
Masticatory Muscle Thickness and Activity Correlates to Eyeball Length, Intraocular Pressure, Retinal and Choroidal Thickness in Healthy Women versus Women with Myopia

 ,
,  , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Protocol
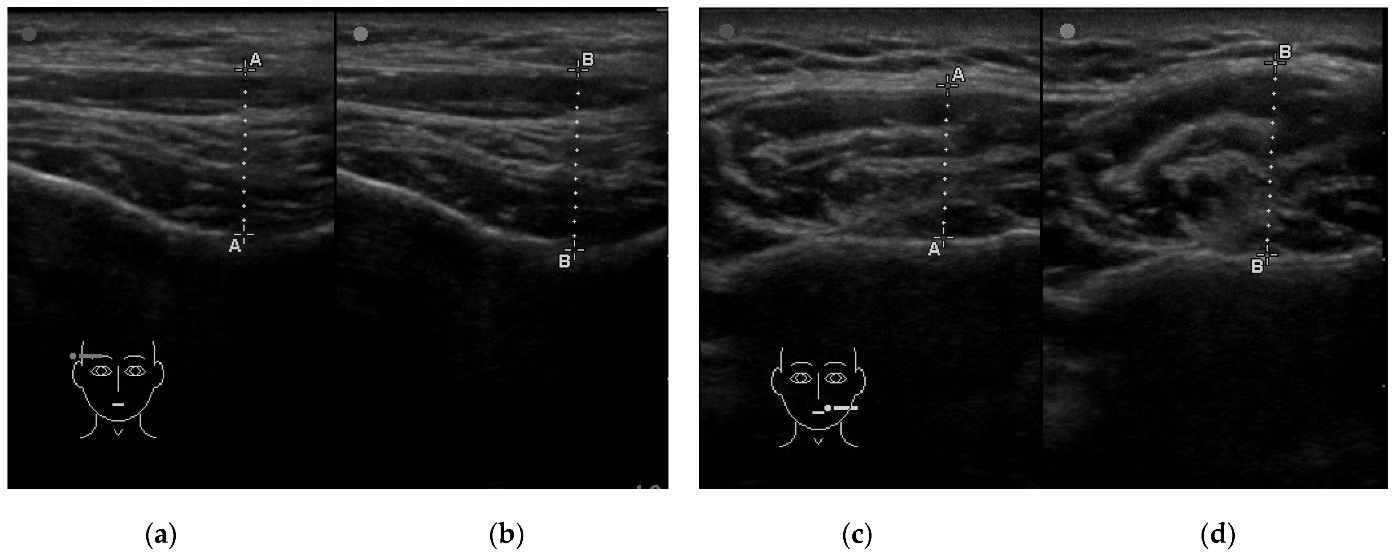
2.2.1. Assessment of Muscle Thickness
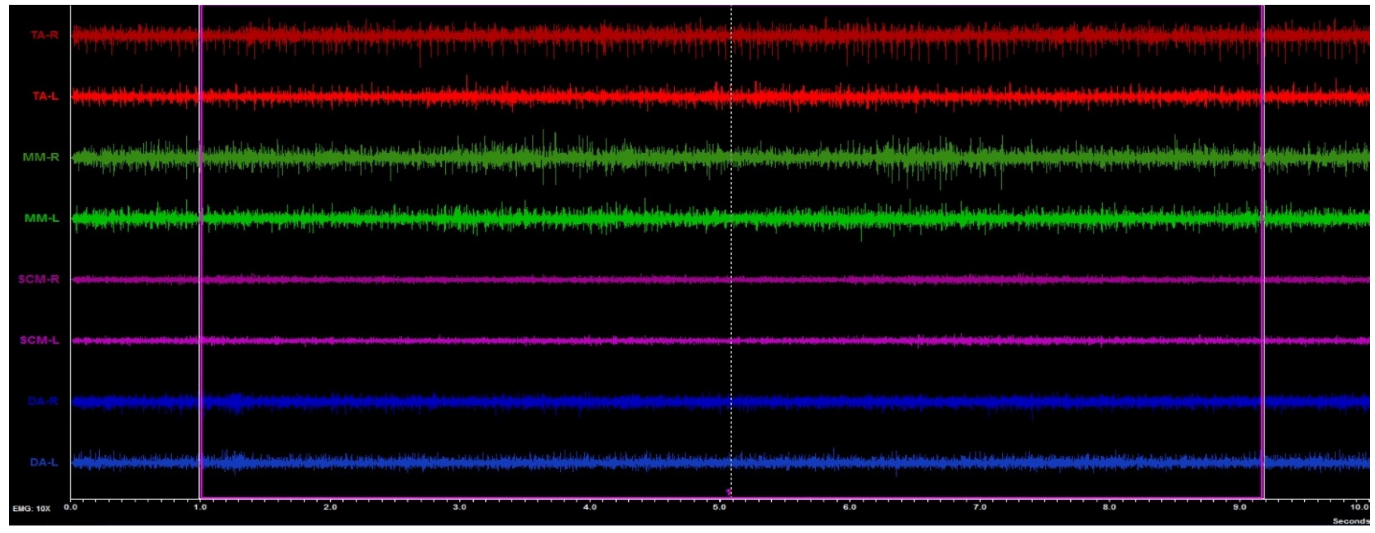
2.2.2. Assessment of the Muscle Activity
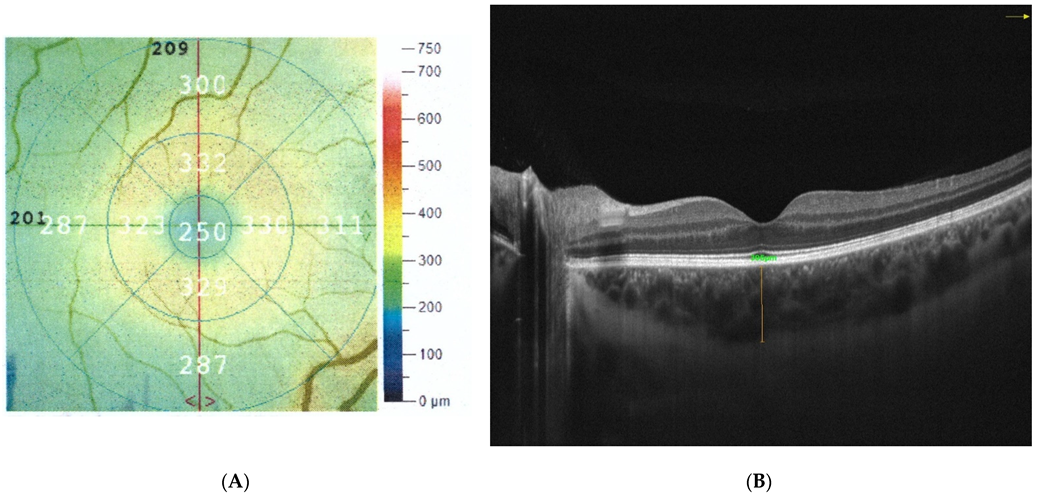
2.2.3. Ophthalmic Examination
The Axial Length of the Eyeball
The Thickness of the Retina and Choroid
The Intraocular Pressure
2.2.4. Statistical Analysis
3. Results
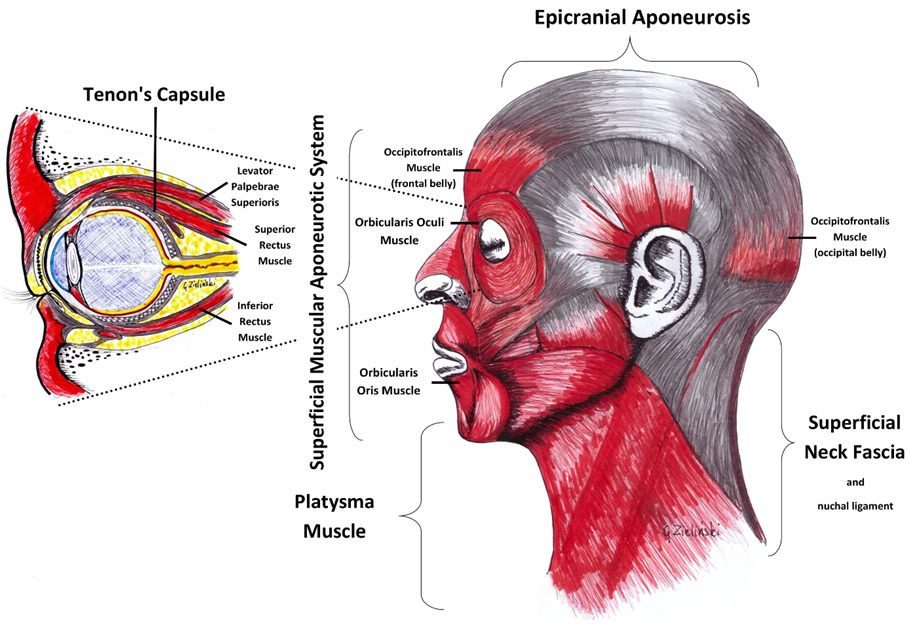
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| μm | micrometers |
| μV | microvolt |
| CFT | central foveal thickness |
| Clench | ultrasound muscles examination in the maximum voluntary clenching |
| CPS | cervical proprioceptive system |
| DA | anterior belly of the digastric muscle |
| Dsph | Diopters |
| IOP | intraocular pressure |
| L | Left site |
| mm | millimeters |
| MM | the superficial part of the masseter muscle |
| mmHg | millimeter of mercury |
| p | Pearson test |
| R | Right site |
| RDC/TMD | Research Diagnostic Criteria for Temporomandibular Disorders |
| Rest | ultrasound muscles examination in the relaxed mandible position with slight contact between opposing teeth |
| s | Spearman rho test |
| SCM | middle part of the sternocleidomastoid muscle belly |
| sEMG | surface electromyography |
| SMAS | superficial musculoaponeurotic system |
| TA | part of the temporalis muscle |
| TMD | temporomandibular disorders |
| VOR | vestibulo-ocular reflex |
References
- Hrynchak, P.K.; Mittelstaedt, A.; Machan, C.M.; Bunn, C.; Irving, E.L. Increase in Myopia Prevalence in Clinic-Based Populations across a Century. Optom. Vis. Sci. 2013, 90, 1331–1341. [Google Scholar] [CrossRef]
- Holden, B.A.; Fricke, T.R.; Wilson, D.A.; Jong, M.; Naidoo, K.S.; Sankaridurg, P.; Wong, T.Y.; Naduvilath, T.J.; Resnikoff, S. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology 2016, 123, 1036–1042. [Google Scholar] [CrossRef] [Green Version]
- Grzybowski, A.; Kanclerz, P.; Tsubota, K.; Lanca, C.; Saw, S.-M. A Review on the Epidemiology of Myopia in School Children Worldwide. BMC Ophthalmol. 2020, 20, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carr, B.J.; Stell, W.K. The Science Behind Myopia. In Webvision: The Organization of the Retina and Visual System; Kolb, H., Fernandez, E., Nelson, R., Eds.; University of Utah Health Sciences Center: Salt Lake City, UT, USA, 1995. [Google Scholar]
- Tideman, J.W.L.; Polling, J.R.; Vingerling, J.R.; Jaddoe, V.W.V.; Williams, C.; Guggenheim, J.A.; Klaver, C.C.W. Axial Length Growth and the Risk of Developing Myopia in European Children. Acta Ophthalmol. 2018, 96, 301–309. [Google Scholar] [CrossRef]
- Flitcroft, D.I.; He, M.; Jonas, J.B.; Jong, M.; Naidoo, K.; Ohno-Matsui, K.; Rahi, J.; Resnikoff, S.; Vitale, S.; Yannuzzi, L. IMI—Defining and Classifying Myopia: A Proposed Set of Standards for Clinical and Epidemiologic Studies. Investig. Ophthalmol. Vis. Sci. 2019, 60, M20–M30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikuno, Y. Overview of the complications of high myopia. Retina 2017, 37, 2347–2351. [Google Scholar] [CrossRef]
