1. Introduction
Hydrogel scleral buckles (HSB) were first introduced as an alternative to silicone buckles for treatment of rhegmatogenous retinal detachment in the 1980s and are thought to possess better softness and elasticity. Softness increase comfort and decreases the rate of scleral erosion and protrusion. Elasticity and mild hydration of hydrogel in the tissue could fill the dead space between the eyeball and the surrounding tissue. In addition, this material in the past was thought to absorb and slowly release antibiotics, further preventing bacterial growth [
1]. Complications associated with this material have been reported due to hydrophilic degradation, causing swelling, extrusion, intraocular intrusion, strabismus, infection, bony erosion, and even globe loss [
2,
3,
4,
5,
6,
7,
8,
9]. It was gradually removed from the market in the 1990s.
Many patients developed HSB-related complications decades after implantation. Some of the cases were initially diagnosed with thyroid-associated orbitopathy, idiopathic orbital fibrosis, orbital tumors, conjunctival cysts, or neurological disorders [
4,
6,
10,
11]. Removal of this brittle material was challenging due to its fragile characteristics and the surrounding adhesion to ocular tissue due to fibrosis. The perforation rate during surgery can be as high as 18% [
3]. For surgeons who were unfamiliar with this material, incomplete removal, recurrent retinal detachment (up to 29.4%), scleral rupture (up to 17.6%) and other surgical associated complications can occur [
3,
6].
In this study, we investigated the various clinical manifestations of delayed complications of swollen HSB and shared our surgical techniques to avoid the severe complications associated with manipulations.
2. Materials and Methods
We collected all patients with late HSB complications who underwent surgery for HSB removal in Taipei Veterans General Hospital, a tertiary medical center, from 2004 to 2021. Age, sex, time interval between HSB implantation and removal, presenting symptoms, initial diagnosis, clinical findings, surgical technique, intraoperative findings, and outcome were retrospectively reviewed.
Intraocular pressure (IOP) change was defined as the change in IOP before surgery and one month after surgery. The reason we chose IOP one month postoperatively for comparison is that post-operative tissue edema usually subsides at this time. IOP reduction was defined as a >20% IOP decrease compared to pre-operative IOP.
Location of HSB was categorized into groups according to the relative location to the globe equator in orbit-computed tomography (CT): anterior-located and posterior-located HSB. Anterior-located HSB were defined as more than 50% of HSB coverage anterior to the globe equator in sagittal cut, while the others were defined as posterior-located HSB.
SPSS statistical software version 22.0 (IBM corp., Armonk, NY, USA) was used for data management and statistical analysis. Categorical and paired continuous data were compared using the Fisher’s exact test and Wilcoxon Signed ranks test, respectively.
3. Results
In total, we collected eleven cases;
Table 1 summarizes the clinical data. One patient had bulbar atrophy before the diagnosis of swollen HSB (
Figure 1).
