
Salivary Protein and Electrolyte Profiles during Primary Teeth Eruption: A Cross-Sectional Study
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wise, G.E.; Frazier-Bowers, S.; D’souza, R.N. Cellular, molecular, and genetic determinants of tooth eruption. Crit. Rev. Oral Biol. Med. 2002, 13, 323–335. [Google Scholar] [CrossRef] [Green Version]
- Thesleff, I. The genetic basis of tooth development and dental defects. Am. J. Med. Genet. Part A 2006, 140, 2530–2535. [Google Scholar] [CrossRef]
- Barlow, B.S.; Kanellis, M.J.; Slayton, R.L. Tooth eruption symptoms: A survey of parents and health professionals. J. Dent. Child. 2002, 69, 148–150. [Google Scholar]
- Iavarone, F.; Olianas, A.; Patini, R.; Gallenzi, P.; Di Tonno, L.; Desiderio, C.; Cabras, T.; Manconi, B.; Vincenzoni, F.; Cordaro, M.; et al. Top down proteomic analysis of gingival crevicular fluid in deciduous, exfoliating and permanent teeth in children. J. Proteom. 2020, 226, 103890. [Google Scholar] [CrossRef]
- Nahajowski, M.; Hnitecka, S.; Antoszewska-Smith, J.; Rumin, K.; Dubowik, M.; Sarul, M. Factors influencing an eruption of teeth associated with a dentigerous cyst: A systematic review and meta-analysis. BMC Oral Health 2021, 21, 180. [Google Scholar] [CrossRef]
- Rao, P.V.; Reddy, A.P.; Lu, X.; Dasari, S.; Krishnaprasad, A.; Biggs, E.; Roberts, C.T., Jr.; Nagalla, S.R. Proteomic identification of salivary biomarkers of type-2 diabetes. J. Proteome Res. 2009, 8, 239–245. [Google Scholar] [CrossRef]
- Deshpande, R.R.; Panvalkar, P.S.; Kulkarni, A.A.; Gadkri, T.V. Age-related changes of the human salivary secretory total protein complex and trace elements in children between the age group of 3-16 years. J. Biomed. Sci. Res. 2011, 3, 362–367. [Google Scholar]
- Dezan, C.; Nicolau, J.; Souza, D.; Walter, L. Flow rate, amylase activity, and protein and sialic acid concentrations of saliva from children aged 18, 30 and 42 months attending a baby clinic. Arch. Oral Biol. 2002, 47, 423–427. [Google Scholar] [CrossRef]
