
Radiofrequency Ablation in Vertebral Body Metastasis with and without Percutaneous Cement Augmentation: A Systematic Review Addressing the Need for SPINE Stability Evaluation
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
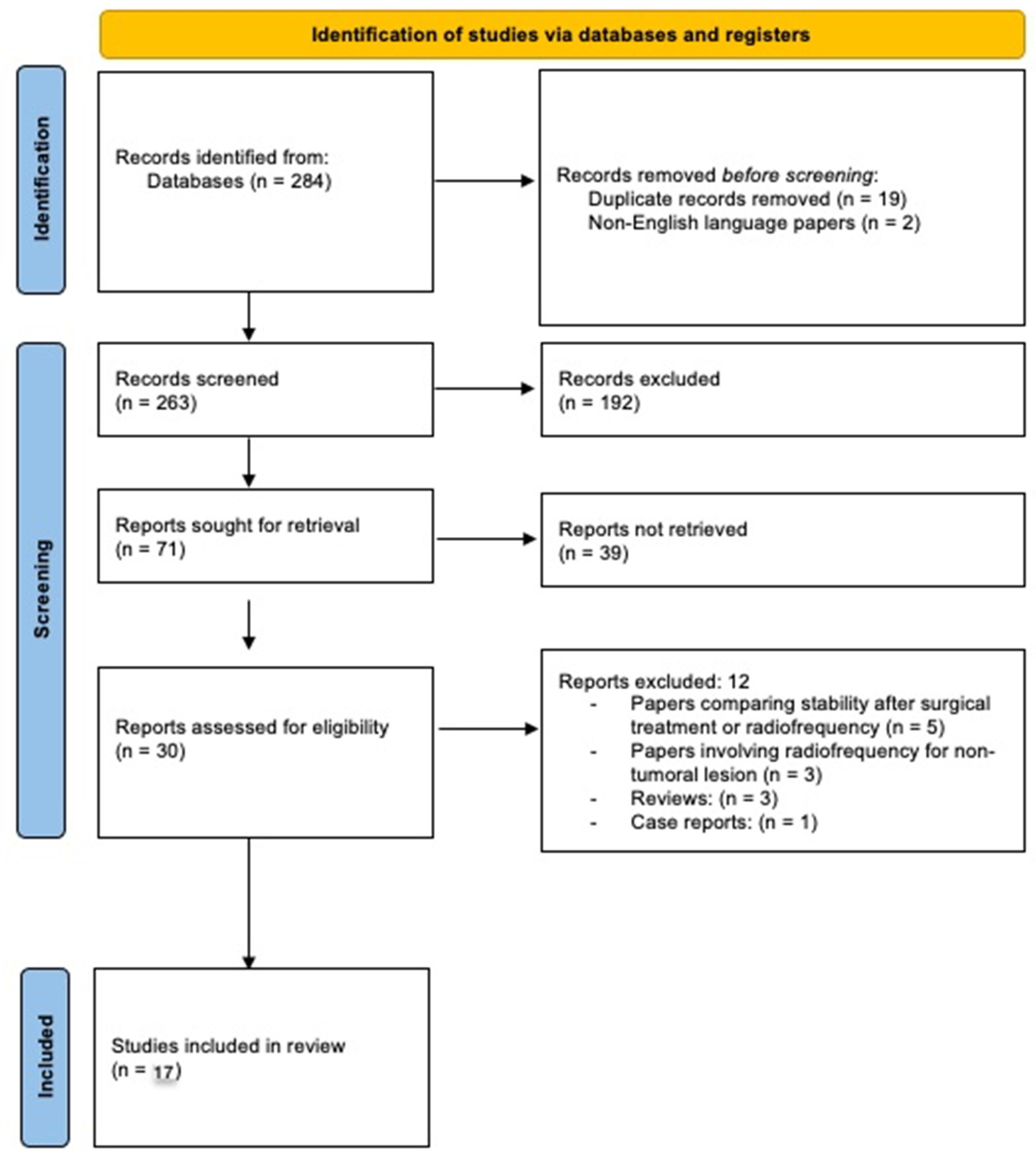
3. Results
Limitations of the Study
4. Discussion
4.1. Overview on Non-RFA Therapeutic Strategies
4.2. Radiofrequency Ablation
4.3. Cement Augmentation Techniques
4.4. Combination of Ablative and Cement Augmentation Treatments and Spine Stability
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Murali, N.; Turmezei, T.; Bhatti, S.; Patel, P.; Marshall, T.; Smith, T. What is the effectiveness of radiofrequency ablation in the management of patients with spinal metastases? A systematic review and meta-analysis. J. Orthop. Surg. Res. 2021, 16, 659. [Google Scholar] [CrossRef] [PubMed]
- Giammalva, G.R.; Costanzo, R.; Paolini, F.; Benigno, U.E.; Porzio, M.; Brunasso, L.; Basile, L.; Gulì, C.; Pino, M.A.; Gerardi, R.M.; et al. Management of Spinal Bone Metastases with Radiofrequency Ablation, Vertebral Reinforcement and Transpedicular Fixation: A Retrospective Single-Center Case Series. Front. Oncol. 2022, 11, 5896. [Google Scholar] [CrossRef]
- Sayed, D.; Jacobs, D.; Sowder, T.; Haines, D.; Orr, W. Prospective Evaluation Spinal Radiofrequency Ablation Combined with Cement Augmentation for Painful Spinal Vertebral Metastasis: A Single-Center Prospective Study. Available online: http://www.painphysicianjournal.com (accessed on 1 January 2022).
- Arrigoni, F.; de Cataldo, C.; Bruno, F.; Palumbo, P.; Zugaro, L.; di Staso, M.; Gravina, G.L.; Barile, A.; Masciocchi, C. Ablation, consolidation and radiotherapy for the management of metastatic lesions of the spine: Impact on the quality of life in a mid-term clinical and diagnostic follow-up in a pilot study. Med. Oncol. 2020, 37, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Masala, S.; Roselli, M.; Massari, F.; Fiori, R.; Ursone, A.; Fossile, E.; Laudisi, A.; Simonetti, G. Radiofrequency Heat Ablation and Vertebroplasty in the Treatment of Neoplastic Vertebral Body Fractures. Anticancer Res. 2004, 24, 3129–3134. [Google Scholar] [PubMed]
