
Comparison between Ultrasound-Guided and Palpatory Localization of the Dorsal Joint Space of the Shoulder Joint

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participant Recruitment and Inclusion and Exclusion Criteria
2.3. Study Procedure, Materials, and Evaluation
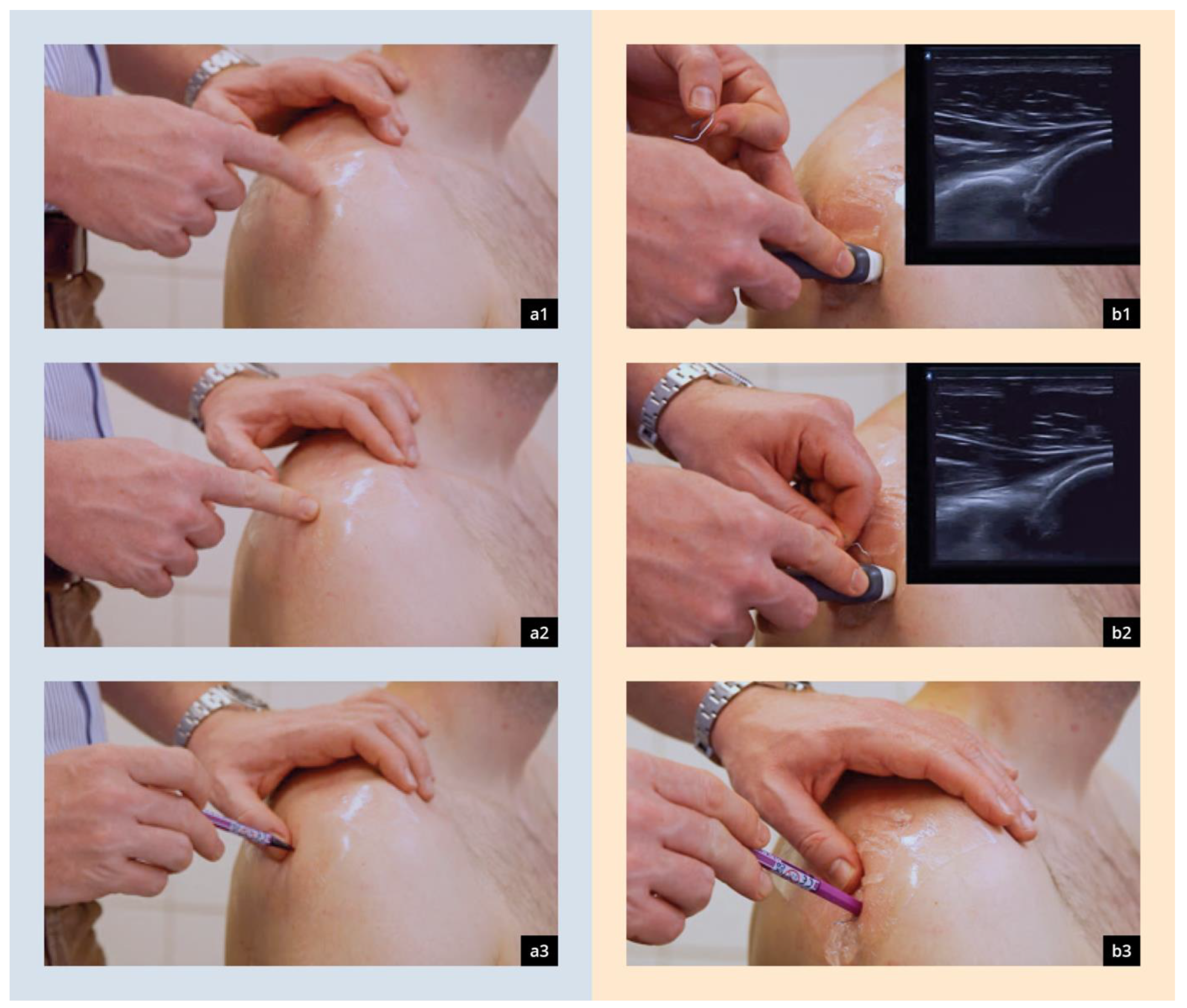
2.3.1. Palpatory Localization of the Dorsal Joint Space
2.3.2. Ultrasound-Guided Localization of the Dorsal Joint Space

2.4. Cut-Off for Experienced Participants
2.5. Statistical Analysis
3. Results
3.1. Demography
3.2. Palpatory Localization (PalpMethod)
3.3. Ultrasound-Guided Localization (SonoMethod)
3.4. Comparative Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bernau, A.; Heeg, P. Intraarticular punctures and injections: Indications--prevention of infection--technique--complications. Orthopade 2003, 32, 548–569; quiz 569–570. [Google Scholar] [CrossRef] [PubMed]
- Baruffi, S.; Saber, A.Y.; Martins, T.; Varacallo, M. Shoulder Arthrocentesis Technique; StatPearls Publishing Copyright © 2023; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2023. [Google Scholar]
- Kerlan, R.K.; Glousman, R.E. Injections and techniques in athletic medicine. Clin. Sports Med. 1989, 8, 541–560. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, R.C.; Zanaboni, A.; Genninger, J.; Costantino, T.G. Ultrasound-versus landmark-guided medium-sized joint arthrocentesis: A randomized clinical trial. Acad. Emerg. Med. 2022, 29, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, M.J.; Kumar, S.; Chandan, C.B.; Kumar, P.; Kumar, B.; Sinha, R.R.; Kumar, A. Morphometry and Morphology of the Acromion Process and Its Implications in Subacromial Impingement Syndrome. Cureus 2023, 15, e44329. [Google Scholar] [CrossRef] [PubMed]
- Castagna, A.; Conti, M.; Mouhsine, E.; Bungaro, P.; Garofalo, R. Arthroscopic biceps tendon tenodesis: The anchorage technical note. Knee Surg. Sports Traumatol. Arthrosc. 2006, 14, 581–585. [Google Scholar] [CrossRef] [PubMed]
- Castagna, A.; Mouhsine, E.; Conti, M.; Vinci, E.; Borroni, M.; Giardella, A.; Garofalo, R. Chondral print on humeral head: An indirect sign of long head biceps tendon instability. Knee Surg. Sports Traumatol. Arthrosc. 2007, 15, 645–648. [Google Scholar] [CrossRef] [PubMed]
- Youm, T.; Murray, D.H.; Kubiak, E.N.; Rokito, A.S.; Zuckerman, J.D. Arthroscopic versus mini-open rotator cuff repair: A comparison of clinical outcomes and patient satisfaction. J. Shoulder Elbow Surg. 2005, 14, 455–459. [Google Scholar] [CrossRef]
