
A Simple Clinical Scoring System to Determine the Risk of Pancreatic Cancer in the General Population
 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Data Collection
2.3. Scoring System Development
2.4. Validation of the Scoring System
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Individuals in the Test Set
3.2. Clinical Data Associated with PC and the Development of a Simple Clinical Scoring System
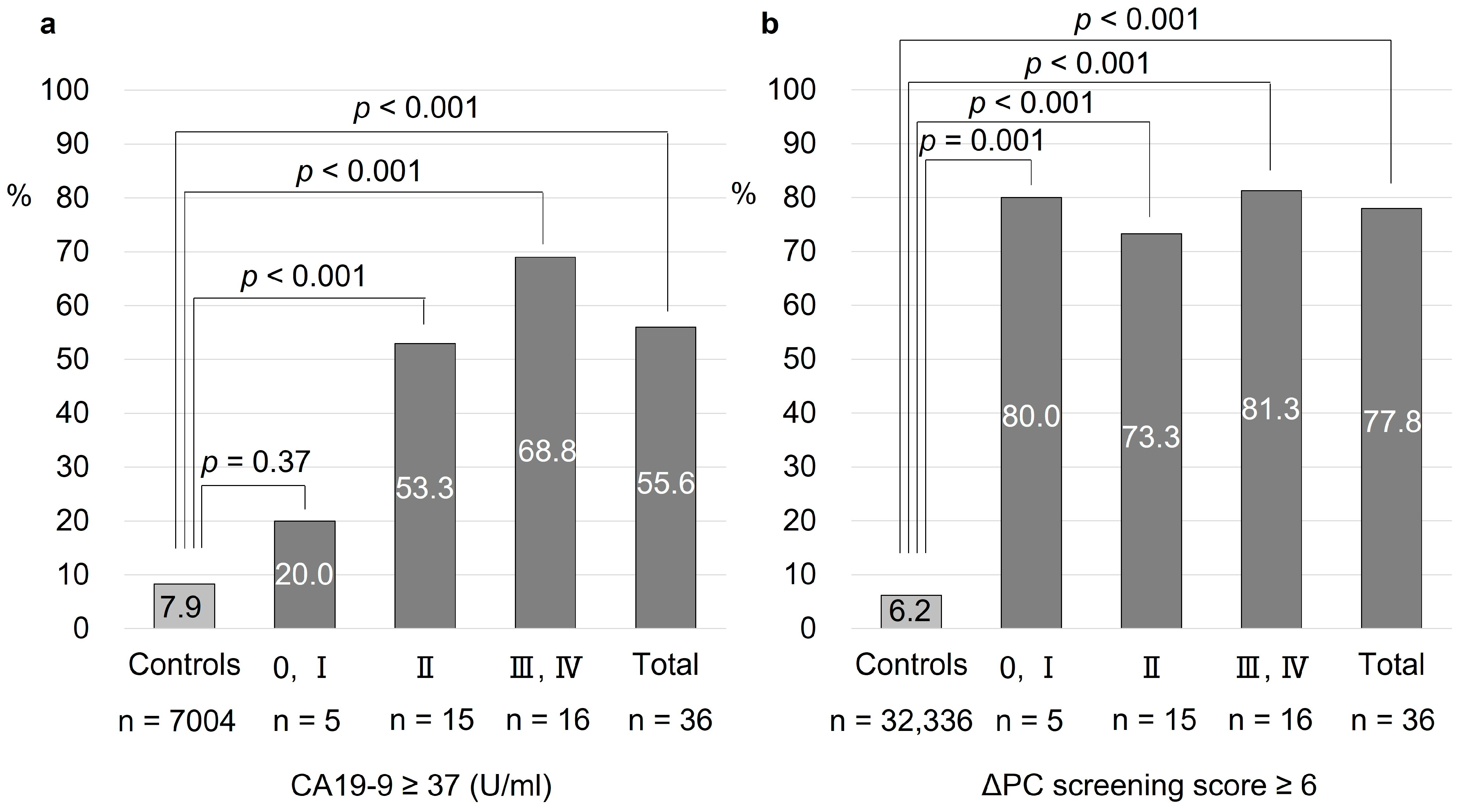
3.3. Validation of the ΔPC Screening Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA. Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Viale, P.H. The American Cancer Society’s facts and figures: 2020 edition. J. Adv. Pract. Oncol. 2020, 11, 135. [Google Scholar]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting Cancer Incidence and Deaths to 2030: The Unexpected Burden of Thyroid, Liver, and Pancreas Cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed]
- Kanno, A.; Masamune, A.; Hanada, K.; Maguchi, H.; Shimizu, Y.; Ueki, T.; Hasebe, O.; Ohtsuka, T.; Nakamura, M.; Takenaka, M.; et al. Multicenter Study of Early Pancreatic Cancer in Japan. Pancreatology 2018, 18, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Egawa, S.; Toma, H.; Ohigashi, H.; Okusaka, T.; Nakao, A.; Hatori, T.; Maguchi, H.; Yanagisawa, A.; Tanaka, M. Japan Pancreatic Cancer Registry; 30th Year Anniversary: Japan pancreas society. Pancreas 2012, 41, 985–992. [Google Scholar] [CrossRef]
- Canto, M.I.; Harinck, F.; Hruban, R.H.; Offerhaus, G.J.; Poley, J.W.; Kamel, I.; Nio, Y.; Schulick, R.S.; Bassi, C.; Kluijt, I.; et al. International Cancer of the Pancreas Screening (CAPS) Consortium Summit on the Management of Patients with Increased Risk for Familial Pancreatic Cancer. Gut 2013, 62, 339–347. [Google Scholar] [CrossRef]
- Chari, S.T. Detecting Early Pancreatic Cancer: Problems and Prospects. Semin. Oncol. 2007, 34, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Kenner, B.J.; Chari, S.T.; Cleeter, D.F.; Go, V.L.W. Early Detection of Sporadic Pancreatic Cancer: Strategic Map for Innovation—A White Paper. Pancreas 2015, 44, 686–692. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.H.; Lee, J.M.; Cho, J.Y.; Lee, K.B.; Kim, J.E.; Moon, S.K.; Kim, S.J.; Baek, J.H.; Kim, S.H.; Kim, S.H.; et al. Small (≤20 Mm) Pancreatic Adenocarcinomas: Analysis of Enhancement Patterns and Secondary Signs with Multiphasic Multidetector CT. Radiology 2011, 259, 442–452. [Google Scholar] [CrossRef] [PubMed]