- Proschek, D.; Kurth, A.; Proschek, P.; Vogl, T.J.; Mack, M.G. Prospective Pilot-study of Combined Bipolar Radiofrequency Ablation and Application of Bone Cement in Bone Metastases. Anticancer Res. 2009, 29, 2787–2792. [Google Scholar]
- Georgy, B.A. Bone cement deposition patterns with plasma-mediated radio-frequency ablation and cement augmentation for advanced metastatic spine lesions. Am. J. Neuroradiol. 2009, 30, 1197–1202. [Google Scholar] [CrossRef]
- Bagla, S.; Sayed, D.; Smirniotopoulos, J.; Brower, J.; Neal Rutledge, J.; Dick, B.; Carlisle, J.; Lekht, I.; Georgy, B. Multicenter Prospective Clinical Series Evaluating Radiofrequency Ablation in the Treatment of Painful Spine Metastases. Cardiovasc. Interv. Radiol. 2016, 39, 1289–1297. [Google Scholar] [CrossRef]
- He, Y.; Han, S.; Wu, C.; Ge, F.; Wang, J. Comparison of the postoperative pain change and spinal stenosis rate between percutaneous vertebroplasty combined with radiofrequency ablation and with 125I particle implantation in the treatment of metastatic spinal cord compression: A retrospective study. J. Interv. Med. 2021, 4, 197–202. [Google Scholar] [CrossRef]
- Lane, M.D.; Le, H.B.Q.; Lee, S.; Young, C.; Heran, M.K.S.; Badii, M.; Clarkson, P.W.; Munk, P.L. Combination radiofrequency ablation and cementoplasty for palliative treatment of painful neoplastic bone metastasis: Experience with 53 treated lesions in 36 patients. Skelet. Radiol. 2011, 40, 25–32. [Google Scholar] [CrossRef]
- Lu, C.-W.; Shao, J.; Wu, Y.-G.; Wang, C.; Wu, J.-H.; Lv, R.-X.; Ding, M.-C.; Shi, Z.-C.; Mao, N.-F. Which Combination Treatment Is Better for Spinal Metastasis, Percutaneous Vertebroplasty with Radiofrequency Ablation, 125 I Seed, Zoledronic Acid, or Radiotherapy? Am. J. Ther. 2017, 26, 1–7. Available online: http://www.americantherapeutics.com (accessed on 1 January 2022).
