
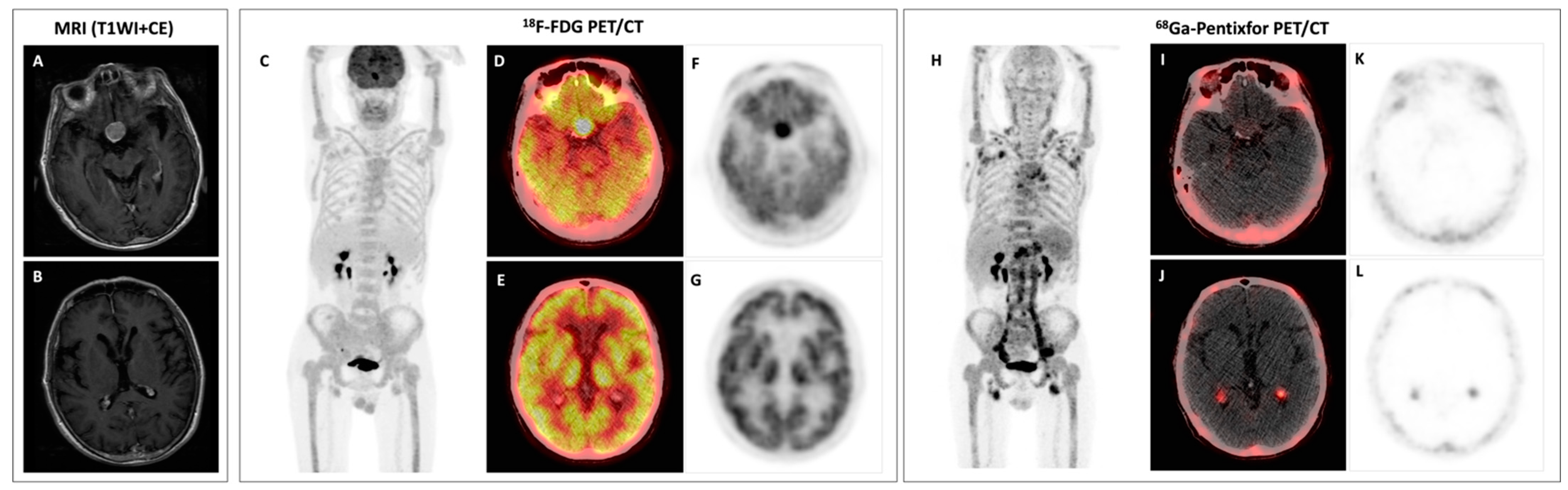
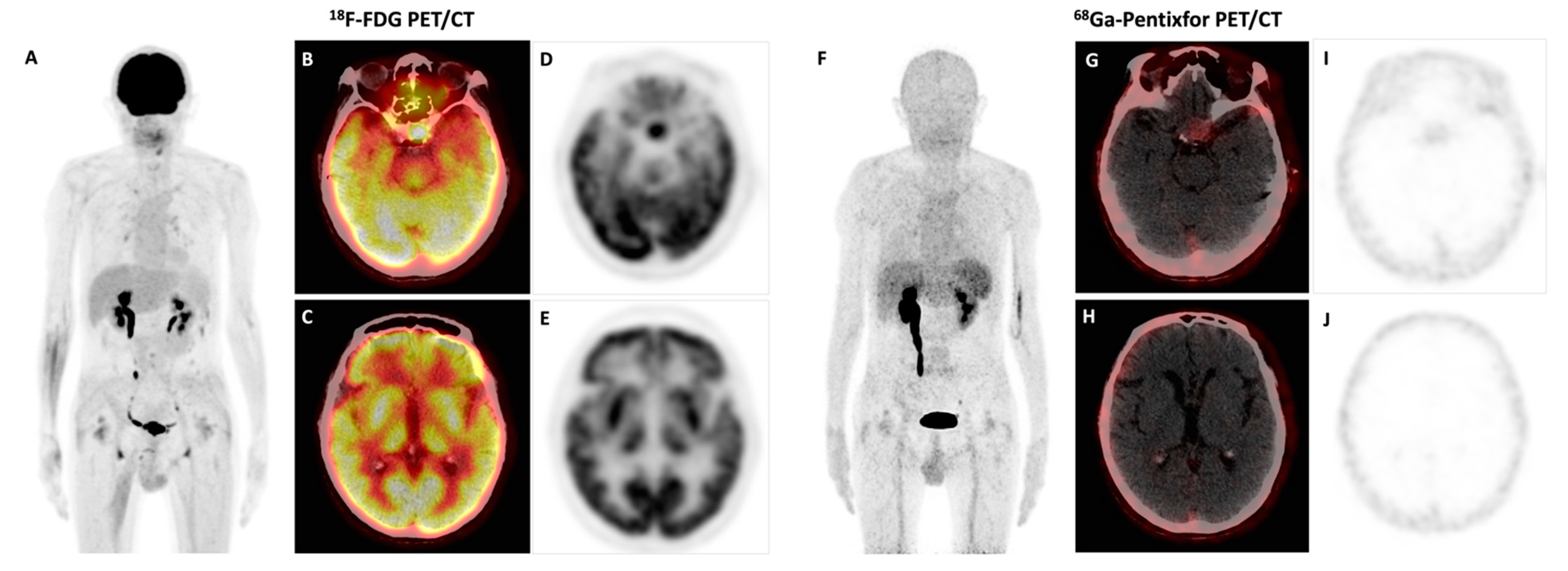
Bing–Neel Syndrome and Coexisting Pituitary Macroadenoma in a Patient with Waldenström Macroglobulinemia Revealed by 18F-FDG and 68Ga-Pentixafor PET/CT

{kind=link}
{kind=link}
Abstract
:

Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hunter, Z.R.; Yang, G.; Xu, L.; Liu, X.; Castillo, J.J.; Treon, S.P. Genomics, Signaling, and Treatment of Waldenstrom Macroglobulinemia. J. Clin. Oncol. 2017, 35, 994–1001. [Google Scholar] [CrossRef] [PubMed]
- Mazzucchelli, M.; Frustaci, A.M.; Deodato, M.; Cairoli, R.; Tedeschi, A. Waldenstrom’s Macroglobulinemia: An Update. Mediterr. J. Hematol. Infect. Dis. 2018, 10, e2018004. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Cao, X.; Pan, Q.; Li, J.; Feng, J.; Li, F. 68Ga-Pentixafor PET/CT for Imaging of Chemokine Receptor 4 Expression in Waldenström Macroglobulinemia/Lymphoplasmacytic Lymphoma: Comparison to 18F-FDG PET/CT. J. Nucl. Med. 2019, 60, 1724–1729. [Google Scholar] [CrossRef] [PubMed]
- Minnema, M.C.; Kimby, E.; D’Sa, S.; Fornecker, L.-M.; Poulain, S.; Snijders, T.J.; Kastritis, E.; Kremer, S.; Fitsiori, A.; Simon, L.; et al. Guideline for the diagnosis, treatment and response criteria for Bing-Neel syndrome. Haematologica 2017, 102, 43–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castillo, J.J.; D’Sa, S.; Lunn, M.; Minnema, M.C.; Tedeschi, A.; Lansigan, F.; Palomba, M.L.; Varettoni, M.; Garcia-Sanz, R.; Nayak, L.; et al. Central nervous system involvement by Waldenstrom macroglobulinaemia (Bing-Neel syndrome): A multi-institutional retrospective study. Br. J. Haematol. 2016, 172, 709–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitsiori, A.; Fornecker, L.M.; Simon, L.; Karentzos, A.; Galanaud, D.; Outteryck, O.; Vermersch, O.; Pruvo, P.; Gerardin, J.-P.; Lebrun-Frenay, E.; et al. Imaging spectrum of Bing-Neel syndrome: How can a radiologist recognise this rare neurological complication of Waldenstrom’s macroglobulinemia? Eur. Radiol. 2019, 29, 102–114. [Google Scholar] [CrossRef] [PubMed]