- Manny, R.E.; Mitchell, G.L.; Cotter, S.A.; Jones-Jordan, L.A.; Kleinstein, R.N.; Mutti, D.O.; Twelker, J.D.; Zadnik, K. CLEERE Study Group Intraocular Pressure, Ethnicity, and Refractive Error. Optom. Vis. Sci. 2011, 88, 1445–1453. [Google Scholar] [CrossRef]
- Hysi, P.G.; Choquet, H.; Khawaja, A.P.; Wojciechowski, R.; Tedja, M.S.; Yin, J.; Simcoe, M.J.; Patasova, K.; Mahroo, O.A.; Thai, K.K.; et al. Meta-Analysis of 542,934 Subjects of European Ancestry Identifies New Genes and Mechanisms Predisposing to Refractive Error and Myopia. Nat. Genet. 2020, 52, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Chen, S.; Liu, Y.; Lin, F.; Song, Y.; Li, T.; Aung, T.; Zhang, X. Lowering Intraocular Pressure: A Potential Approach for Controlling High Myopia Progression. Investig. Ophthalmol. Vis. Sci. 2021, 62, 17. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.C.K.; Lam, C.S.Y.; Yap, M.K.H. Retinal Thickness in Myopic and Non-Myopic Eyes. Ophthalmic Physiol. Opt. 2010, 30, 776–784. [Google Scholar] [CrossRef]
- Myers, C.E.; Klein, B.E.K.; Meuer, S.M.; Swift, M.K.; Chandler, C.S.; Huang, Y.; Gangaputra, S.; Pak, J.W.; Danis, R.P.; Klein, R. Retinal Thickness Measured by Spectral Domain Optical Coherence Tomography in Eyes without Retinal Abnormalities: The Beaver Dam Eye Study. Am. J. Ophthalmol. 2015, 159, 445–456.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.; Wei, P.; Li, J. The Thickness Changes of Retina in High Myopia Patients during the Third Trimester of Pregnancy: A Pilot Study. BMC Ophthalmol. 2021, 21, 382. [Google Scholar] [CrossRef] [PubMed]
- Nishida, Y.; Fujiwara, T.; Imamura, Y.; Lima, L.H.; Kurosaka, D.; Spaide, R.F. Choroidal Thickness and Visual Acuity in Highly Myopic Eyes. Retina 2012, 32, 1229–1236. [Google Scholar] [CrossRef] [PubMed]
- Monaco, A.; Cattaneo, R.; Spadaro, A.; Giannoni, M.; Di Martino, S.; Gatto, R. Visual Input Effect on EMG Activity of Masticatory and Postural Muscles in Healthy and in Myopic Children. Eur. J. Paediatr Dent. 2006, 7, 18–22. [Google Scholar] [PubMed]
- Zieliński, G.; Matysik-Woźniak, A.; Rapa, M.; Baszczowski, M.; Ginszt, M.; Zawadka, M.; Szkutnik, J.; Rejdak, R.; Gawda, P. The Influence of Visual Input on Electromyographic Patterns of Masticatory and Cervical Spine Muscles in Subjects with Myopia. J. Clin. Med. 2021, 10, 5376. [Google Scholar] [CrossRef]
- Zieliński, G.; Filipiak, Z.; Ginszt, M.; Matysik-Woźniak, A.; Rejdak, R.; Gawda, P. The Organ of Vision and the Stomatognathic System—Review of Association Studies and Evidence-Based Discussion. Brain Sci. 2022, 12, 14. [Google Scholar] [CrossRef]
- Fiorucci, E.; Bucci, G.; Cattaneo, R.; Monaco, A. The Measurement of Surface Electromyographic Signal in Rest Position for the Correct Prescription of Eyeglasses. IEEE Trans. Instrum. Meas. 2012, 61, 419–428. [Google Scholar] [CrossRef]
- Czepita, M.; Czepita, D.; Safranow, K. Role of Gender in the Prevalence of Myopia among Polish Schoolchildren. J. Ophthalmol. 2019, 2019, 9748576. [Google Scholar] [CrossRef]
- Czepita, D.; Mojsa, A.; Ustianowska, M.; Czepita, M.; Lachowicz, E. Role of Gender in the Occurrence of Refractive Errors. Ann. Acad. Med. Stetin 2007, 53, 5–7. [Google Scholar]