- Lv, N.; Geng, R.; Ling, F.; Zhou, Z.; Liu, M. Clinical efficacy and safety of bone cement combined with radiofrequency ablation in the treatment of spinal metastases. BMC Neurol. 2020, 20, 418. [Google Scholar] [CrossRef] [PubMed]
- Maugeri, R.; Graziano, F.; Basile, L.; Gulì, C.; Giugno, A.; Giammalva, G.R.; Visocchi, M.; Iacopino, D.G. Reconstruction of vertebral body after radiofrequency ablation and augmentation in dorsolumbar metastatic vertebral fracture: Analysis of clinical and radiological outcome in a clinical series of 18 patients. In Acta Neurochirurgica, Supplementum; Springer: Wien, Austria, 2017; Volume 124, pp. 81–86. [Google Scholar] [CrossRef]
- Pezeshki, P.S.; Davidson, S.; Murphy, K.; McCann, C.; Slodkowska, E.; Sherar, M.; Yee, A.J.; Whyne, C.M. Comparison of the effect of two different bone-targeted radiofrequency ablation (RFA) systems alone and in combination with percutaneous vertebroplasty (PVP) on the biomechanical stability of the metastatic spine. Eur. Spine J. 2016, 25, 3990–3996. [Google Scholar] [CrossRef]
- Reyes, M.; Georgy, M.; Brook, L.; Ortiz, O.; Brook, A.; Agarwal, V.; Muto, M.; Manfre, L.; Marcia, S.; Georgy, B.A. Multicenter clinical and imaging evaluation of targeted radiofrequency ablation (t-RFA) and cement augmentation of neoplastic vertebral lesions. J. NeuroInterventional Surg. 2018, 10, 176–182. [Google Scholar] [CrossRef]
- Shawky Abdelgawaad, A.; Ezzati, A.; Krajnovic, B.; Seyed-Emadaldin, S.; Abdelrahman, H. Radiofrequency ablation and balloon kyphoplasty for palliation of painful spinal metastases. Eur. Spine J. 2021, 30, 2874–2880. [Google Scholar] [CrossRef] [PubMed]
- Wallace, A.N.; Greenwood, T.J.; Jennings, J.W. Radiofrequency ablation and vertebral augmentation for palliation of painful spinal metastases. J. Neuro-Oncol. 2015, 124, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.L.; He, X.J.; Li, H.P.; Zang, Q.J.; Wang, G.Y. Image-guided minimally invasive percutaneous treatment of spinal metastasis. Exp. Ther. Med. 2017, 13, 705–709. [Google Scholar] [CrossRef] [Green Version]
- Cofano, F.; di Perna, G.; Marengo, N.; Ajello, M.; Melcarne, A.; Zenga, F.; Garbossa, D. Transpedicular 3D endoscope-assisted thoracic corpectomy for separation surgery in spinal metastases: Feasibility of the technique and preliminary results of a promising experience. Neurosurg. Rev. 2020, 43, 351–360. [Google Scholar] [CrossRef]
- Cofano, F.; di Perna, G.; Monticelli, M.; Marengo, N.; Ajello, M.; Mammi, M.; Vercelli, G.; Petrone, S.; Tartara, F.; Zenga, F.; et al. Carbon fiber reinforced vs titanium implants for fixation in spinal metastases: A comparative clinical study about safety and effectiveness of the new “carbon-strategy”. J. Clin. Neurosci. 2020, 75, 106–111. [Google Scholar] [CrossRef]
- Cofano, F.; di Perna, G.; Alberti, A.; Baldassarre, B.M.; Ajello, M.; Marengo, N.; Tartara, F.; Zenga, F.; Garbossa, D. Neurological outcomes after surgery for spinal metastases in symptomatic patients: Does the type of decompression play a role? A comparison between different strategies in a 10-year experience. J. Bone Oncol. 2021, 26, 100340. [Google Scholar] [CrossRef]
- di Perna, G.; Cofano, F.; Mantovani, C.; Badellino, S.; Marengo, N.; Ajello, M.; Comite, L.M.; Palmieri, G.; Tartara, F.; Zenga, F.; et al. Separation surgery for metastatic epidural spinal cord compression: A qualitative review. J. Bone Oncol. 2020, 25, 100320. [Google Scholar] [CrossRef]
