
The Feasibility of Ultra-Sensitive Phonocardiography in Acute Chest Pain Patients of a Tertiary Care Emergency Department (ScorED Feasibility Study)

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Data Acquisition
2.2. Data Analysis
3. Results
4. Discussion
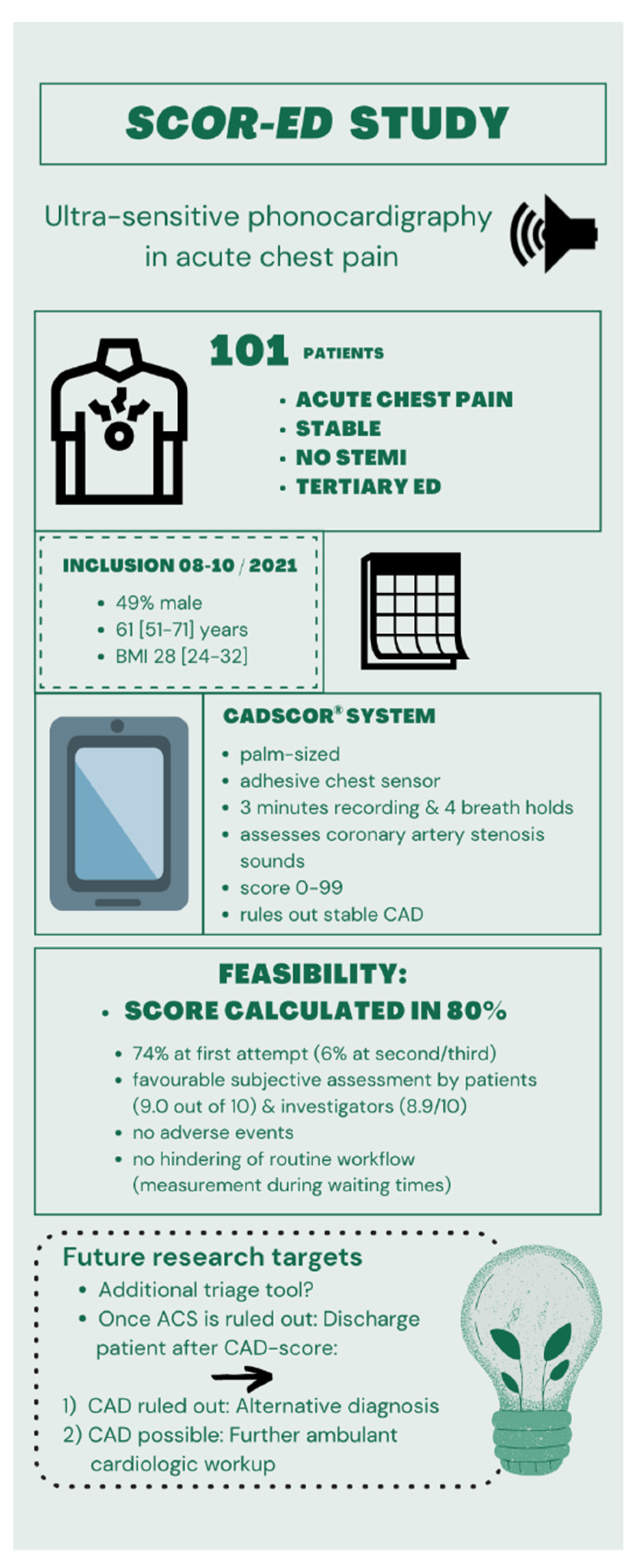
- Ultra-sensitive phonocardiography in chest pain patients presenting to an emergency department is feasible.
- The CAD score is already utilized to rule out stable coronary artery disease.
