
Craniovertebral Junction Instability after Oncological Resection: A Narrative Review
 , ,
, , 
Abstract
:1. Introduction
Search Strategy and Studies Selection
2. Anatomy and Biomechanics
2.1. The Occipital Bone
2.2. The Atlas
2.3. The Axis
2.4. The Joint Complex
2.5. The Craniocervical Muscle Complex
2.6. Biomechanics Aspects
3. Pathological and Radiological Features of the CVJ Neoplasms
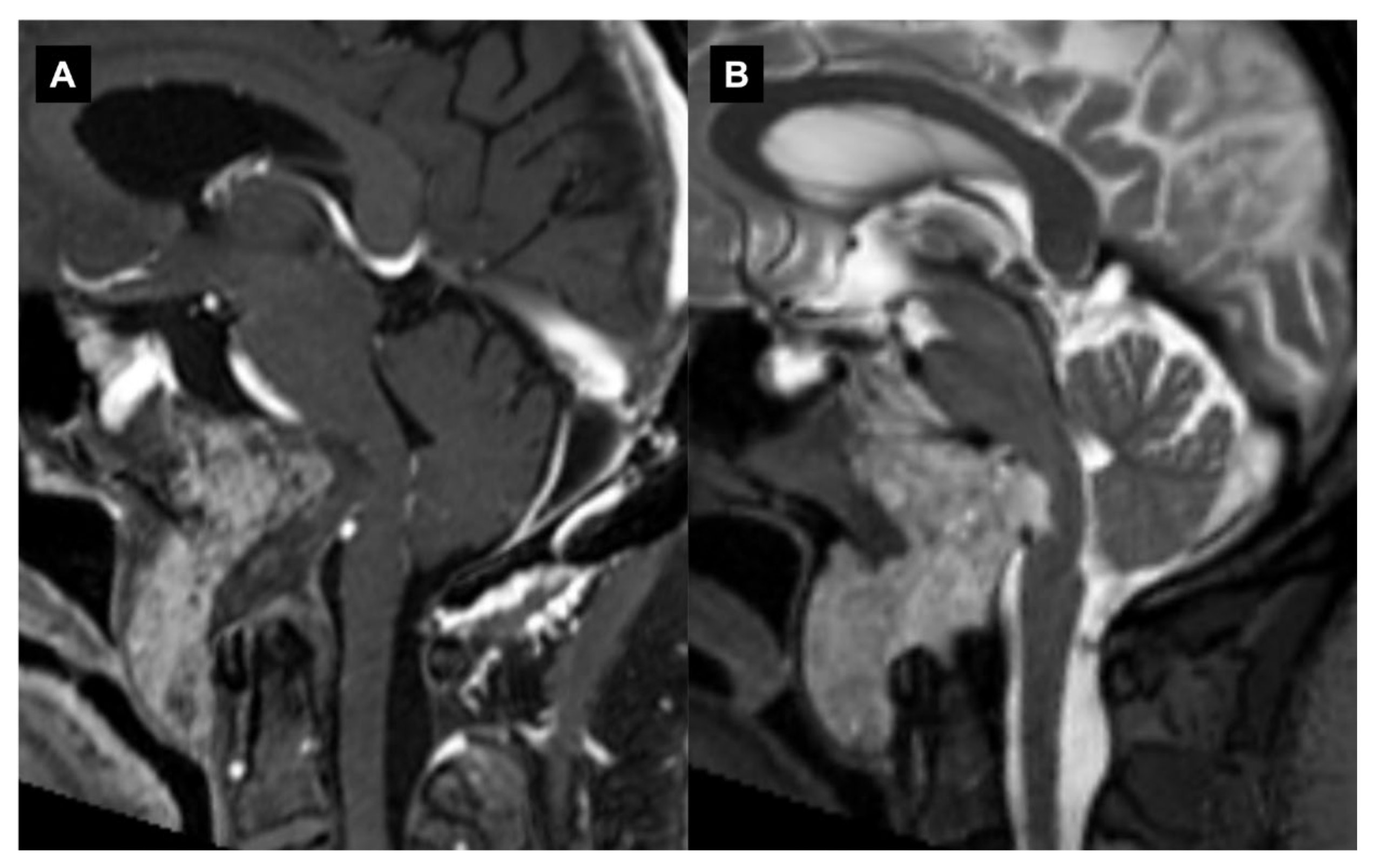
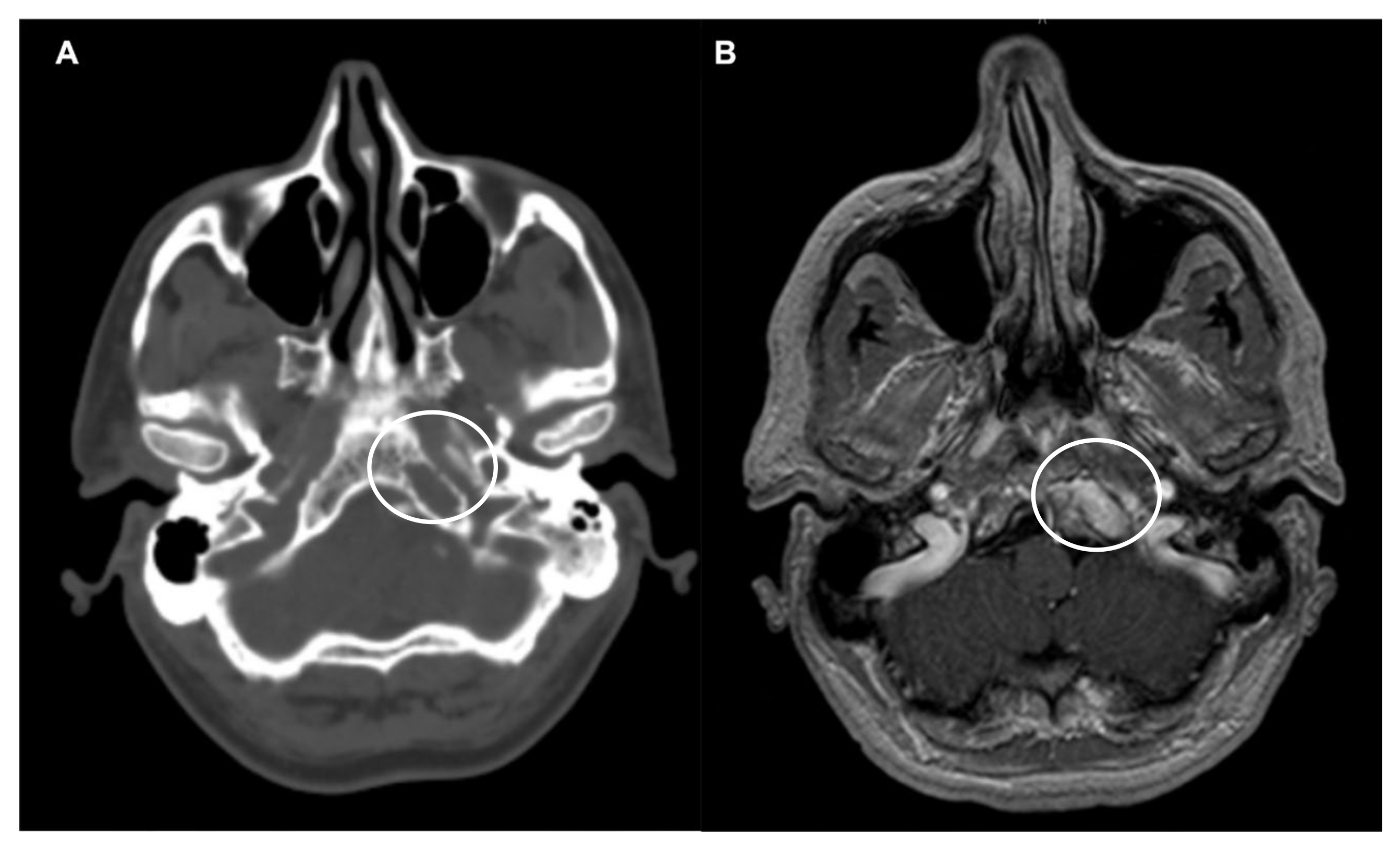
