
A Transfer Learning Approach for Clinical Detection Support of Monkeypox Skin Lesions

Abstract
:1. Introduction
1.1. Motivation and Contribution
- Improved accuracy of monkeypox detection: By using transfer learning, we have achieved the improved accuracy of monkeypox detection.
- Better understanding of the features that distinguish monkeypox: By analyzing the features and patterns learned by the deep learning model, we present insights into the characteristics that distinguish monkeypox from other diseases or healthy tissue. This can help to improve our understanding of the disease and inform future research.
- Improved disease surveillance: Monkeypox is a rare disease, and detecting it early is crucial for preventing its spread. By developing a more accurate and efficient method for detecting monkeypox using transfer learning, researchers have contributed to better disease surveillance and control.
1.2. Paper Organization
2. Related Work
2.1. Skin Lesion Detection and Diagnosis Using AI
2.2. Monkeypox Detection Using AI and Deep Learning Techniques
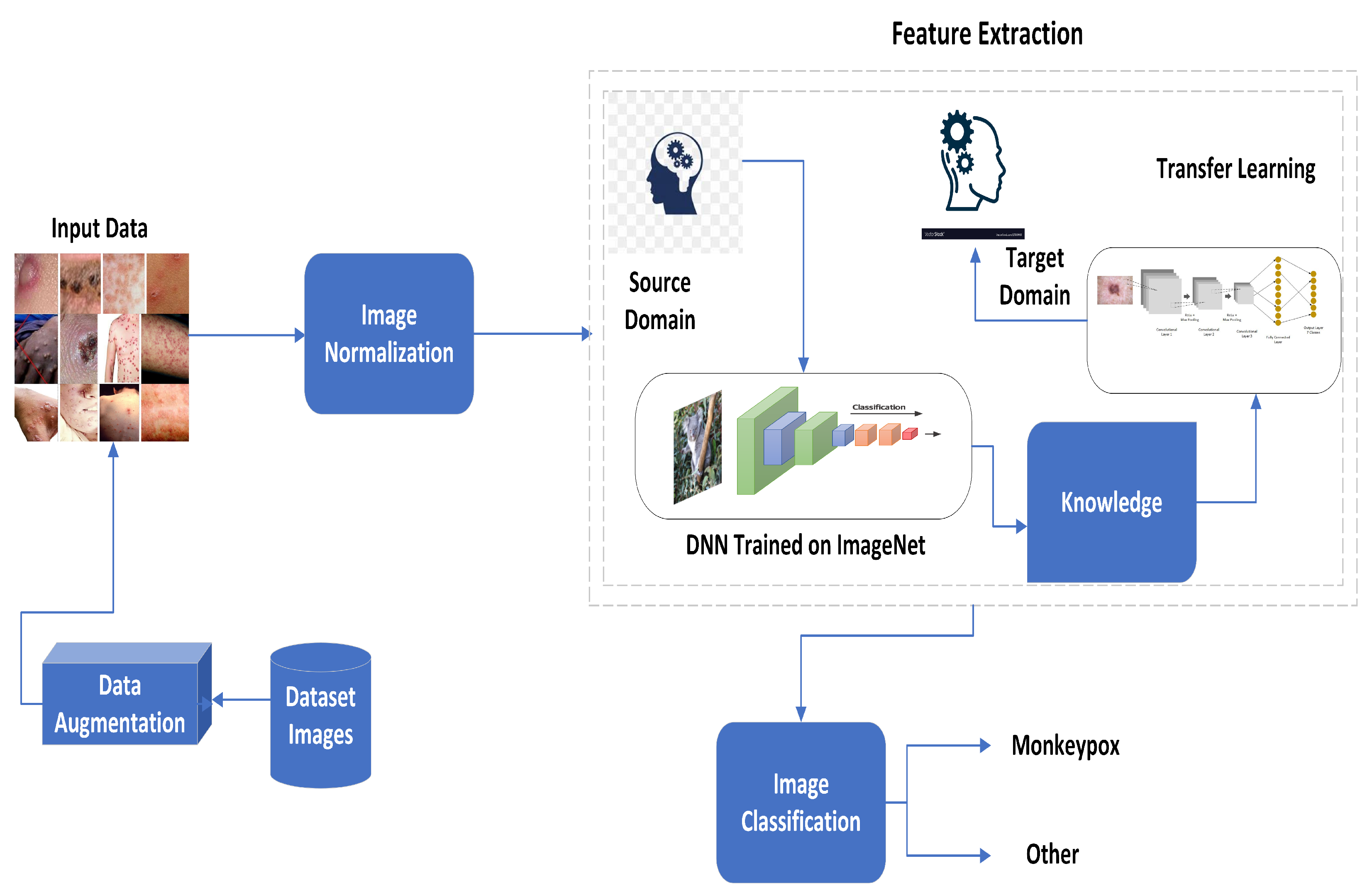
3. Proposed Methodology
3.1. Data Acquisition and Preparation
3.2. Preprocessing
3.3. Feature Extraction
3.4. Image Classification
| Algorithm 1: Algorithm for MonkeyPox Detection. |
 |
4. Results and Analysis
4.1. Experimental Setup
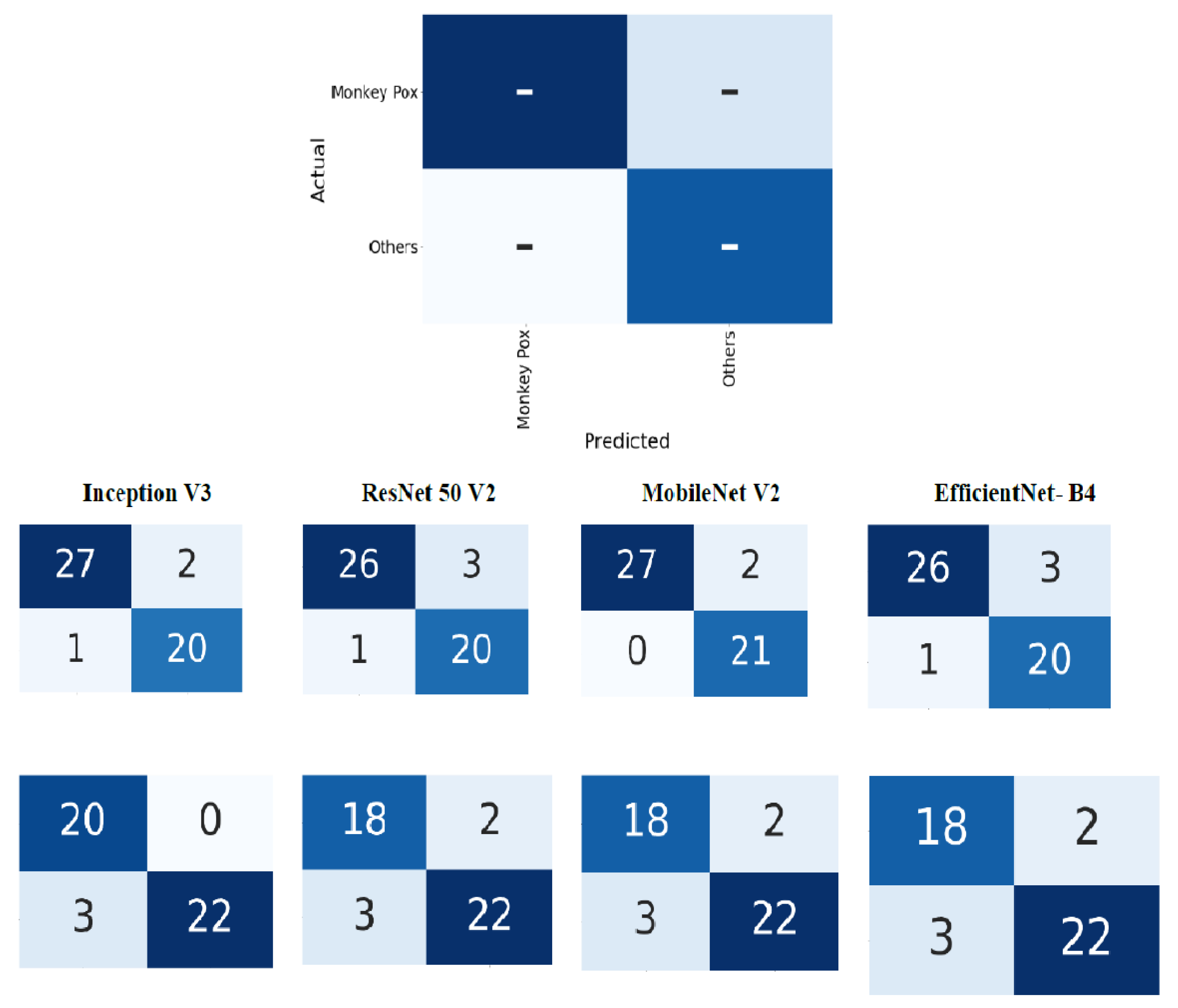
4.2. Evaluation Metrics
- True positives (TP): The target and predicted output are both monkeypox.