- After having ruled out acute coronary syndrome via a guideline-directed algorithm, the CADScor®System could help to classify chest pain patients into those with and without coronary artery disease, making a specific further cardiovascular workup possible.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Vrints, C.J. Update on the emergency department diagnosis and risk stratification of acute chest pain. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Wertli, M.M.; Dangma, T.D.; Müller, S.E.; Gort, L.M.; Klauser, B.S.; Melzer, L.; Held, U.; Steurer, J.; Hasler, S.; Burgstaller, J.M. Non-cardiac chest pain patients in the emergency department: Do physicians have a plan how to diagnose and treat them? A retrospective study. PLoS ONE 2019, 14, e0211615. [Google Scholar] [CrossRef] [Green Version]
- Azimpour, F.; Caldwell, E.; Tawfik, P.; Duval, S.; Wilson, R.F. Audible Coronary Artery Stenosis. Am. J. Med. 2016, 129, 515–521.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, S.E.; Hansen, J.; Zimmermann, H.; Hammershøi, D.; Toft, E.; Struijk, J. Coronary artery disease and low frequency heart sound signatures. Comput. Cardiol. 2011, 38, 481–484. [Google Scholar]
- Semmlow, J.; Rahalkar, K. Acoustic Detection of Coronary Artery Disease. Annu. Rev. Biomed. Eng. 2007, 9, 449–469. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.L.; Winther, S.; Wilson, R.F.; Bøttcher, M. A novel approach to diagnosing coronary artery disease: Acoustic detection of coronary turbulence. Int. J. Cardiovasc. Imaging 2017, 33, 129–136. [Google Scholar] [CrossRef]
- Schnaubelt, S.; Domanovits, H.; Niederdoeckl, J.; Schuetz, N.; Cacioppo, F.; Oppenauer, J.; Spiel, A.O.; Laggner, A.N. The Impact of the COVID-19 Pandemic on Incidences of Atrial Fibrillation and Electrical Cardioversion at a Tertiary Care Emergency Department: An Inter- and Intra-year Analysis. Front. Med. 2020, 7, 595881. [Google Scholar] [CrossRef]
- Behringer, W.; Dodt, C.; Eisenburger, P.; Laggner, A.N. Aspects of intensive care medicine in emergency medicine. Med. Klin. Intensivmed. Notfmed. 2020, 115, 625–632. [Google Scholar] [CrossRef]
- Winther, S.; Schmidt, S.E.; Holm, N.R.; Toft, E.; Struijk, J.J.; Bøtker, H.E.; Bøttcher, M. Diagnosing coronary artery disease by sound analysis from coronary stenosis induced turbulent blood flow: Diagnostic performance in patients with stable angina pectoris. Int. J. Cardiovasc. Imaging 2015, 32, 235–245. [Google Scholar] [CrossRef] [Green Version]
