
Myocardial Recovery
 , , , and
, , , and
Abstract
:1. Introduction
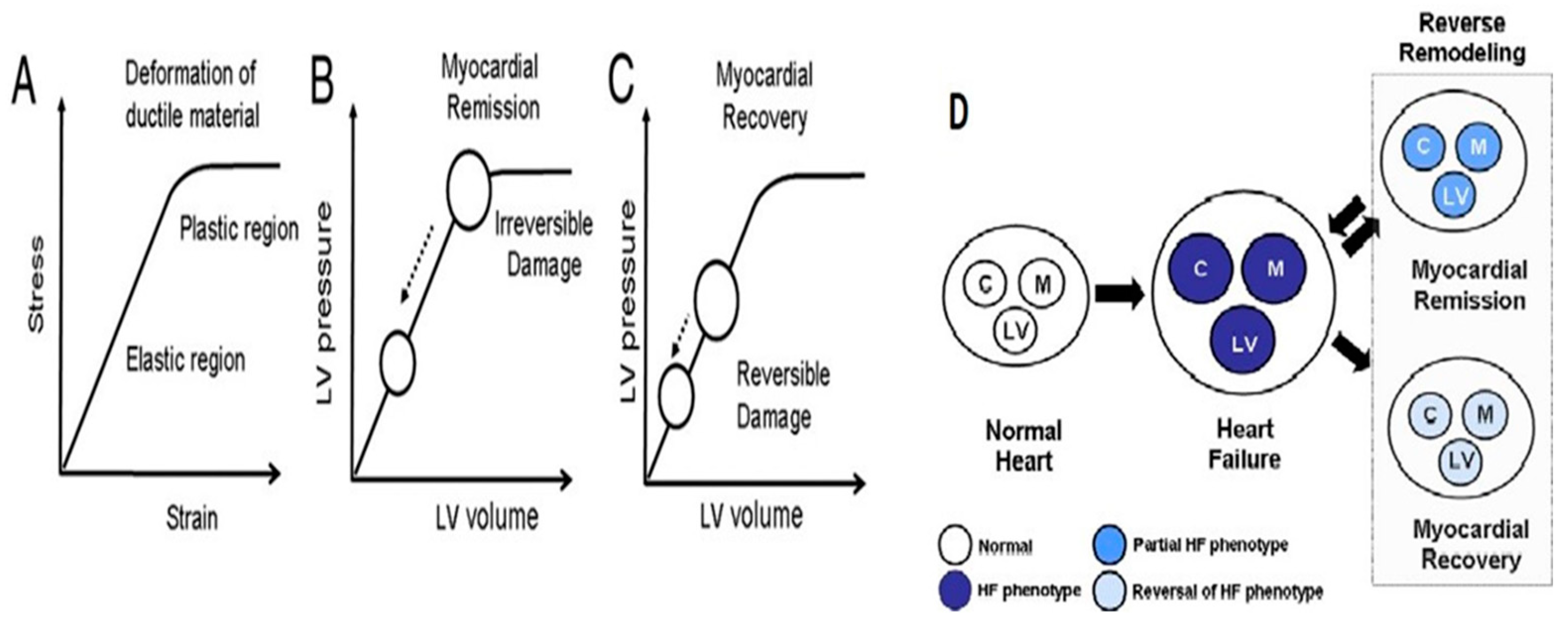
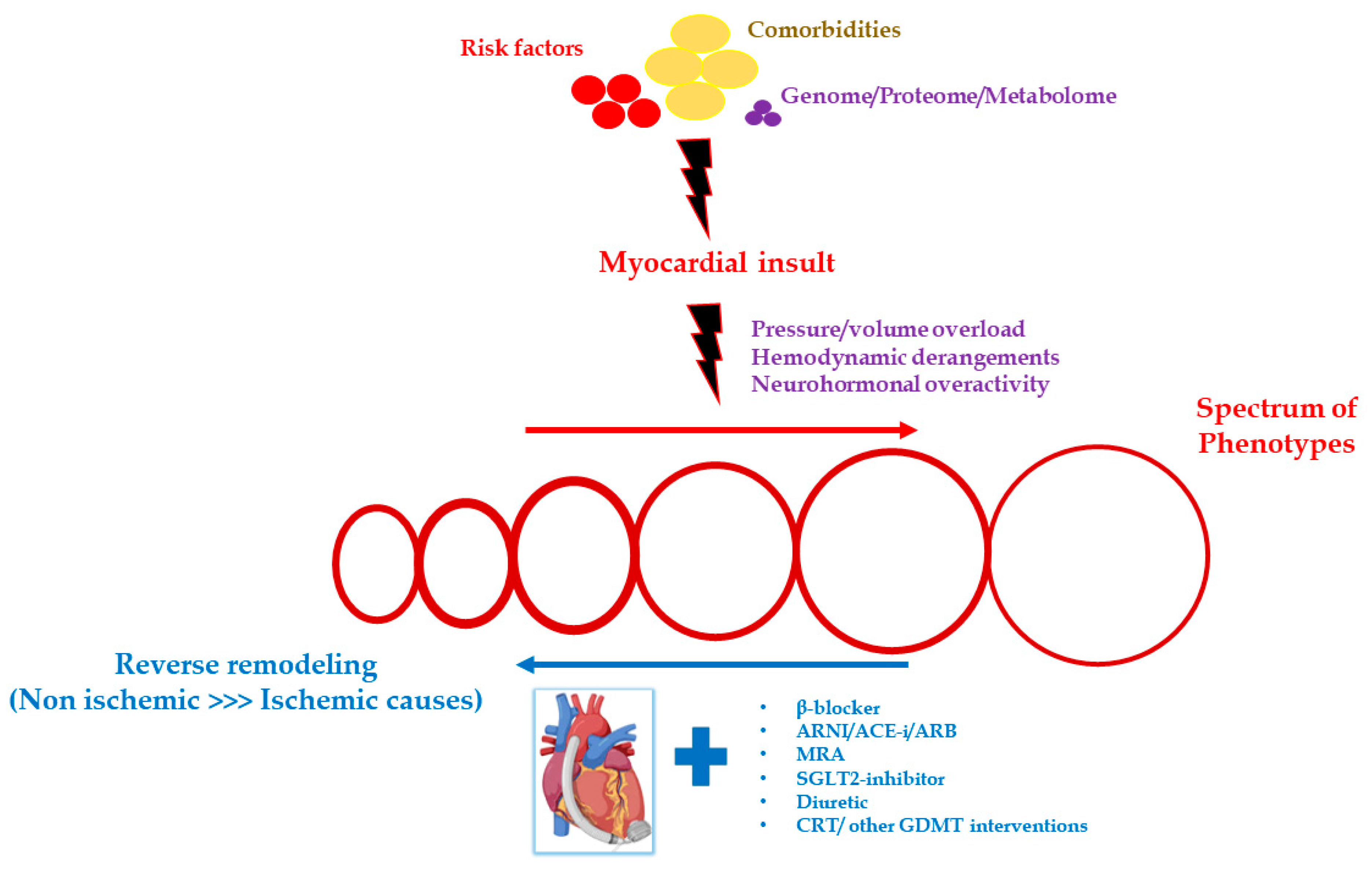
2. Pathophysiology
3. Biomarkers
3.1. Biochemists
3.1.1. Natriuretic Peptides (Brain Natriuretic Peptide (BNP), N-Terminal Pro–B-Type Natriuretic Peptide (NT-proBNP))
3.1.2. Troponin
3.1.3. Soluble ST2 (sST2)
3.1.4. Interleukin-8 (IL-8)
3.2. Electrocardiogram
3.3. Visual Techniques
3.4. Molecular Techniques
3.4.1. MicroRNAs
- miR 23a, 195, 21, 24, 125b, 195, 199a: associated with myocardial recovery after LVAD support patients;
- miR-26b-5p, miR-145-5p, miR-92a-3p, miR-30e-5p and miR29a-3p: found elevated in cardiac resynchronization therapy (CRT) patients who responded to treatment;
- miR-30d: increased in responders to CRT placement (strong association) and also associated with an improvement in LVEF [14].
3.4.2. Other Indicators
- IGF-I mRNA: from studies, it was observed to be increased in patients who received a left ventricular assist device (LVAD) with the drug protocol of Harefield and who showed myocardial recovery [15];
- Fas and TNFR1: these two molecules were studied in the Intervention in Myocarditis and Acute Cardiomyopathy (IMAC) study and their increased values were negatively related to the improvement of myocardial function in recent-onset cardiomyopathies, possibly reflecting an increased apoptotic process [16].
4. LVAD Therapy
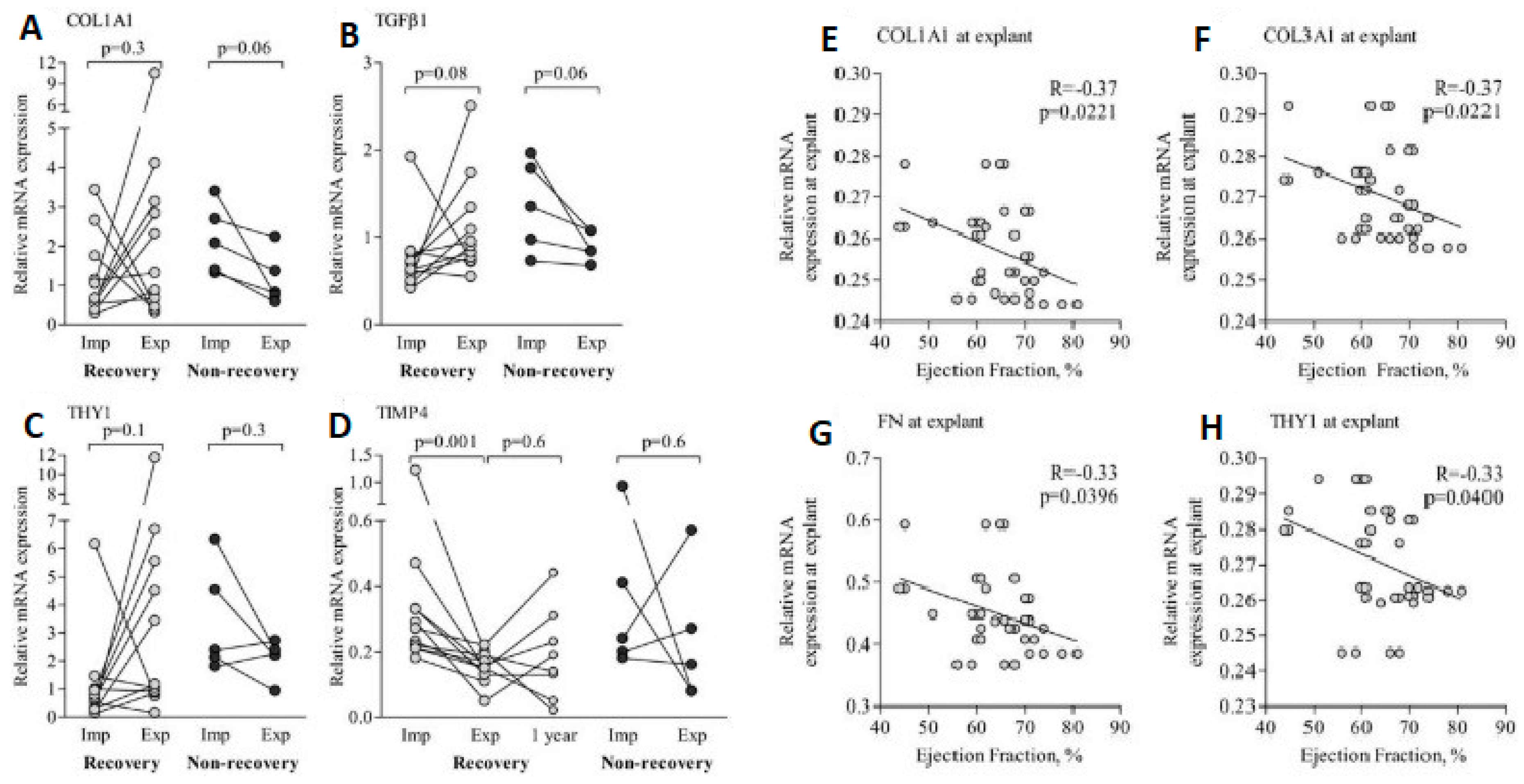
4.1. Extracellular Matrix
4.2. Protein Changes
4.3. Apoptosis
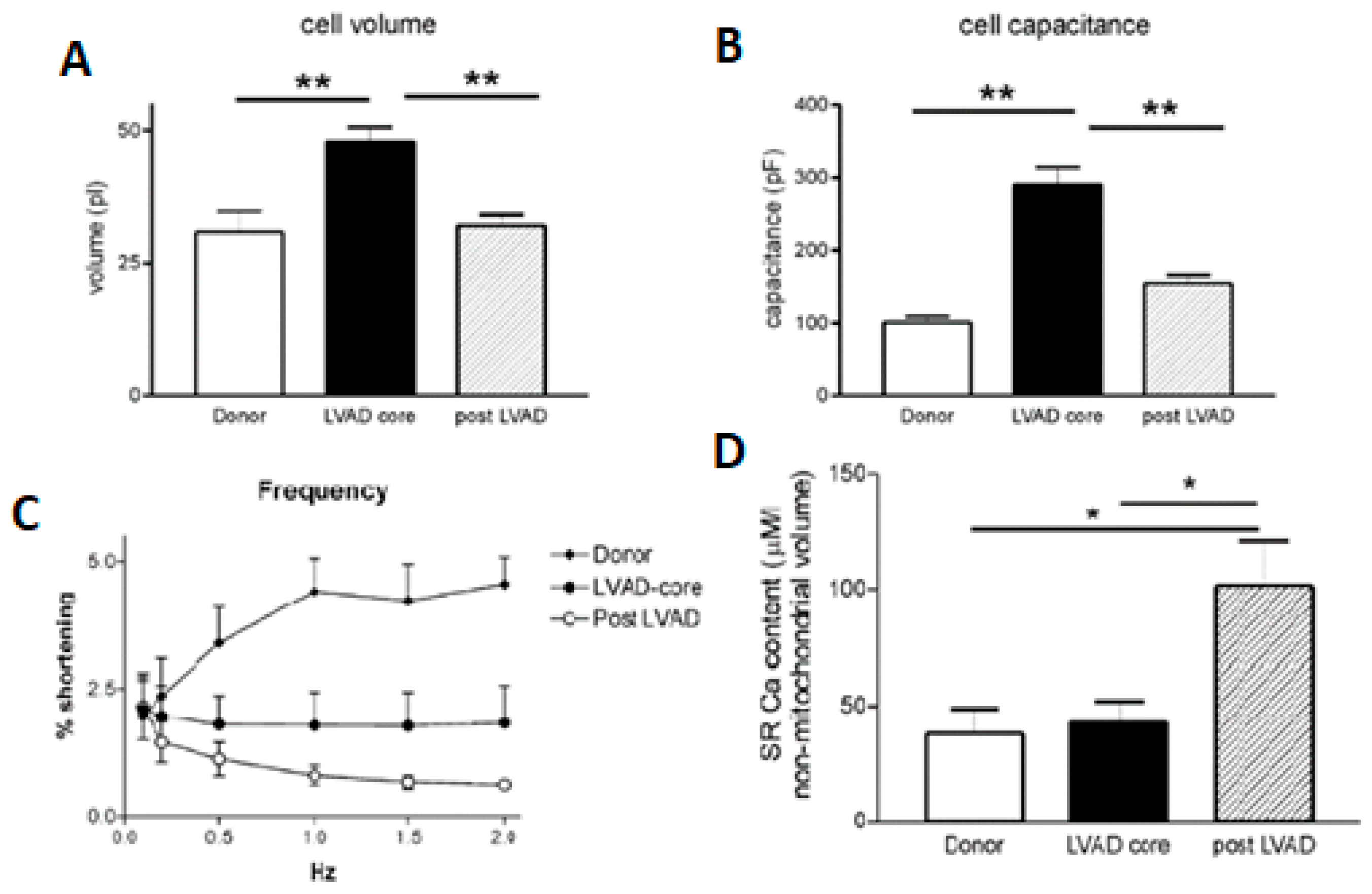
4.4. Sarcoplasmic Reticulum
4.5. B-Receptors
4.6. Energy
4.7. Genome
5. Side Effects
6. Weaning from LVAD Studies—Patient Selection
7. Treatment of Arrhythmias and Use of CRT
8. Medical Treatment and Cardiac Rehabilitation
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mann, D.L.; Barger, P.M.; Burkhoff, D. Myocardial recovery and the failing heart: Myth, magic, or molecular target? J. Am. Coll. Cardiol. 2012, 60, 2465–2472. [Google Scholar] [CrossRef]
- Marinescu, K.K.; Uriel, N.; Mann, D.L.; Burkhoff, D. Left ventricular assist device-induced reverse remodeling: It’s not just about myocardial recovery. Expert Rev. Med. Devices 2017, 14, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Motiwala, S.R.; Gaggin, H.K. Biomarkers to Predict Reverse Remodeling and Myocardial Recovery in Heart Failure. Curr. Heart Fail. Rep. 2016, 13, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Hoevelmann, J.; Muller, E.; Azibani, F.; Kraus, S.; Cirota, J.; Briton, O.; Ntsekhe, M.; Ntusi, N.A.B.; Sliwa, K.; Viljoen, C.A. Prognostic value of NT-proBNP for myocardial recovery in peripartum cardiomyopathy (PPCM). Clin. Res. Cardiol. 2021, 110, 1259–1269. [Google Scholar] [CrossRef]
- Broch, K.; Eek, C.; Wergeland, R.; Ueland, T.; Skardal, R.; Aukrust, P.; Skulstad, H.; Gullestad, L. NT-proBNP predicts myocardial recovery after non-ST-elevation acute coronary syndrome. Scand. Cardiovasc. J. 2012, 46, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Somuncu, M.U.; Tatar, F.P.; Kalayci, B.; Avci, A.; Gudul, N.E.; Serbest, N.G.; Demir, A.R.; Can, M. Role of N-terminal pro-B-type natriuretic peptide and troponin T in predicting right ventricular recovery in myocardial infarction. Horm. Mol. Biol. Clin. Investig. 2021, 43, 27–33. [Google Scholar] [CrossRef]
- Motiwala, S.R.; Gaggin, H.K.; Gandhi, P.U.; Belcher, A.; Weiner, R.B.; Baggish, A.L.; Szymonifka, J.; Januzzi, J.L., Jr. Concentrations of highly sensitive cardiac troponin-I predict poor cardiovascular outcomes and adverse remodeling in chronic heart failure. J. Cardiovasc. Transl. Res. 2015, 8, 164–172. [Google Scholar] [CrossRef]