Table 2 shows the presenting symptoms of the patients. The symptoms included limitation of extraocular movement (ten eyes, 90.9%), ocular redness (eight eyes, 72.7%), ocular fullness (eight eyes, 72.7%), pain (six eyes, 54.5%), and exposed ocular foreign body (five eyes, 45.5%). Six patients (54.5%) received a correct diagnosis when referred to the medical center. Initial diagnoses other than swollen HSB included eyeball rupture (one eye, 9.1%), and orbital tumor (four eyes, 36.4%). Six patients (54.5%) had glaucoma in the diseased eyes and were treated with at least one combined form or two antiglaucoma medications before orbital HSB swelling was found. Four patients (66.7%) were male, but there was no significance of sex and glaucoma correlation according to Chi-Square analysis (
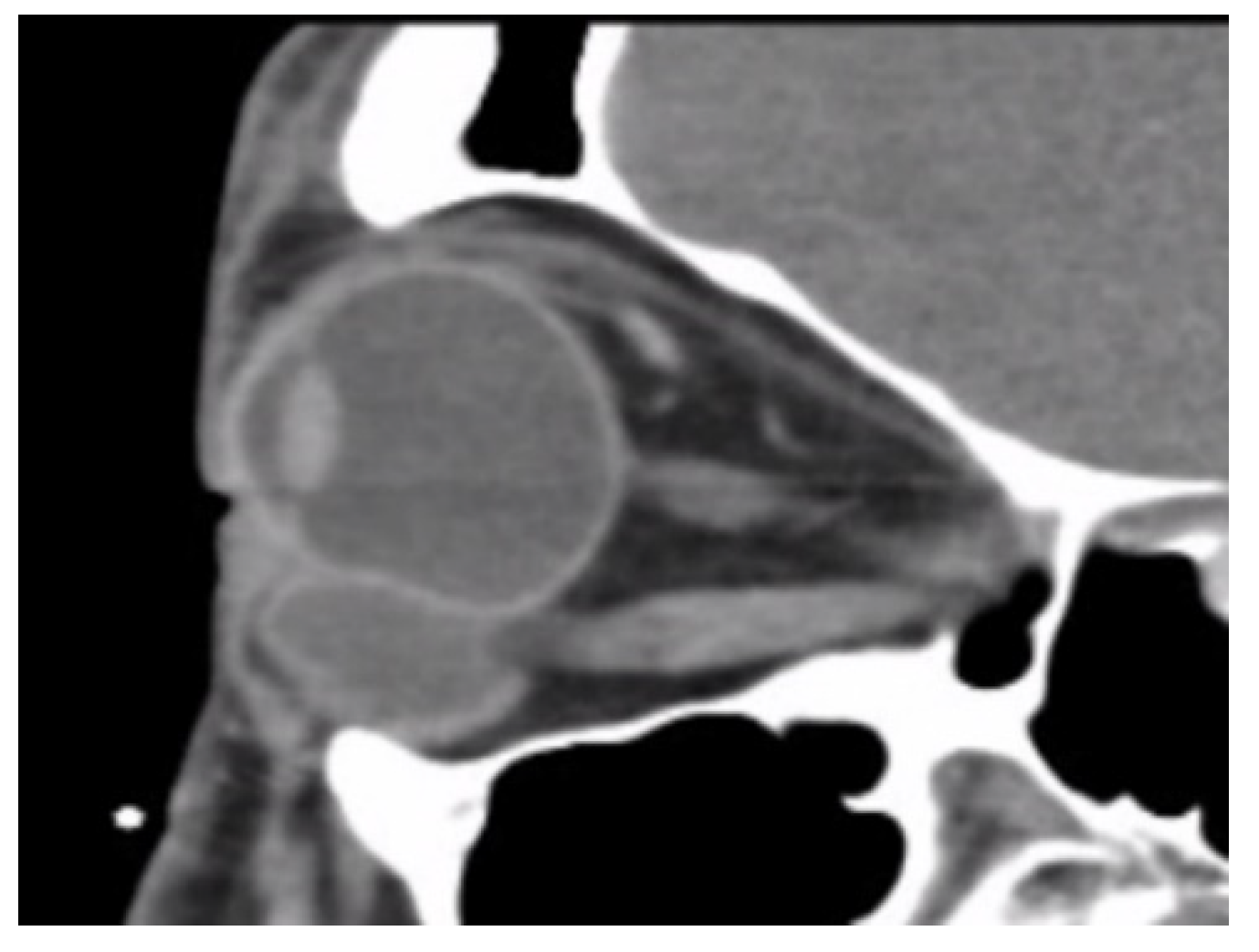
p = 0.652). In the six patients with glaucoma, four cases had inadequate IOP control and one case received minimally invasive glaucoma surgery due to uncontrolled IOP one year before HSB removal. New onset of limitations of extraocular movement prompted the doctors to survey for orbital lesions. The typical CT image finding of HSB is a circumferential and homogenous mass around the globe. As this material usually swells when it absorbs water and forms a pseudocapsule around itself, CT images show an isointense signal with a vitreous and non-infiltrative lesion that deforms the eyeball. A scattered, and hyperintense signal, which corresponds to calcific change, can also be found around the swollen HSB (
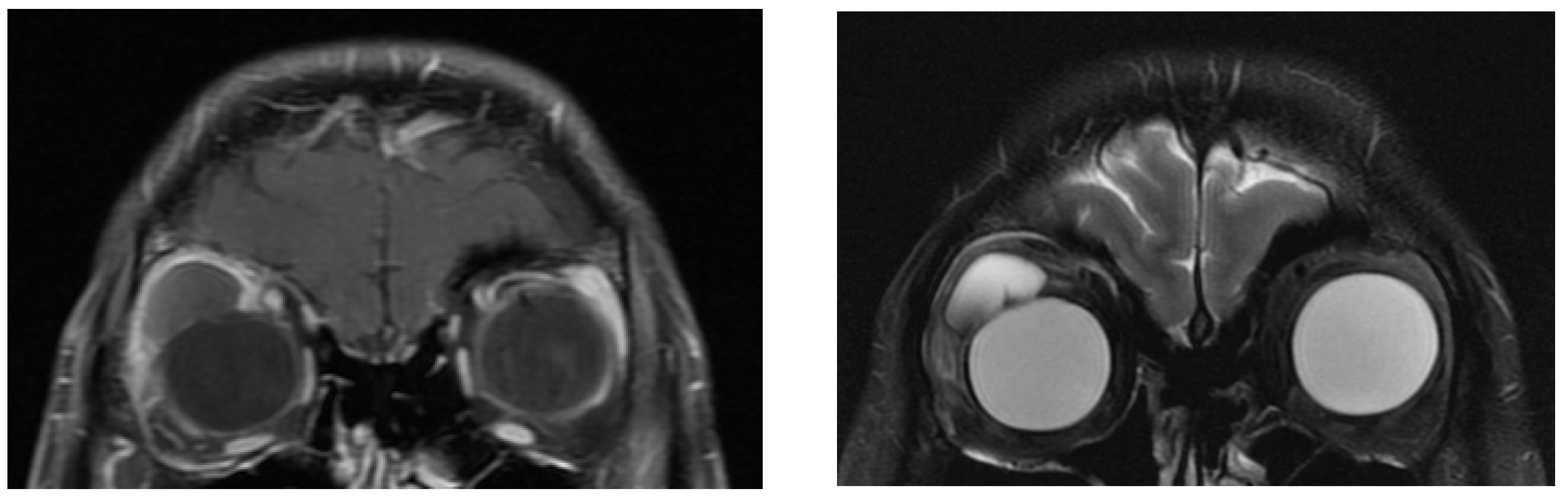