- Winther, S.; Nissen, L.; Schmidt, S.E.; Westra, J.; Rasmussen, L.D.; Knudsen, L.L.; Madsen, L.H.; Johansen, J.K.; Larsen, B.S.; Struijk, J.; et al. Diagnostic performance of an acoustic-based system for coronary artery disease risk stratification. Heart 2017, 104, 928–935. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.E.; Winther, S.; Larsen, B.S.; Groenhoej, M.H.; Nissen, L.; Westra, J.; Frost, L.; Holm, N.R.; Mickley, H.; Steffensen, F.H.; et al. Coronary artery disease risk reclassification by a new acoustic-based score. Int. J. Cardiovasc. Imaging 2019, 35, 2019–2028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindner, G.; Woitok, B.K. Emergency department overcrowding: Analysis and strategies to manage an international phenomenon. Wien. Klin. Wochenschr. 2021, 133, 229–233. [Google Scholar] [CrossRef] [PubMed]
- van der Linden, M.C.; Meester, B.E.; van der Linden, N. Emergency department crowding affects triage processes. Int. Emerg. Nurs. 2016, 29, 27–31. [Google Scholar] [CrossRef]
- Basu, S.; Harris, A.; Mason, S.; Norman, J. A longitudinal assessment of occupational stress in Emergency Department Nursing Staff. J. Nurs. Manag. 2019, 28, 167–174. [Google Scholar] [CrossRef]
- Schwartz, M.P. Office or Emergency Department: What’s the difference? South. Med. J. 1995, 88, 1020–1024. [Google Scholar] [CrossRef]
- Janicki, A.J.; Frisch, S.O.; Patterson, P.D.; Brown, A.; Frisch, A. Emergency Medicine Residents Experience Acute Stress While Working in the Emergency Department. West. J. Emerg. Med. 2021, 22, 94–100. [Google Scholar] [CrossRef]
- Acarix. CADScor®System User Manual; Acarix: Malmo, Sweden, 2019. [Google Scholar]
- Malakar, A.K.; Choudhury, D.; Halder, B.; Paul, P.; Uddin, A.; Chakraborty, S. A review on coronary artery disease, its risk factors, and therapeutics. J. Cell. Physiol. 2019, 234, 16812–16823. [Google Scholar] [CrossRef]
- Bjørnsen, L.P.; Naess-Pleym, L.E.; Dale, J.; Grenne, B.; Wiseth, R. Description of chest pain patients in a Norwegian emergency department. Scand. Cardiovasc. J. 2019, 53, 28–34. [Google Scholar] [CrossRef]
- Negi, S. Atherosclerotic Coronary Heart Disease Epidemiology, Classification and Management. Cardiovasc. Hematol. Disord. Targets 2010, 10, 257–261. [Google Scholar] [CrossRef]
- Curfman, G. Acute Chest Pain in the Emergency Department. JAMA Intern. Med. 2018, 178, 220. [Google Scholar] [CrossRef] [PubMed]
- Winther, S.; Nissen, L.; Schmidt, S.E.; Westra, J.; Andersen, I.T.; Nyegaard, M.; Madsen, L.H.; Knudsen, L.L.; Urbonaviciene, G.; Larsen, B.S.; et al. Advanced heart sound analysis as a new prognostic marker in stable coronary artery disease. Eur. Heart J. Digit. Health 2021, 2, 279–289. [Google Scholar] [CrossRef]