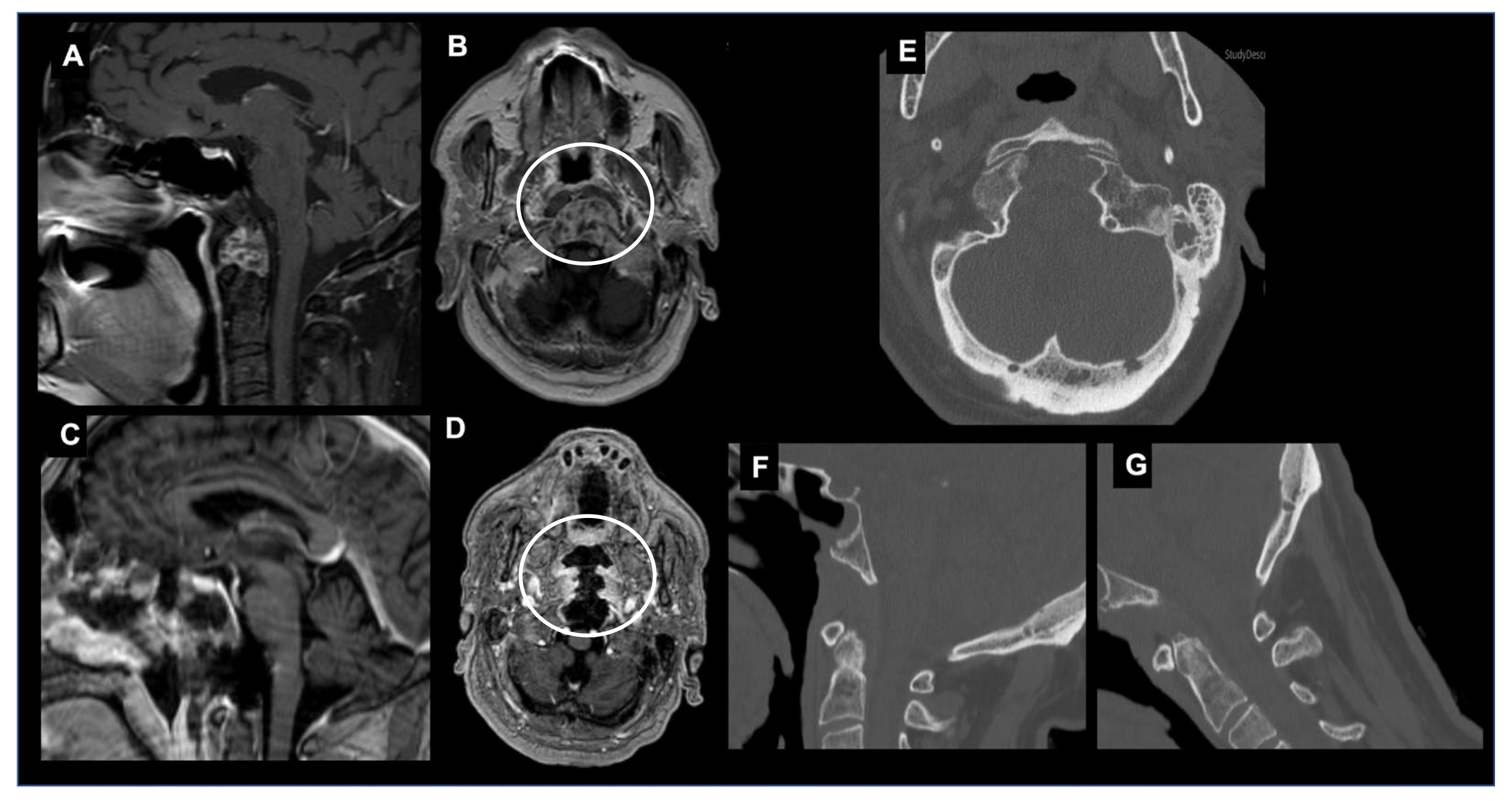
3.1. Chordomas
3.2. Meningiomas
3.3. Spinal Nerve Sheath Tumors
3.4. Chondrosarcomas
3.5. Secondary Tumors of the CVJ
4. Radiological Criteria of CVJ Instability
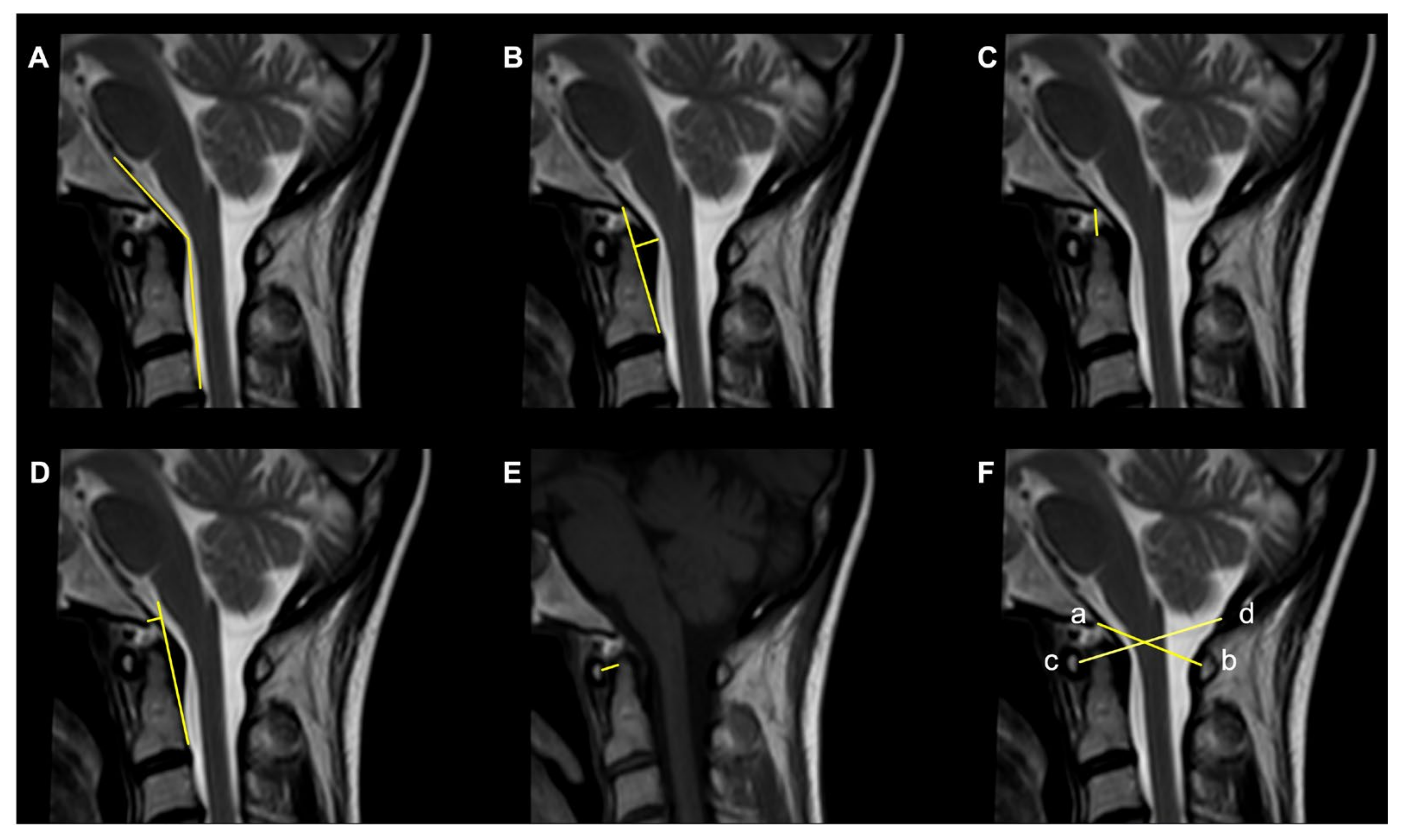
- The Clivoaxial Angle (CXA), which is the angle between the clivus line and the posterior axial line, examines the brainstem deformity induced by the odontoid process. A CXA of 135 degrees or less is considered “potentially pathological” [71].