- Yang, H.L.; Sun, Z.Y.; Wu, G.Z.; Chen, K.W.; Gu, Y.; Qian, Z.L. Do vertebroplasty and kyphoplasty have an antitumoral effect? Med. Hypotheses 2011, 76, 145–146. [Google Scholar] [CrossRef] [PubMed]
- Bouza, C.; López-Cuadrado, T.; Cediel, P.; Saz-Parkinson, Z.; Amate, J.M. Balloon kyphoplasty in malignant spinal fractures: A systematic review and meta-analysis. BMC Palliat. Care 2009, 8, 12. [Google Scholar] [CrossRef] [Green Version]
- Fox, S.; Spiess, M.; Hnenny, L.; Fourney, D.R. Spinal Instability Neoplastic Score (SINS): Reliability Among Spine Fellows and Resident Physicians in Orthopedic Surgery and Neurosurgery. Glob. Spine J. 2017, 7, 744–748. [Google Scholar] [CrossRef]
- Cofano, F.; di Perna, G.; Zenga, F.; Ducati, A.; Baldassarre, B.; Ajello, M.; Marengo, N.; Ceroni, L.; Lanotte, M.; Garbossa, D. The Neurology-Stability-Epidural compression assessment: A new score to establish the need for surgery in spinal metastases. Clin. Neurol. Neurosurg. 2020, 195, 105896. [Google Scholar] [CrossRef]
- Fisher, C.G.; DiPaola, C.P.; Ryken, T.C.; Bilsky, M.H.; Shaffrey, C.I.; Berven, S.H.; Harrop, J.; Fehlings, M.; Boriani, S.; Chou, D.; et al. A Novel Classification System for Spinal Instability in Neoplastic Disease: An Evidence-Based Approach and Expert Consensus from the Spine Oncology Study Group. Spine 2010, 35, E1221–E1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fourney, D.R.; Frangou, E.M.; Ryken, T.C.; DiPaola, C.P.; Shaffrey, C.I.; Berven, S.H.; Bilsky, M.H.; Harrop, J.S.; Fehlings, M.G.; Boriani, S.; et al. Spinal Instability Neoplastic Score: An Analysis of Reliability and Validity from the Spine Oncology Study Group. J. Clin Oncol. 2011, 29, 3072–3077. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Authors and Year | Study Location | Type of Study | No. of Patients (No. of Lesions) | Type of Procedure | Inclusion Criteria | Exclusion Criteria | Study Endpoints |
|---|---|---|---|---|---|---|---|
| Sayed et al., 2019 [3] | USA | Single-center prospective study | 30 (34) | RFA (2) vs. RFA + PVP (28) | At least one painful thoracic or lumbar metastasis, age at least 18 years | Vertebral metastatic disease in the cervical spine, spinal cord compression from posterior tumor extension | Evaluation of pain reduction (NRS-11); improvement of quality of life (FACT-G7) |
| Masala et al., 2004 [5] | Italy | Single-center experience | 3 | RFA + PVP | Tokuhashi prognostic scoring system < 6 | Osteoblastic tumors, retropulsion fractures, spread of tumor within the epidural space, local infection, coagulative disorders, involvement or missing integrity of pedicles or joint facets | Evaluation of pain reduction (VAS) |
| Proschek et al., 2009 [6] | Germany | Pilot study | 16 | RFA (8) vs. RFA + PVP (8) | Mechanical back pain, absence of neurological deficit | Vertebral fractures, radicular neurological symptoms, coagulation disorders, local infection | Evaluation of pain reduction (VAS); improvement of quality of life (Oswestry Disability Questionnaire) |
| Arrigoni et al., 2020 [4] | Italy | Pilot study | 11 | RFA, microwave ablation (MWA), cryoablation (CA) + PVP + adjuvant RT | At least one vertebral osteolytic metastatic lesion, disabling refractory back pain, KPS > 70 | Asymptomatic lesions, spinal osteoblastic metastatic lesions without risk of fracture, platelets count < 50,000, local or systemic infection | Stability of the vertebral lesion 6 months after treatment (RECIST criteria); improvement of pain (VAS); improvement of quality of life (ECOG-PS) |