{kind=link}
| Total | Male | Female | p-Value | No Known CAD | Previously Known CAD | p-Value | CAD Score > 20 | CAD Score ≤ 20 | p-Value | CAD Score Not Calculated | No ACS as Final Diagnosis | ACS as Final Diagnosis | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N (% of total) | 105 | 51 (48.6) | 54 (51.4) | 71 (67.6) | 34 (32.4) | 59 (56.2) | 25 (23.8) | 21 (20.0) | 102 (97.1) | 3 (2.9) | |||
| Male sex, n (%) | 51 (48.6) | 27 (38.0) | 24 (70.6) | 0.020 | 34 (57.6) | 5 (20.0) | <0.001 | 12 (57.1) | 49 (48) | 2 (66.7) | |||
| Caucasian, n (%) | 99 (94.3) | 48 (94.1) | 51 (94.4) | 0.943 | 65 (91.5) | 34 (100) | 0.081 | 57 (96.6) | 22 (88.0) | 0.121 | 20 (95.2) | 96 (94.1) | 3 (100) |
| Age, years (IQR) | 61 (51–71) | 62 (53–71) | 61 (49–71) | 0.426 | 57 (48–68) | 69 (62–78) | <0.001 | 68 (58–74) | 49 (46–56) | <0.001 | 61 (55–72) | 61 (51–71) | 66 (53–86) |
| BMI, kg/m2 (IQR) | 28 (24–32) | 28 (23–32) | 29 (25–32) | 0.348 | 28 (24–31) | 28 (24–33) | 0.627 | 28 (23–32) | 25 (23–30) | 0.085 | 29 (25–32) | 28 (24–32) | 31 (26–37) |
| Systolic blood pressure, mmHg (IQR) | 144 (129–155) | 140 (128–150) | 148 (129–160) | 0.129 | 144 (130–155) | 142 (123–155) | 0.578 | 149 (140–160) | 130 (115–147) | 0.009 | 138 (127–155) | 142 (128–156) | 150 (147–153) |
| Diastolic blood pressure, mmHg (IQR) | 80 (67–87) | 81 (71–88) | 76 (66.5–84.8) | 0.137 | 80 (69–89) | 79 (65–86) | 0.231 | 80 (65–86) | 79 (70–91) | 0.966 | 80 (75–89) | 80 (67–87) | 79 (66–92) |
| SpO2 (FiO2 0.21), % (IQR) | 98 (96–100) | 97 (96–99) | 98 (97–100) | 0.066 | 98 (97–100) | 98 (96–99) | 0.184 | 98 (96–99) | 100 (98–100) | <0.001 | 96 (95–98) | 98 (96–100) | 99 (97–100) |
| Heart rate, beats/min (IQR) | 75 (63–87) | 77 (62–89) | 74 (64–86) | 0.396 | 75 (64–87) | 76 (62–87) | 0.873 | 74 (61–84) | 67 (61–82) | 0.058 | 88 (83–96) | 76 (63–87) | 64 (53–75) |
| Comorbidities | |||||||||||||
| AHTN, n (%) | 57 (54.3) | 27 (52.9) | 30 (55.5) | 0.938 | 27 (38.0) | 30 (88.2) | <0.001 | 39 (66.1) | 6 (24.0) | <0.001 | 12 (57.1) | 55 (53.9) | 2 (66.7) |
| HLP, n (%) | 34 (32.4) | 19 (37.3) | 15 (27.8) | 0.300 | 14 (19.7) | 20 (58.8) | <0.001 | 22 (37.3) | 3 (12.0) | 0.013 | 9 (42.9) | 33 (32.4) | 1 (33.3) |
| DM II, n (%) | 26 (24.8) | 16 (31.4) | 10 (18.5) | 0.127 | 13 (18.3) | 13 (38.2) | 0.027 | 19 (32.2) | 1 (4.0) | 0.060 | 6 (28.6) | 26 (25.5) | 0 |
| CAD previously known, n (%) | 34 (32.4) | 24 (47.1) | 10 (18.5) | 0.002 | 22 (37.3) | 3 (12.0) | 0.013 | 9 (42.9) | 33 (32.4) | 1 (33.3) | |||
| Previous MCI, n (%) | 13 (12.4) | 8 (15.7) | 5 (9.3) | 0.313 | 0 | 13 (38.2) | <0.001 | 12 (20.3) | 0 | 0.115 | 1 (4.8) | 12 (11.8) | 1 (33.3) |