- Jones-Jordan, L.A.; Sinnott, L.T.; Chu, R.H.; Cotter, S.A.; Kleinstein, R.N.; Manny, R.E.; Mutti, D.O.; Twelker, J.D.; Zadnik, K. CLEERE Study Group Myopia Progression as a Function of Sex, Age, and Ethnicity. Investig. Ophthalmol. Vis. Sci. 2021, 62, 36. [Google Scholar] [CrossRef]
- Bueno, C.H.; Pereira, D.D.; Pattussi, M.P.; Grossi, P.K.; Grossi, M.L. Gender Differences in Temporomandibular Disorders in Adult Populational Studies: A Systematic Review and Meta-Analysis. J. Oral Rehabil 2018, 45, 720–729. [Google Scholar] [CrossRef] [PubMed]
- Bagis, B.; Ayaz, E.A.; Turgut, S.; Durkan, R.; Özcan, M. Gender Difference in Prevalence of Signs and Symptoms of Temporomandibular Joint Disorders: A Retrospective Study on 243 Consecutive Patients. Int. J. Med. Sci. 2012, 9, 539–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satiroğlu, F.; Arun, T.; Işik, F. Comparative Data on Facial Morphology and Muscle Thickness Using Ultrasonography. Eur. J. Orthod. 2005, 27, 562–567. [Google Scholar] [CrossRef]
- Chang, P.-H.; Chen, Y.-J.; Chang, K.-V.; Wu, W.-T.; Özçakar, L. Ultrasound Measurements of Superficial and Deep Masticatory Muscles in Various Postures: Reliability and Influencers. Sci. Rep. 2020, 10, 14357. [Google Scholar] [CrossRef]
- Macrae, P.R.; Jones, R.D.; Myall, D.J.; Melzer, T.R.; Huckabee, M.-L. Cross-Sectional Area of the Anterior Belly of the Digastric Muscle: Comparison of MRI and Ultrasound Measures. Dysphagia 2013, 28, 375–380. [Google Scholar] [CrossRef]
- Strini, P.J.S.A.; Strini, P.J.S.A.; de Souza Barbosa, T.; Gavião, M.B.D. Assessment of Thickness and Function of Masticatory and Cervical Muscles in Adults with and without Temporomandibular Disorders. Arch. Oral Biol. 2013, 58, 1100–1108. [Google Scholar] [CrossRef]
- Ginszt, M.; Zieliński, G. Novel Functional Indices of Masticatory Muscle Activity. J. Clin. Med. 2021, 10, 1440. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of Recommendations for SEMG Sensors and Sensor Placement Procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Shi, Q.; Wang, G.-Y.; Cheng, Y.-H.; Pei, C. Comparison of IOL-Master 700 and IOL-Master 500 Biometers in Ocular Biological Parameters of Adolescents. Int. J. Ophthalmol. 2021, 14, 1013–1017. [Google Scholar] [CrossRef]
- Buckhurst, P.J.; Wolffsohn, J.S.; Shah, S.; Naroo, S.A.; Davies, L.N.; Berrow, E.J. A New Optical Low Coherence Reflectometry Device for Ocular Biometry in Cataract Patients. Br. J. Ophthalmol. 2009, 93, 949–953. [Google Scholar] [CrossRef] [Green Version]
- Koman-Wierdak, E.; Róg, J.; Brzozowska, A.; Toro, M.D.; Bonfiglio, V.; Załuska-Ogryzek, K.; Karakuła-Juchnowicz, H.; Rejdak, R.; Nowomiejska, K. Analysis of the Peripapillary and Macular Regions Using OCT Angiography in Patients with Schizophrenia and Bipolar Disorder. J. Clin. Med. 2021, 10, 4131. [Google Scholar] [CrossRef] [PubMed]
- Gella, L.; Raman, R.; Sharma, T. Macular Thickness Measurements Using Copernicus Spectral Domain Optical Coherence Tomography. Saudi J. Ophthalmol. 2015, 29, 121–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonfiglio, V.; Ortisi, E.; Scollo, D.; Reibaldi, M.; Russo, A.; Pizzo, A.; Faro, G.; Macchi, I.; Fallico, M.; Toro, M.D.; et al. Vascular Changes after Vitrectomy for Rhegmatogenous Retinal Detachment: Optical Coherence Tomography Angiography Study. Acta Ophthalmol. 2019, 98, e563–e569. [Google Scholar] [CrossRef] [PubMed]