| Georgy et al., 2009 [7] | USA | Retrospective study | 37 | pmRFA + PVP | Painful vertebral metastasis associated with at least one of the following criteria: cortical disruption, epidural extension, paraspinal extension | Painful vertebral metastasis not associated with at least one of the following criteria: cortical disruption, epidural extension, paraspinal extension | Evaluation of cement disposition pattern (standard PACS System); evaluation of pain reduction (VAS) |
| Bagla et al., 2016 [8] | USA | Single-arm prospective multicenter study | 50 | RFA + PVP | Painful vertebral bone metastasis in at least one thoraco-lumbar vertebra, age at least 18 years, pain concordant to the metastatic lesion site | Painful vertebral bone metastasis in cervical spine, posterior tumor extension with cord compression | Improvement of pain (NPRS); improvement of back-related disability (MODI); improvement of quality of life (FACT-G7, FACT-BP) |
| Giammalva et al., 2022 [2] | Italy | Retrospective study | 54 | Concomitant RFA + PVP + posterior open/percutaneous transpedicular fixation | Karnofsky score ≥ 60, unremitting thoraco-lumbar pain (VAS score ≥ 5), osteolytic lesion on neuroimaging, unresecable tumors (according to Tokuhashi score), intractable pain with chemotherapy, radiation therapy and refractory to analgesic drugs | Karnofsky score < 60, mild thoraco-lumbar pain (VAS < 5), osteoblastic tumors on neuroimaging, general contraindications for surgery (infection, allergy, bleeding diseases), intradural and intramedullary tumors and neurological impairments caused by spinal metastasis itself | Evaluation of pain improvement (VAS); bone distribution of cement (Saliou filling score) |
| He et al., 2021 [9] | China | Retrospective study | 40 | PVP + RFA (19) vs. PVP + 123I (21) | Clear history and pathological diagnosis of malignant tumors; improved CT and enhanced MRI findings of the spine before the operation; narrowing of the spinal canal and epidural compression in the local spinal cord visible on sagittal MRI scans before surgery; osteolytic bone destruction of spinal metastasis; one or several clinical manifestations of the following secondary spinal cord injury: (a) local or radiation pain and progressive aggravation; (b) sensory function damage and progressive aggravation; (c) motor function damage and progressive aggravation; (d) sphincter function abnormality; and (e) involvement of < 4 vertebral body segments in the tumors | Predicted survival time of < 3 months; primary spinal tumors, such as multiple myeloma; spinal infectious diseases, such as spinal tuberculosis and other bacterial infections; severe cardiovascular and cerebrovascular diseases, respiratory failure, liver and kidney failure, and inability to tolerate surgery; coagulation dysfunction; severe skin infection in the operation area | Evaluation of pain improvement (VAS); evaluation of spinal stenosis rate on MRI (SSR) |