- The Grabb–Oakes line, which is the perpendicular distance from the dura to the line drawn from the basion to the posterior inferior edge of the C2 vertebra. It is a measure of the encroachment of the odontoid process into the upper spinal canal (basilar invagination) and investigates ventral brainstem compression. A measurement ≥9 mm is considered pathological [68].
- The Basion–Dens Interval (BDI) measures the vertical distance between the basion and the dens and is considered pathological if ≥10 mm [72].
- The Basion–Axial Interval (BAI) is the distance from the tip of the basion to the posterior axial line and is pathological if ≥12 mm [72].
- The translational BAI and translational BDI are the change in mm of the BAI and BDI between the flexion and extension positions of the head [68].
- The Atlantodental Interval (ADI) is the distance between the posterior surface of the anterior atlas ring and the anterior surface of the odontoid process. An ADI >5 mm in adults and >4 mm in children is an indication for surgery [73].
- The Condyle–C1 interval (CC1) measures the distance between the occipital condyle and C1 at four equidistant points and is pathological in children if >4 mm, with a high diagnostic accuracy [73].
- The Powers ratio is calculated by measuring the distance between the basion and the posterior arch of the atlas and then dividing it by the distance between the opisthion and the anterior arch of the atlas [74].
5. Surgical Approaches to the CVJ
6. Anterior Surgical Approaches to the CVJ
6.1. Transoral Approach
6.2. Transoral Endoscopic Approach
6.3. Endoscopic Endonasal Approach
6.4. Instability after EEA
7. Posterior Surgical Approaches to the CVJ
7.1. Type of Tumor and Aim of Surgery
7.2. Approach Selection and Anatomical Considerations
7.3. Spinal Instability
7.4. Posterior Approach
7.5. Posterolateral Approach
8. Principles of Fixation Techniques and Materials
8.1. Indication for Stabilization
8.2. Options to Stabilize the CVJ
8.3. Technical Aspects
9. Limitations and Future Research
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karam, Y.R.; Menezes, A.H.; Traynelis, V.C. Posterolateral approaches to the craniovertebral junction. Neurosurgery 2010, 66, A135–A140. [Google Scholar] [CrossRef]
- Frempong-Boadu, A.K.; Faunce, W.A.; Fessler, R.G. Endoscopically assisted transoral-transpharyngeal approach to the craniovertebral junction. Neurosurgery 2002, 51, S60–S66. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.; Barrenechea, I.J.; Lesser, J.; Sen, C.; Perin, N.I. Occipitocervical fusion after resection of craniovertebral junction tumors. J. Neurosurg. Spine 2006, 4, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Zuckerman, S.L.; Kreines, F.; Powers, A.; Iorgulescu, J.B.; Elder, J.B.; Bilsky, M.H.; Laufer, I. Stabilization of Tumor-Associated Craniovertebral Junction Instability: Indications, Operative Variables, and Outcomes. Neurosurgery 2017, 81, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Luksanapruksa, P.; Buchowski, J.M.; Wright, N.M.; Valone, F.H.; Peters, C.; Bumpass, D.B. Outcomes and effectiveness of posterior occipitocervical fusion for suboccipital spinal metastases. J. Neurosurg. Spine 2017, 26, 554–559. [Google Scholar] [CrossRef]
- Baethge, C.; Goldbeck-Wood, S.; Mertens, S. SANRA-a scale for the quality assessment of narrative review articles. Res. Integr. Peer Rev. 2019, 4, 5. [Google Scholar] [CrossRef]
- Rhoton, A. Rhoton Cranial Anatomy and Surgical Approaches; Congress of Neurological Surgeons: Schaumburg, IL, USA, 2003. [Google Scholar]
- Unnithan, A.S.; Omofoye, O.; Lemos-Rodriguez, A.M.; Sreenath, S.B.; Doan, V.; Zanation, A.M.; Recinos, P.; Sasaki-Adams, D.M. The Expanded Endoscopic Endonasal Approach to Anterior Communicating Artery Aneurysms: A Cadaveric Morphometric Study. World Neurosurg. 2016, 89, 26–32. [Google Scholar] [CrossRef]
- Morera, V.A.; Fernandez-Miranda, J.C.; Prevedello, D.M.; Madhok, R.; Barges-Coll, J.; Gardner, P.; Carrau, R.; Snyderman, C.H.; Rhoton, A.L.; Kassam, A.B. “Far-Medial” Expanded Endonasal Approach to the Inferior Third of the Clivus. Oper. Neurosurg. 2010, 66, ons211–ons220. [Google Scholar] [CrossRef]
- Menezes, A.H.; Traynelis, V.C. Anatomy and biomechanics of normal craniovertebral junction (a) and biomechanics of stabilization (b). Childs Nerv. Syst. 2008, 24, 1091–1100. [Google Scholar] [CrossRef]
- Steinmetz, M.P.; Mroz, T.E.; Benzel, E.C. Craniovertebral junction: Biomechanical considerations. Neurosurgery 2010, 66, 7–12. [Google Scholar] [CrossRef]
- Lopez, A.J.; Scheer, J.K.; Leibl, K.E.; Smith, Z.A.; Dlouhy, B.J.; Dahdaleh, N.S. Anatomy and biomechanics of the craniovertebral junction. Neurosurg. Focus 2015, 38, E2. [Google Scholar] [CrossRef] [PubMed]
- Menezes, A.H. Craniocervical developmental anatomy and its implications. Childs Nerv. Syst. 2008, 24, 1109–1122. [Google Scholar] [CrossRef]
- Menezes, A.H.; VanGilder, J.C.; Graf, C.J.; McDonnell, D.E. Craniocervical abnormalities. A comprehensive surgical approach. J. Neurosurg. 1980, 53, 444–455. [Google Scholar] [CrossRef]
- Tubbs, R.S.; Kelly, D.R.; Humphrey, E.R.; Chua, G.D.; Shoja, M.M.; Salter, E.G.; Acakpo-Satchivi, L.; Wellons, J.C.; Blount, J.P.; Oakes, W.J. The tectorial membrane: Anatomical, biomechanical, and histological analysis. Clin. Anat. 2007, 20, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Debernardi, A.; DʼAliberti, G.; Talamonti, G.; Villa, F.; Piparo, M.; Collice, M. The craniovertebral junction area and the role of the ligaments and membranes. Neurosurgery 2015, 76 (Suppl. S1), S22–S32. [Google Scholar] [CrossRef] [PubMed]
- Menezes, A.H.; Traynelis, V.C.; Fenoy, A.J.; Gantz, B.J.; Kralik, S.F.; Donovan, K.A. Honored guest presentation: Surgery at the crossroads: Craniocervical neoplasms. Clin. Neurosurg. 2005, 52, 218–228. [Google Scholar]
- Menezes, A.H. Craniovertebral junction neoplasms in the pediatric population. Childs Nerv. Syst. 2008, 24, 1173–1186. [Google Scholar] [CrossRef]
- Chen, Y.F.; Liu, H.M. Imaging of craniovertebral junction. Neuroimaging Clin. N. Am. 2009, 19, 483–510. [Google Scholar] [CrossRef]
- Cavallo, L.M.; Messina, A.; Cappabianca, P.; Esposito, F.; de Divitiis, E.; Gardner, P.; Tschabitscher, M. Endoscopic endonasal surgery of the midline skull base: Anatomical study and clinical considerations. Neurosurg. Focus 2005, 19, E2. [Google Scholar] [CrossRef]