Figure 2). In MRI study, the HSB usually show hypointensity in T1-weighted images and hyperintensity in T2-weighted images, as these materials absorb water (
Figure 3). According to the location of HSB in orbital CT, we categorized the HSB coverage into two groups: anterior-located (
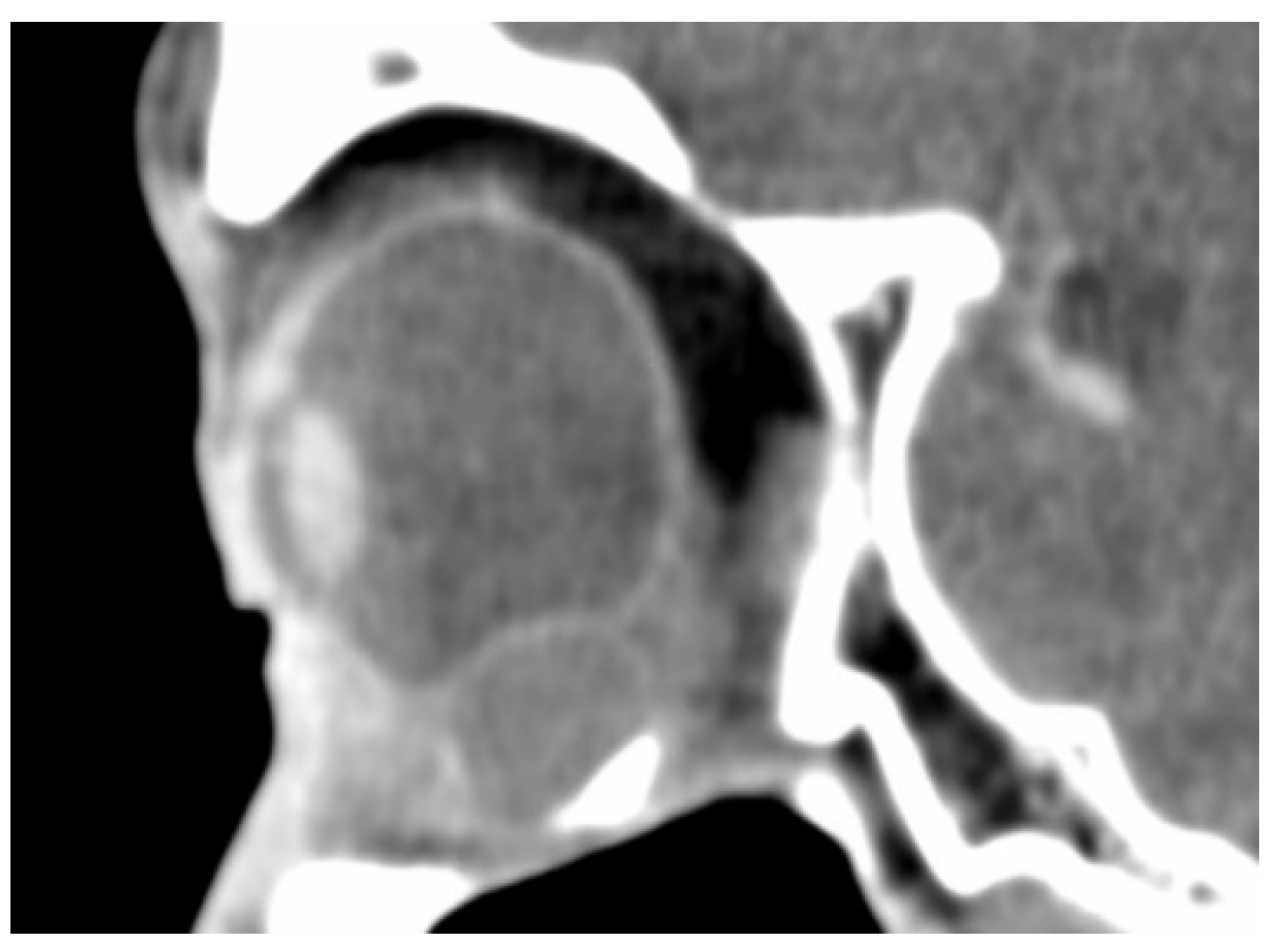
Figure 4) and posterior-located HSB (
Figure 5). In the six patients with glaucoma, four (66.7%) showed posterior-located HSB. However, Fisher’s exact test of the relationship between the posterior-located HSB and glaucoma diagnosis did not reach clinical significance (
p = 0.061).
All cases’ HSB were finally removed through one external conjunctival wound if the HSB could be easily approached anteriorly, or through one skin wound if the HSB were posteriorly located.