- Tytherleigh-Strong, G. Burkhart’s View of the Shoulder: A Cowboy’s Guide to Advanced Shoulder Arthroscopy; Burkhart, S.S., Lo, I.K.Y., Brady, P.C., Eds.; Lippincott, Williams & Wilkins: Philadelphia, PA, USA, 2006; p. 225. ISBN 0-7817-8000-4. [Google Scholar] [CrossRef]
- Tantillo, T.J.; Katsigiorgis, G. Arthrocentesis; StatPearls Publishing Copyright © 2024; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2024. [Google Scholar]
- Hamada, H.; Sugaya, H.; Takahashi, N.; Matsuki, K.; Tokai, M.; Ueda, Y.; Hoshika, S.; Kuniyoshi, K. Incidence of Axillary Nerve Injury After Arthroscopic Shoulder Stabilization. Arthroscopy 2020, 36, 1555–1564. [Google Scholar] [CrossRef]
- MacGillivray, J.D.; Fealy, S.; Potter, H.G.; O’Brien, S.J. Multiplanar analysis of acromion morphology. Am. J. Sports Med. 1998, 26, 836–840. [Google Scholar] [CrossRef]
- Vähäkari, M.; Leppilahti, J.; Hyvönen, P.; Ristiniemi, J.; Päivänsalo, M.; Jalovaara, P. Acromial shape in asymptomatic subjects: A study of 305 shoulders in different age groups. Acta Radiol. 2010, 51, 202–206. [Google Scholar] [CrossRef]
- Kadavkolan, A.S.; Lehmann, L.J.; Reichert, M.; Lattka, K.; Moursy, M. Does Acromion Morphology Depend on the Extremity or on Gender in the Population? J. Comput. Assist. Tomogr. 2017, 41, 121–124. [Google Scholar] [CrossRef]
- Farmer, K.W.; Wright, T.W. Shoulder arthroscopy: The basics. J. Hand Surg. Am. 2015, 40, 817–821. [Google Scholar] [CrossRef] [PubMed]
- Sibbitt, W.L., Jr.; Kettwich, L.G.; Band, P.A.; Chavez-Chiang, N.R.; DeLea, S.L.; Haseler, L.J.; Bankhurst, A.D. Does ultrasound guidance improve the outcomes of arthrocentesis and corticosteroid injection of the knee? Scand. J. Rheumatol. 2012, 41, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Wiler, J.L.; Costantino, T.G.; Filippone, L.; Satz, W. Comparison of ultrasound-guided and standard landmark techniques for knee arthrocentesis. J. Emerg. Med. 2010, 39, 76–82. [Google Scholar] [CrossRef] [PubMed]
- AWMF AK-Pd. S1-Leitlinie Intraartikuläre Punktionen und Injektionen: Hygienemaßnahmen: AWMF. 2015. [Langfassung der Leitlinie Intraartikuläre Punktionen und Injektionen: Hygienemaßnahmen]. Available online: https://register.awmf.org/de/leitlinien/detail/029-006 (accessed on 20 August 2015).
- Puebla, D.L.; Farrow, R.A. Ultrasound-Guided Arthrocentesis; StatPearls Publishing Copyright © 2023; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2023. [Google Scholar]
- Gruber, G.; Schamberger, C.; Konermann, W. Sonografie in Orthopädie, Unfallchirurgie und Rheumatologie: Aktuelle Standardschnittebenen der DEGUM; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar] [CrossRef]