- McKee, E.C.; Ely, A.L.; Duncan, J.E.; Dosunmu, E.O.; Freedman, S.F. A Comparison of Icare PRO and Tono-Pen XL Tonometers in Anesthetized Children. J. AAPOS 2015, 19, 332–337. [Google Scholar] [CrossRef]
- Beneyto, P.; Barajas, M.A.; Garcia-de-Blas, F.; del Cura, I.; Sanz, T.; Vello, R.; Salvador, C. Predictive Value of Tonometry with Tono-Pen® XL in Primary Care. Br. J. Gen. Pr. 2007, 57, 653–654. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Elsevier Science: Burlington, VT, USA, 2013; ISBN 978-1-4832-7648-9. [Google Scholar]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect Size Estimates: Current Use, Calculations, and Interpretation. J. Exp. Psychol Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakens, D. Calculating and Reporting Effect Sizes to Facilitate Cumulative Science: A Practical Primer for t-Tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef] [Green Version]
- Gordon, R.A.; Donzis, P.B. Refractive Development of the Human Eye. Arch. Ophthalmol. 1985, 103, 785–789. [Google Scholar] [CrossRef]
- Rozema, J.J.; Ní Dhubhghaill, S. Age-Related Axial Length Changes in Adults: A Review. Ophthalmic Physiol. Opt. 2020, 40, 710–717. [Google Scholar] [CrossRef]
- Meng, W.; Butterworth, J.; Malecaze, F.; Calvas, P. Axial Length of Myopia: A Review of Current Research. OPH 2011, 225, 127–134. [Google Scholar] [CrossRef]
- Zereid, F.M.; Osuagwu, U.L. Myopia and Regional Variations in Retinal Thickness in Healthy Eyes. J. Ophthalmic Vis. Res. 2020, 15, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Kong, M.; Choi, D.Y.; Han, G.; Song, Y.-M.; Park, S.Y.; Sung, J.; Hwang, S.; Ham, D.-I. Measurable Range of Subfoveal Choroidal Thickness With Conventional Spectral Domain Optical Coherence Tomography. Transl. Vis. Sci. Technol. 2018, 7, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoseini-Yazdi, H.; Vincent, S.J.; Collins, M.J.; Read, S.A.; Alonso-Caneiro, D. Wide-Field Choroidal Thickness in Myopes and Emmetropes. Sci. Rep. 2019, 9, 3474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, P.; Saw, S.-M.; Cheung, C.Y.; Girard, M.J.A.; Mari, J.M.; Bhargava, M.; Tan, C.; Tan, M.; Yang, A.; Tey, F.; et al. Choroidal Thickness and High Myopia: A Case–Control Study of Young Chinese Men in Singapore. Acta Ophthalmol. 2015, 93, e585–e592. [Google Scholar] [CrossRef] [PubMed]
- Stecco, C.; Hammer, W.I. Functional Atlas of the Human Fascial System; Elsevier Ltd.: Edinburgh, UK, 2015; ISBN 978-0-7020-4430-4. [Google Scholar]
- Sterniak, M. Terapia Krótkowzrocznosci Nabytej u Dzieci Metodą Manipulacji Powięzi—Studium Przypadku. Fizjoterapia I Rechabilitacja 2017, 88, 6–11. [Google Scholar]
- AlShareef, S.; Newton, B.W. Accessory Nerve Injury. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Whitney, Z.B.; Jain, M.; Zito, P.M. Anatomy, Skin, Superficial Musculoaponeurotic System (SMAS) Fascia. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Davidge, K.M.; van Furth, W.R.; Agur, A.; Cusimano, M. Naming the Soft Tissue Layers of the Temporoparietal Region: Unifying Anatomic Terminology across Surgical Disciplines. Neurosurgery 2010, 67, ons120–ons129. [Google Scholar] [CrossRef]