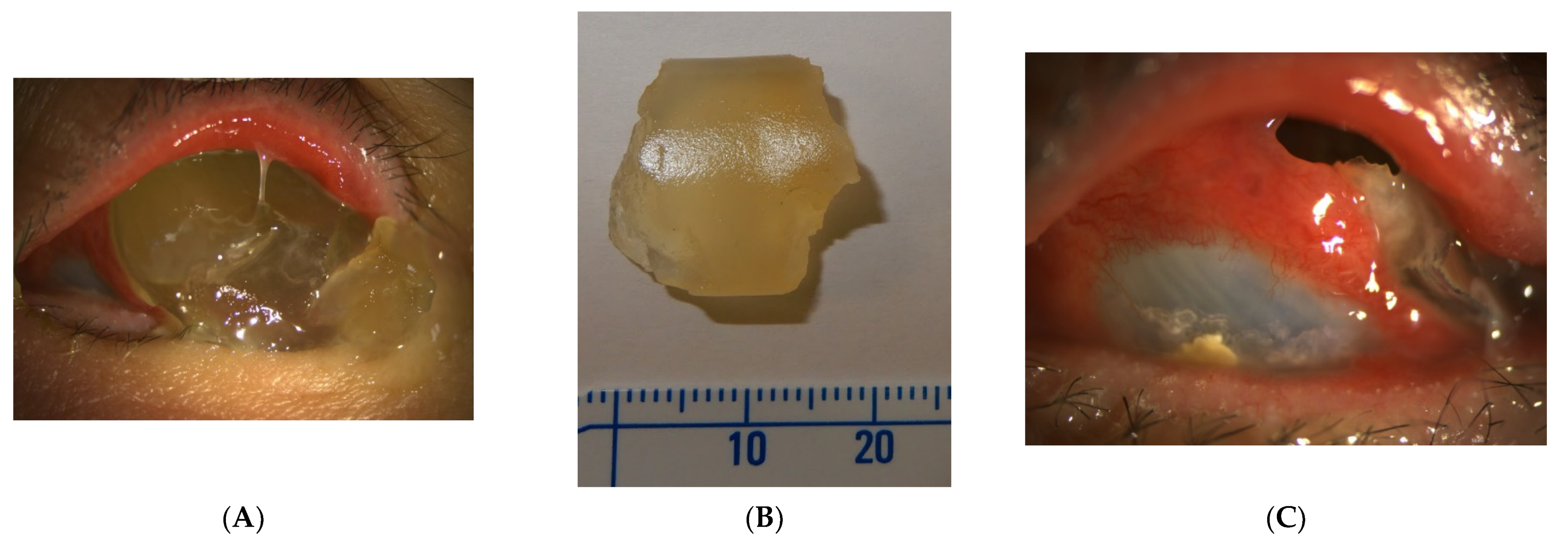
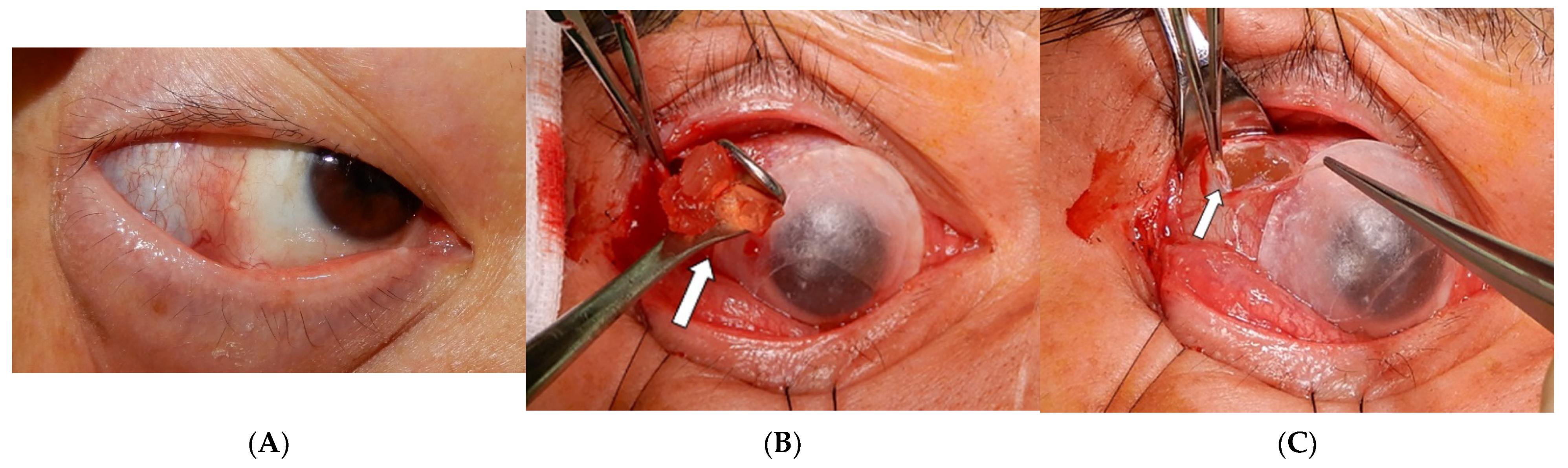
Table 3 summarized the surgical approach of the study cases. Lateral canthotomy was suggested to better expose the surgical field. This jelly-like hydrogel was fragile and can easily be broken into pieces in an attempt to remove it. We used blunt instruments such as muscle hooks or a Desmarres lid retractor to scoop out rather than grab the swelling buckles (
Figure 6A,B). A pseudocapsule was usually found during the dissection of orbital space (
Figure 6C). Surgeons preferred not to dissect further, as removal of the HSB inside the pseudocapsule was adequate.
At the end of surgery, irrigation of the empty space with antibiotics and steroids was performed to prevent infection and decrease inflammation, respectively. The HSB were safely removed in all patients. Evisceration was performed in addition to HSB removal in one case due to severe orbital cellulitis. In the surgical field, no implants were found other than HSB. No intraoperative scleral rupture was noted. There was no endophthalmitis, recurrence of retinal detachment, delayed bleeding or associated complications found in the follow-up period after surgery.
After removal of the HSB, ocular symptoms improved in most cases (
Table 2). However, a small residual degree of eye movement limitation was found in two cases. No patients received further strabismus surgery. In the six glaucoma patients, four of them showed IOP improvement one month after HSB removal. There was no change of antiglaucoma medication during this period. However, there was no statistical significance of IOP change before and after HSB removal in the ten cases using Wilcoxon signed ranks test (