- Husebye, T.; Eritsland, J.; Arnesen, H.; Bjornerheim, R.; Mangschau, A.; Seljeflot, I.; Andersen, G.O. Association of interleukin 8 and myocardial recovery in patients with ST-elevation myocardial infarction complicated by acute heart failure. PLoS ONE 2014, 9, e112359. [Google Scholar] [CrossRef]
- Lee, S.G.; Cheong, J.P.; Shin, J.K.; Kim, J.W.; Park, J.H. Persistent ST-segment elevation after primary stenting for acute myocardial infarction: Its relation to left ventricular recovery. Clin. Cardiol. 2002, 25, 372–377. [Google Scholar] [CrossRef]
- Prenner, S.B.; Swat, S.A.; Ng, J.; Baldridge, A.; Wilcox, J.E. Parameters of repolarization heterogeneity are associated with myocardial recovery in acute heart failure. Int. J. Cardiol. 2020, 301, 147–151. [Google Scholar] [CrossRef]
- Beleslin, B.; Ostojic, M.; Djordjevic-Dikic, A.; Vukcevic, V.; Stojkovic, S.; Nedeljkovic, M.; Stankovic, G.; Orlic, D.; Milic, N.; Stepanovic, J.; et al. The value of fractional and coronary flow reserve in predicting myocardial recovery in patients with previous myocardial infarction. Eur. Heart J. 2008, 29, 2617–2624. [Google Scholar] [CrossRef] [PubMed]
- Meimoun, P.; Malaquin, D.; Benali, T.; Boulanger, J.; Zemir, H.; Sayah, S.; Luycx-Bore, A.; Doutrelan, L.; Tribouilloy, C. Non-invasive coronary flow reserve after successful primary angioplasty for acute anterior myocardial infarction is an independent predictor of left ventricular recovery and in-hospital cardiac events. J. Am. Soc. Echocardiogr. 2009, 22, 1071–1079. [Google Scholar] [CrossRef] [PubMed]
- Palmer, S.; Layland, J.; Carrick, D.; Williams, P.D.; Judkins, C.; Gong, F.F.; Burns, A.T.; Whitbourn, R.J.; MacIsaac, A.I.; Wilson, A.M. The Index of Microcirculatory Resistance Postpercutaneous Coronary Intervention Predicts Left Ventricular Recovery in Patients With Thrombolyzed ST-Segment Elevation Myocardial Infarction. J. Interv. Cardiol. 2016, 29, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.; Bristow, M.R.; Port, J.D. MicroRNAs in Heart Failure, Cardiac Transplantation, and Myocardial Recovery: Biomarkers with Therapeutic Potential. Curr. Heart Fail. Rep. 2017, 14, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Barton, P.J.; Felkin, L.E.; Birks, E.J.; Cullen, M.E.; Banner, N.R.; Grindle, S.; Hall, J.L.; Miller, L.W.; Yacoub, M.H. Myocardial insulin-like growth factor-I gene expression during recovery from heart failure after combined left ventricular assist device and clenbuterol therapy. Circulation 2005, 112, I46–I50. [Google Scholar] [CrossRef]
- Sheppard, R.; Bedi, M.; Kubota, T.; Semigran, M.J.; Dec, W.; Holubkov, R.; Feldman, A.M.; Rosenblum, W.D.; McTiernan, C.F.; McNamara, D.M.; et al. Myocardial expression of fas and recovery of left ventricular function in patients with recent-onset cardiomyopathy. J. Am. Coll. Cardiol. 2005, 46, 1036–1042. [Google Scholar] [CrossRef]
- Butler, C.R.; Jugdutt, B.I. The paradox of left ventricular assist device unloading and myocardial recovery in end-stage dilated cardiomyopathy: Implications for heart failure in the elderly. Heart Fail. Rev. 2012, 17, 615–633. [Google Scholar] [CrossRef]
- Hunt, S.A. Comment--the REMATCH trial: Long-term use of a left ventricular assist device for end-stage heart failure. J. Card. Fail. 2002, 8, 59–60. [Google Scholar] [CrossRef]
- Felkin, L.E.; Lara-Pezzi, E.; George, R.; Yacoub, M.H.; Birks, E.J.; Barton, P.J. Expression of extracellular matrix genes during myocardial recovery from heart failure after left ventricular assist device support. J. Heart Lung Transplant. 2009, 28, 117–122. [Google Scholar] [CrossRef]