- True negatives (TN): The target and predicted output are both other.
- False positives (FP): The target is other and the predicted output is monkeypox.
- False negatives (FN): The target is monkeypox and the predicted output is other.
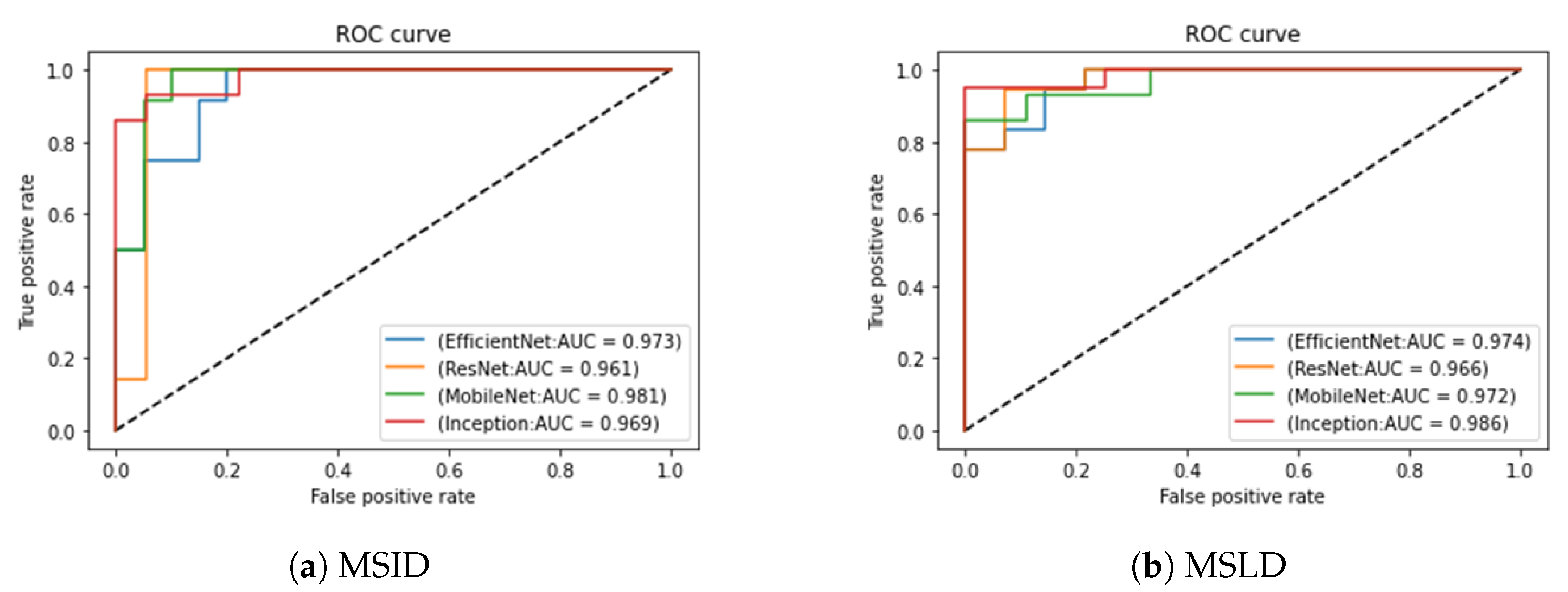
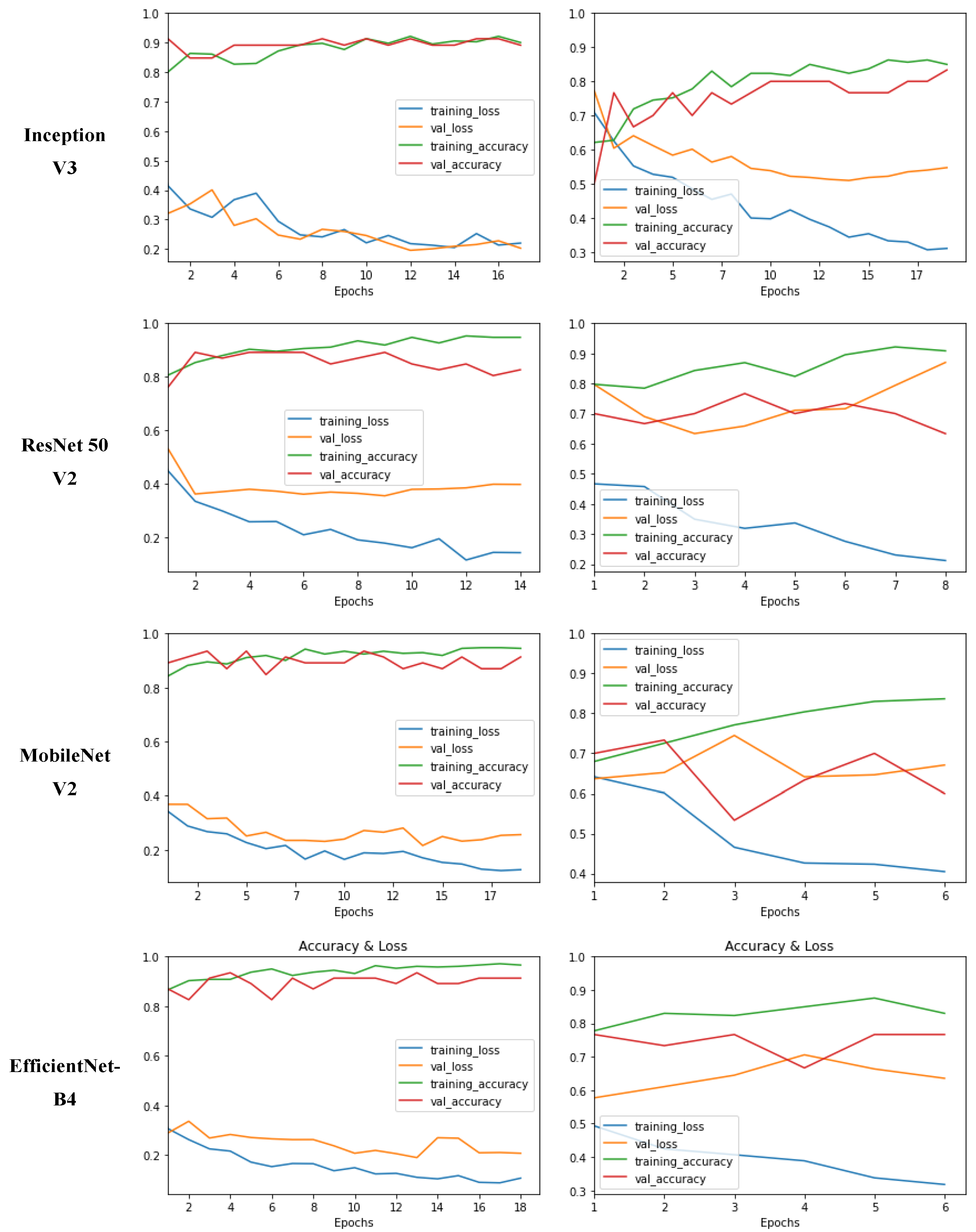
4.3. Experimental Results
5. Conclusions and Future Research Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kok, J.N.; Boers, E.J.; Kosters, W.A.; Van der Putten, P.; Poel, M. Artificial intelligence: Definition, trends, techniques, and cases. Artif. Intell. 2009, 1, 270–299. [Google Scholar]
- Ullah, A.; Azeem, M.; Ashraf, H.; Alaboudi, A.A.; Humayun, M.; Jhanjhi, N.Z. Secure healthcare data aggregation and transmission in IoT—A survey. IEEE Access 2021, 9, 16849–16865. [Google Scholar] [CrossRef]
- Khalil, M.I.; Tehsin, S.; Humayun, M.; Jhanjhi, N.; AlZain, M.A. Multi-Scale network for thoracic organs segmentation. Comput. Mater. Contin. 2022, 70, 3251–3265. [Google Scholar]
- Tehsin, S.; Zameer, S.; Saif, S. Myeloma cell detection in bone marrow aspiration using microscopic images. In Proceedings of the 2019 11th International Conference on Knowledge and Smart Technology (KST), Phuket, Thailand, 23–26 January 2019; pp. 57–61. [Google Scholar]
- Shah, R.; Chircu, A. IoT and AI in healthcare: A systematic literature review. Issues Inf. Syst. 2018, 19, 33–41. [Google Scholar]
- Alshehri, F.; Muhammad, G. A comprehensive survey of the Internet of Things (IoT) and AI-based smart healthcare. IEEE Access 2020, 9, 3660–3678. [Google Scholar] [CrossRef]