- Messana, I.; Cabras, T.; Iavarone, F.; Manconi, B.; Huang, L.; Martelli, C.; Olianas, A.; Sanna, M.T.; Pisano, E.; Sanna, M.; et al. Chrono-Proteomics of Human Saliva: Variations of the Salivary Proteome during Human Development. J. Proteome Res. 2015, 14, 1666–1677. [Google Scholar] [CrossRef] [Green Version]
- Manconi, B.; Cabras, T.; Pisano, E.; Sanna, M.; Olianas, A.; Fanos, V.; Faa, G.; Nemolato, S.; Iavarone, F.; Castagnola, M.; et al. Modifications of the acidic soluble salivary proteome in human children from birth to the age of 48months investigated by a top-down HPLC–ESI–MS platform. J. Proteom. 2013, 91, 536–543. [Google Scholar] [CrossRef]
- Inzitari, R.; Vento, G.; Capoluongo, E.; Boccacci, S.; Fanali, C.; Cabras, T.; Romagnoli, C.; Giardina, B.; Messana, I.; Castagnola, M. Proteomic Analysis of Salivary Acidic Proline-Rich Proteins in Human Preterm and At-Term Newborns. J. Proteome Res. 2007, 6, 1371–1377. [Google Scholar] [CrossRef]
- Cabras, T.; Pisano, E.; Boi, R.; Olianas, A.; Manconi, B.; Inzitari, R.; Fanali, C.; Giardina, B.; Castagnola, M.; Messana, I. Age-Dependent Modifications of the Human Salivary Secretory Protein Complex. J. Proteome Res. 2009, 8, 4126–4134. [Google Scholar] [CrossRef]
- Castagnola, M.; Inzitari, R.; Fanali, C.; Iavarone, F.; Vitali, A.; Desiderio, C.; Messana, I. The surprising composition of the salivary proteome of preterm human newborn. Mol. Cell. Proteom. 2011, 10, M110.003467. [Google Scholar] [CrossRef] [Green Version]
- Morzel, M.; Palicki, O.; Chabanet, C.; Lucchi, G.; Ducoroy, P.; Chambon, C.; Nicklaus, S. Saliva electrophoretic protein profiles in infants: Changes with age and impact of teeth eruption and diet transition. Arch. Oral Biol. 2011, 56, 634–642. [Google Scholar] [CrossRef]
- Tabbara, N. Identification of the Salivary Proteome in Children Throughout the Course of Dental Eruption; The University of Western Ontario: London, Canada, 2013. [Google Scholar]
- Gill, J.K.; Kaur, M.; Kaur, K.; Goel, S. Salivary biomarkers as a diagnostic indicator-a brief review. J. Adv. Med. Dent. Sci. Res. 2017, 5, 87. [Google Scholar]
- Carpenter, G.H. The secretion, components, and properties of saliva. Annu. Rev. Food Sci. Technol. 2013, 4, 267–276. [Google Scholar] [CrossRef]