- Mahr, C.; Gundry, R.L. Hold or fold--proteins in advanced heart failure and myocardial recovery. Proteom. Clin. Appl. 2015, 9, 121–133. [Google Scholar] [CrossRef]
- Bruckner, B.A.; Stetson, S.J.; Farmer, J.A.; Radovancevic, B.; Frazier, O.H.; Noon, G.P.; Entman, M.L.; Torre-Amione, G.; Youker, K.A. The implications for cardiac recovery of left ventricular assist device support on myocardial collagen content. Am. J. Surg. 2000, 180, 498–502. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Narula, J. Molecular biology of myocardial recovery. Surg. Clin. N. Am. 2004, 84, 223–242. [Google Scholar] [CrossRef] [PubMed]
- Dandel, M.; Hetzer, R. Myocardial recovery during mechanical circulatory support: Long-term outcome and elective ventricular assist device implantation to promote recovery as a treatment goal. Heart Lung Vessel. 2015, 7, 289–296. [Google Scholar] [PubMed]
- Latif, N.; Yacoub, M.H.; George, R.; Barton, P.J.; Birks, E.J. Changes in sarcomeric and non-sarcomeric cytoskeletal proteins and focal adhesion molecules during clinical myocardial recovery after left ventricular assist device support. J. Heart Lung Transplant. 2007, 26, 230–235. [Google Scholar] [CrossRef]
- Birks, E.J.; Hall, J.L.; Barton, P.J.; Grindle, S.; Latif, N.; Hardy, J.P.; Rider, J.E.; Banner, N.R.; Khaghani, A.; Miller, L.W.; et al. Gene profiling changes in cytoskeletal proteins during clinical recovery after left ventricular-assist device support. Circulation 2005, 112, I57–I64. [Google Scholar] [CrossRef] [PubMed]
- Rame, J.E.; Lavandero, S. Subcellular Remodeling of the T-Tubule Membrane System: The Limits of Myocardial Recovery Revealed? Circulation 2017, 135, 1646–1650. [Google Scholar] [CrossRef] [PubMed]
- Terracciano, C.M.; Harding, S.E.; Adamson, D.; Koban, M.; Tansley, P.; Birks, E.J.; Barton, P.J.; Yacoub, M.H. Changes in sarcolemmal Ca entry and sarcoplasmic reticulum Ca content in ventricular myocytes from patients with end-stage heart failure following myocardial recovery after combined pharmacological and ventricular assist device therapy. Eur. Heart J. 2003, 24, 1329–1339. [Google Scholar] [CrossRef]
- Madamanchi, A. Beta-adrenergic receptor signaling in cardiac function and heart failure. McGill J. Med. 2007, 10, 99–104. [Google Scholar]
- Pandalai, P.K.; Bulcao, C.F.; Merrill, W.H.; Akhter, S.A. Restoration of myocardial beta-adrenergic receptor signaling after left ventricular assist device support. J. Thorac. Cardiovasc. Surg. 2006, 131, 975–980. [Google Scholar] [CrossRef]
- Akhter, S.A.; D’Souza, K.M.; Malhotra, R.; Staron, M.L.; Valeroso, T.B.; Fedson, S.E.; Anderson, A.S.; Raman, J.; Jeevanandam, V. Reversal of impaired myocardial beta-adrenergic receptor signaling by continuous-flow left ventricular assist device support. J. Heart Lung Transplant. 2010, 29, 603–609. [Google Scholar] [CrossRef]
- Gupte, A.A.; Hamilton, D.J.; Cordero-Reyes, A.M.; Youker, K.A.; Yin, Z.; Estep, J.D.; Stevens, R.D.; Wenner, B.; Ilkayeva, O.; Loebe, M.; et al. Mechanical unloading promotes myocardial energy recovery in human heart failure. Circ. Cardiovasc. Genet. 2014, 7, 266–276. [Google Scholar] [CrossRef] [PubMed]
- Badolia, R.; Ramadurai, D.K.A.; Abel, E.D.; Ferrin, P.; Taleb, I.; Shankar, T.S.; Krokidi, A.T.; Navankasattusas, S.; McKellar, S.H.; Yin, M.; et al. The Role of Nonglycolytic Glucose Metabolism in Myocardial Recovery Upon Mechanical Unloading and Circulatory Support in Chronic Heart Failure. Circulation 2020, 142, 259–274. [Google Scholar] [CrossRef]
