
Superselective Catheter Angiographies of the Wrist (SCAW): Approaches for Vascularized Bone Grafts

Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
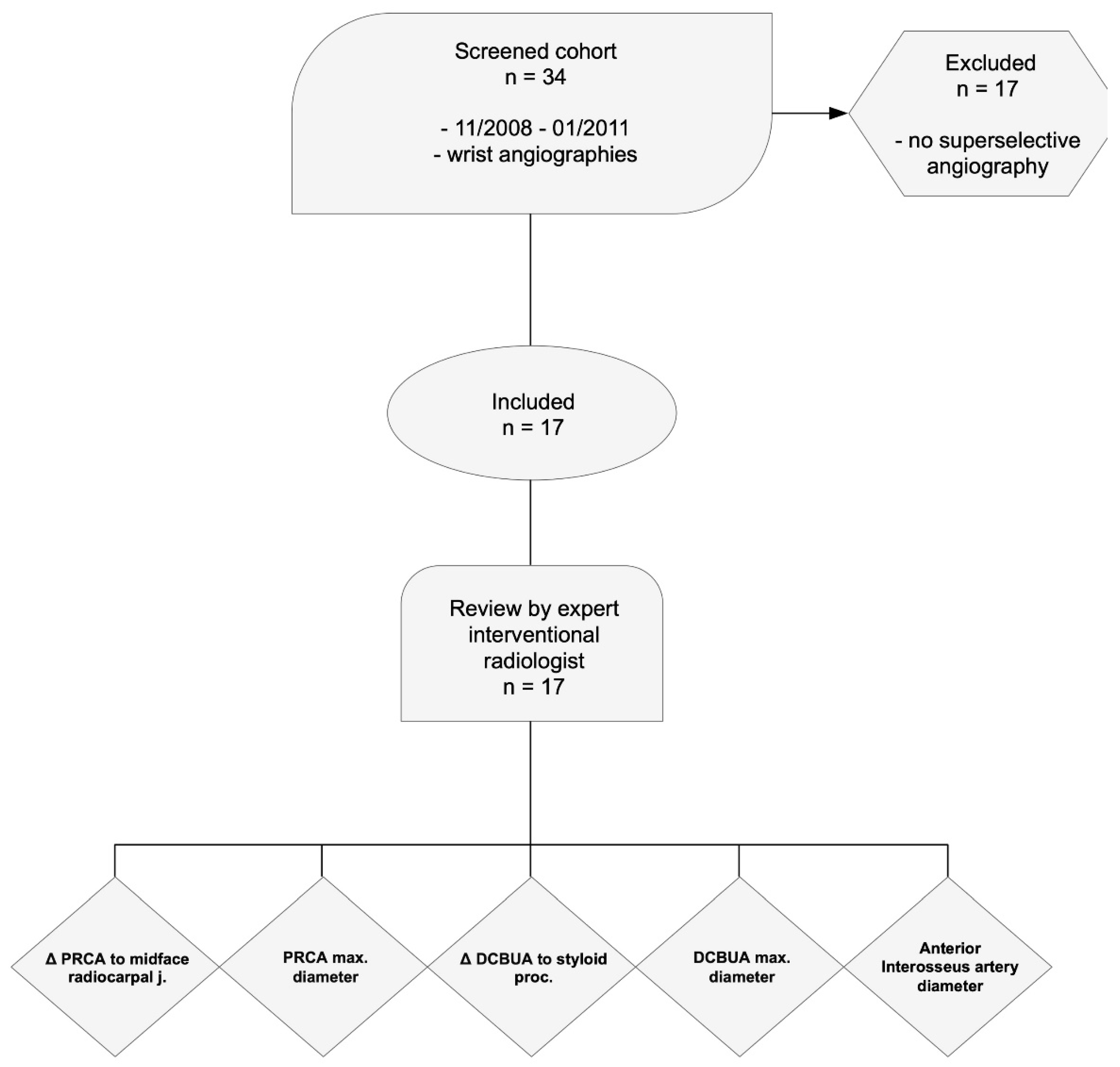
2.2. Patients
2.3. Superselective Catheter Angiographies of the Wrist (SCAW)
2.4. Radiological Assessment
2.5. Statistical Analysis
3. Results
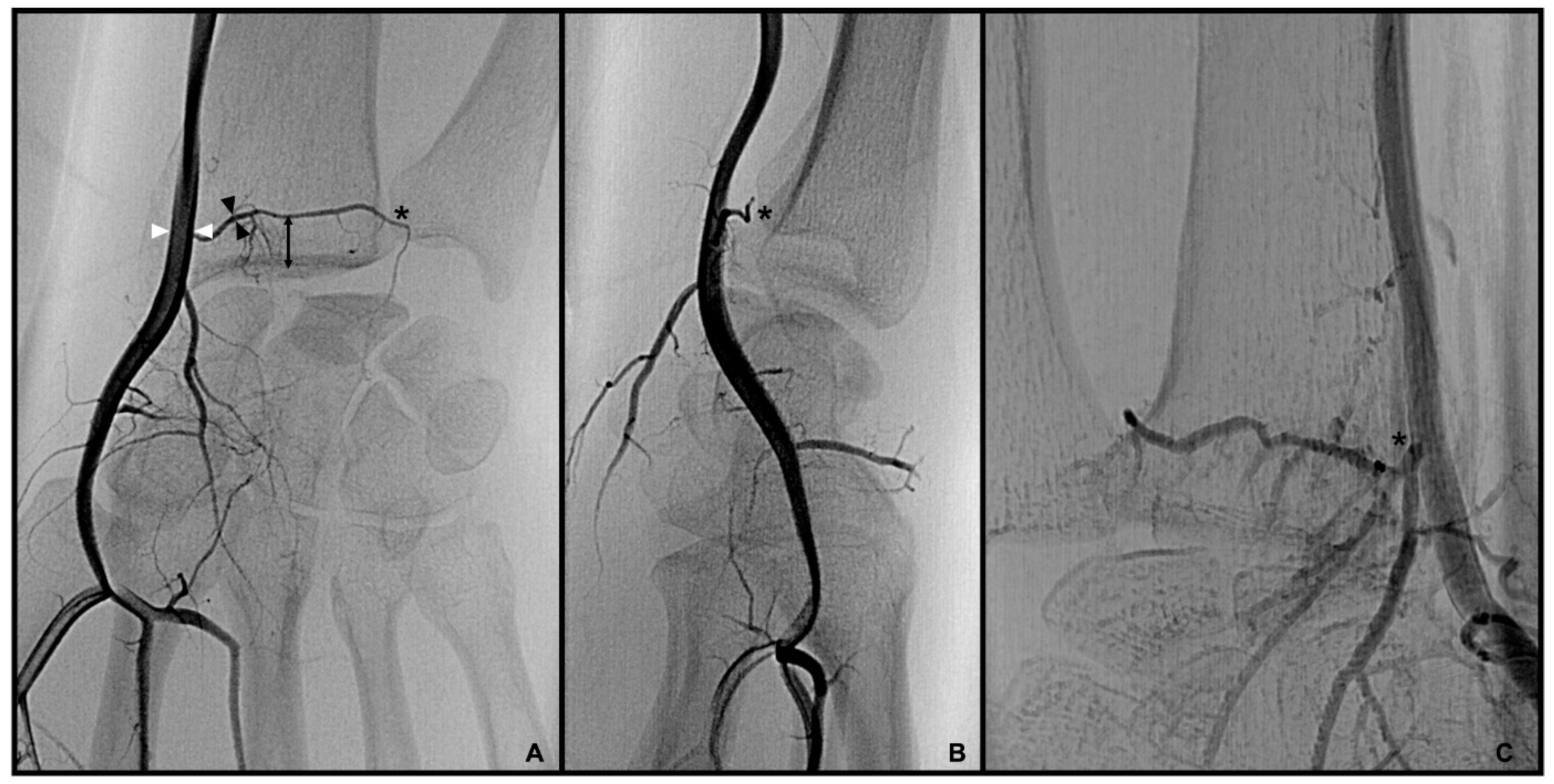
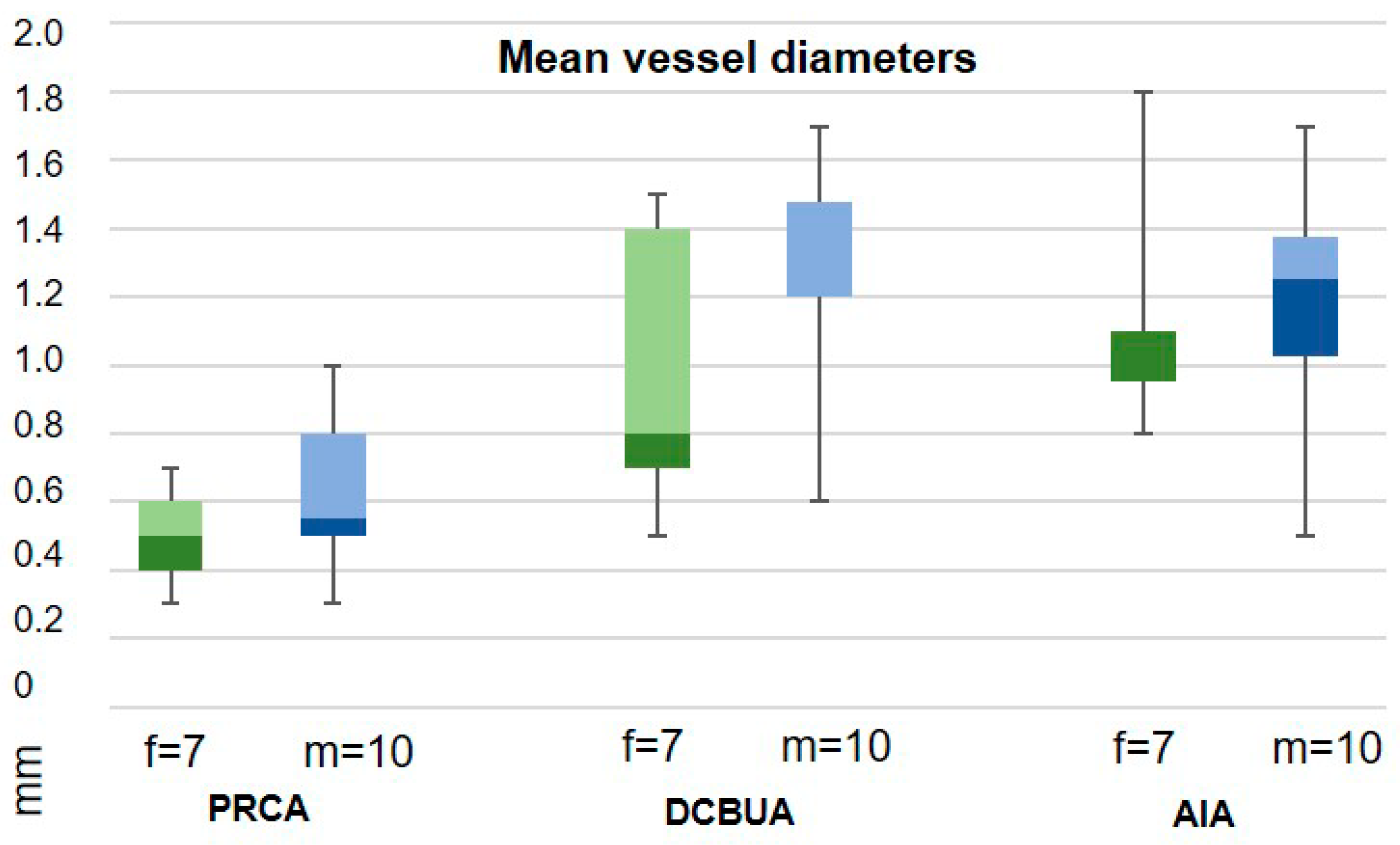
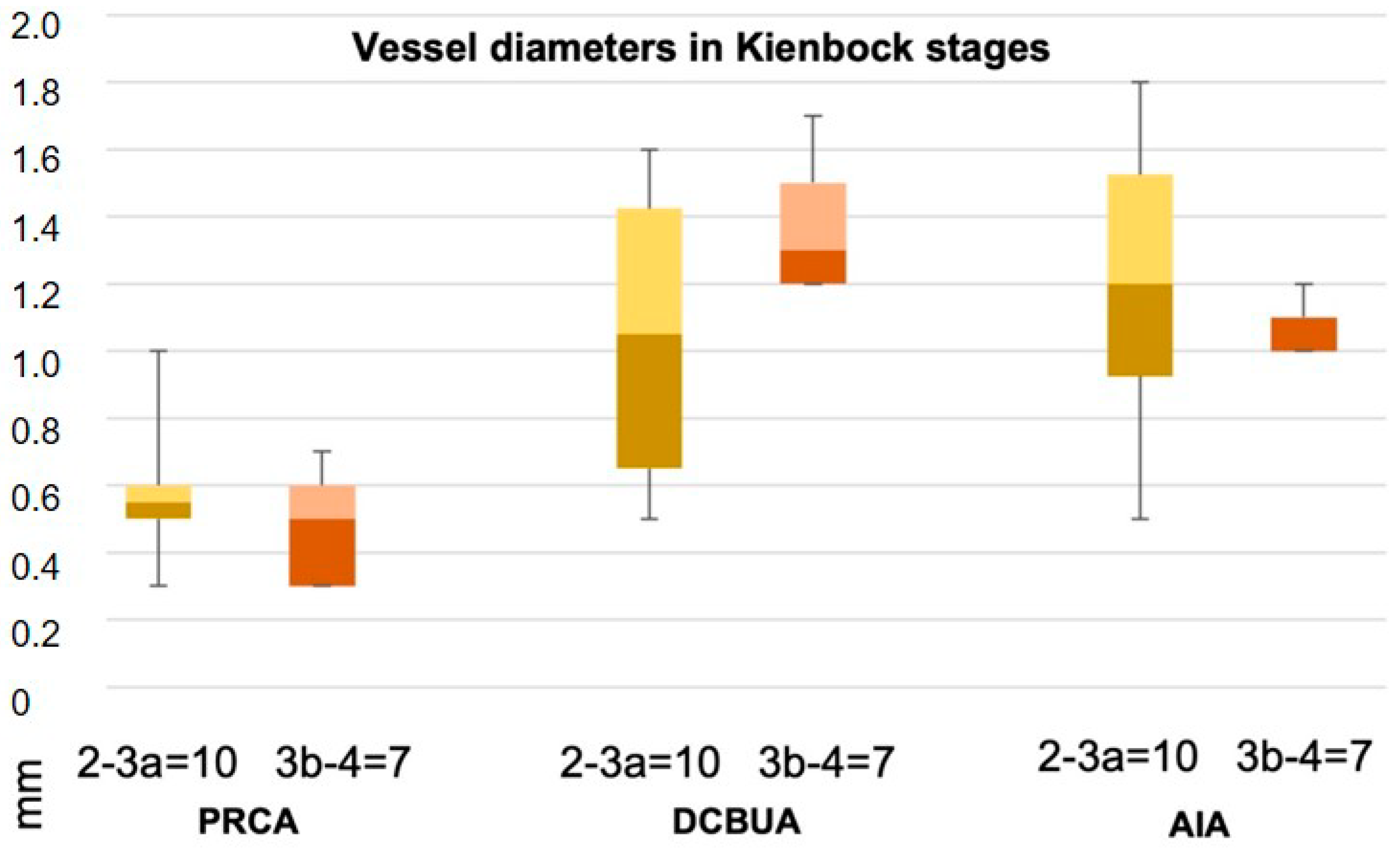
3.1. Palmar Radiocarpal Artery and Palmar Radiocarpal Arch (PRCA)
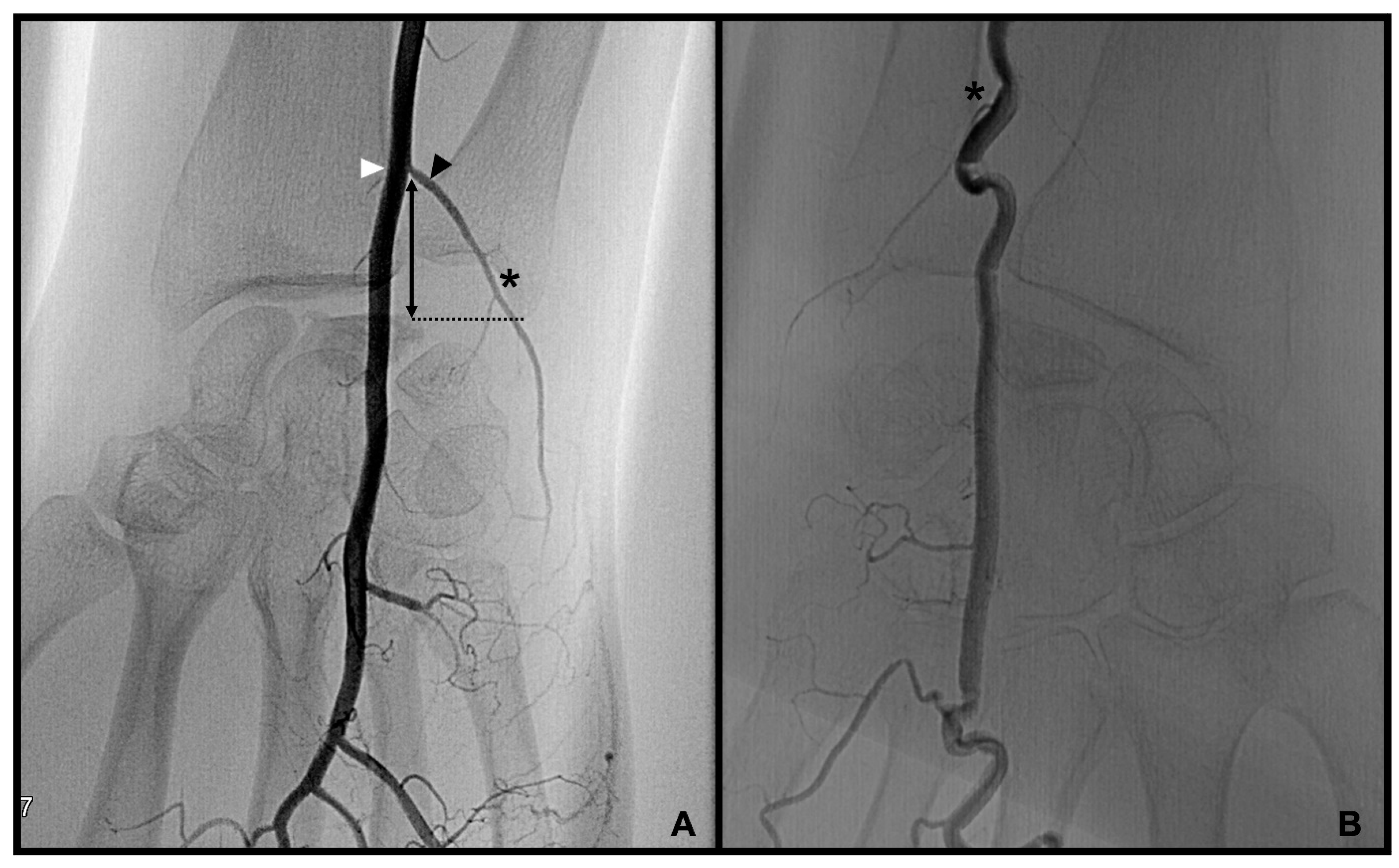
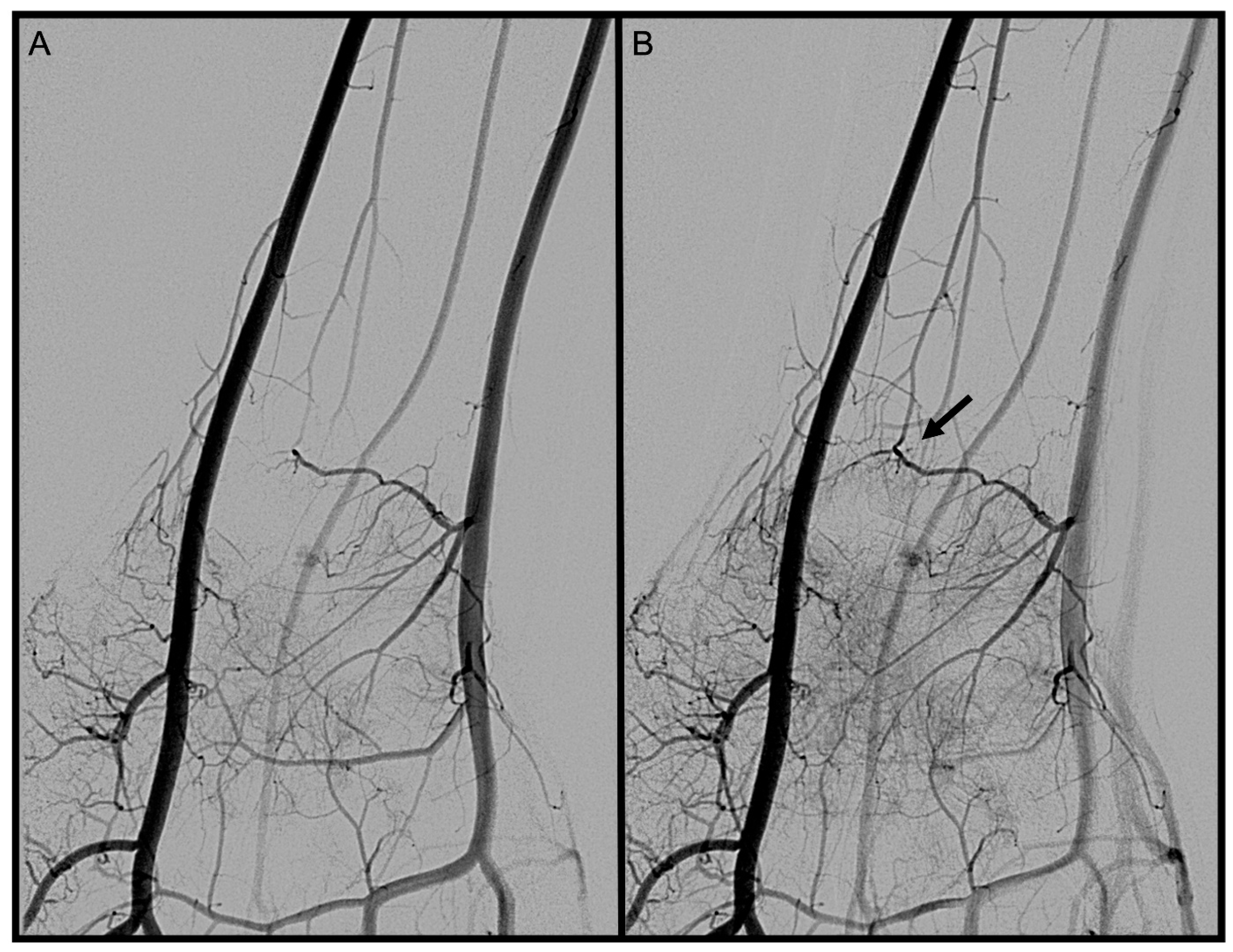
3.2. Dorsal Carpal Branch of the Ulnar Artery (DCBUA)
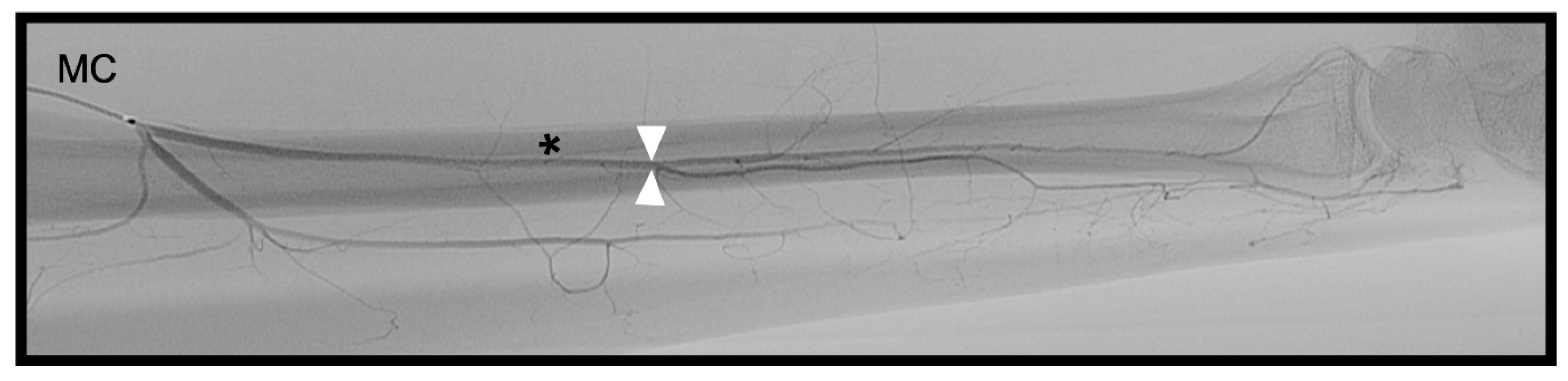
3.3. Anterior Interosseous Artery (AIA)
3.4. Treatment Strategies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SCAW | superselective catheter angiographies of the wrist |
| PRCA | palmar radiocarpal artery |