- Oudhoff, M.J.; Bolscher, J.G.M.; Nazmi, K.; Kalay, H.; Hof, W.V.; Amerongen, A.V.N.; Veerman, E.C.I. Histatins are the major wound-closure stimulating factors in human saliva as identified in a cell culture assay. FASEB J. 2008, 22, 3805–3812. [Google Scholar] [CrossRef] [Green Version]
- Oudhoff, M.J.; Kroeze, K.L.; Nazmi, K.; van den Keijbus, P.A.; van’t Hof, W.; Fernandez-Borja, M.; Veerman, E.C. Structure-activity analysis of histatin, a potent wound healing peptide from human saliva: Cyclization of histatin potentiates molar activity 1000-fold. FASEB J. 2009, 23, 3928–3935. [Google Scholar] [CrossRef] [Green Version]
- Morzel, M.; Jeannin, A.; Lucchi, G.; Truntzer, C.; Pecqueur, D.; Nicklaus, S.; Chambon, C.; Ducoroy, P. Human infant saliva peptidome is modified with age and diet transition. J. Proteom. 2012, 75, 3665–3673. [Google Scholar] [CrossRef]
- Bobek, L.A.; Levine, M.J. Cystatins—Inhibitors of cysteine proteinases. Crit. Rev. Oral Biol. Med. 1992, 3, 307–332. [Google Scholar] [CrossRef] [Green Version]
- Dickinson, D.; Thiesse, M.; Hicks, M. Expression of Type 2 Cystatin Genes CST1-CST5 in Adult Human Tissues and the Developing Submandibular Gland. DNA Cell Biol. 2002, 21, 47–65. [Google Scholar] [CrossRef]
- Katsukawa, H.; Ninomiya, Y. Capsaicin Induces Cystatin S-like Substances in Submandibular Saliva of the Rat. J. Dent. Res. 1999, 78, 1609–1616. [Google Scholar] [CrossRef]
- Fábián, T.K.; Hermann, P.; Beck, A.; Fejérdy, P.; Fábián, G. Salivary Defense Proteins: Their Network and Role in Innate and Acquired Oral Immunity. Int. J. Mol. Sci. 2012, 13, 4295–4320. [Google Scholar] [CrossRef] [Green Version]
- Gibbons, R.J.; Hay, D.I.; Schlesinger, D.H. Delineation of a segment of adsorbed salivary acidic proline-rich proteins which promotes adhesion of Streptococcus gordonii to apatitic surfaces. Infect. Immun. 1991, 59, 2948–2954. [Google Scholar] [CrossRef] [Green Version]
- Böttcher, M.F.; Häggström, P.; Björkstén, B.; Jenmalm, M. Total and allergen-specific immunoglobulin A levels in saliva in relation to the development of allergy in infants up to 2 years of age. Clin. Exp. Allergy 2002, 32, 1293–1298. [Google Scholar] [CrossRef]