- Bundesärztekammer. (Muster-) Logbuch, Dokumentation der Weiterbildung gemäß (Muster-)Weiterbildungsordnung (MWBO) über die Facharztweiterbildung Orthopädie und Unfallchirurgie. 2011. Available online: https://www.bundesaerztekammer.de/fileadmin/user_upload/_old-files/downloads/MLogbuch-7.5-FA_O_U.pdf (accessed on 20 August 2015).
- Alvarez, P.; Morro, M.R.; Ballesteros, J.R.; Llusa, M.; Cugat, R. Anatomy and Portals in Shoulder Arthroscopy. In Sports Injuries: Prevention, Diagnosis, Treatment and Rehabilitation; Doral, M.N., Karlsson, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2015; pp. 1–25. [Google Scholar] [CrossRef]
- Konermann, W.; Gruber, G. (Eds.) Ultraschalldiagnostik der Bewegungsorgane; Georg Thieme: Stuttgart, Germany, 2011; Volume 3. [Google Scholar]
- Konermann, W.; Gruber, G. Ultraschalldiagnostik der Bewegungsorgane: Kursbuch nach den Richtlinien der DEGUM und der DGOU; Georg Thieme: Stuttgart, Germany, 2011. [Google Scholar]
- O’Neill, P.J.; Cosgarea, A.J.; Freedman, J.A.; Queale, W.S.; McFarland, E.G. Arthroscopic proficiency: A survey of orthopaedic sports medicine fellowship directors and orthopaedic surgery department chairs. Arthroscopy 2002, 18, 795–800. [Google Scholar] [CrossRef] [PubMed]
- Sethi, P.M.; Kingston, S.; Elattrache, N. Accuracy of anterior intra-articular injection of the glenohumeral joint. Arthrosc. J. Arthrosc. Relat. Surg. 2005, 21, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Rijs, Z.; de Groot, P.C.J.; Zwitser, E.W.; Visser, C.P.J. Is the Anterior Injection Approach Without Ultrasound Guidance Superior to the Posterior Approach for Adhesive Capsulitis of the Shoulder? A Sequential, Prospective Trial. Clin. Orthop. Relat. Res. 2021, 479, 2483–2489. [Google Scholar] [CrossRef] [PubMed]
- Sethi, P.M.; El Attrache, N. Accuracy of intra-articular injection of the glenohumeral joint: A cadaveric study. Orthopedics 2006, 29, 149–152. [Google Scholar] [CrossRef]
- Hecker, A.; Jungwirth-Weinberger, A.; Bauer, M.R.; Tondelli, T.; Uçkay, I.; Wieser, K. The accuracy of joint aspiration for the diagnosis of shoulder infections. J. Shoulder Elbow Surg. 2020, 29, 516–520. [Google Scholar] [CrossRef]
- Challoumas, D.; Biddle, M.; McLean, M.; Millar, N.L. Comparison of Treatments for Frozen Shoulder: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e2029581. [Google Scholar] [CrossRef]