- Wohlschlaeger, J.; Levkau, B.; Brockhoff, G.; Schmitz, K.J.; von Winterfeld, M.; Takeda, A.; Takeda, N.; Stypmann, J.; Vahlhaus, C.; Schmid, C.; et al. Hemodynamic support by left ventricular assist devices reduces cardiomyocyte DNA content in the failing human heart. Circulation 2010, 121, 989–996. [Google Scholar] [CrossRef]
- Castillero, E.; Ali, Z.A.; Akashi, H.; Giangreco, N.; Wang, C.; Stohr, E.J.; Ji, R.; Zhang, X.; Kheysin, N.; Park, J.S.; et al. Structural and functional cardiac profile after prolonged duration of mechanical unloading: Potential implications for myocardial recovery. Am. J. Physiol. Heart Circ. Physiol. 2018, 315, H1463–H1476. [Google Scholar] [CrossRef] [PubMed]
- Diakos, N.A.; Selzman, C.H.; Sachse, F.B.; Stehlik, J.; Kfoury, A.G.; Wever-Pinzon, O.; Catino, A.; Alharethi, R.; Reid, B.B.; Miller, D.V.; et al. Myocardial atrophy and chronic mechanical unloading of the failing human heart: Implications for cardiac assist device-induced myocardial recovery. J. Am. Coll. Cardiol. 2014, 64, 1602–1612. [Google Scholar] [CrossRef] [PubMed]
- Farrar, D.J.; Holman, W.R.; McBride, L.R.; Kormos, R.L.; Icenogle, T.B.; Hendry, P.J.; Moore, C.H.; Loisance, D.Y.; El-Banayosy, A.; Frazier, H. Long-term follow-up of Thoratec ventricular assist device bridge-to-recovery patients successfully removed from support after recovery of ventricular function. J. Heart Lung Transplant. 2002, 21, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Dandel, M.; Weng, Y.; Siniawski, H.; Potapov, E.; Lehmkuhl, H.B.; Hetzer, R. Long-term results in patients with idiopathic dilated cardiomyopathy after weaning from left ventricular assist devices. Circulation 2005, 112, I37–I45. [Google Scholar] [CrossRef]
- Birks, E.J. Myocardial recovery in patients with chronic heart failure: Is it real? J. Card. Surg. 2010, 25, 472–477. [Google Scholar] [CrossRef]
- Simon, M.A.; Kormos, R.L.; Murali, S.; Nair, P.; Heffernan, M.; Gorcsan, J.; Winowich, S.; McNamara, D.M. Myocardial recovery using ventricular assist devices: Prevalence, clinical characteristics, and outcomes. Circulation 2005, 112, I32–I36. [Google Scholar] [CrossRef]
- Boehmer, J.P.; Starling, R.C.; Cooper, L.T.; Torre-Amione, G.; Wittstein, I.; Dec, G.W.; Markham, D.W.; Zucker, M.J.; Gorcsan, J., 3rd; McTiernan, C.; et al. Left ventricular assist device support and myocardial recovery in recent onset cardiomyopathy. J. Card. Fail. 2012, 18, 755–761. [Google Scholar] [CrossRef]
- Pan, S.; Aksut, B.; Wever-Pinzon, O.E.; Rao, S.D.; Levin, A.P.; Garan, A.R.; Fried, J.A.; Takeda, K.; Hiroo, T.; Yuzefpolskaya, M.; et al. Incidence and predictors of myocardial recovery on long-term left ventricular assist device support: Results from the United Network for Organ Sharing database. J. Heart Lung Transplant. 2015, 34, 1624–1629. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.R.; Saeed, O.; Murthy, S.; Bhatia, V.; Shin, J.J.; Wang, D.; Negassa, A.; Pullman, J.; Goldstein, D.J.; Maybaum, S. Combining neurohormonal blockade with continuous-flow left ventricular assist device support for myocardial recovery: A single-arm prospective study. J. Heart Lung Transplant. 2013, 32, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Birks, E.J.; George, R.S.; Hedger, M.; Bahrami, T.; Wilton, P.; Bowles, C.T.; Webb, C.; Bougard, R.; Amrani, M.; Yacoub, M.H.; et al. Reversal of severe heart failure with a continuous-flow left ventricular assist device and pharmacological therapy: A prospective study. Circulation 2011, 123, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Topkara, V.K.; Garan, A.R.; Fine, B.; Godier-Furnemont, A.F.; Breskin, A.; Cagliostro, B.; Yuzefpolskaya, M.; Takeda, K.; Takayama, H.; Mancini, D.M.; et al. Myocardial Recovery in Patients Receiving Contemporary Left Ventricular Assist Devices: Results From the Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS). Circ. Heart Fail. 2016, 9, e003157. [Google Scholar] [CrossRef] [PubMed]