| DCBUA | dorsal carpal branch of the ulnar artery |
| AIA | anterior interosseous artery |
| STROBE | The Strengthening the Reporting of Observational Studies in Epidemiology Initiative |
References
- Kuhlmann, J.N.; Guerin-Surville, H. Bone graft pedicled to the transverse artery of the carpus (ramus carpeus palmaris). Bull Assoc. Anat. 1980, 64, 243–252. [Google Scholar]
- Kuhlman, J.N.; Mimoun, M.; Boabighi, A.; Baux, S. Vascularized bone graft pedicled on the volar carpal artery for nonunion of the scaphoid. J. Hand. Surg. 1987, 12, 203–210. [Google Scholar]
- Mathoulin, C.; Haerle, M. Vascularized Bone Graft from the Palmar Carpal Artery for Treatment of Scaphoid Nonunion. J. Hand Surg. 1998, 23, 318–323. [Google Scholar] [CrossRef]
- Haerle, M.; Schaller, H.E.; Mathoulin, C. Vascular anatomy of the palmar surfaces of the distal radius and ulna: Its relevance to pedicled bone grafts at the distal palmar forearm. J. Hand Surg. 2003, 28, 131–136. [Google Scholar] [CrossRef]
- Mathoulin, C.; Haerle, M.; Vandeputte, G. Greffon osseux vascularis? dans la reconstruction des os du carpe. Ann. Chir. Plast. Esthtique 2005, 50, 43–48. [Google Scholar] [CrossRef]
- Mathoulin, C.; Wahegaonkar, A.L. Revascularization of the lunate by a volar vascularized bone graft and an osteotomy of the radius in treatment of the Kienböck’s disease. Microsurgery. Wiley Subscr. Serv. Inc. 2009, 29, 373–378. [Google Scholar] [CrossRef]
- Gras, M.; Mathoulin, C. Vascularized bone graft pedicled on the volar carpal artery from the volar distal radius as primary procedure for scaphoid non-union. Orthop. Traumatol. Surg. Res. 2011, 97, 800–806. [Google Scholar] [CrossRef] [Green Version]
- Gelberman, R.H.; Panagis, J.S.; Taleisnik, J.; Baumgaertner, M. The arterial anatomy of the human carpus. Part I: The extraosseous vascularity. J. Hand Surg. 1983, 8, 367–375. [Google Scholar] [CrossRef]