- Moulding, H.D.; Bilsky, M.H. Metastases to the craniovertebral junction. Neurosurgery 2010, 66, A113–A118. [Google Scholar] [CrossRef]
- Fehlings, M.G.; David, K.S.; Vialle, L.; Vialle, E.; Setzer, M.; Vrionis, F.D. Decision making in the surgical treatment of cervical spine metastases. Spine 2009, 34, S108–S117. [Google Scholar] [CrossRef]
- Benglis, D.; Levi, A.D. Neurologic findings of craniovertebral junction disease. Neurosurgery 2010, 66, A13–A21. [Google Scholar] [CrossRef] [PubMed]
- Dickman, C.A.; Hadley, M.N.; Pappas, C.T.E.; Sonntag, K.H.; Geisler, F.H. Cruciate paralysis: A clinical and radiographic analysis of injuries to the cervicomedullary junction. J. Neurosurg. 1990, 73, 850–858. [Google Scholar] [CrossRef] [PubMed]
- Michie, I.; Clark, M. Neurological syndromes associated with cervical and craniocervical anomalies. Arch. Neurol. 1968, 18, 241–247. [Google Scholar] [CrossRef]
- Fourney, D.R.; Gokaslan, Z.L. Spinal instability and deformity due to neoplastic conditions. Neurosurg. Focus 2003, 14, e8. [Google Scholar] [CrossRef] [PubMed]
- Meyer, F.B.; Ebersold, M.J.; Reese, D.F. Benign tumors of the foramen magnum. J. Neurosurg. 1984, 61, 136–142. [Google Scholar] [CrossRef]
- Garg, K.; Tandon, V.; Kumar, R.; Chandra, P.S.; Kale, S.S.; Sharma, B.S.; Mahapatra, A.K. Craniovertebral Junction Anomalies: An Overlooked Cause of “Posterior Circulation Stroke”. Neurol. India 2022, 70, 149. [Google Scholar]
- Erdem, E.; Angtuaco, E.; Van Hemert, R.; Park, J.S.; Al-mefty, O. Comprehensive Review of Intracranial Chordoma. Radiographics 2003, 23, 995–1009. [Google Scholar] [CrossRef]
- Jian, B.J.; Bloch, O.G.; Yang, I.; Han, S.J.; Aranda, D.; Parsa, A.T. A comprehensive analysis of intracranial chordoma and survival: A systematic review. Br. J. Neurosurg. 2011, 25, 446–453. [Google Scholar] [CrossRef]
- Glasauer, F.E.; Egnatchick, J.E. Restless legs syndrome: An unusual cause for a perplexing syndrome. Spinal Cord 1999, 37, 862–865. [Google Scholar] [CrossRef]
- Vogl, T.J.; Bisdas, S. Differential diagnosis of jugular foramen lesions. Skull Base 2009, 19, 3–16. [Google Scholar] [CrossRef]
- Parlato, C.; Tessitore, E.; Schonauer, C.; Moraci, A. Management of benign craniovertebral junction tumors. Acta Neurochir. 2003, 145, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Fiani, B.; Jarrah, R.; Shields, J.; Durrani, S.; Panico, N.; Mualem, W.; Nathani, K.R.; Pasko, K. A Comprehensive Overview of Pediatric Neoplasms at the Craniocervical Junction: Meningiomas, Schwannomas, and Chordomas. Cureus 2022, 14, e31083. [Google Scholar] [CrossRef] [PubMed]
- Bakker, S.H.; Jacobs, W.C.H.; Pondaag, W.; Gelderblom, H.; Nout, R.A.; Dijkstra, P.D.S.; Peul, W.C.; Vleggeert-Lankamp, C.L.A. Chordoma: A systematic review of the epidemiology and clinical prognostic factors predicting progression-free and overall survival. Eur. Spine J. 2018, 27, 3043–3058. [Google Scholar] [CrossRef] [PubMed]
- Beccaria, K.; Sainte-Rose, C.; Zerah, M.; Puget, S. Paediatric Chordomas. Orphanet J. Rare Dis. 2015, 10, 116. [Google Scholar] [CrossRef]
- Fernandez-Miranda, J.C.; Gardner, P.A.; Snyderman, C.H.; Devaney, K.O.; Mendenhall, W.M.; Suárez, C.; Rinaldo, A.; Ferlito, A. Clival chordomas: A pathological, surgical, and radiotherapeutic review. Head Neck 2014, 36, 892–906. [Google Scholar] [CrossRef]
- La Corte, E.; Broggi, M.; Raggi, A.; Schiavolin, S.; Acerbi, F.; Danesi, G.; Farinotti, M.; Felisati, G.; Maccari, A.; Pollo, B.; et al. Peri-operative prognostic factors for primary skull base chordomas: Results from a single-center cohort. Acta Neurochir. 2020, 163, 689–697. [Google Scholar] [CrossRef]
- Kano, H.; Lunsford, L.D. Stereotactic radiosurgery of intracranial chordomas, chondrosarcomas, and glomus tumors. Neurosurg. Clin. N. Am. 2013, 24, 553–560. [Google Scholar] [CrossRef]
- Alahmari, M.; Temel, Y. Skull base chordoma treated with proton therapy: A systematic review. Surg. Neurol. Int. 2019, 10, 96. [Google Scholar] [CrossRef]
- Zou, M.X.; Lv, G.H.; Zhang, Q.S.; Wang, S.F.; Li, J.; Wang, X. Bin Prognostic Factors in Skull Base Chordoma: A Systematic Literature Review and Meta-Analysis. World Neurosurg. 2018, 109, 307–327. [Google Scholar] [CrossRef]
- Hung, Y.P.; Diaz-Perez, J.A.; Cote, G.M.; Wejde, J.; Schwab, J.H.; Nardi, V.; Chebib, I.A.; Deshpande, V.; Selig, M.K.; Bredella, M.A.; et al. Dedifferentiated Chordoma: Clinicopathologic and Molecular Characteristics with Integrative Analysis. Am. J. Surg. Pathol. 2020, 44, 1213–1223. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.F.; Hao, D.P.; Chen, H.S.; Liu, J.H.; Hou, F.; Xu, W.J. Computed tomography and magnetic resonance imaging features of cervical chordoma. Oncol. Lett. 2018, 16, 861–865. [Google Scholar] [CrossRef]
- Santegoeds, R.G.C.; Temel, Y.; Beckervordersandforth, J.C.; Van Overbeeke, J.J.; Hoeberigs, C.M. State-of-the-Art Imaging in Human Chordoma of the Skull Base. Curr. Radiol. Rep. 2018, 6, 16. [Google Scholar] [CrossRef] [PubMed]
- La Corte, E.; Dei Cas, M.; Raggi, A.; Patanè, M.; Broggi, M.; Schiavolin, S.; Calatozzolo, C.; Pollo, B.; Pipolo, C.; Bruzzone, M.G.; et al. Long and Very-Long-Chain Ceramides Correlate with A More Aggressive Behavior in Skull Base Chordoma Patients. Int. J. Mol. Sci. 2019, 20, 4480. [Google Scholar] [CrossRef]
- Azzopardi, C.; Grech, R.; Mizzi, A. Teaching NeuroImages: Chordoma. Neurology 2014, 83, e110–e111. [Google Scholar] [CrossRef]
- Paun, L.; Gondar, R.; Borrelli, P.; Meling, T.R. Foramen magnum meningiomas: A systematic review and meta-analysis. Neurosurg. Rev. 2021, 44, 2583–2596. [Google Scholar] [CrossRef]
- McGovern, S.L.; Aldape, K.D.; Munsell, M.F.; Mahajan, A.; DeMonte, F.; Woo, S.Y. A comparison of World Health Organization tumor grades at recurrence in patients with non-skull base and skull base meningiomas. J. Neurosurg. 2010, 112, 925–933. [Google Scholar] [CrossRef] [PubMed]
- Sade, B.; Chahlavi, A.; Krishnaney, A.; Nagel, S.; Choi, E.; Lee, J.H. World Health Organization Grades II and III meningiomas are rare in the cranial base and spine. Neurosurgery 2007, 61, 1194–1198. [Google Scholar] [CrossRef]