- Wever-Pinzon, J.; Selzman, C.H.; Stoddard, G.; Wever-Pinzon, O.; Catino, A.; Kfoury, A.G.; Diakos, N.A.; Reid, B.B.; McKellar, S.; Bonios, M.; et al. Impact of Ischemic Heart Failure Etiology on Cardiac Recovery During Mechanical Unloading. J. Am. Coll. Cardiol. 2016, 68, 1741–1752. [Google Scholar] [CrossRef] [PubMed]
- Birks, E.J.; Drakos, S.G.; Patel, S.R.; Lowes, B.D.; Selzman, C.H.; Starling, R.C.; Trivedi, J.; Slaughter, M.S.; Alturi, P.; Goldstein, D.; et al. Prospective Multicenter Study of Myocardial Recovery Using Left Ventricular Assist Devices (RESTAGE-HF [Remission from Stage D Heart Failure]): Medium-Term and Primary End Point Results. Circulation 2020, 142, 2016–2028. [Google Scholar] [CrossRef]
- Holzhauser, L.; Lang, R.M.; Raikhelkar, J.; Sayer, G.; Uriel, N. Reverse Ramp Testing in Left Ventricular Assist Device Support and Myocardial Recovery. ASAIO J. 2020, 66, e1–e4. [Google Scholar] [CrossRef]
- Monteagudo Vela, M.; Rial Baston, V.; Panoulas, V.; Riesgo Gil, F.; Simon, A. A detailed explantation assessment protocol for patients with left ventricular assist devices with myocardial recovery. Interact. Cardiovasc. Thorac. Surg. 2021, 32, 298–305. [Google Scholar] [CrossRef]
- Bonios, M.J.; Koliopoulou, A.; Wever-Pinzon, O.; Taleb, I.; Stehlik, J.; Xu, W.; Wever-Pinzon, J.; Catino, A.; Kfoury, A.G.; Horne, B.D.; et al. Cardiac Rotational Mechanics As a Predictor of Myocardial Recovery in Heart Failure Patients Undergoing Chronic Mechanical Circulatory Support: A Pilot Study. Circ. Cardiovasc. Imaging 2018, 11, e007117. [Google Scholar] [CrossRef]
- Kanelidis, A.J.; Grinstein, J. Left Ventricular Hemodynamics: Can a Direct Assessment of Left Ventricular Performance Help to Guide Myocardial Recovery in LVAD Recipients? J. Card. Fail. 2022, 28, 807–809. [Google Scholar] [CrossRef]
- Rosenbaum, A.N.; Geske, J.B.; Stulak, J.M.; Kushwaha, S.S.; Clavell, A.L.; Behfar, A. Left Ventricular Hemodynamics and Relationship With Myocardial Recovery and Optimization in Patients Supported on CF-LVAD Therapy. J. Card. Fail. 2022, 28, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Dandel, M.; Hetzer, R. Myocardial recovery during mechanical circulatory support: Weaning and explantation criteria. Heart Lung Vessel. 2015, 7, 280–288. [Google Scholar] [PubMed]
- Gupta, D.K.; Skali, H.; Rivero, J.; Campbell, P.; Griffin, L.; Smith, C.; Foster, C.; Claggett, B.; Glynn, R.J.; Couper, G.; et al. Assessment of myocardial viability and left ventricular function in patients supported by a left ventricular assist device. J. Heart Lung Transplant. 2014, 33, 372–381. [Google Scholar] [CrossRef] [PubMed]
- Pana, T.A.; Savla, J.; Kepinski, I.; Fairbourn, A.; Afzal, A.; Mammen, P.; Drazner, M.; Subramaniam, R.M.; Xing, C.; Morton, K.A.; et al. Bidirectional Changes in Myocardial (18)F-Fluorodeoxyglucose Uptake After Human Ventricular Unloading. Circulation 2022, 145, 151–154. [Google Scholar] [CrossRef]
- Shah, P.; Psotka, M.; Taleb, I.; Alharethi, R.; Shams, M.A.; Wever-Pinzon, O.; Yin, M.; Latta, F.; Stehlik, J.; Fang, J.C.; et al. Framework to Classify Reverse Cardiac Remodeling With Mechanical Circulatory Support: The Utah-Inova Stages. Circ. Heart Fail. 2021, 14, e007991. [Google Scholar] [CrossRef]