- Izumi, Y.; Hanada, K.; Okazaki, A.; Minami, T.; Hirano, N.; Ikemoto, J.; Kanemitsu, K.; Nakadoi, K.; Shishido, T.; Katamura, Y.; et al. Endoscopic Ultrasound Findings and Pathological Features of Pancreatic Carcinoma in Situ. Endosc. Int. Open 2019, 7, E585–E593. [Google Scholar] [CrossRef]
- Mikata, R.; Ishihara, T.; Tada, M.; Tawada, K.; Saito, M.; Kurosawa, J.; Sugiyama, H.; Sakai, Y.; Tsuyuguchi, T.; Miyazaki, M.; et al. Clinical Usefulness of Repeated Pancreatic Juice Cytology via Endoscopic Naso-Pancreatic Drainage Tube in Patients with Pancreatic Cancer. J. Gastroenterol. 2013, 48, 866–873. [Google Scholar] [CrossRef]
- Hanada, K.; Minami, T.; Shimizu, A.; Fukuhara, M.; Yano, S.; Sasaki, K.; Koda, M.; Sugiyama, K.; Yonehara, S.; Yanagisawa, A. Roles of ERCP in the Early Diagnosis of Pancreatic Cancer. Diagnostics 2019, 9, 30. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the Freely Available Easy-to-Use Software “EZR” for Medical Statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Honda, K.; Kobayashi, M.; Okusaka, T.; Rinaudo, J.A.; Huang, Y.; Marsh, T.; Sanada, M.; Sasajima, Y.; Nakamori, S.; Shimahara, M.; et al. Plasma Biomarker for Detection of Early Stage Pancreatic Cancer and Risk Factors for Pancreatic Malignancy Using Antibodies for Apolipoprotein-AII Isoforms. Sci. Rep. 2015, 5, 15921. [Google Scholar] [CrossRef]
- Radon, T.P.; Massat, N.J.; Jones, R.; Alrawashdeh, W.; Dumartin, L.; Ennis, D.; Duffy, S.W.; Kocher, H.M.; Pereira, S.P.; Guarner, L.; et al. Identification of a Three-Biomarker Panel in Urine for Early Detection of Pancreatic Adenocarcinoma. Clin. Cancer Res. 2015, 21, 3512–3521. [Google Scholar] [CrossRef]
- Que, R.; Ding, G.; Chen, J.; Cao, L. Analysis of Serum Exosomal MicroRNAs and Clinicopathologic Features of Patients with Pancreatic Adenocarcinoma. World J. Surg. Oncol. 2013, 11, 219. [Google Scholar] [CrossRef]
- Pang, T.; Ding, G.; Wu, Z.; Jiang, G.; Yang, Y.; Zhang, X. A Novel Scoring System to Analyze Combined Effect of Lifestyle Factors on Pancreatic Cancer Risk: A Retrospective Case-Control Study. Sci. Rep. 2017, 7, 13657. [Google Scholar] [CrossRef] [PubMed]