- Marasini, S.; Khadka, J.; Sthapit, P.R.K.; Sharma, R.; Nepal, B.P. Ocular Morbidity on Headache Ruled out of Systemic Causes—A Prevalence Study Carried out at a Community Based Hospital in Nepal. J. Optom. 2012, 5, 68–74. [Google Scholar] [CrossRef] [Green Version]
- Bhatia, R.; Dureja, G.P.; Tripathi, M.; Bhattacharjee, M.; Bijlani, R.L.; Mathur, R. Role of Temporalis Muscle over Activity in Chronic Tension Type Headache: Effect of Yoga Based Management. Indian J. Physiol. Pharm. 2007, 51, 333–344. [Google Scholar]
- Bendtsen, L.; Fernández-de-la-Peñas, C. The Role of Muscles in Tension-Type Headache. Curr. Pain Headache Rep. 2011, 15, 451–458. [Google Scholar] [CrossRef]
- Zorena, K.; Gładysiak, A.; Ślęzak, D. Early Intervention and Nonpharmacological Therapy of Myopia in Young Adults. J. Ophthalmol. 2018, 2018, 4680603. [Google Scholar] [CrossRef] [Green Version]
- Strini, P.J.S.A.; Strini, P.H.S.A.; Barbosa, T.S.; Gavião, M.B.D. Effects of Head Posture on Cervical Muscle Thickness and Activity in Young Adults With and Without Temporomandibular Disorders. J. Musculoskelet. Pain 2014, 22, 89–98. [Google Scholar] [CrossRef]
- Grgić, V. Cervicogenic proprioceptive vertigo: Etiopathogenesis, clinical manifestations, diagnosis and therapy with special emphasis on manual therapy. Lijec Vjesn 2006, 128, 288–295. [Google Scholar] [PubMed]
- Yahia, A.; Ghroubi, S.; Jribi, S.; Mâlla, J.; Baklouti, S.; Ghorbel, A.; Elleuch, M.H. Chronic Neck Pain and Vertigo: Is a True Balance Disorder Present? Ann. Phys. Rehabil. Med. 2009, 52, 556–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luan, H.; Gdowski, M.J.; Newlands, S.D.; Gdowski, G.T. Convergence of Vestibular and Neck Proprioceptive Sensory Signals in the Cerebellar Interpositus. J. Neurosci. 2013, 33, 1198–1210. [Google Scholar] [CrossRef]
- Shankar Kikkeri, N.; Nagalli, S. Trigeminal Neuralgia. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Go, J.L.; Kim, P.E.; Zee, C.S. The Trigeminal Nerve. Semin. Ultrasound CT MR 2001, 22, 502–520. [Google Scholar] [CrossRef]
- Zieliński, G.; Byś, A.; Szkutnik, J.; Majcher, P.; Ginszt, M. Electromyographic Patterns of Masticatory Muscles in Relation to Active Myofascial Trigger Points of the Upper Trapezius and Temporomandibular Disorders. Diagnostics 2021, 11, 580. [Google Scholar] [CrossRef]
- Christensen, L.V.; Radue, J.T. Lateral Preference in Mastication: An Electromyographic Study. J. Oral Rehabil. 1985, 12, 429–434. [Google Scholar] [CrossRef]
- Frayne, E.; Coulson, S.; Adams, R.; Croxson, G.; Waddington, G. Laterality of Proprioception in the Orofacial Muscles and Temporomandibular Joint. Neurosci. Lett. 2016, 635, 111–116. [Google Scholar] [CrossRef]
- Pan, C.W.; Klein, B.E.; Cotch, M.F.; Shrager, S.; Klein, R.; Folsom, A.; Kronmal, R.; Shea, S.J.; Burke, G.L.; Saw, S.M.; et al. Racial Variations in the Prevalence of Refractive Errors in the United States: The Multi-Ethnic Study of Atherosclerosis. Am. J. Ophthalmol. 2013, 155, 1129–1138.e1. [Google Scholar] [CrossRef] [Green Version]