- Ladnyj, I.D.; Ziegler, P.; Kima, E. A human infection caused by Monkeypox virus in Basankusu Territory, Democratic Republic of the Congo. Bull. World Health Organ. 1972, 46, 593–597. [Google Scholar] [PubMed]
- Thornhill, J.P.; Barkati, S.; Walmsley, S.; Rockstroh, J.; Antinori, A.; Harrison, L.B.; Palich, R.; Nori, A.; Reeves, I.; Habibi, M.S.; et al. Monkeypox virus infection in humans across 16 countries—April–June 2022. N. Engl. J. Med. 2022, 387, 679–691. [Google Scholar] [CrossRef]
- Tarín-Vicente, E.J.; Alemany, A.; Agud-Dios, M.; Ubals, M.; Suñer, C.; Antón, A.; Arando, M.; Arroyo-Andrés, J.; Calderón-Lozano, L.; Casañ, C.; et al. Clinical presentation and virological assessment of confirmed human Monkeypox virus cases in Spain: A prospective observational cohort study. Lancet 2022, 400, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Alakunle, E.F.; Okeke, M.I. Monkeypox virus: A neglected zoonotic pathogen spreads globally. Nat. Rev. Microbiol. 2022, 20, 507–508. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. Monkeypox: What do we know about the outbreaks in Europe and North America? BMJ 2022, 377, o1274. [Google Scholar] [CrossRef]
- Alakunle, E.; Moens, U.; Nchinda, G.; Okeke, M.I. Monkeypox virus in Nigeria: Infection biology, epidemiology, and evolution. Viruses 2020, 12, 1257. [Google Scholar] [CrossRef] [PubMed]
- Shafaati, M.; Zandi, M. Monkeypox virus neurological manifestations in comparison to other orthopoxviruses. Travel Med. Infect. Dis. 2022, 49, 102414. [Google Scholar] [CrossRef] [PubMed]
- Sepehrinezhad, A.; Ashayeri Ahmadabad, R.; Sahab-Negah, S. Monkeypox virus from neurological complications to neuroinvasive properties: Current status and future perspectives. J. Neurol. 2022, 270, 101–108. [Google Scholar] [CrossRef]