p = 0.189,
Table 4).
4. Discussion
HSB absorb tissue fluids and progressively expand over the decades. The swelling of hydrogel itself has a mass effect on the orbital area, causing compression of the globe. HSB can cause inflammation and fibrosis of the surrounding tissue, and a pseudocapsule usually forms to enclose the hydrogel. If the material distends to a greater extent, it can intrude into the sclera or conjunctiva, or extrude from the orbit [
2,
4,
10]. Delayed HSB complications associated with implant swelling and protrusion are usually found from 54 to 284 months after surgery [
3]. The indications to remove the implant include pain, ocular discomfort, ocular inflammation, cosmetic concerns and diplopia [
3,
6]. In our patient group, the most common symptom was limitations of extraocular movement. The most severe complication of HSB in our study was the marked extension of hydrogel within the orbit, leading to compression, extrusion, and orbital cellulitis in one case. Ocular redness was thought to be caused by an immune reaction to the exposed foreign body. Strabismus was possibly due to myotoxicity, adhesion and scarring [
12]. Strabismus can develop after all kinds of scleral buckle implants in around 5–25% of patients in the long term [
12,
13]. However, HSB-related strabismus has been reported in up to 29% of patients in the previous literature, probably due to its evident mass effect, displacing the ocular content and muscles [
3]. As expanded HSB can cause a distinct bulky effect and more severe ocular motility disturbance, the removal of expanded HSB is helpful in reducing the extent of diplopia and the following strabismus surgery.