- Luong, T.Q.; Shu, Y.-H.; Modjtahedi, B.S.; Fong, D.S.; Choudry, N.; Tanaka, Y.; Nau, C.L. Racial and Ethnic Differences in Myopia Progression in a Large, Diverse Cohort of Pediatric Patients. Investig. Ophthalmol. Vis. Sci. 2020, 61, 20. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Myopia Subject (n = 21) | Subject without Refractive Error (n = 19) | |||||||
|---|---|---|---|---|---|---|---|---|
| Side | Mean | SD | Mean | SD | Test | p | ||
| Refractive Error (Dsph) | R | −3.00 | 0.50 | NA | NA | NA | NA | |
| L | −3.00 | 1.50 | ||||||
| Axial Length (mm) | R | 24.27 | 0.69 | 23.30 | 0.55 | t | 4.85 | 0.00 * ES = 1.56 |
| L | 24.31 | 0.84 | 23.27 | 0.56 | t | 4.51 | 0.00 * ES = 1.46 | |
| Retinal Thickness (μm) | R | 252.71 | 18.14 | 244.26 | 12.16 | t | 1.71 | 0.10 |
| L | 245.95 | 31.10 | 242.11 | 11.89 | z | 1.30 | 0.19 | |
| Choroidal Thickness (μm) | R | 349.05 | 82.86 | 343.32 | 82.53 | t | 0.22 | 0.83 |
| L | 322.86 | 83.71 | 328.89 | 84.29 | t | −0.23 | 0.82 | |
| Intraocular Pressure (mmHg) | R | 16.10 | 4.07 | 15.11 | 4.29 | t | 0.75 | 0.46 |
| L | 15.48 | 4.20 | 14.79 | 3.85 | t | 0.54 | 0.59 | |
| Myopia Subject (n = 21) | Subject without Refractive Error (n = 19) | Test | p | ||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||
| TA RestR (mm) | 13.18 | 1.78 | 12.20 | 1.48 | t | 1.90 | 0.06 |
| TA ClenchR (mm) | 13.86 | 1.82 | 12.77 | 1.49 | t | 2.06 | 0.04 * ES = 0.60 |
| MM RestR (mm) | 11.94 | 2.18 | 12.42 | 1.51 | t | −0.81 | 0.42 |
| MM ClenchR (mm) | 13.48 | 2.39 | 13.52 | 1.58 | t | −0.05 | 0.96 |
| DA RestR (mm) | 6.55 | 0.63 | 6.67 | 0.81 | z | −0.33 | 0.75 |
| DA ClenchR (mm) | 6.47 | 0.55 | 6.67 | 0.83 | z | −0.64 | 0.52 |
| SCM RestR (mm) | 9.36 | 1.37 | 10.25 | 1.37 | t | −2.05 | 0.04 * ES = 0.65 |
| SCM ClenchR (mm) | 9.37 | 1.31 | 10.26 | 1.42 | t | −2.06 | 0.04 * ES = 0.69 |
| TAR (μV) | 1.80 | 0.84 | 2.05 | 1.99 | z | 0.66 | 0.51 |
| MMR (μV) | 2.53 | 1.67 | 2.18 | 1.31 | z | 0.58 | 0.56 |
| DAR (μV) | 1.30 | 0.37 | 1.16 | 0.39 | z | −0.96 | 0.34 |
| SCMR (μV) | 1.70 | 0.75 | 1.93 | 0.76 | z | 1.57 | 0.12 |
| TA RestL (mm) | 12.25 | 1.78 | 12.20 | 1.90 | z | −0.03 | 0.98 |
| TA ClenchL (mm) | 12.88 | 1.87 | 12.80 | 2.00 | z | 0.22 | 0.83 |
| MM RestL (mm) | 12.43 | 2.30 | 12.69 | 1.55 | z | −1.02 | 0.31 |
| MM ClenchL (mm) | 13.78 | 2.40 | 13.75 | 1.53 | z | −0.03 | 0.98 |
| DA RestL (mm) | 6.70 | 0.97 | 6.56 | 0.75 | t | 0.37 | 0.71 |
| DA ClenchL (mm) | 6.61 | 0.98 | 6.58 | 0.74 | t | 0.09 | 0.93 |
| SCM RestL (mm) | 9.51 | 1.55 | 10.00 | 1.14 | t | −1.12 | 0.27 |
| SCM ClenchL (mm) | 9.56 | 1.55 | 9.99 | 1.15 | t | −1.00 | 0.33 |
| TAL (μV) | 1.90 | 0.93 | 2.30 | 1.80 | z | −0.35 | 0.72 |
| MML (μV) | 2.01 | 1.09 | 2.40 | 1.65 | z | −1.14 | 0.26 |
| DAL (μV) | 1.40 | 0.49 | 1.33 | 0.45 | z | −0.22 | 0.83 |
| SCML (μV) | 1.71 | 0.75 | 1.63 | 0.54 | z | 0.50 | 0.62 |
| Myopia Subject | Subject without Refractive Error | ||||
|---|---|---|---|---|---|
| r | p | r | p | ||
| Axial LengthR (mm) | TA RestR (mm) | 0.18 p | 0.43 | 0.33 p | 0.17 |
| TA ClenchR (mm) | 0.24 p | 0.30 | 0.32 p | 0.19 | |
| MM RestR (mm) | 0.08 p | 0.72 | 0.52 p | 0.02 * | |
| MM ClenchR (mm) | 0.06 p | 0.80 | 0.62 p | 0.00 * | |