- Wan, A.K.L.; Seow, W.K.; Purdie, D.M.; Bird, P.S.; Walsh, L.; Tudehope, D.I. Immunoglobulins in saliva of preterm and full-term infants. A longitudinal study from 0–18 months of age. Oral Microbiol. Immunol. 2003, 18, 72–78. [Google Scholar] [CrossRef]
- Gleeson, M.; Cripps, A.W. Development of mucosal immunity in the first year of life and relationship to sudden infant death syndrome. FEMS Immunol. Med. Microbiol. 2004, 42, 21–33. [Google Scholar] [CrossRef]
- Bellavia, S.; Moreno, J.; Sanz, E.; Picas, E.I.; Blanco, A. α-Amylase activity of human neonate and adult saliva. Arch. Oral Biol. 1979, 24, 117–121. [Google Scholar] [CrossRef]
- Ruhl, S.; Rayment, S.A.; Schmalz, G.; Hiller, K.-A.; Troxler, R.F. Proteins in Whole Saliva during the First Year of Infancy. J. Dent. Res. 2005, 84, 29–34. [Google Scholar] [CrossRef]
- Janiani, P.; Ravindran, V. Comparative evaluation of the antimicrobial effects of probiotic milk and probiotic powder on the salivary Streptococcus mutans counts and the plaque scores in children aged 3–6 years: A randomized controlled trial. Dent. Med. Probl. 2022, 59, 99–104. [Google Scholar] [CrossRef]
- De Oliveira, R.; Navas, E.; Duran, C.; Pinto, M.; Gutierrez, J.; Eblen-Zajjur, A. Aging related changes in mixed basal saliva concentration of sodium, potassium and chloride in healthy non medicated humans. Curr. Aging Sci. 2014, 7, 110–114. [Google Scholar] [CrossRef]
- Castagnola, M.; Cabras, T.; Vitali, A.; Sanna, M.T.; Messana, I. Biotechnological implications of the salivary proteome. Trends Biotechnol. 2011, 29, 409–418. [Google Scholar] [CrossRef]
- Sarvaiya, B.; Mehta, D.; Singh, V.; Arora, R.; Bhayya, D.; Singh, D. Comparison of relationship between salivary electrolyte levels and dental caries in children with Down syndrome. J. Nat. Sci. Biol. Med. 2015, 6, 144–148. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, V.P.; Franco, M.M.; Marques, C.P.; de Carvalho, R.C.; Leite, S.A.; Pereira, A.L.; Benatti, B.B. Salivary levels of calcium, phosphorus, potassium, albumin and correlation with serum biomarkers in hemodialysis patients. Arch. Oral Biol. 2016, 62, 58–63. [Google Scholar] [CrossRef]