- Bhattacharya, M.; Dhama, K.; Chakraborty, C. Recently spreading human Monkeypox virus infection and its transmission during COVID-19 pandemic period: A travelers’ prospective. Travel Med. Infect. Dis. 2022, 49, 102398. [Google Scholar] [CrossRef] [PubMed]
- WHO. Multi-Country Monkeypox Outbreak in Non-Endemic Countries; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Kumar, N.; Acharya, A.; Gendelman, H.E.; Byrareddy, S.N. The 2022 outbreak and the pathobiology of the Monkeypox virus. J. Autoimmun. 2022, 131, 102855. [Google Scholar] [CrossRef]
- Altindis, M.; Puca, E.; Shapo, L. Diagnosis of Monkeypox virus–An overview. Travel Med. Infect. Dis. 2022, 50, 102459. [Google Scholar] [CrossRef]
- Ali, S.N.; Ahmed, M.; Paul, J.; Jahan, T.; Sani, S.M.; Noor, N.; Hasan, T. Monkeypox skin lesion detection using deep learning models: A feasibility study. arXiv 2022, arXiv:2207.03342. [Google Scholar]
- Unnikrishnan, M.; Gontu, H.L.; Khwairakpam, B.S.; Sagar, P. Detection of covid from chest x-rays using gan. EPRA Int. J. Res. Dev. (IJRD) 2022, 7, 166–175. [Google Scholar] [CrossRef]
- Fraiwan, M.; Faouri, E. On the Automatic Detection and Classification of Skin Cancer Using Deep Transfer Learning. Sensors 2022, 22, 4963. [Google Scholar] [CrossRef]
- Alwakid, G.; Gouda, W.; Humayun, M.; Sama, N.U. Melanoma Detection Using Deep Learning-Based Classifications. Healthcare 2022, 10, 2481. [Google Scholar] [CrossRef]
- Banasode, P.; Patil, M.; Ammanagi, N. A Melanoma Skin Cancer Detection Using Machine Learning Technique: Support Vector Machine. IOP Conf. Ser.: Mater. Sci. Eng. 2021, 1065, 012039. [Google Scholar] [CrossRef]