- Beck, E. Die Verpflanzung des Os pisiforme am Gefässstiel zur Behandlung der Lunatummalazie [Transfer of pisiform bone on vascular pedicle in the treatment of lunatomalacia]. Handchirurgie 1971, 3, 64–67. [Google Scholar]
- Oppikofer, C.; Büchler, U.; Schmid, E. The surgical anatomy of the dorsal carpal branch of the ulnar artery: Basis for a neurovascular dorso-ulnar pedicled flap. Surg. Radiol. Anat. 1992, 14, 97–101. [Google Scholar] [CrossRef]
- Hasegawa, H.; Shimizu, T.; Omokawa, S.; Kawamura, K.; Sananpanich, K.; Mahakkanukrauh, P.; Tanaka, Y. Vascularized pedicled bone graft from the distal radius supplied by the anterior interosseous artery for treatment of ulnar shaft nonunion: An anatomical study of cadavers and a case report. Microsurgery 2020, 40, 479–485. [Google Scholar] [CrossRef]
- Panse, N.S.; Joshi, S.B.; Sahasrabudhe, P.B.; Bahetee, B.; Gurude, P.; Chandanwale, A. The Anterior Interosseus Artery Perforator Flap: Anatomical Dissections and Clinical Study. World J. Plast. Surg. 2017, 6, 152–158. [Google Scholar]
- Andro, C.; Richou, J.; Schiele, P.; Hu, W.; Le Nen, D. Radius graft pedicled on the anterior interosseous artery for recurrent ulnar nonunion. Orthop. Traumatol. Surg. Res. 2011, 97, S12–S15. [Google Scholar] [CrossRef] [Green Version]
- Germann, G.; Sauerbier, M.; Steinau, H.U.; Wood, M.B. Reverse segmental pedicled ulna transfer as a salvage procedure in wrist fusion. J. Hand Surg. 2001, 26, 589–592. [Google Scholar] [CrossRef]
- Berezovsky, D.R.; Bordoni, B. Anatomy, Shoulder and Upper Limb, Forearm Arteries. [Updated 2022 Aug 1]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Hubmer, M.G.; Fasching, T.; Haas, F.; Koch, H.; Schwarzl, F.; Weiglein, A.; Scharnagl, E. The posterior