| Lane et al., 2010 [10] | Canada | Retrospective study | 36 (53) | RFA + PVP | Focal pain clinically localized to a region with imaging confirming the presence of bony tumor involvement; pain partially or totally refractory to analgesic medications; unacceptable side-effects of additional medication; at least 18 years of age; life expectancy of greater than 1 month. Bony metastases with adjacent soft tissue and/or posterior aspect of vertebral body tumor involvement were not excluded. | Extensive pathological destruction of the posterior wall of the vertebral body with > 40% reduction in the antero-posterior canal dimension; purely osteosclerotic metastases; patients with INRs > 1.3; platelet counts < 50,000; and any local or systemic infection | Evaluation of pain improvement (VAS) |
| Lu et al., 2017 [11] | China | Retrospective study | 169 | PVP + RFA (51) PVP + 123I (49) PVP + zoledronic acid (38) PVP + RT (31) | Not specified | Not specified | Evaluation of pain improvement (VAS; WHO Pain Relief scale); evaluation of motor dysfunction (ODI) |
| Lv et al., 2020 [12] | China | Retrospective study | 87 (125) Group A: 35 (47) Group B: 52 (78) | PVP + RFA (Group A) vs. PVP (Group B) | Definite diagnosis of spinal metastatic cancer (pathological or cytological diagnosis); structurally intact posterior margin of the vertebral body without nerve root symptoms; thoracic and lumbar vertebral body lesions, which are mainly lesions of osteolytic destruction or mixed destruction; willingness to undergo the proposed procedure (signed informed consent) and relatively good treatment compliance | Incomplete structure of the posterior margin of the vertebral cortex or infiltration of tumor into the dura, accompanied by nerve root symptoms; osteogenic lesions; terminal patients; severe cardiopulmonary disease or coagulation dysfunction | Evaluation of pain and function improvement (VAS, ODI); anterior and intermediate vertebral body height; bone cement leakage; local tumor recurrence |
| Maugeri et al., 2017 [13] | Italy | Retrospective study | 18 | RFA + PVP + posterior transpedicular fixation | Unresecable tumors, according to Tokuhashi score; Karnofsky score > 60; osteolytic lesion on neuroimaging; VAS > 5; intractable pain with CT, RT or other treatments | General contraindications for surgery (infection, allergy, bleeding diseases); poor general condition (Karnofsky score < 60); osteoblastic tumors on neuroimaging; VAS < 5; spinal cord or nerve compression or intradural and intramedullary tumors | Evaluation of pain improvement (VAS); bone distribution of polymethylmethacrylate (Saliou filling score) |
| Pezeshki et al., 2016 [14] | Canada | Cadaver simulation study | 6 (cadaver specimens) | RFA; RFA + PVP | / | / | Evaluation of the biomechanics of the spine after RFA + PVP (load-induced canal narrowing, LICN) |
| Reyes et al., 2017 [15] | USA; Italy | Retrospective multicenter study | 49 (72) | RFA + PVP | Not specified | Not specified | Evaluation of pain and function improvement (VAS; ODI); evaluation of local tumor recurrence (contrast-enhanced MRI, FDG-PET) |
| Abdelgawaad et al., 2021 [16] | Germany; Egypt | Retrospective study | 60 (75) | RFA + BKP + adjuvant RT | Painful osteolytic spinal metastases refractory to analgesics; absence of neurologic deficit or cord compression; stable posterior column according to the Spinal Instability Neoplastic Score (SINS). Posterior vertebral wall defects were not considered contraindications. | Entirely osteoblastic lesions; lesions associated with marked spinal instability requiring spinal instrumentation surgery | Evaluation of pain improvement (VAS) |