Incorrect initial diagnosis can lead to incomplete removal and increase iatrogenic complications for unprepared surgeons [
4,
10]. In our study, four patients (36.4%) were initially diagnosed as having an orbital tumor when they were referred to us. Surgeons who were not familiar with HSB removal may not be able to remove this fragile material safely. The rate of unexpected perforation during surgery ranges from 5.3% to 17.6% [
3,
6,
7]. A comprehensive exam of the retina and supplemental retinal laser may be needed before the operation. Recurrent retinal detachment can occur in from 5.3% to 29.4% of patients after HSB removal [
3,
6,
7]. Endophthalmitis, corneal edema, glaucoma, and scleral necrosis were also reported as complications of removal surgery [
6,
7].
A proper surgical approach is essential to extract the brittle hydrogel smoothly and avoid disturbing ocular structures. Although the previous literature mentions extensive peritomy, a cryo-assisted approach [
14], suction traction [
15], or the use of boric acid [
16], we use a relatively simple means of removing HSB. An extensive peritomy can result in scleral perforation when dissecting the periocular tissue. Further adhesion and scarring of tissue could ensue. Compression of the globe during manipulation may cause recurrent retinal detachment while the HSB are removed. In contrast, we make a relatively small wound around the skin or fornix and lateral canthotomy to better expose the surgical field. This external approach near the orbital ring can further make a tunnel to the target implant. Usually, the implant is enclosed by a pseudocapsule. The jelly-like material can be extracted with blunt instruments such as a Desmarres lid retractor or muscle hook through the tunnel (
Figure 6). At the end of surgery, irrigating the space with steroids and antibiotics may decrease the degree of inflammation and rate of infection.
It is worth mentioning that none of the previous studies mentioned glaucoma status or refractory IOP before removal of the implant. In our study, six patients had glaucoma, and four of them had inadequate IOP control. There are two possible explanations for this. First, these patients had a longer interval between HSB implantation surgery and removal, ranging from 26 to 30 years. Previous large-population studies documented the interval between implantation and removal from 8 to 23 years [
3,
6,
17]. With an extended period in our study, pathological changes in periorbital tissue such as fibrotic change, impaired ocular circulation and ocular compression, can play a role in glaucomatous development. Another explanation is that the relative location and degrees of HSB coverage may influence the development of glaucoma. Four out of the six cases with glaucoma in our study showed HSB coverage posterior to the equator. Compared to the anterior location, posteriorly located HSB cannot release the swelling pressure through protrusion of the orbital exit. Previous studies documented the degrees of HSB coverage but not the relative location to the equator. Roldán-Pallarés et al. followed up 415 cases with hydrogel implantation for up to seven years [
17]. More than half of the patients received HSB coverage over 180 degrees, and 45% of the patients had 360-degree encircling HSB coverage. None of these patients reported elevated IOP or glaucoma status, but unspecified orbital fullness was noted in only six cases. These may imply that the relative location compared to the globe equator, not the range of HSB coverage, may be the key factor that influences IOP. The relationship between IOP elevation and the location of swelling HSB must be proven through further studies.
5. Conclusions
Although HSB had not been used for more than 30 years, delayed complications associated with this material still emerged in recent years. Patients could present with various clinical manifestations. A detailed history, examination, and image findings are the keys to correct diagnosis and proper removal of the implant. In our study, an external approach was proved to be a safe way to remove HSB. Blunt instruments are suggested to prevent inadvertent perforation. Early diagnosis and meticulous management are essential to avoid severe sequelae in these patients.