- Dührsen, L.; Emami, P.; Matschke, J.; Abboud, T.; Westphal, M.; Regelsberger, J. Meninigiomas of the Craniocervical Junction--A Distinctive Subgroup of Meningiomas. PLoS ONE 2016, 11, e0153405. [Google Scholar] [CrossRef] [PubMed]
- Harter, P.N.; Braun, Y.; Plate, K.H. Classification of meningiomas-advances and controversies. Chin. Clin. Oncol. 2017, 6, S2. [Google Scholar] [CrossRef]
- Miranda, P.; Simal, J.A.; Vila, M.; Hernández, M.; Menor, F.; Álvarez-Garijo, J.A. Posterior fossa clear cell meningioma without dural attachment in a child. Childs Nerv. Syst. 2009, 25, 389–392. [Google Scholar] [CrossRef]
- Wu, B.; Shen, S.H.; Chen, L.Y.; Liu, W.D. Dural Tail Sign in the Resection of Ventral Foramen Magnum Meningiomas via a Far Lateral Approach: Surgical Implications. World Neurosurg. 2015, 84, 1402–1411. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Takeda, M.; Takahashi, T.; Yamahata, H.; Mitsuhara, T.; Niiro, T.; Hanakita, J.; Hida, K.; Arita, K.; Kurisu, K. Ginkgo leaf sign: A highly predictive imaging feature of spinal meningioma. J. Neurosurg. Spine 2015, 23, 642–646. [Google Scholar] [CrossRef]
- Cavalcanti, D.D.; Martirosyan, N.L.; Verma, K.; Safavi-Abbasi, S.; Porter, R.W.; Theodore, N.; Sonntag, V.K.H.; Dickman, C.A.; Spetzler, R.F. Surgical management and outcome of schwannomas in the craniocervical region. J. Neurosurg. 2011, 114, 1257–1267. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, F.J.; Folpe, A.L.; Giannini, C.; Perry, A. Pathology of peripheral nerve sheath tumors: Diagnostic overview and update on selected diagnostic problems. Acta Neuropathol. 2012, 123, 295–319. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wang, X.; Wu, H.; Chen, Z.; Yuan, Q.; Jian, F. C2 dumbbell-shaped peripheral nerve sheath tumors: Surgical management and relationship with venous structures. Clin. Neurol. Neurosurg. 2016, 151, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.A.; Kumar, M.; Malgonde, M. Dumbbell-shaped neurofibroma of the upper thoracic spine: A case report. South Asian J. Cancer 2013, 2, 226. [Google Scholar] [CrossRef]
- Mehta, G.U.; Huynh, H.; Lekovic, G.P. Peripheral nerve sheath tumors in Neurofibromatosis Type 2: Surgical and histopathologic features. Clin. Neurol. Neurosurg. 2020, 190, 105649. [Google Scholar] [CrossRef]
- Tora, M.S.; Xenos, D.; Texakalidis, P.; Boulis, N.M. Treatment of neurofibromatosis 1-associated malignant peripheral nerve sheath tumors: A systematic review. Neurosurg. Rev. 2020, 43, 1039–1046. [Google Scholar] [CrossRef]
- Abul-Kasim, K.; Thurnher, M.M.; McKeever, P.; Sundgren, P.C. Intradural spinal tumors: Current classification and MRI features. Neuroradiology 2008, 50, 301–314. [Google Scholar] [CrossRef]
- Soderlund, K.A.; Smith, A.B.; Rushing, E.J.; Smirniotopolous, J.G. Radiologic-pathologic correlation of pediatric and adolescent spinal neoplasms: Part 2, Intradural extramedullary spinal neoplasms. AJR. Am. J. Roentgenol. 2012, 198, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Koeller, K.K.; Shih, R.Y. Intradural Extramedullary Spinal Neoplasms: Radiologic-Pathologic Correlation. Radiographics 2019, 39, 468–490. [Google Scholar] [CrossRef] [PubMed]
- Dasenbrock, H.H.; Chiocca, E.A. Skull base chordomas and chondrosarcomas: A population-based analysis. World Neurosurg. 2015, 83, 468–470. [Google Scholar] [CrossRef]
- Vujovic, S.; Henderson, S.; Presneau, N.; Odell, E.; Jacques, T.; Tirabosco, R.; Boshoff, C.; Flanagan, A. Brachyury, a crucial regulator of notochordal development, is a novel biomarker for chordomas. J. Pathol. 2006, 209, 157–165. [Google Scholar] [CrossRef]
- Pashayan, R.; Cavanaugh, W.M.; Warshel, C.D.; Payne, D.R. Plasmacytoma of the Cervical Spine: A Case Study. J. Chiropr. Med. 2017, 16, 170–174. [Google Scholar] [CrossRef]
- O’Sullivan, M.D.; Lyons, F.; Morris, S.; Synnott, K.; Munigangaiah, S.; Devitt, A. Metastasis Affecting Craniocervical Junction: Current Concepts and an Update on Surgical Management. Glob. Spine J. 2018, 8, 866–871. [Google Scholar] [CrossRef] [PubMed]
- Henderson, F.C.; Francomano, C.A.; Koby, M.; Tuchman, K.; Adcock, J.; Patel, S. Cervical medullary syndrome secondary to craniocervical instability and ventral brainstem compression in hereditary hypermobility connective tissue disorders: 5-year follow-up after craniocervical reduction, fusion, and stabilization. Neurosurg. Rev. 2019, 42, 915–936. [Google Scholar] [CrossRef]
- Riascos, R.; Bonfante, E.; Cotes, C.; Guirgui, M.; Hakimelahi, R.; West, C. Imaging of Atlanto-Occipital and Atlantoaxial Traumatic Injuries: What the Radiologist Needs to Know. Radiographics 2015, 35, 2121–2134. [Google Scholar] [CrossRef]
- Kasliwal, M.K.; Fontes, R.B.; Traynelis, V.C. Occipitocervical dissociation-incidence, evaluation, and treatment. Curr. Rev. Musculoskelet. Med. 2016, 9, 247–254. [Google Scholar] [CrossRef]
- Henderson, F.C.; Henderson, F.C.; Wilson, W.A.; Mark, A.S.; Koby, M. Utility of the clivo-axial angle in assessing brainstem deformity: Pilot study and literature review. Neurosurg. Rev. 2018, 41, 149–163. [Google Scholar] [CrossRef]
- Rojas, C.A.; Bertozzi, J.C.; Martinez, C.R.; Whitlow, J. Reassessment of the craniocervical junction: Normal values on CT. AJNR. Am. J. Neuroradiol. 2007, 28, 1819–1823. [Google Scholar] [CrossRef] [PubMed]
- Pang, D.; Nemzek, W.R.; Zovickian, J. Atlanto-occipital dislocation: Part 1--normal occipital condyle-C1 interval in 89 children. Neurosurgery 2007, 61, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.; Vasquez, L.; Tyroch, A.; Trier, T. Association of Atlanto-Occipital Dislocation, Retroclival Hematoma, and Hydrocephalus: Management and Survival in a Pediatric Patient. J. Neurol. Surg. Rep. 2017, 78, e46–e51. [Google Scholar] [CrossRef] [PubMed]
- Traynelis, V.C.; Marano, G.D.; Dunker, R.O.; Kaufman, H.H. Traumatic atlanto-occipital dislocation. Case report. J. Neurosurg. 1986, 65, 863–870. [Google Scholar] [CrossRef]
- Bellabarba, C.; Mirza, S.K.; West, G.A.; Mann, F.A.; Dailey, A.T.; Newell, D.W.; Chapman, J.R. Diagnosis and treatment of craniocervical dislocation in a series of 17 consecutive survivors during an 8-year period. J. Neurosurg. Spine 2006, 4, 429–440. [Google Scholar] [CrossRef] [PubMed]