| Wallace et al., 2015 [17] | USA | Retrospective study | 72 (110) | RFA + PVP (95%) ± adjuvant RT | Not specified | Entirely osteoblastic lesions; lesions associated with pathologic compression fracture with spinal instability or causing metastatic spinal cord compression. Tumor within 1 cm of the spinal cord or nerves was not a contraindication for RFA. | Evaluation of pain improvement (NRS-11) |
| Yang et al., 2017 [18] | China | Retrospective study | 42 (52) | RFA + PVP (25); PVP alone (17) | Evident history of the primary tumor, or diagnosis by aspiration biopsy; experienced sudden or persistent pain in the neck, chest, back, or waist; complete clinical record available | Not specified | Evaluation of pain improvement (VAS); evaluation of neurological status (Frankel classification) |
| Authors and Year | Mean Age (Range) | Type of Anesthesia | Procedure Modality | Post-Procedural Imaging | Average Duration of Procedure | Post-Procedure Complications | Post-Procedure Follow-Up Duration | Local Recurrence During Follow-Up |
|---|---|---|---|---|---|---|---|---|
| Sayed et al., 2019 [3] | 62.9 ± 13.45 | Conscious sedation; local anesthesia | CT/fluoroscopy-guided | Non-enhanced MRI/CT scan | 9.56 min | None | 3 days, 1 week, 1 month, 3 months | No local recurrence |
| Masala et al., 2004 [5] | 72.3 (63–82) | Conscious sedation; local anesthesia | CT/fluoroscopy-guided | Non-enhanced CT scan | 35–45 min | None | None | Not specified |
| Proschek et al., 2009 [6] | 59.5 (52–69) | Conscious sedation; local anesthesia | CT/fluoroscopy-guided | Non-enhanced CT scan | Not specified | None | Average of 20.4 months (range 8–36 months) | No local recurrence |
| Arrigoni et al., 2020 [4] | 62.9 (49–76) | Conscious sedation; local or spinal anesthesia | CT/fluoroscopy-guided | Non-enhanced CT scan | Not specified | None | Every 6 months Average 18 months (range 6–48 months) | Enlargement of lesion’s volume and vertebral fracture at 6 months follow-up in 2 patients |
| Bagla et al., 2016 [8] | 61 (23–83) | Conscious sedation (70%) or general anesthesia (30%) | CT/fluoroscopy-guided | Not reported | 6.7 min | Neuropathic pain, syncope, rupture of disk adjacent to the treated vertebra | 3 days,1 week, 1 month, 3 months | Not specified |
| Gerogy et al., 2009 [7] | Not reported | Not reported | CT/fluoroscopy-guided | Non-enhanced CT scan | 1.5–6 min | Bone cement extravasation (venous, cortical, epidural, neural foramina) | 2–4 weeks | Not specified |
| Giammalva et al., 2022 [2] | 63.44 (34–86) | General anesthesia | CT/fluoroscopy-guided | Non-enhanced CT scan | 60.4 min | Perivertebral cement leakage | 1 week, 1 month, 3 months, 6 months | Not specified |
| He et al., 2021 [9] | Median age 58 (18–76) | Local anesthesia | CT/fluoroscopy-guided | Non-enhanced CT scan | 10–15 min | Local edema, increased pain, numbness of the lower extremities, transient aggravation of lower extremity function, decreased mobility in some patients after the operation, abnormal stool function and abnormal urine function after the operation | 1 week, 1 month, 3 months | Not specified |
| Lu et al., 2017 [11] | 56.9 (37–77) | Conscious sedation; local anesthesia | CT/fluoroscopy-guided | Non-enhanced CT scan | Not specified | Asymptomatic bone cement extravasation (paravertebral soft tissues, paravertebral veins, epidural space, adjacent disk) after PVP + RFA | 1 week, 1 month, 6 months | Not specified |