Author Contributions
H.-Y.Y., W.-K.Y. and C.-C.T. helped with data collection. H.-Y.Y. wrote the main manuscript text. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The protocol was approved by the Institutional Review Board of Taipei Veterans General Hospital and supervised by “the Institutional Review Board of Taipei Veterans General Hospital”. After a review by Human Research Protection Center, the implementation of the protocol was approved. All the methods were carried out in accordance with relevant guidelines and regulations, and informed consent was obtained from all participants in the study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Das, T.; Namperumalsamy, P. Scleral buckling with hydrogel implant. Indian J. Ophthalmol. 1991, 39, 41–43. [Google Scholar] [PubMed]
- Bernardino, C.R.; Mihora, L.D.; Fay, A.M.; Rubin, P.A. Orbital complications of hydrogel scleral buckles. Ophthalmic Plast. Reconstr. Surg. 2006, 22, 206–208. [Google Scholar] [CrossRef] [PubMed]
- Crama, N.; Klevering, B.J. The Removal of Hydrogel Explants: An Analysis of 467 Consecutive Cases. Ophthalmology 2016, 123, 32–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czyz, C.N.; Petrie, T.P.; Everman, K.R.; Cahill, K.V.; Foster, J.A. Hydrogel explant extrusion masquerading as a malignant eyelid lesion. Ophthalmic Plast. Reconstr. Surg. 2013, 29, e25–e27. [Google Scholar] [CrossRef] [PubMed]
- Figueira, E.C.; Francis, I.C.; Wilcsek, G.A. Scleral MIRAgel causing bony orbital erosion. Orbit 2007, 26, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Kearney, J.J.; Lahey, J.M.; Borirakchanyavat, S.; Schwartz, D.M.; Wilson, D.; Tanaka, S.C.; Robins, D. Complications of hydrogel explants used in scleral buckling surgery. Am. J. Ophthalmol. 2004, 137, 96–100. [Google Scholar] [CrossRef]
- Le Rouic, J.F.; Bettembourg, O.; D’Hermies, F.; Azan, F.; Renard, G.; Chauvaud, D. Late swelling and removal of Miragel buckles: A comparison with silicone indentations. Retina 2003, 23, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Roh, M.; Lee, N.G.; Miller, J.B. Complications Assoicated with MIRAgel for Treatment of Retinal Detachment. Semin. Ophthalmol. 2018, 33, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Rubinstein, T.J.; Choudhary, M.M.; Modi, Y.S.; Ehlers, J.P.; Perry, J.D. Globe Loss from Intraocular Invasion of MIRAgel Scleral Buckle Components. Ophthalmic Plast. Reconstr. Surg. 2016, 32, 329–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shields, C.L.; Demirci, H.; Marr, B.P.; Mashayekhi, A.; Materin, M.A.; Shields, J.A. Expanding MIRAgel scleral buckle simulating an orbital tumor in four cases. Ophthalmic Plast. Reconstr. Surg. 2005, 21, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Sadaka, A.; Ortiz, J.; Berry, S.; Lee, A.G.; Li, H.K.; Divatia, M.; Malik, A. Late proptosis and ophthalmoplegia from hydrogel scleral buckle. Can. J. Ophthalmol. J. Can. d’ophtalmologie 2018, 53, e190–e193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farr, A.K.; Guyton, D.L. Strabismus after retinal detachment surgery. Curr. Opin. Ophthalmol. 2000, 11, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Rabinowitz, R.; Velez, F.G.; Pineles, S.L. Risk factors influencing the outcome of strabismus surgery following retinal detachment surgery with scleral buckle. J. Am. Assoc. Pediatric Ophthalmol. Strabismus 2013, 17, 594–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Rouic, J.F.; Bejjani, R.; Azan, F.; Bettembourg, O.; Renard, G.; Chauvaud, D. Cryoextraction of episcleral Miragel® buckle elements: A new technique to reduce fragmentation. Ophthalmic Surg. Lasers 2002, 33, 237–239. [Google Scholar] [CrossRef] [PubMed]
- Richards, A.L.; Meyer, D.R. Late complications of hydrogel scleral buckle implants and a technique for effective removal. Ophthalmic Plast. Reconstr. Surg. 2012, 28, 455–458. [Google Scholar] [CrossRef] [PubMed]
- Roldán-Pallarés, M.; Avila, M.I.; Refojo, M.F. The use of boric acid solution to help in the removal of biodegraded Miragel episcleral buckles. Retina 2005, 25, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Roldán-Pallarés, M.; Hernández-Montero, J.; Llanes, F.; Fernández-Rubio, J.E.; Ortega, F. MIRAgel: Hydrolytic degradation and long-term observations. Arch. Ophthalmol. 2007, 125, 511–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}