- Horn, E.M.; Feiz-Erfan, I.; Lekovic, G.P.; Dickman, C.A.; Sonntag, V.K.H.; Theodore, N. Survivors of occipitoatlantal dislocation injuries: Imaging and clinical correlates. J. Neurosurg. Spine 2007, 6, 113–120. [Google Scholar] [CrossRef]
- Fisher, C.G.; Dipaola, C.P.; Ryken, T.C.; Bilsky, M.H.; Shaffrey, C.I.; Berven, S.H.; Harrop, J.S.; Fehlings, M.G.; Boriani, S.; Chou, D.; et al. A novel classification system for spinal instability in neoplastic disease: An evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine 2010, 35, E1221–E1229. [Google Scholar] [CrossRef]
- Crockard, H.A. The transoral approach to the base of the brain and upper cervical cord. Ann. R. Coll. Surg. Engl. 1985, 67, 321–325. [Google Scholar]
- Hsu, W.; Wolinsky, J.-P.; Gokaslan, Z.L.; Sciubba, D.M. Transoral Approaches to the Cervical Spine. Neurosurgery 2010, 66, A119–A125. [Google Scholar] [CrossRef]
- Menezes, A.H. Surgical approaches: Postoperative care and complications “transoral–transpalatopharyngeal approach to the craniocervical junction”. Child’s Nerv. Syst. 2008, 24, 1187–1193. [Google Scholar] [CrossRef]
- Youssef, A.S.; Sloan, A.E. Extended Transoral Approaches. Neurosurgery 2010, 66, A126–A134. [Google Scholar] [CrossRef] [PubMed]
- Youssef, A.S.; Guiot, B.; Black, K.; Sloan, A.E. Modifications of the transoral approach to the craniovertebral junction: Anatomic study and clinical correlations. Neurosurgery 2008, 62, 145–154. [Google Scholar] [CrossRef]
- Klionsky, D.J.; Abdelmohsen, K.; Abe, A.; Abedin, M.J.; Abeliovich, H.; Arozena, A.A.; Adachi, H.; Adams, C.M.; Adams, P.D.; Adeli, K.; et al. Guidelines for the use and interpretation of assays for monitoring autophagy (3rd edition). Autophagy 2016, 12, 1–222. [Google Scholar] [CrossRef] [PubMed]
- Perrini, P.; Benedetto, N.; Guidi, E.; Di Lorenzo, N. Transoral approach and its superior extensions to the craniovertebral junction malformations: Surgical strategies and results. Neurosurgery 2009, 64, 331–342, discussion 342. [Google Scholar] [CrossRef]
- Jones, D.C.; Hayter, J.P.; Vaughan, E.D.; Findlay, G.F. Oropharyngeal morbidity following transoral approaches to the upper cervical spine. Int. J. Oral Maxillofac. Surg. 1998, 27, 295–298. [Google Scholar] [CrossRef]
- La Corte, E.; Aldana, P.R. Endoscopic approach to the upper cervical spine and clivus: An anatomical study of the upper limits of the transoral corridor. Acta Neurochir. 2017, 159, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Visocchi, M.; Della Pepa, G.M.; Doglietto, F.; Esposito, G.; La Rocca, G.; Massimi, L. Video-assisted microsurgical transoral approach to the craniovertebral junction: Personal experience in childhood. Child’s Nerv. Syst. 2011, 27, 825–831. [Google Scholar] [CrossRef]
- Kassam, A.; Snyderman, C.H.; Mintz, A.; Gardner, P.; Carrau, R.L. Expanded endonasal approach: The rostrocaudal axis. Part I. Crista galli to the sella turcica. Neurosurg. Focus. 2005, 19, E3. [Google Scholar] [CrossRef]
- Kassam, A.; Snyderman, C.H.; Mintz, A.; Gardner, P.; Carrau, R.L. Expanded endonasal approach: The rostrocaudal axis. Part II. Posterior clinoids to the foramen magnum. Neurosurg. Focus. 2005, 19, E4. [Google Scholar] [CrossRef]
- La Corte, E.; Aldana, P.R.; Schiariti, M.; Maccari, A.; Ferroli, P. Endoscopic approaches to the craniovertebral junction. Acta Neurochir. 2014, 156, 293–295. [Google Scholar] [CrossRef]
- Kasemsiri, P.; Carrau, R.L.; Ditzel Filho, L.F.S.; Prevedello, D.M.; Otto, B.A.; Old, M.; De Lara, D.; Kassam, A.B. Advantages and limitations of endoscopic endonasal approaches to the skull base. World Neurosurg. 2014, 82, S12–S21. [Google Scholar] [CrossRef]
- Kassam, A.B.; Snyderman, C.; Gardner, P.; Carrau, R.; Spiro, R.; Sonntag, V.K.H.; Cappabianca, P.; Cavallo, L.M.; Jho, H.D. The expanded endonasal approach: A fully endoscopic transnasal approach and resection of the odontoid process: Technical case report. Neurosurgery 2005, 57, E213. [Google Scholar] [CrossRef]
- Gempt, J.; Lehmberg, J.; Meyer, B.; Stoffel, M. Endoscopic transnasal resection of the odontoid in a patient with severe brainstem compression. Acta Neurochir. 2010, 152, 559–560. [Google Scholar] [CrossRef]
- Gempt, J.; Lehmberg, J.; Grams, A.E.; Berends, L.; Meyer, B.; Stoffel, M. Endoscopic transnasal resection of the odontoid: Case series and clinical course. Eur. Spine J. 2011, 20, 661–666. [Google Scholar] [CrossRef]
- Lee, A.; Sommer, D.; Reddy, K.; Murty, N.; Gunnarsson, T. Endoscopic transnasal approach to the craniocervical junction. Skull Base 2010, 20, 199–202. [Google Scholar] [CrossRef]
- Nayak, J.V.; Gardner, P.A.; Vescan, A.D.; Carrau, R.L.; Kassam, A.B.; Snyderman, C.H. Experience with the expanded endonasal approach for resection of the odontoid process in rheumatoid disease. Am. J. Rhinol. 2007, 21, 601–606. [Google Scholar] [CrossRef]
- Gladi, M.; Iacoangeli, M.; Specchia, N.; Re, M.; Dobran, M.; Alvaro, L.; Moriconi, E.; Scerrati, M. Endoscopic transnasal odontoid resection to decompress the bulbo-medullary junction: A reliable anterior minimally invasive technique without posterior fusion. Eur. Spine J. 2012, 21 (Suppl. S1), 55–60. [Google Scholar] [CrossRef] [PubMed]
- van Abel, K.M.; Mallory, G.W.; Kasperbauer, J.L.; Moore, E.J.; Price, D.L.; O’Brien, E.K.; Olsen, K.D.; Krauss, W.E.; Clarke, M.J.; Jentoft, M.E.; et al. Transnasal odontoid resection: Is there an anatomic explanation for differing swallowing outcomes? Neurosurg. Focus 2014, 37, E16. [Google Scholar] [CrossRef] [PubMed]
- Aldana, P.R.; Naseri, I.; La Corte, E. The Naso-Axial Line. Oper. Neurosurg. 2012, 71, ons308–ons314. [Google Scholar] [CrossRef] [PubMed]
- La Corte, E.; Aldana, P.R.; Ferroli, P.; Greenfield, J.P.; Härtl, R.; Anand, V.K.; Schwartz, T.H. The rhinopalatine line as a reliable predictor of the inferior extent of endonasal odontoidectomies. Neurosurg. Focus 2015, 38, E16. [Google Scholar] [CrossRef] [PubMed]
- Messina, A.; Bruno, M.C.; Decq, P.; Coste, A.; Cavallo, L.M.; De Divittis, E.; Cappabianca, P.; Tschabitscher, M. Pure endoscopic endonasal odontoidectomy: Anatomical study. Neurosurg. Rev. 2007, 30, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.H.; Ganesan, D.; Prepageran, N.; Waran, V. A minimally invasive endoscopic transnasal approach to the craniovertebral junction in the paediatric population. Eur. Arch. Otorhinolaryngol. 2014, 271, 3101–3105. [Google Scholar] [CrossRef] [PubMed]