- Shirzaii, M.; Heidari, F. Evaluation chemical composition of unstimulated saliva, in patients with type I diabetes mellitus. Zahedan J. Res. Med. Sci. 2013, 15, 15–18. [Google Scholar]
- Bang, J.; Cimasoni, G.; Rosenbusch, C.; Duckert, A. Sodium, Potassium and Calcium Contents of Crevicular Exudate: Their Relations to Gingivitis and Periodontitis. J. Periodontol. 1973, 44, 770–774. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Age (Month) | Weight (kg) | Gender | Total (%) | ||
|---|---|---|---|---|---|---|
| Group | Mean ± Standard Deviation | Mean ± Standard Deviation | Male Number (%) | Female Number (%) | ||
| A | 5.17 ± 6.16 | 6.59 ± 8.59 | 25 (51) | 24 (49) | 49 (100) | |
| B | 7.16 ± 14.07 | 1.95 ± 10.26 | 32 (60.4) | 21 (39.6) | 53 (100) | |
| C | 8.33 ± 42.11 | 2.19 ± 14.17 | 18 (40) | 27 (60) | 45 (100) | |
| Clinical Signs and Symptoms | Number (%) |
|---|---|
| Gastrointestinal complications | 24 (46.15) |
| Gingival swelling or redness | 27 (51.92) |
| Perioral redness | 8 (15.38) |
| Irritability | 42 (80.76) |
| Hyper-salivation | 45 (86.53) |
| Putting hand in the mouth | 50 (96.15) |
| Skin rashes | 4 (7.69) |
| Malaise | 16 (30.76) |
| Fever | 35 (67.30) |
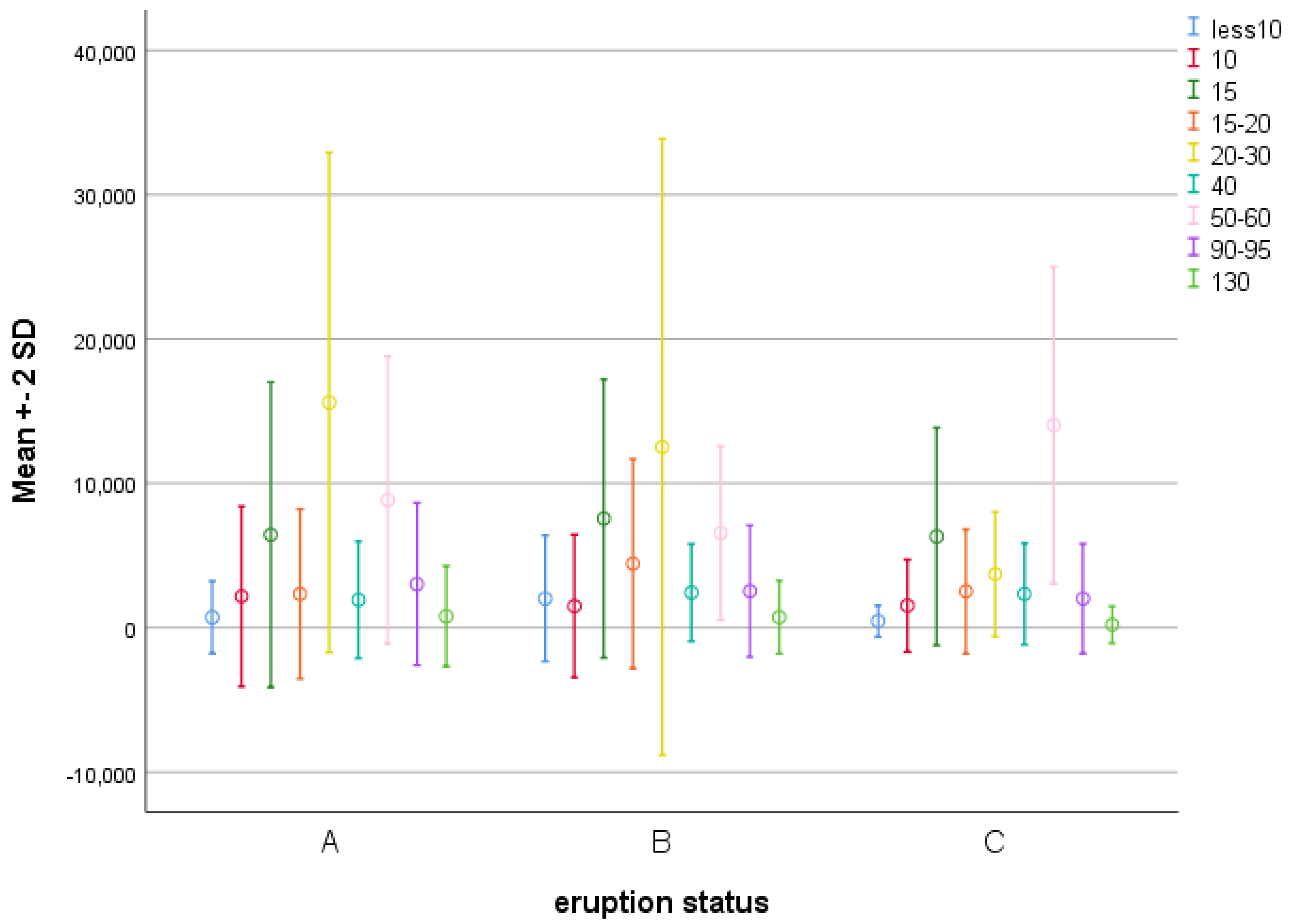
| Molecular Weight (KD) | A | B | C | p-Value * |
|---|---|---|---|---|
| Mean ± Standard Deviation | Mean ± Standard Deviation | Mean ± Standard Deviation | ||
| <10 | 1228.80 ± 698.15 | 2181.35 ± 2021.60 | 548.79 ± 463.13 | <0.001 |
| 10 | 3082.02 ± 2201.19 | 2473.94 ± 1489.30 | 1541.47 ± 1455.47 | 0.261 |
| 15 | 5765.84 ± 6933.28 | 4821.13 ± 7565.93 | 3607.24 ± 6122.51 | 0.375 |
| 20–15 | 2910.68 ± 2313.71 | 3629.41 ± 4440.93 | 2174.24 ± 2486.53 | <0.001 |
| 30–20 | 9399.27 ± 15,960.54 | 10,672.66 ± 12,512.34 | 2143.05 ± 3643.56 | <0.001 |
| 40 | 1985.90 ± 1944.01 | 1684.75 ± 2431.67 | 1780.50 ± 2326.70 | 0.378 |
| 60–50 | 5010.35 ± 9048.58 | 3010.74 ± 6554.44 | 5547.18 ± 13,961.51 | <0.001 |