| Family history of CAD, n (%) | 27 (25.7) | 9 (17.6) | 18 (33.3) | 0.085 | 13 (18.3) | 14 (41.2) | 0.007 | 15 (25.4) | 8 (32.0) | 0.450 | 4 (19.0) | 25 (24.5) | 2 (66.7) |
| CKI, n (%) | 5 (4.8) | 2 (4.2) | 3 (5.6) | 0.686 | 2 (2.8) | 3 (8.8) | 0.131 | 1 (1.7) | 2 (8.0) | 0.182 | 2 (9.5) | 3 (2.9) | 2 (66.7) |
| PAD, n (%) | 10 (9.5) | 7 (13.7) | 3 (5.6) | 0.154 | 2 (2.8) | 8 (23.5) | <0.001 | 7 (11.9) | 2 (8.0) | 0.766 | 1 (4.8) | 9 (8.8) | 1 (33.3) |
| Vascular status | |||||||||||||
| BaPWV, m/s (IQR) | 14.0 (12.5–15.8) | 13.9 (12.7–15.8) | 14.1 (12.3–16.0) | 0.653 | 13.5 (12.4–15.7) | 14.2 (12.8–17.8) | 0.253 | 14.8 (12.8–17.2) | 12.5 (12.0–13.7) | 0.429 | 14.1 (12.7–15.8) | 14.0 (12.5–15.8) | 12.8 (12.3–12.9) |
| cfPWV, m/s (IQR) | 9.5 (8.4–11.4) | 9.4 (8.6–11.4) | 9.7 (8.1–11.6) | 0.720 | 9.3 (8.1–11.1) | 10.2 (9.4–12.9) | 0.061 | 10.5 (9.0–12.8) | 8.3 (7.8–9.1) | <0.001 | 9.8 (9.4–12.1) | 10.3 (7.9–13.0) | 8.5 (8.0–9.1) |
| Smoking status | |||||||||||||
| Never, n (%) | 43 (41.0) | 15 (29.4) | 28 (51.9) | 0.019 | 34 (47.9) | 9 (26.5) | 0.037 | 23 (39.0) | 14 (56.0) | 0.080 | 6 (28.6) | 41 (40.2) | 2 (66.7) |
| Former, n (%) | 38 (36.2) | 24 (47.1) | 14 (25.9) | 0.024 | 18 (25.4) | 20 (58.8) | <0.001 | 23 (39.0) | 5 (20.0) | 0.054 | 10 (47.6) | 37 (36.3) | 1 (33.3) |
| Active, n (%) | 24 (22.9) | 12 (23.5) | 12 (22.2) | 0.873 | 19 (36.8) | 5 (14.7) | 0.169 | 12 (22.0) | 6 (24.0) | 0.876 | 5 (23.8) | 24 (23.5) | 0 |
| Chief complaint | |||||||||||||
| Typical AP, n (%) | 92 (87.6) | 44 (86.3) | 48 (88.9) | 0.684 | 62 (87.3) | 30 (88.2) | 0.894 | 50 (84.7) | 23 (92.0) | 0.446 | 19 (90.5) | 89 (87.3) | 3 (100) |
| Atypical AP, n (%) | 6 (5.7) | 3 (5.9) | 3 (5.6) | 0.943 | 4 (5.6) | 2 (5.9) | 0.959 | 5 (8.5% | 0 | 0.158 | 1 (4.8) | 6 (5.9) | 0 |
| Non-specific chest pain, n (%) | 7 (6.7) | 4 (7.8) | 3 (5.6) | 0.639 | 5 (7.0) | 2 (5.9) | 0.824 | 4 (6.8) | 2 (8.0) | 0.759 | 1 (4.8) | 7 (6.9) | 0 |
| Symptom evaluation | |||||||||||||
| Pain worsening with exercise, n (%) | 34 (32.4) | 17 (33.3) | 17 (31.5) | 0.839 | 20 (28.2) | 14 (41.2) | 0.183 | 17 (28.8) | 8 (32.0) | 0.963 | 9 (42.9) | 33 (32.4) | 1 (33.3) |
| Cardiac origin of pain assumed by patient, n (%) | 36 (34.3) | 19 (37.3) | 17 (31.5) | 0.533 | 22 (31) | 14 (41.2% | 0.303 | 19 (32.2) | 8 (32.0) | 0.783 | 9 (42.9) | 35 (34.3) | 1 (33.3) |
| Pain reproducible with palpation, n (%) | 21 (20.0) | 10 (19.6) | 11 (20.4) | 0.922 | 18 (25.4) | 3 (8.8) | 0.048 | 13 (22.0) | 5 (20.0) | 0.934 | 3 (14.3) | 20 (19.6) | 1 (33.3) |
