (45) | 28 (47) | 9 (41) | 0.80 |
| Hospital length of stay, days | 17 (10–34) | 20 (14–37) | 8 (4–20) | 0.001 |
| Need for rehabilitation in survivors | 13 (35) | 10 (36) | 3 (33) | 1 |
| Number of days alive out-of-hospital at day 180 | 0 (0–136) [n = 79] | 0 (0–139) [n = 57] | 0 (0–90) [n = 22] | 0.40 |
| Number of days alive out-of-hospital at day 180 among in-hospital survivors | 143 (119–161) | 143 (125–162) | 141 (90–155) | 0.34 |
| Therapeutic burden | 34 (42) | 29 (48) | 4 (18) | 0.01 |
| Survivors (n = 37) | Non-Survivors (n = 45) | OR (95% CI) | p-Value | |
|---|---|---|---|---|
| Demographics | ||||
| Age, (per 1-increase) | 77 (74–80) | 78 (74–83) | 1.05 (0.97–1.15) | 0.24 |
| Age, >80 years | 9 (24) | 19 (42) | 2.27 (0.89–6.12) | 0.09 |
| Male gender | 26 (70) | 33 (73) | 1.16 (0.44–3.07) | 0.76 |
| CFS (per 1-increase) | 3 (2–3) | 3 (2–4) | 1.19 (0.89–1.64) | 0.25 |
| CFS grade ≥ 4 | 8 (22) | 18 (40) | 2.42 (0.93–6.74) | 0.08 |
| Charlson null besides age | 11 (30) | 13 (29) | 0.96 (0.37–2.53) | 0.93 |
| Disease history and severity on admission | ||||
| Hospital-acquired COVID-19 | 3 (8) | 12 (27) | 4.12 (1.18–19.30) | 0.04 |
| Serum albumin < 26.3 g/L | 17 (57) | 16 (43) | 0.58 (0.22–1.53) | 0.27 |
| Plasma D-dimer, mg/L | 1.99 (0.99–3.30) | 1.47 (0.98–2.89) | 0.99 (0.90–1.10) | 0.86 |
| SOFA score (per 1-increase) | 3.0 (3.0–4.0) | 4.0 (4.0–7.0) | 1.28 (1.07, 1.60) | 0.01 |
| CT scan extension > 50% | 17/25 (68) | 20/32 (63) | 0.78 (0.25–2.35) | 0.66 |
| Admission during first wave | 12 (32) | 14 (31) | 0.91 (0.49, 1.71) | 0.77 |
| Respiratory support during the first hours | ||||
| Oxygen supply modality | 0.08 | |||
| HFNO/conventional oxygen | 25 (68) | 18 (40) | 1 | |
| Non-invasive ventilation | 8 (22) | 14 (31) | 2.43 (0.86–7.27) | |
| Mechanical ventilation | 4 (11) | 13 (29) | 4.51 (1.45–18.16) | |
| PaO2/FiO2 ratio *, mmHg | 143 (82–192) | 106 (72–163) | 1.03 (0.64–1.69) | 0.91 |
| Management and complications in the ICU | ||||
| Dexamethasone | 30 (81) | 38 (85) | 1.27 (0.39–4.09) | 0.69 |
| Invasive mechanical ventilation | 12 (32) | 32 (71) | 5.13 (2.05–13.61) | <0.001 |
| Prone positioning | 5/12 (42) | 27/32 (84) | 7.56 (1.77–36.65) | 0.01 |
| Nitric oxide | 0/12 | 13/32 (41) | NA ** | 0.009 |
| Acute kidney injury KDIGO-3 | 4 (11) | 26 (58) | 11.29 (3.73–42.77) | <0.001 |
| Renal replacement therapy | 2 (5) | 15 (33) | 8.75 (2.23–58.41) | 0.006 |
| Norepinephrine infusion | 8 (22) | 33 (73) | 9.97 (3.73–29.35) | <0.001 |
| Norepinephrine > 0.5 µg/kg/min | 1/8 (11) | 22/33 (67) | 16.00 (2.49–316.87) | 0.01 |
| Limitation of therapeutic effort | ||||
| Early LTE | 9 (24) | 13 (29) | 1.26 (0.47–3.49) | 0.64 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lacoste-Palasset, T.; Sutterlin, L.; M’Rad, A.; Modestin, L.; Mourman, V.; Pepin-Lehalleur, A.; Malissin, I.; Naim, G.; Grant, C.; Guérin, E.; et al. Impact of Early Limitation of Therapeutic Effort in Elderly COVID-19 Patients Admitted to the Intensive Care Unit—A Cohort Study. J. Pers. Med. 2022, 12, 1501. https://doi.org/10.3390/jpm12091501
Lacoste-Palasset T, Sutterlin L, M’Rad A, Modestin L, Mourman V, Pepin-Lehalleur A, Malissin I, Naim G, Grant C, Guérin E, et al. Impact of Early Limitation of Therapeutic Effort in Elderly COVID-19 Patients Admitted to the Intensive Care Unit—A Cohort Study. Journal of Personalized Medicine. 2022; 12(9):1501. https://doi.org/10.3390/jpm12091501
Chicago/Turabian StyleLacoste-Palasset, Thomas, Laetitia Sutterlin, Aymen M’Rad, Louis Modestin, Vianney Mourman, Adrien Pepin-Lehalleur, Isabelle Malissin, Giulia Naim, Caroline Grant, Emmanuelle Guérin, and et al. 2022. "Impact of Early Limitation of Therapeutic Effort in Elderly COVID-19 Patients Admitted to the Intensive Care Unit—A Cohort Study" Journal of Personalized Medicine 12, no. 9: 1501. https://doi.org/10.3390/jpm12091501