- Yadav, N.; Alfayeed, S.M.; Khamparia, A.; Pandey, B.; Thanh, D.N.; Pande, S. Hsv model-based segmentation driven facial acne detection using deep learning. Expert Syst. 2022, 39, e12760. [Google Scholar] [CrossRef]
- Sandeep, R.; Vishal, K.; Shamanth, M.; Chethan, K. Diagnosis of visible diseases using cnns. In Proceedings of International Conference on Communication and Artificial Intelligence; Springer: Berlin, Germany, 2022; pp. 459–468. [Google Scholar]
- Glock, K.; Napier, C.; Gary, T.; Gupta, V.; Gigante, J.; Schaffner, W.; Wang, Q. Measles rash identification using transfer learning and deep convolutional neural networks. In Proceedings of the IEEE International Conference on Big Data (Big Data), Online, 15–18 December 2021; pp. 3905–3910. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the IEEE CVPR, Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- Sitaula, C.; Shahi, T.B. Monkeypox virus detection using pretrained deep learning-based approaches. arXiv 2022, arXiv:2209.04444. [Google Scholar]
- Ahsan, M.M.; Uddin, M.R.; Farjana, M.; Sakib, A.N.; Momin, K.A.; Luna, S.A. Image Data collection and implementation of deep learning-based model in detecting Monkeypox disease using modified VGG16. arXiv 2022, arXiv:2206.01862. [Google Scholar]
- Ariansyah, M.H.; Winarno, S.; Sani, R.R. Monkeypox and Measles Detection using CNN with VGG-16 Transfer Learning. J. Comput. Res. Innov. 2023, 8, 32–44. [Google Scholar] [CrossRef]
- Bala, D. Monkeypox Skin Images Dataset (MSID) [Data Set]. 2022. Kaggle. Available online: https://www.kaggle.com/datasets/dipuiucse/monkeypoxskinimagedataset (accessed on 25 October 2022).