- Tanriverdi, O.; Tugcu, B.; Gunaldi, O.; Baydin, S.S.; Demirgil, B.T.; Sam, B.; Kucukyuruk, B.; Tanriover, N. The selective odontoidectomy: Endoscopic endonasal approach to the craniocervical junction. J. Craniofac. Surg. 2014, 25, 1482–1487. [Google Scholar] [CrossRef] [PubMed]
- Mendes, G.A.C.; Dickman, C.A.; Rodriguez-Martinez, N.G.; Kalb, S.; Crawford, N.R.; Sonntag, V.K.H.; Preul, M.C.; Little, A.S. Endoscopic endonasal atlantoaxial transarticular screw fixation technique: An anatomical feasibility and biomechanical study. J. Neurosurg. Spine 2015, 22, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Forbes, J.A.; Kumar, C.; McGough, D.; Palmisciano, P.; Hussein, A.E.; Zhebrykov, D.; Gibson, J.; Andaluz, N.; Sedaghat, A.R.; Prestigiacomo, C.J.; et al. Anterior occipital condyle screw placement through the endonasal corridor: Proof of concept study with cadaveric analysis. Eur. Spine J. 2023, 32, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Baldassarre, B.; DI Perna, G.; Portonero, I.; Penner, F.; Cofano, F.; Marco, R.; Marengo, N.; Garbossa, D.; Pecorari, G.; Zenga, F. Craniovertebral junction chordomas: Case series and strategies to overcome the surgical challenge. J. Craniovertebral Junction Spine 2021, 12, 420–431. [Google Scholar]
- Perez-Orribo, L.; Little, A.S.; Lefevre, R.D.; Reyes, P.R.; Newcomb, A.G.U.S.; Prevedello, D.M.; Roldan, H.; Nakaji, P.; Dickman, C.A.; Crawford, N.R. Biomechanical evaluation of the craniovertebral junction after anterior unilateral condylectomy: Implications for endoscopic endonasal approaches to the cranial base. Neurosurgery 2013, 72, 1021–1029. [Google Scholar] [CrossRef]
- Kooshkabadi, A.; Choi, P.A.; Koutourousiou, M.; Snyderman, C.H.; Wang, E.W.; Fernandez-Miranda, J.C.; Gardner, P.A. Atlanto-occipital Instability Following Endoscopic Endonasal Approach for Lower Clival Lesions: Experience with 212 Cases. Neurosurgery 2015, 77, 888–897. [Google Scholar] [CrossRef]
- Iacoangeli, M.; Gladi, M.; Alvaro, L.; Di Rienzo, A.; Specchia, N.; Scerrati, M. Endoscopic endonasal odontoidectomy with anterior C1 arch preservation in elderly patients affected by rheumatoid arthritis. Spine J. 2013, 13, 542–548. [Google Scholar] [CrossRef]
- Re, M.; Iacoangeli, M.; Di Somma, L.; Alvaro, L.; Nasi, D.; Magliulo, G.; Gioacchini, F.M.; Fradeani, D.; Scerrati, M. Endoscopic endonasal approach to the craniocervical junction: The importance of anterior C1 arch preservation or its reconstruction. Acta Otorhinolaryngol. Ital. 2016, 36, 107–118. [Google Scholar] [CrossRef]
- Palmisciano, P.; Al Fawares, Y.; Woodhouse, C.; Yang, G.; Xu, A.; D’Herbemont, S.; Hoang, S.; McGuire, J.L.; Phillips, K.M.; Cheng, J.; et al. The Impact of C1 Anterior Arch Preservation on Spine Stability after Odontoidectomy: Systematic Review and Meta-Analysis. World Neurosurg. 2022, 167, 165–175.e2. [Google Scholar] [CrossRef]
- Fridley, J.; Gokaslan, Z.L. The evolution of surgical management for vertebral column tumors. J. Neurosurg. Spine 2019, 30, 417–423. [Google Scholar] [CrossRef]
- Fridley, J.; Oyelese, A.; Gokaslan, Z. Primary osseous and metastatic neoplasms of the CVJ. In Surgery of the Cranio-Vertebral Junction; Tessitore, E., Dehdashti, A.R., Schonauer, C., Thomé, C., Eds.; Springer Nature Switzerland AG: Cham, Switzerland, 2020; pp. 353–365. [Google Scholar] [CrossRef]
- Boriani, S.; Weinstein, J.N.; Biagini, R. Primary bone tumors of the spine. Terminology and surgical staging. Spine 1997, 22, 1036–1044. [Google Scholar] [CrossRef]
- Lau, C.S.M.; Mahendraraj, K.; Ward, A.; Chamberlain, R.S. Pediatric Chordomas: A Population-Based Clinical Outcome Study Involving 86 Patients from the Surveillance, Epidemiology, and End Result (SEER) Database (1973–2011). Pediatr. Neurosurg. 2016, 51, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Refai, D.; Shin, J.H.; Iannotti, C.; Benzel, E.C. Dorsal approaches to intradural extramedullary tumors of the craniovertebral junction. J. Craniovertebral Junction Spine 2010, 1, 49–54. [Google Scholar]
- Laufer, I.; Rubin, D.G.; Lis, E.; Cox, B.W.; Stubblefield, M.D.; Yamada, Y.; Bilsky, M.H. The NOMS framework: Approach to the treatment of spinal metastatic tumors. Oncologist 2013, 18, 744–751. [Google Scholar] [CrossRef] [PubMed]
- Denis, F. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine 1983, 8, 817–831. [Google Scholar] [CrossRef] [PubMed]
- Sciubba, D.M.; Chaichana, K.L.; Woodworth, G.F.; McGirt, M.J.; Gokaslan, Z.L.; Jallo, G.I. Factors associated with cervical instability requiring fusion after cervical laminectomy for intradural tumor resection. J. Neurosurg. Spine 2008, 8, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Katsumi, Y.; Honma, T.; Nakamura, T. Analysis of cervical instability resulting from laminectomies for removal of spinal cord tumor. Spine 1989, 14, 1171–1176. [Google Scholar] [CrossRef]
- Zdeblick, T.A.; Abitbol, J.J.; Kunz, D.N.; McCabe, R.P.; Garfin, S. Cervical stability after sequential capsule resection. Spine 1993, 18, 2005–2008. [Google Scholar] [CrossRef]
- Jiang, H.; He, J.; Zhan, X.; He, M.; Zong, S.; Xiao, Z. Occipito-cervical fusion following gross total resection for the treatment of spinal extramedullary tumors in craniocervical junction: A retrospective case series. World J. Surg. Oncol. 2015, 13, 279. [Google Scholar] [CrossRef]
- Tatter, C.; Fletcher-Sandersjöö, A.; Persson, O.; Burström, G.; Grane, P.; Edström, E.; Elmi-Terander, A. Incidence and predictors of kyphotic deformity following resection of cervical intradural tumors in adults: A population-based cohort study. Acta Neurochir. 2020, 162, 2905–2913. [Google Scholar] [CrossRef] [PubMed]
- Noh, S.H.; Takahashi, T.; Inoue, T.; Park, S.M.; Hanakita, J.; Minami, M.; Kanematsu, R.; Shimauchi-Ohtaki, H.; Ha, Y. Postoperative spinal deformity and instability after cervical spinal cord tumor resection in adults: A systematic review and meta-analysis. J. Clin. Neurosci. 2022, 100, 148–154. [Google Scholar] [CrossRef]
- Avila, M.J.; Walter, C.M.; Skoch, J.; Abbasifard, S.; Patel, A.S.; Sattarov, K.; Baaj, A.A. Fusion after intradural spine tumor resection in adults: A review of evidence and practices. Clin. Neurol. Neurosurg. 2015, 138, 169–173. [Google Scholar] [CrossRef] [PubMed]