| DA RestR (mm) | 0.28 s | 0.21 | −0.05 p | 0.85 | |
| DA ClenchR (mm) | 0.18 s | 0.43 | −0.03 p | 0.92 | |
| SCM RestR (mm) | −0.23 p | 0.31 | −0.28 p | 0.24 | |
| SCM ClenchR (mm) | −0.23 p | 0.32 | −0.30 p | 0.21 | |
| TAR (μV) | −0.24 s | 0.29 | 0.14 s | 0.57 | |
| MMR (μV) | 0.34 s | 0.13 | −0.03 s | 0.90 | |
| DAR (μV) | −0.23 p | 0.32 | 0.20 s | 0.41 | |
| SCMR (μV) | 0.29 p | 0.20 | 0.23 s | 0.35 | |
| Retinal Thickness R ( μm) | TA RestR (mm) | 0.40 p | 0.07 | −0.15 p | 0.53 |
| TA ClenchR (mm) | 0.38 p | 0.09 | −0.24 p | 0.32 | |
| MM RestR (mm) | −0.28 p | 0.21 | −0.17 p | 0.49 | |
| MM ClenchR (mm) | −0.09 p | 0.69 | −0.06 p | 0.82 | |
| DA RestR (mm) | −0.09 s | 0.71 | −0.03 p | 0.89 | |
| DA ClenchR (mm) | −0.13 s | 0.59 | −0.07 p | 0.76 | |
| SCM RestR (mm) | −0.26 p | 0.25 | −0.47 p | 0.04 * | |
| SCM ClenchR (mm) | −0.25 p | 0.27 | −0.48 p | 0.04 * | |
| TAR (μV) | −0.52 s | 0.02 * | −0.21 s | 0.39 | |
| MMR (μV) | −0.23 s | 0.31 | 0.12 s | 0.62 | |
| DAR (μV) | −0.28 p | 0.22 | 0.36 s | 0.13 | |
| SCMR (μV) | −0.03 p | 0.91 | 0.07 s | 0.77 | |
| Choroidal Thickness R ( μm) | TA RestR (mm) | 0.38 p | 0.09 | −0.17 p | 0.48 |
| TA ClenchR (mm) | 0.37 p | 0.10 | −0.16 p | 0.51 | |
| MM RestR (mm) | −0.08 p | 0.72 | −0.33 p | 0.17 | |
| MM ClenchR (mm) | 0.02 p | 0.92 | −0.22 p | 0.36 | |
| DA RestR (mm) | −0.19 s | 0.41 | −0.13 p | 0.59 | |
| DA ClenchR (mm) | −0.28 s | 0.23 | −0.14 p | 0.56 | |
| SCM RestR (mm) | −0.09 p | 0.69 | 0.18 p | 0.46 | |
| SCM ClenchR (mm) | −0.13 p | 0.57 | 0.19 p | 0.44 | |
| TAR (μV) | 0.29 s | 0.21 | −0.28 s | 0.24 | |
| MMR (μV) | 0.19 s | 0.41 | −0.10 s | 0.69 | |
| DAR (μV) | 0.10 p | 0.66 | 0.08 s | 0.74 | |
| SCMR (μV) | 0.37 p | 0.09 | −0.21 s | 0.39 | |
| Intraocular PressureR (mmHg) | TA RestR (mm) | 0.16 p | 0.49 | 0.37 p | 0.11 |
| TA ClenchR (mm) | 0.18 p | 0.43 | 0.34 p | 0.15 | |
| MM RestR (mm) | −0.04 p | 0.88 | −0.07 p | 0.78 | |
| MM ClenchR (mm) | 0.09 p | 0.70 | −0.08 p | 0.74 | |
| DA RestR (mm) | 0.36 s | 0.11 | −0.14 p | 0.58 | |
| DA ClenchR (mm) | 0.40 s | 0.08 | −0.10 p | 0.69 | |
| SCM RestR (mm) | −0.23 p | 0.31 | −0.14 p | 0.57 | |
| SCM ClenchR (mm) | −0.23 p | 0.31 | −0.15 p | 0.55 | |
| TAR (μV) | 0.33 s | 0.14 | 0.10 s | 0.68 | |
| MMR (μV) | 0.08 s | 0.74 | −0.31 s | 0.19 | |
| DAR (μV) | 0.17 p | 0.46 | 0.07 s | 0.78 | |
| SCMR (μV) | −0.20 p | 0.38 | −0.49 s | 0.03 * | |
| Myopia Subject | Subject without Refractive Error | ||||
|---|---|---|---|---|---|
| r | p | r | p | ||
| Axial LengthL (mm) | TA RestL (mm) | −0.08 p | 0.72 | 0.28 s | 0.25 |
| TA ClenchL (mm) | 0.18 p | 0.43 | 0.32 s | 0.19 | |
| MM RestL (mm) | 0.27 s | 0.23 | 0.21 p | 0.39 | |
| MM ClenchL (mm) | 0.19 p | 0.41 | 0.38 p | 0.10 | |
| DA RestL (mm) | 0.12 p | 0.60 | −0.22 s | 0.37 | |
| DA ClenchL (mm) | 0.06 p | 0.79 | −0.30 p | 0.21 | |
| SCM RestL (mm) | −0.23 p | 0.33 | 0.03 p | 0.91 | |
| SCM ClenchL (mm) | −0.13 s | 0.58 | 0.02 p | 0.94 | |
| TAL (μV) | −0.76 s | 0.00 * | 0.00 s | 1.00 | |
| MML (μV) | 0.03 s | 0.91 | 0.21 s | 0.38 | |
| DAL (μV) | −0.12 s | 0.61 | 0.43 p | 0.07 | |
| SCML (μV) | −0.37 s | 0.10 | 0.36 s | 0.13 | |
| Retinal ThicknessL (μm) | TA RestL (mm) | −0.16 s | 0.48 | −0.06 s | 0.80 |