- Dwyer, T.; Hoit, G.; Lee, A.; Watkins, E.; Henry, P.; Leroux, T.; Veillette, C.; Theodoropoulos, J.; Ogilvie-Harris, D.; Chahal, J. Injection of Bone Marrow Aspirate for Glenohumeral Joint Osteoarthritis: A Pilot Randomized Control Trial. Arthrosc. Sports Med. Rehabil. 2021, 3, e1431–e1440. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.N.; Nayyar, S.; Hasan, S.; Khatib, O.; Sidash, S.; Jazrawi, L.M. Comparison of ultrasound-guided versus blind glenohumeral injections: A cadaveric study. J. Shoulder Elbow Surg. 2012, 21, 1664–1668. [Google Scholar] [CrossRef]
- Ćićak, N.; Matasović, T.; Bajraktarević, T. Ultrasonographic guidance of needle placement for shoulder arthrography. J. Ultrasound Med. 1992, 11, 135–137. [Google Scholar] [CrossRef] [PubMed]
- Crossan, K.; Rawson, D. Shoulder Arthrogram; StatPearls Publishing Copyright © 2022; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Souza, P.M.; Aguiar, R.O.; Marchiori, E.; Bardoe, S.A. Arthrography of the shoulder: A modified ultrasound guided technique of joint injection at the rotator interval. Eur. J. Radiol. 2010, 74, e29–e32. [Google Scholar] [CrossRef]
- Konermann, W.; Gruber, G. Standard ultrasound sections of the upper extremity--shoulder and elbow joint. Ultraschall Med. 1998, 19, 130–138. [Google Scholar] [CrossRef]
- Gupta, H.; Robinson, P. Normal shoulder ultrasound: Anatomy and technique. Semin. Musculoskelet. Radiol. 2015, 19, 203–211. [Google Scholar] [CrossRef]
- Intraartikuläre Punktionen und Injektionen. Hygienemaßnahmen HygMed 40-9:366 [Internet]. 2015. Available online: https://www.crd.york.ac.uk/PROSPERO/ (accessed on 30 August 2015).
- Berona, K.; Abdi, A.; Menchine, M.; Mailhot, T.; Kang, T.; Seif, D.; Chilstrom, M. Success of ultrasound-guided versus landmark-guided arthrocentesis of hip, ankle, and wrist in a cadaver model. Am. J. Emerg. Med. 2017, 35, 240–244. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stein, S.; Weimer, A.; Berthold, S.; Weimer, J.M.; Suda, A.J.; Tuffs, C.; Schmidmaier, G.; Schamberger, C.T. Comparison between Ultrasound-Guided and Palpatory Localization of the Dorsal Joint Space of the Shoulder Joint. Diagnostics 2024, 14, 650. https://doi.org/10.3390/diagnostics14060650
Stein S, Weimer A, Berthold S, Weimer JM, Suda AJ, Tuffs C, Schmidmaier G, Schamberger CT. Comparison between Ultrasound-Guided and Palpatory Localization of the Dorsal Joint Space of the Shoulder Joint. Diagnostics. 2024; 14(6):650. https://doi.org/10.3390/diagnostics14060650
Chicago/Turabian StyleStein, Stephan, Andreas Weimer, Svenja Berthold, Johannes Matthias Weimer, Arnold J. Suda, Christopher Tuffs, Gerhard Schmidmaier, and Christian T. Schamberger. 2024. "Comparison between Ultrasound-Guided and Palpatory Localization of the Dorsal Joint Space of the Shoulder Joint" Diagnostics 14, no. 6: 650. https://doi.org/10.3390/diagnostics14060650