| HEART score, points (IQR) | 4 (3–6) | 5 (3–6) | 4 (3–5) | 0.155 | 3 (2–4) | 6 (5–7) | <0.001 | 5 (3–6) | 3 (2–3.5) | <0.001 | 5 (3–5.5) | 4 (3–6) | 5 (3.5–5.5) |
| GRACE score, points (IQR) | 79 (59–106) | 83 (65–111) | 72 (58–93) | 0.042 | 68 (53–85) | 101 (81–123) | <0.001 | 85 (68–111) | 56 (47–63) | <0.001 | 83 (70–107) | 78 (59–105) | 93 (56–122) |
| NYHA I, n (%) | 81 (77.1) | 35 (68.6) | 46 (85.2) | 0.026 | 61 (85.6) | 20 (58.8) | 0.004 | 44 (74.6) | 21 (84.0) | 0.398 | 16 (76.2) | 78 (76.5) | 3 (100) |
| NYHA II, n (%) | 20 (19.0) | 13 (25.5) | 7 (13.0) | 0.112 | 10 (14.1) | 10 (29.4) | 0.051 | 13 (22.0) | 4 (16.0) | 0.638 | 3 (14.3) | 20 (19.6) | 0 |
| NYHA III, n (%) | 3 (2.9) | 3 (5.9) | 0 | 0.073 | 0 | 3 (8.8) | 0.059 | 2 (3.4) | 0 | 0.323 | 1 (4.8) | 3 (2.9) | 0 |
| NYHA IV, n (%) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| ECG details | |||||||||||||
| ST elevation (not significant), n (%) | 4 (3.8) | 2 (3.9) | 2 (3.7) | 0.919 | 1 (1.4) | 3 (8.8) | 0.050 | 2 (3.4) | 0 | 0.255 | 2 (9.5) | 4 (3.9) | 0 |
| ST depression (not significant), n (%) | 4 (3.8) | 1 (2.0) | 3 (5.6) | 0.357 | 1 (1.4) | 3 (8.8) | 0.050 | 3 (5.1) | 0 | 0.331 | 1 (4.8) | 4 (3.9) | 0 |
| Outcome | |||||||||||||
| Primarily discharged, n (%) | 85 (81.0) | 38 (74.5) | 47 (87) | 0.102 | 64 (90.1) | 21 (61.8) | <0.001 | 47 (79.7) | 23 (92.0) | 0.133 | 15 (71.4) | 85 (83.3) | 0 |
| Normal ward admission, n (%) | 16 (15.2) | 12 (23.5) | 4 (7.4) | 0.022 | 4 (5.6) | 12 (35.3) | <0.001 | 9 (15.3) | 2 (8.0) | 0.249 | 5 (23.8) | 15 (14.7) | 1 (33.3) |
| IMCU admission, n (%) | 4 (3.8) | 1 (2.0) | 3 (5.6) | 0.336 | 3 (4.2) | 1 (2.9) | 0.748 | 3 (5.1) | 0 | 0.254 | 1 (4.8) | 2 (2.0) | 2 (66.7) |
| Total | Male | Female | p-Value | No Known CAD | Previously Known CAD | p-Value | CAD Score > 20 | CAD Score ≤ 20 | CAD Score Not Calculated | No ACS as Final Diagnosis | ACS as Final Diagnosis | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N (% of total) | 105 | 51 (48.6) | 54 (51.4) | 71 (67.6) | 34 (32.4) | 59 (56.2) | 25 (23.8) | 21 (20.0) | 102 (97.1) | 3 (2.9) | ||
| Numerical CAD score, points (IQR) | 33 (18–45) | 42 (33–55) | 21 (12–34) | <0.001 | 26 (14–35) | 45 (33–55) | <0.001 | 37 (30–53) | 14 (8–18) | 32 (18–44) | 45 (34–62) | |
| Score successfully calculated, n (%) | 84 (80.0) | 39 (76.5) | 45 (83.3) | 0.380 | 59 (83.1) | 25 (73.5) | 0.251 | 81 (79.4) | 3 (100) | |||
| Score failed to calculate, n (%) | 21 (20.0) | 12 (23.5) | 9 (16.7) | 0.380 | 12 (16.9) | 9 (26.5) | 0.251 | 21 (20.6) | 0 | |||
| Measurement stopped by patient, n (%) | 9 (8.6) | 5 (9.8) | 4 (7.4) | 0.661 | 4 (5.6) | 5 (14.7) | 0.120 | 9 (42.9) | 9 (8.8) | 0 | ||