- La Corte, E.; Broggi, M.; Bosio, L.; Danesi, G.; Ferroli, P. Tailored surgical strategy in clival chordomas: An extraordinary selection bias that limits approach comparison. J. Neurosurg. Sci. 2018, 62, 519–521. [Google Scholar] [CrossRef] [PubMed]
- Mazur, M.D.; Couldwell, W.T.; Cutler, A.; Shah, L.M.; Brodke, D.S.; Bachus, K.; Dailey, A.T. Occipitocervical Instability After Far-Lateral Transcondylar Surgery: A Biomechanical Analysis. Neurosurgery 2017, 80, 140–145. [Google Scholar] [CrossRef]
- Vishteh, A.G.; Crawford, N.R.; Melton, M.S.; Spetzler, R.F.; Sonntag, V.K.H.; Dickman, C.A. Stability of the craniovertebral junction after unilateral occipital condyle resection: A biomechanical study. J. Neurosurg. 1999, 90, 91–98. [Google Scholar] [CrossRef]
- Kshettry, V.R.; Healy, A.T.; Colbrunn, R.; Beckler, D.T.; Benzel, E.C.; Recinos, P.F. Biomechanical evaluation of the craniovertebral junction after unilateral joint-sparing condylectomy: Implications for the far lateral approach revisited. J. Neurosurg. 2017, 127, 829–836. [Google Scholar] [CrossRef]
- Shiban, E.; Török, E.; Wostrack, M.; Meyer, B.; Lehmberg, J. The far-lateral approach: Destruction of the condyle does not necessarily result in clinically evident craniovertebral junction instability. J. Neurosurg. 2016, 125, 196–201. [Google Scholar] [CrossRef]
- Alalade, A.F.; Ogando-Rivas, E.; Forbes, J.; Ottenhausen, M.; Uribe-Cardenas, R.; Hussain, I.; Nair, P.; Lehner, K.; Singh, H.; Kacker, A.; et al. A Dual Approach for the Management of Complex Craniovertebral Junction Abnormalities: Endoscopic Endonasal Odontoidectomy and Posterior Decompression with Fusion. World Neurosurg. X 2019, 2, 100010. [Google Scholar] [CrossRef]
- Champagne, P.O.; Voormolen, E.H.; Mammar, H.; Bernat, A.L.; Krichen, W.; Penet, N.; Froelich, S. Delayed Instrumentation Following Removal of Cranio-Vertebral Junction Chordomas: A Technical Note. J. Neurol. Surg. B. Skull Base 2020, 81, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Li, L.; Wang, P.; Yin, Y.; Bu, B.; Zhou, D. Intraoperative computed tomography with an integrated navigation system in stabilization surgery for complex craniovertebral junction malformation. J. Spinal Disord. Tech. 2014, 27, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Marengo, N.; Di Perna, G.; Baldassarre, B.M.; Cofano, F.; De Marco, R.; Zeppa, P.; Petrone, S.; Ajello, M.; Garbossa, D.; Zenga, F. 3D-printed guides for cervical pedicle screw placement in primary spine tumor: Case report and technical description. Front. Surg. 2022, 9, 1011846. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surgical Approach | Advantages | Disadvantages |
|---|---|---|
| Transoral | Provide direct anterior access to the CJV from the lower portion of the clivus to C3 Furnish a safe trajectory for extradural midline lesions, avoiding traction and/or manipulation of critical anatomical structures (e.g., cranial nerves, vertebral arteries, brainstem) Permit an excellent decompression of the ventral medulla and upper cervical spinal cord, especially in irreducible ventral pathology | High risk of morbidity including swallowing and respiratory complication, CSF leakage and meningitis in case of intradural pathology Invasive and destructive approach for the surrounding structures (e.g., soft palate and oropharyngeal mucosa or bony structures in case a wider exposure is needed); this instance can be reduced with the endoscopic transoral approach. |
| Endoscopic Endonasal | Provide a direct anterior access to the CJV from the clivus to the odontoid process Furnish a safe trajectory for extradural midline lesions, avoiding traction and/or manipulation of critical anatomical structures (e.g., cranial nerves, vertebral arteries, brainstem) Minimally invasive approach that reduces the mortality and morbidity related to the standard transoral approach | Less exposure in the sagittal plane, especially below the axis, compared to the transoral approach Risk of CSF leakage and infection although less frequent than with the transoral approach |
| Posterior | Provide a safer surgical corridor for intradural tumors compared to anterior approaches in terms of CSF leakage and infections Extreme versatile approach to treat several types of dorsal lesions (e.g., meningiomas, schwannomas, intramedullary tumors) Capability to perform posterior fixation procedure within the same surgical time | Risk of neurovascular injury during dissection procedures Risk of postoperative cervical pain Limited access for the resection of lesions extending into intradural and extradural compartments |
| Posterolateral | Provide a safer surgical corridor for intradural tumors compared to anterior approaches in terms of CSF leakage and infections Extreme versatile approach to treat several types of dorsal lesions (e.g., meningiomas, schwannomas, intramedullary tumors) Capability to perform posterior fixation procedure within the same surgical time Allows the resection of lesion extending into intradural and extradural compartments | Higher risk of neurovascular injury during surgical exposure compared to posterior approach More challenging compared to the posterior approach, requires adequate surgical expertise |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ottenhausen, M.; Greco, E.; Bertolini, G.; Gerosa, A.; Ippolito, S.; Middlebrooks, E.H.; Serrao, G.; Bruzzone, M.G.; Costa, F.; Ferroli, P.; et al. Craniovertebral Junction Instability after Oncological Resection: A Narrative Review. Diagnostics 2023, 13, 1502. https://doi.org/10.3390/diagnostics13081502
Ottenhausen M, Greco E, Bertolini G, Gerosa A, Ippolito S, Middlebrooks EH, Serrao G, Bruzzone MG, Costa F, Ferroli P, et al. Craniovertebral Junction Instability after Oncological Resection: A Narrative Review. Diagnostics. 2023; 13(8):1502. https://doi.org/10.3390/diagnostics13081502
Chicago/Turabian StyleOttenhausen, Malte, Elena Greco, Giacomo Bertolini, Andrea Gerosa, Salvatore Ippolito, Erik H. Middlebrooks, Graziano Serrao, Maria Grazia Bruzzone, Francesco Costa, Paolo Ferroli, and et al. 2023. "Craniovertebral Junction Instability after Oncological Resection: A Narrative Review" Diagnostics 13, no. 8: 1502. https://doi.org/10.3390/diagnostics13081502