- Klein, A.P.; Lindström, S.; Mendelsohn, J.B.; Steplowski, E.; Arslan, A.A.; Bueno-de-Mesquita, H.B.; Fuchs, C.S.; Gallinger, S.; Gross, M.; Helzlsouer, K.; et al. An Absolute Risk Model to Identify Individuals at Elevated Risk for Pancreatic Cancer in the General Population. PLoS ONE 2013, 8, e72311. [Google Scholar] [CrossRef] [PubMed]
- Yu, A.; Woo, S.M.; Joo, J.; Yang, H.R.; Lee, W.J.; Park, S.J.; Nam, B.H. Development and Validation of a Prediction Model to Estimate Individual Risk of Pancreatic Cancer. PLoS ONE 2016, 11, e0146473. [Google Scholar] [CrossRef] [PubMed]
- Nakatochi, M.; Lin, Y.; Ito, H.; Hara, K.; Kinoshita, F.; Kobayashi, Y.; Ishii, H.; Ozaka, M.; Sasaki, T.; Sasahira, N.; et al. Prediction Model for Pancreatic Cancer Risk in the General Japanese Population. PLoS ONE 2018, 13, e0203386. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Vergouwe, Y. Towards Better Clinical Prediction Models: Seven Steps for Development and an ABCD for Validation. Eur. Heart J. 2014, 35, 1925–1931. [Google Scholar] [CrossRef] [PubMed]
- Silverman, D.T.; Schiffman, M.; Everhart, J.; Goldstein, A.; Lillemoe, K.D.; Swanson, G.M.; Schwartz, A.G.; Brown, L.M.; Greenberg, R.S.; Schoenberg, J.B.; et al. Diabetes Mellitus, Other Medical Conditions and Familial History of Cancer as Risk Factors for Pancreatic Cancer. Br. J. Cancer 1999, 80, 1830–1837. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Kandlakunta, H.; Nagpal, S.J.S.; Feng, Z.; Hoos, W.; Petersen, G.M.; Chari, S.T. Model to Determine Risk of Pancreatic Cancer in Patients with New-Onset Diabetes. Gastroenterology 2018, 155, 730–739.e3. [Google Scholar] [CrossRef] [PubMed]
- Carreras-Torres, R.; Johansson, M.; Gaborieau, V.; Haycock, P.C.; Wade, K.H.; Relton, C.L.; Martin, R.M.; Smith, G.D.; Brennan, P. The Role of Obesity, Type 2 Diabetes, and Metabolic Factors in Pancreatic Cancer: A Mendelian Randomization Study. J. Natl. Cancer Inst. 2017, 109, djx012. [Google Scholar] [CrossRef]
- Sah, R.P.; Sharma, A.; Nagpal, S.; Patlolla, S.H.; Sharma, A.; Kandlakunta, H.; Anani, V.; Angom, R.S.; Kamboj, A.K.; Ahmed, N.; et al. Phases of Metabolic and Soft Tissue Changes in Months Preceding a Diagnosis of Pancreatic Ductal Adenocarcinoma. Gastroenterology 2019, 156, 1742–1752. [Google Scholar] [CrossRef]
- Toft, J.; Hadden, W.J.; Laurence, J.M.; Lam, V.; Yuen, L.; Janssen, A.; Pleass, H. Imaging Modalities in the Diagnosis of Pancreatic Adenocarcinoma: A Systematic Review and Meta-Analysis of Sensitivity, Specificity and Diagnostic Accuracy. Eur. J. Radiol. 2017, 92, 17–23. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| PC Group | Control Group | ||||