| TA ClenchL (mm) | −0.09 s | 0.68 | −0.03 s | 0.92 | |
| MM RestL (mm) | 0.21 s | 0.37 | 0.00 p | 1.00 | |
| MM ClenchL (mm) | 0.10 s | 0.68 | 0.03 p | 0.89 | |
| DA RestL (mm) | 0.07 s | 0.76 | 0.04 s | 0.86 | |
| DA ClenchL (mm) | −0.05 s | 0.83 | 0.01 p | 0.98 | |
| SCM RestL (mm) | −0.15 s | 0.53 | −0.10 p | 0.68 | |
| SCM ClenchL (mm) | −0.12 s | 0.59 | −0.11 p | 0.65 | |
| TAL (μV) | −0.26 s | 0.25 | −0.11 s | 0.66 | |
| MML (μV) | −0.17 s | 0.45 | −0.05 s | 0.85 | |
| DAL (μV) | 0.07 s | 0.77 | 0.39 p | 0.09 | |
| SCML (μV) | −0.12 s | 0.60 | 0.00 s | 0.99 | |
| Choroidal thicknessL (μm) | TA RestL (mm) | 0.06 p | 0.80 | 0.17 s | 0.48 |
| TA ClenchL (mm) | −0.15 p | 0.52 | 0.09 s | 0.73 | |
| MM RestL (mm) | −0.19 s | 0.40 | −0.31 p | 0.20 | |
| MM ClenchL (mm) | −0.21 p | 0.36 | −0.20 p | 0.41 | |
| DA RestL (mm) | −0.18 p | 0.42 | −0.16 s | 0.50 | |
| DA ClenchL (mm) | 0.04 p | 0.87 | −0.22 p | 0.36 | |
| SCM RestL (mm) | −0.01 p | 0.97 | 0.28 p | 0.24 | |
| SCM ClenchL (mm) | −0.04 s | 0.88 | 0.29 p | 0.23 | |
| TAL (μV) | 0.53 s | 0.01 * | −0.27 s | 0.26 | |
| MML (μV) | 0.09 s | 0.71 | 0.08 s | 0.75 | |
| DAL (μV) | 0.06 s | 0.78 | 0.12 | 0.63 | |
| SCML (μV) | 0.46 s | 0.04 * | 0.20 s | 0.42 | |
| Intraocular Pressure L (mmHg) | TA RestL (mm) | 0.35 p | 0.12 | 0.09 s | 0.71 |
| TA ClenchL (mm) | 0.29 p | 0.20 | 0.09 s | 0.71 | |
| MM RestL (mm) | −0.10 s | 0.66 | 0.11 p | 0.65 | |
| MM ClenchL (mm) | 0.08 p | 0.73 | 0.13 p | 0.58 | |
| DA RestL (mm) | 0.43 p | 0.05 | 0.39 s | 0.10 | |
| DA ClenchL (mm) | 0.48 p | 0.03 * | 0.36 p | 0.14 | |
| SCM RestL (mm) | −0.13 p | 0.58 | 0.08 p | 0.75 | |
| SCM ClenchL (mm) | −0.24 s | 0.30 | 0.07 p | 0.77 | |
| TAL (μV) | 0.22 s | 0.33 | −0.11 s | 0.65 | |
| MML (μV) | −0.04 s | 0.88 | −0.08 s | 0.73 | |
| DAL (μV) | −0.31 s | 0.17 | 0.06 p | 0.79 | |
| SCML (μV) | 0.16 s | 0.50 | −0.17 s | 0.48 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zieliński, G.; Wójcicki, M.; Rapa, M.; Matysik-Woźniak, A.; Baszczowski, M.; Ginszt, M.; Litko-Rola, M.; Szkutnik, J.; Różyło-Kalinowska, I.; Rejdak, R.; et al. Masticatory Muscle Thickness and Activity Correlates to Eyeball Length, Intraocular Pressure, Retinal and Choroidal Thickness in Healthy Women versus Women with Myopia. J. Pers. Med. 2022, 12, 626. https://doi.org/10.3390/jpm12040626
Zieliński G, Wójcicki M, Rapa M, Matysik-Woźniak A, Baszczowski M, Ginszt M, Litko-Rola M, Szkutnik J, Różyło-Kalinowska I, Rejdak R, et al. Masticatory Muscle Thickness and Activity Correlates to Eyeball Length, Intraocular Pressure, Retinal and Choroidal Thickness in Healthy Women versus Women with Myopia. Journal of Personalized Medicine. 2022; 12(4):626. https://doi.org/10.3390/jpm12040626
Chicago/Turabian StyleZieliński, Grzegorz, Marcin Wójcicki, Maria Rapa, Anna Matysik-Woźniak, Michał Baszczowski, Michał Ginszt, Monika Litko-Rola, Jacek Szkutnik, Ingrid Różyło-Kalinowska, Robert Rejdak, and et al. 2022. "Masticatory Muscle Thickness and Activity Correlates to Eyeball Length, Intraocular Pressure, Retinal and Choroidal Thickness in Healthy Women versus Women with Myopia" Journal of Personalized Medicine 12, no. 4: 626. https://doi.org/10.3390/jpm12040626