| 95–90 | 2776.19 ± 2962.21 | 2278.19 ± 2531.97 | 1921.05 ± 2001.25 | 0.169 |
| >130 | 1723.18 ± 774.50 | 1260.46 ± 725.84 | 651.98 ± 211.23 | 0.094 |
| Molecular Weight | Group | Mean | p-Value * |
|---|---|---|---|
| <10 | A vs. B | −1323.44 ± 306.42 | <0.001 |
| A vs. C | 235.02 ± 327.96 | 1 | |
| B vs. C | 1558.46 ± 323.68 | <0.001 | |
| 20–15 | A vs. B | −2127.21 ± 602.27 | 0.002 |
| A vs. C | −172.81 ± 644.61 | 1 | |
| B vs. C | 1954.39 ± 436.20 | 0.008 | |
| 30–20 | A vs. B | 3448.20 ± 1714.10 | 0.139 |
| A vs. C | 12,316.98 ± 1834.60 | <0.001 | |
| B vs. C | 8868.78 ± 1810.66 | <0.001 | |
| 50–60 | A vs. B | 2494.14 ± 907.53 | 0.020 |
| A vs. C | −4912.93 ± 971.33 | <0.001 | |
| B vs. C | −7407.07 ± 958.65 | <0.001 |
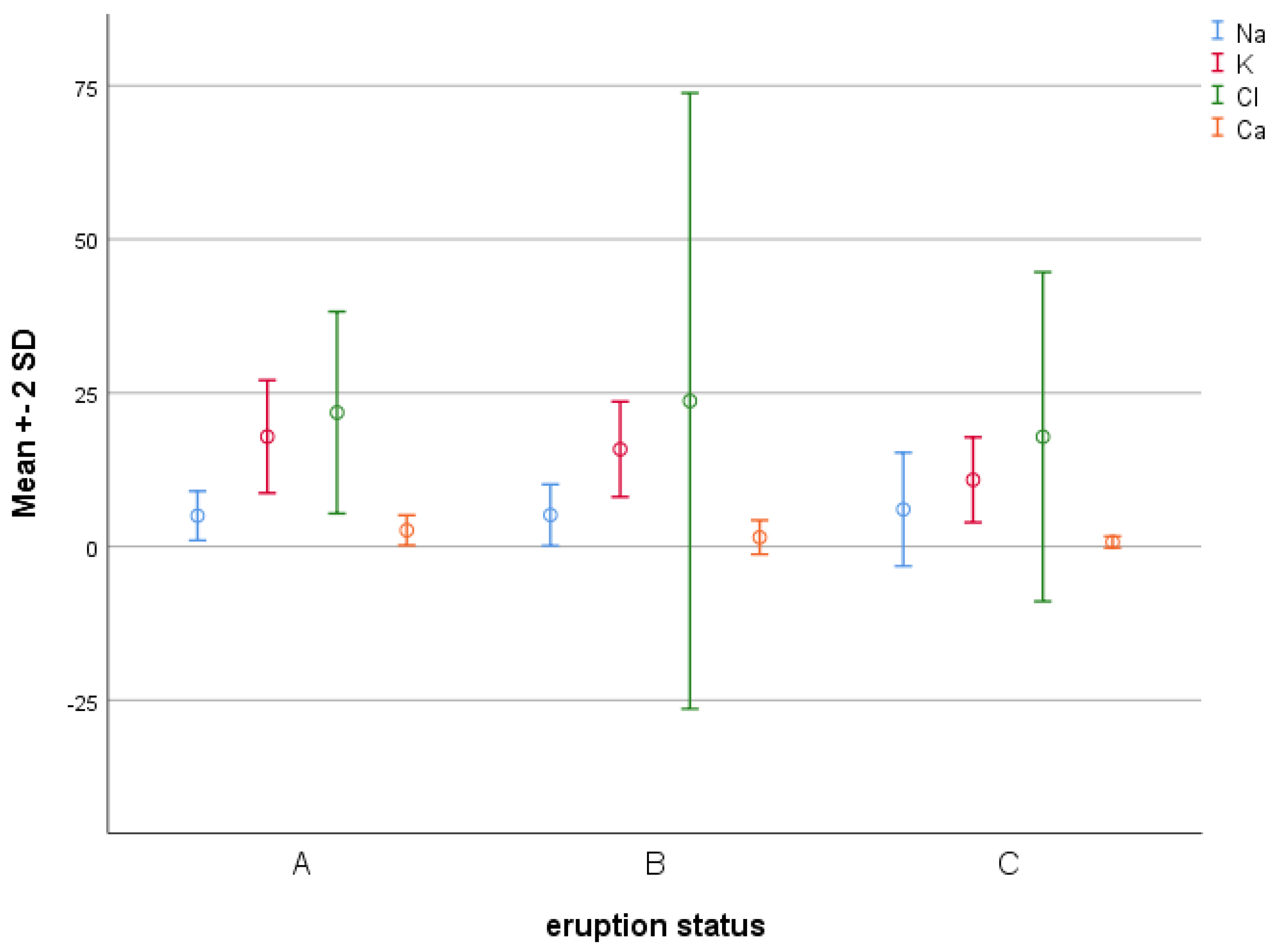
| Electrolyte | A | B | C | p-Value * |
|---|---|---|---|---|
| Mean ± Standard Deviation | Mean ± Standard Deviation | Mean ± Standard Deviation | ||
| Sodium | 2.15 ± 4.81 | 2.53 ± 5.14 | 4.58 ± 6.16 | 0.114 |
| Potassium | 4.13 ± 16.90 | 3.88 ± 16.01 | 3.79 ± 11.10 | <0.001 |
| Chloride | 8.06 ± 21.21 | 24.55 ± 23.60 | 13.25 ± 17.45 | 0.22 |
| Calcium | 1.22 ± 2.64 | 1.38 ± 1.49 | 0.46 ± 0.71 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmadian, M.; Maleki Kambakhsh, S.; Einollahi, N.; Babazadeh, S.; Tofangchiha, M.; D’Amato, G.; Patini, R. Salivary Protein and Electrolyte Profiles during Primary Teeth Eruption: A Cross-Sectional Study. Diagnostics 2023, 13, 1335. https://doi.org/10.3390/diagnostics13071335
Ahmadian M, Maleki Kambakhsh S, Einollahi N, Babazadeh S, Tofangchiha M, D’Amato G, Patini R. Salivary Protein and Electrolyte Profiles during Primary Teeth Eruption: A Cross-Sectional Study. Diagnostics. 2023; 13(7):1335. https://doi.org/10.3390/diagnostics13071335
Chicago/Turabian StyleAhmadian, Mina, Sara Maleki Kambakhsh, Nahid Einollahi, Saber Babazadeh, Maryam Tofangchiha, Giuseppe D’Amato, and Romeo Patini. 2023. "Salivary Protein and Electrolyte Profiles during Primary Teeth Eruption: A Cross-Sectional Study" Diagnostics 13, no. 7: 1335. https://doi.org/10.3390/diagnostics13071335