- Wang, N.C.; Hussain, A.; Adelstein, E.C.; Althouse, A.D.; Sharbaugh, M.S.; Jain, S.K.; Shalaby, A.A.; Voigt, A.H.; Saba, S. Myocardial recovery after cardiac resynchronization therapy in left bundle branch block-associated idiopathic nonischemic cardiomyopathy: A NEOLITH II substudy. Ann. Noninvasive Electrocardiol. 2019, 24, e12603. [Google Scholar] [CrossRef]
- Goldfinger, J.Z.; Nair, A.P. Myocardial recovery and the failing heart: Medical, device and mechanical methods. Ann. Glob. Health 2014, 80, 55–60. [Google Scholar] [CrossRef]
- Nijst, P.; Martens, P.; Mullens, W. Heart Failure with Myocardial Recovery—The Patient Whose Heart Failure Has Improved: What Next? Prog. Cardiovasc. Dis. 2017, 60, 226–236. [Google Scholar] [CrossRef]
- Gopinathannair, R.; Dhawan, R.; Lakkireddy, D.R.; Murray, A.; Angus, C.R.; Farid, T.; Mar, P.L.; Atkins, D.; Olshansky, B. Predictors of myocardial recovery in arrhythmia-induced cardiomyopathy: A multicenter study. J. Cardiovasc. Electrophysiol. 2021, 32, 1085–1092. [Google Scholar] [CrossRef]
- Birks, E.J.; Tansley, P.D.; Hardy, J.; George, R.S.; Bowles, C.T.; Burke, M.; Banner, N.R.; Khaghani, A.; Yacoub, M.H. Left ventricular assist device and drug therapy for the reversal of heart failure. N. Engl. J. Med. 2006, 355, 1873–1884. [Google Scholar] [CrossRef]
- Kyriakopoulos, C.P.; Kapelios, C.J.; Stauder, E.L.; Taleb, I.; Hamouche, R.; Sideris, K.; Koliopoulou, A.G.; Bonios, M.J.; Drakos, S.G. LVAD as a Bridge to Remission from Advanced Heart Failure: Current Data and Opportunities for Improvement. J. Clin. Med. 2022, 11, 3542. [Google Scholar] [CrossRef] [PubMed]
- McCullough, M.; Caraballo, C.; Ravindra, N.G.; Miller, P.E.; Mezzacappa, C.; Levin, A.; Gruen, J.; Rodwin, B.; Reinhardt, S.; van Dijk, D.; et al. Neurohormonal Blockade and Clinical Outcomes in Patients With Heart Failure Supported by Left Ventricular Assist Devices. JAMA Cardiol. 2020, 5, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Mahfood Haddad, T.; Saurav, A.; Smer, A.; Azzouz, M.S.; Akinapelli, A.; Williams, M.A.; Alla, V.M. Cardiac Rehabilitation in Patients With Left Ventricular Assist Device: A Systematic Review and Meta-analysis. J. Cardiopulm Rehabil. Prev. 2017, 37, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Adamopoulos, S.; Corra, U.; Laoutaris, I.D.; Pistono, M.; Agostoni, P.G.; Coats, A.J.S.; Crespo Leiro, M.G.; Cornelis, J.; Davos, C.H.; Filippatos, G.; et al. Exercise training in patients with ventricular assist devices: A review of the evidence and practical advice. A position paper from the Committee on Exercise Physiology and Training and the Committee of Advanced Heart Failure of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2019, 21, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Taleb, I.; Tseliou, E.; Fang, J.C.; Drakos, S.G. A Mechanical Bridge to Recovery as a Bridge to Discovery: Learning From Few and Applying to Many. Circulation 2022, 145, 562–564. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Conducted | Characteristics | Outcome |
|---|---|---|---|
| Thoratec registry [36] | 1990–1999 | Characteristics: 22 patients with non-ischemic heart failure (12 myocarditis, 4 sarcoid cardiomyopathy, 1 viral, 2 idiopathic), 12 female, mean age 32 years, duration of support 57 days, use of Thoratec device (pneumatic LVAD) | Benefit of LVAD in acute myocarditis |