- Bund, C.; Lhermitte, B.; De Seze, J.; Kremer, S.; Namer, I.J. FDG PET and MRI Findings in a Case of Bing-Neel Syndrome. Clin. Nucl. Med. 2018, 43, 262–264. [Google Scholar] [CrossRef] [PubMed]
- Illarramendi, O.A.; Flynt, L.; Wong, F. 18F-FDG PET/CT in the Evaluation of Bing-Neel Syndrome. J. Nucl. Med. Technol. 2019, 47, 343–344. [Google Scholar] [CrossRef] [PubMed]
- Riaz, S.; Priftakis, D.; Arulogun, S.; Wan, S.; Bomanji, J. Before and After Treatment Characterization of Cerebrospinal Disease in Bing-Neel Syndrome Using 18F FDG PET/MRI. Clin. Nucl. Med. 2020, 45, 700–702. [Google Scholar] [CrossRef] [PubMed]
- Ngo, H.T.; Leleu, X.; Lee, J.; Jia, X.; Melhem, M.; Runnels, J.; Moreau, J.; Burwick, A.-S.; Azab, N.; Roccaro, A.K.; et al. SDF-1/CXCR4 and VLA-4 interaction regulates homing in Waldenstrom macroglobulinemia. Blood 2008, 112, 150–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, Q.; Luo, Y.; Cao, X.; Li, J.; Feng, J. Bing–Neel Syndrome and Coexisting Pituitary Macroadenoma in a Patient with Waldenström Macroglobulinemia Revealed by 18F-FDG and 68Ga-Pentixafor PET/CT. Diagnostics 2023, 13, 1334. https://doi.org/10.3390/diagnostics13071334
Pan Q, Luo Y, Cao X, Li J, Feng J. Bing–Neel Syndrome and Coexisting Pituitary Macroadenoma in a Patient with Waldenström Macroglobulinemia Revealed by 18F-FDG and 68Ga-Pentixafor PET/CT. Diagnostics. 2023; 13(7):1334. https://doi.org/10.3390/diagnostics13071334
Chicago/Turabian StylePan, Qingqing, Yaping Luo, Xinxin Cao, Jian Li, and Jun Feng. 2023. "Bing–Neel Syndrome and Coexisting Pituitary Macroadenoma in a Patient with Waldenström Macroglobulinemia Revealed by 18F-FDG and 68Ga-Pentixafor PET/CT" Diagnostics 13, no. 7: 1334. https://doi.org/10.3390/diagnostics13071334