| Measurement stopped by investigator, n (%) | 10 (9.5) | 7 (13.7) | 3 (5.6) | 0.154 | 6 (8.5) | 4 (11.8) | 0.588 | 10 (47.6) | 10 (9.8) | 0 | ||
| Measurement not possible due to technical reason, n (%) | 2 (1.9) | 0 | 2 (3.7) | 0.165 | 2 (2.8) | 0 | 0.323 | 2 (9.5) | 2 (2.0) | 0 | ||
| Feasibility judged by patient, points on Likert scale 0–10 (±SD) | 9.0 (1.8) | 8.9 (2.1) | 9 (1.5) | 0.414 | 9.2 (1.3) | 8.4 (2.5) | 0.200 | 9.3 (1.5) | 9.4 (1.0) | 7.5 (2.7) | 8.9 (1.8) | 9.3 (1.2) |
| Feasibility judged by investigator, points on Likert scale 0–10 (±SD) | 8.9 (2.6) | 9 (2.4) | 8.8 (2.9) | 0.687 | 9.1 (2.6) | 8.5 (2.9) | 0.188 | 9.9 (0.4) | 10 (0) | 4.8 (3.7) | 8.9 (2.7) | 10 (0) |
| 1 attempt, n (%) | 79 (75.2) | 36 (70.6) | 43 (79.6) | 0.283 | 56 (78.9) | 23 (67.7) | 0.212 | 55 (93.2) | 23 (92.0) | 1 (4.8) | 76 (74.5) | 3 (100) |
| 2 attempts, n (%) | 15 (14.3) | 9 (17.6) | 6 (11.1) | 0.339 | 10 (14.1) | 5 (14.7) | 0.932 | 3 (5.1) | 2 (8.0) | 10 (47.6) | 15 (14.7) | 0 |
| 3 attempts, n (%) | 7 (6.7) | 4 (7.8) | 3 (5.6) | 0.639 | 2 (2.8) | 5 (14.7) | 0.062 | 1 (1.7) | 0 | 6 (28.5) | 7 (6.9) | 0 |
| 4 attempts, n (%) | 1 (1.0) | 1 (2.0) | 0 | 0.301 | 0 | 1 (2.9) | 0.147 | 0 | 0 | 1 (4.8) | 1 (1.0) | 0 |
| >4 attempts, n (%) | 3 (2.8) | 1 (2.0) | 2 (3.7) | 0.592 | 3 (4.2) | 0 | 0.224 | 0 | 0 | 3 (14.3) | 3 (2.9) | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schnaubelt, S.; Eibensteiner, F.; Oppenauer, J.; Kornfehl, A.; Brock, R.; Poschenreithner, L.; Du, N.; Baldi, E.; Schlager, O.; Niessner, A.; et al. The Feasibility of Ultra-Sensitive Phonocardiography in Acute Chest Pain Patients of a Tertiary Care Emergency Department (ScorED Feasibility Study). J. Pers. Med. 2022, 12, 631. https://doi.org/10.3390/jpm12040631
Schnaubelt S, Eibensteiner F, Oppenauer J, Kornfehl A, Brock R, Poschenreithner L, Du N, Baldi E, Schlager O, Niessner A, et al. The Feasibility of Ultra-Sensitive Phonocardiography in Acute Chest Pain Patients of a Tertiary Care Emergency Department (ScorED Feasibility Study). Journal of Personalized Medicine. 2022; 12(4):631. https://doi.org/10.3390/jpm12040631
Chicago/Turabian StyleSchnaubelt, Sebastian, Felix Eibensteiner, Julia Oppenauer, Andrea Kornfehl, Roman Brock, Laura Poschenreithner, Na Du, Enrico Baldi, Oliver Schlager, Alexander Niessner, and et al. 2022. "The Feasibility of Ultra-Sensitive Phonocardiography in Acute Chest Pain Patients of a Tertiary Care Emergency Department (ScorED Feasibility Study)" Journal of Personalized Medicine 12, no. 4: 631. https://doi.org/10.3390/jpm12040631