| Berlin Group [37,38] | 1995–2004 and then until 2008 | 32 patients from a total of 131 with dilated cardiomyopathy. Eligible: 30 men, 4.5 months average LVAD support Follow-up study 2008. Of 188 patients with idiopathic dilated cardiomyopathy in 30 LVAD removal. Characteris-tics: LVEF 30–44% and LVEDD 56–60 mm at device removal, use of LVAD, BiVAD, RVAD systems. Results: probability of survival 5 and 10 years after LVAD weaning when at 1 year there was no recurrence of heart failure 84% and 61%, respectively | Of the 32, 4 died 2 for cardiac reasons, 2 for non-cardiac reasons, remaining survival >3 years. Overall study conclusion: LVEDD > 55, LVEF < 45% before LVAD removal and HF duration ≥ 5 years are poor prognostic factors. Patients having 2 of the 3 factors have a reduced chance of recovery Patients with a shorter history of heart failure, were younger and required less time on LVAD support have an increased likelihood of recovery |
| University of Pittsburgh study [39] | 1996–2003 | Of 154 subjects with LVAD, removal was considered possible in 10. Characteristics: 2 ischemic and 8 non-ischemic etiology (4 peripartum cardiomyopathy, 3 myocarditis, 1 idiopathic), 120 days mean support time, mean age 30 years, 88% women | LVAD support offers better outcomes in patients with gestational cardiomyopathy and myocarditis |
| IMAC2 (Intervention in Myocarditis and Acute Cardiomyopathy) cohort [40] | 2002–2008 | 14 patients with acute myocarditis had LVAD inserted, 8 were candidates for recovery. Characteristics: mean age 30 years, 38% male, 10 with pulsatile LVAD 4 with continuous flow, implantation 1 month after symptoms, in recoveries increased inflammation, little fibrosis and reduced LVEDD while in non-recoveries vice versa | Increased likelihood of recovery in recent-onset cardiomyopathy, biopsy and LVEDD guide potential recovery |
| MCS UNOS (United Network Organ Sharing) registry [41] | 2005–2013 | Out of 686 patients, LVAD removal was performed due to recovery in 34. Characteristics of persons with recovery: average age 40 years, women 41%, 33 HeartMate II and 1 Heartware device and average duration of support 382 days while in 66% of them recovery maintained after 1 year | Patients who experienced recovery were younger, female, had non-ischemic cardiomyopathy, had a lower BMI, had not had a prior ICD implanted and had a lower serum creatinine |
| Montefiore Medical Center, Albert Einstein College of Medicine, Bronx, New York [42] | 2006 | 21 patients (8 with coronary artery disease, 13 with idiopathic dilated cardiomyopathy) of 34 initially placed with an LVAD were given neurohormonal blockade and attempted weaning. Characteristics of selected patients: mean age 48 years, disease duration before LVAD up to 821 days, 20 HeartMate II and 1 VentrAssist device. Results: 16 subjects developed reverse remodeling and after device 3 downshift control weaned | The use of neurohormonal blockade aids in reverse remodeling while reduced pre-LVAD disease duration, less fibrosis, less hypertrophy and increased LVAD turns increase the likelihood of weaning |
| Harefield Study [38,43] | 2006–2009 | 15 patients received a pulsatile flow LVAD and pharmacologic protocol for heart failure + clebuterol with 11 having the device removed. Characteristics of patients who recovered: LVEF at withdrawal 65 % mean, LVEDD 56 mm, 321 days of support. Final results: freedom from heart failure deregulation at 1 and 4 years 100% and 89%, respectively 20 patients with nonischemic cardiomyopathy were implanted with a HeartMate II continuous flow LVAD device in combination with neurohormonal blockade and clebuterol. Patient characteristics before LVAD placement: age 16–58, LVEDD 57–91 mm, LVEF 7–34%, PCWP 31 mmHg, supported by inotropes, 16 were male, mean age results: 10 patients experienced 1–3 years of recovery with 66% having experienced heart failure prior to LVAD implantation up to 6 months prior. Further, before device removal at low flow they had a mean LVEF of 70%, LVEDD of 48 mm, PCWP of 6 mmHg | Medication and pulsatile flow LVADs promote recovery. The use of continuous flow LVAD in combination with medication can promote myocardial recovery |