|---|---|---|---|---|---|
| n = 45 | n = 450 | p Value | |||
| Age (years) | 70 | (64–77) | 70 | (64–77) | 1 |
| Sex (male) | 22 | (48.9) | 220 | (48.9) | 1 |
| BMI | 22.6 | (20.7–26.0) | 22.6 | (20.6–24.5) | 0.75 |
| Alcohol consumption (g/day) | |||||
| ≥0, <20 | 36 | (80.0) | 400 | (88.9) | 0.091 |
| ≥20, <60 | 8 | (17.8) | 47 | (10.4) | 0.14 |
| ≥60 | 1 | (2.2) | 3 | (0.7) | 0.32 |
| Smoking | |||||
| Never | 31 | (68.9) | 278 | (61.8) | 0.42 |
| Past | 12 | (26.7) | 136 | (30.2) | 0.73 |
| Current | 2 | (4.4) | 36 | (8.0) | 0.56 |
| Development Set | ||
|---|---|---|
| n = 45 | ||
| Location | ||
| Ph | 19 | (42.2) |
| Pb | 17 | (37.8) |
| Pt | 9 | (20.0) |
| Tumor size (mm) | ||
| ≥0, ≤20 | 11 | (24.4) |
| >20, ≤40 | 28 | (62.2) |
| >40, ≤60 | 3 | (6.7) |
| >60 | 3 | (6.7) |
| UICC Stage | ||
| 0, Ⅰ | 4 | (8.9) |
| Ⅱ | 22 | (48.9) |
| Ⅲ | 4 | (8.9) |
| Ⅳ | 15 | (33.3) |
| Treatment | ||
| Surgery | 25 | (55.6) |
| Chemotherapy | 17 | (37.8) |
| Best supportive care | 3 | (6.7) |
| PC Group | Control Group | Univariate | Multivariate | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n = 45 | n = 450 | p Value | p Value | OR | (95%CI) | ||||
| A. Clinical data at diagnosis of PC | |||||||||
| BMI | <18.5 | 4 | (8.9) | 41 | (9.1) | 0.77 | |||
| BMI | ≥25 | 12 | (26.7) | 89 | (19.8) | 0.33 | |||
| RBC | ≤4.0 (×103/μL) | 10 | (22.2) | 63 | (14.0) | 0.18 | |||
| Hemoglobin | ≤12.0 (g/dL) | 5 | (11.1) | 43 | (9.6) | 0.79 | |||
| Hematocrit | ≤36.0 (%) | 4 | (8.9) | 41 | (9.1) | 1 | |||
| Platelet count | ≤140 (×103/μL) | 1 | (2.2) | 44 | (9.8) | 0.35 | |||
| Albumin | ≤3.8 (mg/dL) | 2 | (4.4) | 43 | (9.6) | 0.57 | |||
| Trigliceride | ≤150 (mg/dL) | 6 | (13.3) | 51 | (11.3) | 0.63 | |||
| HDL | ≤60 (mg/dL) | 3 | (6.7) | 30 | (6.7) | 1 | |||
| LDL | ≥110 (mg/dL) | 9 | (20.0) | 103 | (22.9) | 0.85 | |||
| AST | ≥35 (U/L) | 6 | (13.3) | 32 | (7.1) | 0.14 | |||
| ALT | ≥35 (U/L) | 4 | (8.9) | 30 | (6.7) | 0.53 | |||
| ALP | ≥350 (U/L) | 2 | (4.4) | 24 | (5.3) | 1 | |||
| Glucose | ≥110 (mg/dL) | 23 | (51.1) | 97 | (21.6) | <0.001 | |||
| HbA1c | ≥6.5 (%) | 13 | (28.9) | 39 | (8.7) | <0.001 | 0.78 | 1.15 | (0.43–3.07) |
| B. Change in clinical data from one year before diagnosis (Δ) | |||||||||
| ΔBMI | ≤−0.5 | 20 | (44.4) | 114 | (25.3) | 0.008 | 0.013 | 2.42 | (1.21–4.85) |