| Lv et al., 2020 [12] | 56.9 (37–77) | Conscious sedation; local anesthesia | CT/fluoroscopy-guided | Non-enhanced CT scan | 1.5–2.5 min for anterior vertebral body lesions 2.5–3.5 min for posterior vertebral body lesions | Asymptomatic bone cement leakage (paravertebral soft tissues, epidural space, adjacent disk) Group A: 6.4% Group B: 20.5% | 3 days, 1 month, 6 months | Group A: 11.4% (4) Group B: 30.8% (11) |
| Maugeri et al., 2017 [13] | 55.72 (34–69) | General anesthesia | CT/fluoroscopy-guided | Non-enhanced CT scan | 60.4 min | Asymptomatic bone cement leakage (lateral spinal recess) | 1 week, 1 month, 3 months, 6 months | Not specified |
| Pezeshki et al., 2016 [14] | Cadaver specimens | Cadaver specimens | CT/fluoroscopy-guided | Non-enhanced CT scan | 12 min | / | / | / |
| Reyes et al., 2017 [15] | 64.3 ± 12.6 | Conscious sedation; local anesthesia | CT/fluoroscopy-guided | Non-enhanced CT scan (23); Contrast-enhanced MRI (10); Non-enhanced MRI (8); FDG-PET (10) | 3.7 ± 2.5 min | None | 2–4 weeks | New extension of tumor into a neural foramen with epidural extension (1); increased epidural extension after ablation due to unexpected development of new malignancy (1) |
| Abdelgawaad et al., 2021 [16] | 69 ± 10.2 (50–79) | General anesthesia | CT/fluoroscopy-guided | Plain X-rays | Not specified | Asymptomatic leaks into the needle track (2), into draining veins (2) and into the disk space (1) | 3 days, next follow-up at least at 6 months (mean 13.2 ± 6.3) | Not specified |
| Wallace et al., 2015 [17] | 68.4 ± 18.8 | Conscious sedation; local anesthesia | CT/fluoroscopy-guided | Not specified | 8 min 32 s ± 4 min 49 s | Post-procedure temporary radicular pain (4); 60% percent (3/5) of the radiofrequency ablated vertebrae that were not augmented fractured within the subsequent 12 months. | 1 week, 4 weeks | Not specified |
| Yang et al., 2017 [18] | 62.7 ± 9.0 (46–82) | Conscious sedation; local anesthesia | CT/fluoroscopy-guided | Not specified | 5–15 min | Asymptomatic cement leakage (2); spinal cord compression symptoms (1) improved after 7-days medical therapy. | 1, 3, 6, and 12 months (mean duration 7.8 months) | Partial tumor progression, with the tumors penetrating the nerve segments (5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colonna, S.; Bianconi, A.; Cofano, F.; Prior, A.; Di Perna, G.; Palmieri, G.; Zona, G.; Garbossa, D.; Fiaschi, P. Radiofrequency Ablation in Vertebral Body Metastasis with and without Percutaneous Cement Augmentation: A Systematic Review Addressing the Need for SPINE Stability Evaluation. Diagnostics 2023, 13, 1164. https://doi.org/10.3390/diagnostics13061164
Colonna S, Bianconi A, Cofano F, Prior A, Di Perna G, Palmieri G, Zona G, Garbossa D, Fiaschi P. Radiofrequency Ablation in Vertebral Body Metastasis with and without Percutaneous Cement Augmentation: A Systematic Review Addressing the Need for SPINE Stability Evaluation. Diagnostics. 2023; 13(6):1164. https://doi.org/10.3390/diagnostics13061164
Chicago/Turabian StyleColonna, Stefano, Andrea Bianconi, Fabio Cofano, Alessandro Prior, Giuseppe Di Perna, Giuseppe Palmieri, Gianluigi Zona, Diego Garbossa, and Pietro Fiaschi. 2023. "Radiofrequency Ablation in Vertebral Body Metastasis with and without Percutaneous Cement Augmentation: A Systematic Review Addressing the Need for SPINE Stability Evaluation" Diagnostics 13, no. 6: 1164. https://doi.org/10.3390/diagnostics13061164