| INTERMACS (Interagency Registry for Mechanically Assisted Circulatory Support) Registry [44] | 2006–2015 | Of 13,454 LVAD patients 163 had recovery capable of weaning from the device and 8805 had partial recovery. Characteristics of patients with LVAD removal: Mean age 45 years, 38.7% female, 85.9% non-ischemic cardiomyopathy, 95.7% axial flow LVAD, mean duration of support 16 months | Younger patients (<50), of non-ischemic etiology, with LVEDD < 6.5 cm, PASP < 50 mmHg, time to heart failure diagnosis < 2 years, with axial flow LVAD systems, without optimal medication, had an increased chance of recovery treatment and with diagnoses of myocarditis, cardiomyopathy of pregnancy and cardiomyopathy from the use of andriamycin. Finally, patients in whom a pulsatile flow LVAD was placed had a greater chance of recovery compared to those in continuous flow LVADs |
| Utah Transplantation Affiliated Hospitals Cardiac Transplant Program [45] | 2008–2014 | 154 consecutive patients with documented chronic and dilated cardiomyopathy (ischemic cardiomyopathy/ICM, n = 61; non-ischemic cardiomyopathy/NICM, n = 93) requiring durable support with continuous-flow LVAD were prospectively evaluated with serial echocardiograms and right heart catheterizations Among patients supported with LVAD for at least 6 months, 5% of subjects with ICM and 21% of subjects with NICM achieved left ventricular ejection fraction ≥40% (p = 0.034). LV end-diastolic and end-systolic volumes and diastolic function were significantly and similarly improved in patients with ICM and NICM | LVAD-associated unloading for 6 months resulted in a substantial improvement in myocardial structure, and systolic and diastolic function in 1 in 20 ICM and 1 in 5 NICM patients |
| RESTAGE-HF (REmission from Stage D Heart Failure) Study [46] | 2012–2015 | Of the 40 patients selected, 36 were able to implement the protocol and of these 16 eventually had the LVAD removed. Characteristics of selected patients: mean age 35 years, 68% male, with non-ischemic heart disease of less than 5 years’ duration, 95% with fibrotic support, 17.5% with temporary mechanical support, with mean LVEF values of 15%, and LVAD device the HeartMate II. Final results: of the 36 patients, 16 underwent LVAD removal where they survived 12 months after removal and 14 of these tended to reach 3 years. Further, only serum creatinine was statistically significant in predicting recovery | The use of specific drugs as well as the monitoring of patients with a specific protocol increases the likelihood and duration of recovery after removal of LVAD systems [46] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chrysakis, N.; Xanthopoulos, A.; Magouliotis, D.; Starling, R.C.; Drakos, S.G.; Triposkiadis, F.; Skoularigis, J. Myocardial Recovery. Diagnostics 2023, 13, 1504. https://doi.org/10.3390/diagnostics13081504
Chrysakis N, Xanthopoulos A, Magouliotis D, Starling RC, Drakos SG, Triposkiadis F, Skoularigis J. Myocardial Recovery. Diagnostics. 2023; 13(8):1504. https://doi.org/10.3390/diagnostics13081504
Chicago/Turabian StyleChrysakis, Nikolaos, Andrew Xanthopoulos, Dimitrios Magouliotis, Randall C. Starling, Stavros G. Drakos, Filippos Triposkiadis, and John Skoularigis. 2023. "Myocardial Recovery" Diagnostics 13, no. 8: 1504. https://doi.org/10.3390/diagnostics13081504