- Saha, S.; Chakraborty, T.; Sulaiman, R.B.; Paul, T. A Comparative Analysis of CNN-Based Pretrained Models for the Detection and Prediction of Monkeypox. arXiv 2023, arXiv:2302.10277. [Google Scholar]
- Haque, M.; Ahmed, M.; Nila, R.S.; Islam, S. Classification of human Monkeypox disease using deep learning models and attention mechanisms. arXiv 2022, arXiv:2211.15459. [Google Scholar]
- Sahin, H.; Oztel, I.; Yolcu Oztel, G. Human Monkeypox Classification from Skin Lesion Images with Deep Pre-trained Network using Mobile Application. J. Med. Syst. 2022, 46, 79. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Methodology | Disease | Dataset | Results |
|---|---|---|---|
| Alwakid et al. [22] | Melanoma | HAM10000 | Accuracy: 0.86 Precision: 0.84 Recall: 0.86 F-score: 0.86 |
| Banasode et al. [23] | Melanoma | ISIC | Accuracy: 0.9690 Sensitivity: 0.9570 Specificity: 0.9020 |
| Yadav et al. [24] | acne | Custom Dataset | Precision: 0.88 Recall: 0.88 F-1 score: 0.88 |
| Sandeep et al. [25] | Chicken Pox, Vitiligo, | Custom Dataset | Accuracy: 0.78 Psoriasis, Acne, Melanoma, Lupus, Ringworm and Herpes |
| Glock et al. [26] | Measles | Rash Image Dataset | Sensitivity: 0.817 Specificity: 0.97 Accuracy: 0.95 |
| Nafisa et al. [19] | monkeypox | MSLD | Accuracy: 0.79 Precision: 84.00 Recall: 79.00 F1-score: 81.00 |
| Sitaula et al. [30] | Chickenpox, Measles and Monkeypox | Ahsan et al. [31] | Precision: 0.8544 Recall: 0.8547 F1-score: 0.8540 Accuracy: 0.8713 |
| Ariansyah et al. [32] | Measles and Monkeypox | Bala et al. [33] | Accuracy: 0.8333 Precision: 0.84 Recall: 0.8333 |
| Saha et al. [34] | Monkeypox | Ahsan et al. [31] | Accuracy: 0.80 |
| Haque. et al. [35] | Monkeypox | MSLD | Accuracy: 0.83 Precision: 0.90 Recall: 0.89 F1-score: 0.90 |
| Sahin et al. [36] | Monkeypox | MSLD | Accuracy: 91.11 Precision: 0.90 Recall: 0.90 F1-score: 0.90 |
| Dataset Name | Monkeypox | Others |
|---|---|---|
| MSLD | 102 | 126 |
| MSID | 279 | 198 |
| S# | Technique | Accuracy | Loss | Specificity | Sensitivity | Balanced Accuracy |
|---|---|---|---|---|---|---|
| 1 | Inception V3 | 0.94 | 0.234 | 0.931034 | 0.952381 | 0.941708 |
| 2 | ResNet 50 V2 | 0.92 | 0.2307 | 0.896552 | 0.952381 | 0.924466 |
| 3 | MobileNet V2 | 0.96 | 0.1604 | 0.931034 | 1 | 0.965517 |
| 4 | EfficientNet- B4 | 0.92 | 0.2266 | 0.896552 | 0.952381 | 0.924466 |
| S# | Technique | Accuracy | Loss | Specificity | Sensitivity | Balanced Accuracy |
|---|---|---|---|---|---|---|
| 1 | Inception V3 | 0.9333 | 0.246 | 1 | 0.88 | 0.94 |
| 2 | ResNet 50 V2 | 0.8889 | 0.272 | 0.9 | 0.88 | 0.89 |
| 3 | MobileNet V2 | 0.8889 | 0.311 | 0.9 | 0.88 | 0.89 |
| 4 | EfficientNet- B4 | 0.8889 | 0.277 | 0.9 | 0.88 | 0.89 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almufareh, M.F.; Tehsin, S.; Humayun, M.; Kausar, S. A Transfer Learning Approach for Clinical Detection Support of Monkeypox Skin Lesions. Diagnostics 2023, 13, 1503. https://doi.org/10.3390/diagnostics13081503
Almufareh MF, Tehsin S, Humayun M, Kausar S. A Transfer Learning Approach for Clinical Detection Support of Monkeypox Skin Lesions. Diagnostics. 2023; 13(8):1503. https://doi.org/10.3390/diagnostics13081503
Chicago/Turabian StyleAlmufareh, Maram Fahaad, Samabia Tehsin, Mamoona Humayun, and Sumaira Kausar. 2023. "A Transfer Learning Approach for Clinical Detection Support of Monkeypox Skin Lesions" Diagnostics 13, no. 8: 1503. https://doi.org/10.3390/diagnostics13081503