| ΔRBC | ≤−0.2 (×103/μL) | 17 | (37.8) | 91 | (20.2) | 0.013 | 0.065 | 2.04 | (0.96–4.36) |
| ΔHemoglobin | ≤−0.5 (g/dL) | 17 | (37.8) | 110 | (24.4) | 0.072 | |||
| ΔHematocrit | ≤−1.0 (%) | 20 | (44.4) | 141 | (31.3) | 0.094 | |||
| ΔPlatelet count | ≤−20 (×103/μL) | 9 | (20.0) | 68 | (15.1) | 0.39 | |||
| ΔAlbumin | ≤−0.3 (mg/dL) | 6 | (13.3) | 63 | (14.0) | 1 | |||
| ΔTrigliceride | ≤−10 (mg/dL) | 23 | (51.1) | 169 | (37.6) | 0.079 | |||
| ΔHDL | ≤−10 (mg/dL) | 1 | (2.2) | 27 | (6.0) | 0.50 | |||
| ΔLDL | ≤−20 (mg/dL) | 14 | (31.1) | 48 | (10.7) | <0.001 | 0.048 | 2.31 | (1.01–5.31) |
| ΔAST | ≥5 (U/L) | 7 | (15.6) | 71 | (15.8) | 1 | |||
| ΔALT | ≥5 (U/L) | 12 | (26.7) | 65 | (14.4) | 0.049 | 0.16 | 1.82 | (0.79–4.17) |
| ΔALP | ≥10 (U/L) | 12 | (26.7) | 159 | (35.3) | 0.32 | |||
| ΔGlucose | ≥10 (mg/dL) | 12 | (26.7) | 37 | (8.2) | <0.001 | |||
| ΔHbA1c | ≥0.3 (%) | 18 | (40.0) | 30 | (6.7) | <0.001 | <0.001 | 8.29 | (3.39–20.30) |
| Score | Score Range | |
|---|---|---|
| ΔLDL (mg/dL) | 0–2 | |
| ≤−20 | 2 | |
| >-20, ≤−10 | 1 | |
| >−10 | 0 | |
| ΔHbA1c (%) | 0–5 | |
| ≥0.3 | 5 | |
| ≥0.1, ˂0.3 | 2 | |
| ˂0.1 | 0 | |
| ΔBMI | 0–2 | |
| ≤−0.5 | 2 | |
| >−0.5, ≤0 | 1 | |
| >0 | 0 | |
| Abdominal ultrasound | 0–14 | |
| Pancreatic tumor | 6 | |
| Main pancreatic duct dilation | 6 | |
| Pancreatic cyst | 2 | |
| Total | 0–23 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshimura, D.; Fukasawa, M.; Yoda, Y.; Ohtaka, M.; Ooka, T.; Takano, S.; Kawakami, S.; Fukasawa, Y.; Kuratomi, N.; Harai, S.; et al. A Simple Clinical Scoring System to Determine the Risk of Pancreatic Cancer in the General Population. Diagnostics 2024, 14, 651. https://doi.org/10.3390/diagnostics14060651
Yoshimura D, Fukasawa M, Yoda Y, Ohtaka M, Ooka T, Takano S, Kawakami S, Fukasawa Y, Kuratomi N, Harai S, et al. A Simple Clinical Scoring System to Determine the Risk of Pancreatic Cancer in the General Population. Diagnostics. 2024; 14(6):651. https://doi.org/10.3390/diagnostics14060651
Chicago/Turabian StyleYoshimura, Dai, Mitsuharu Fukasawa, Yoshioki Yoda, Masahiko Ohtaka, Tadao Ooka, Shinichi Takano, Satoshi Kawakami, Yoshimitsu Fukasawa, Natsuhiko Kuratomi, Shota Harai, and et al. 2024. "A Simple Clinical Scoring System to Determine the Risk of Pancreatic Cancer in the General Population" Diagnostics 14, no. 6: 651. https://doi.org/10.3390/diagnostics14060651