interosseous artery in the distal part of the forearm. Is the term ‘recurrent branch of the anterior interosseous artery’ justified? Br. J. Plast. Surg. 2004, 57, 638–644. [Google Scholar] [CrossRef]
- Hu, W.; Martin, D.; Foucher, G.; Baudet, J. Le lambeau interosseux antérieur [Anterior interosseous flap]. Ann. Chir. Plast. Esthet. 1994, 39, 290–300. [Google Scholar]
- Kim, S.; Eichenauer, F.; Asmus, A.; Mutze, S.; Eisenschenk, A.; Honigmann, P. Superselective angiography of the wrist in patients with Kienböck’s disease. BMC Musculoskelet. Disord. 2019, 20, 143. [Google Scholar] [CrossRef] [Green Version]
- Schuind, F.; Eslami, S.; LeDoux, P. Kienböck’s disease. J. Bone Jt. Surg. 2008, 90, 133–139. [Google Scholar] [CrossRef]
- Allan, C.H.; Joshi, A.; Lichtman, D.M. Kienböck’s Disease: Diagnosis and Treatment. J. Am. Acad. Orthop. Surg. 2001, 9, 128–136. [Google Scholar] [CrossRef] [Green Version]
- Lesley, N.; Lichtman, D. Klassifikation und Behandlung des Morbus Kienböck: Eine Ubersicht über die vergangenen 100 Jahre und ein Blick in die Zukunft (Classification and Treatment of Kienböck’s Disease: A Review of the Past 100 Years, and a Look at the Future). Handchir. Mikrochir. Plast. Chir. 2010, 42, 171–176. [Google Scholar] [CrossRef]
- Irisarri, C. Atiologie der Lunatumnekrose (Aetiology of Kienböck’s Disease). Handchir. Mikrochir. Plast. Chir. 2010, 42, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Lichtman, D.M.; Pientka, W.F.; Bain, G.I. Kienböck Disease: A New Algorithm for the 21st Century. J. Wrist Surg. 2016, 06, 002–010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE-Initiative. Das Strengthening the Reporting of Observational Studies in Epidemiology (STROBE-) Statement [The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting of observational studies]. Internist 2008, 49, 688–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lichtman, D.M.; Mack, G.R.; MacDonald, R.I.; Gunther, S.F.; Wilson, J.N. Kienböck’s disease: The role of silicone replacement arthroplasty. J. Bone Joint Surg. Am. 1977, 59, 899–908. [Google Scholar] [CrossRef] [PubMed]
- Hagen, B. Invasive oder nichtinvasive Angiographie? Die Rolle der “klassischen” Katheter-Angiographie [Invasive or noninvasive angiography? The role of “classical” catheter angiography]. Radiologe 1997, 37, 493–500. [Google Scholar] [CrossRef]
- Rabinov, J.D.; Leslie-Mazwi, T.M.; Hirsch, J.A. Diagnostic angiography of the cerebrospinal vasculature. Handb. Clin. Neurol. 2016, 135, 151–163. [Google Scholar] [CrossRef]
- Dubey, P.P.; Chauhan, N.K.; Siddiqui, M.S.; Verma, A.K. Study of vascular supply of lunate and consideration applied to Kienböck disease. Hand Surg. 2011, 16, 9–13. [Google Scholar] [CrossRef]


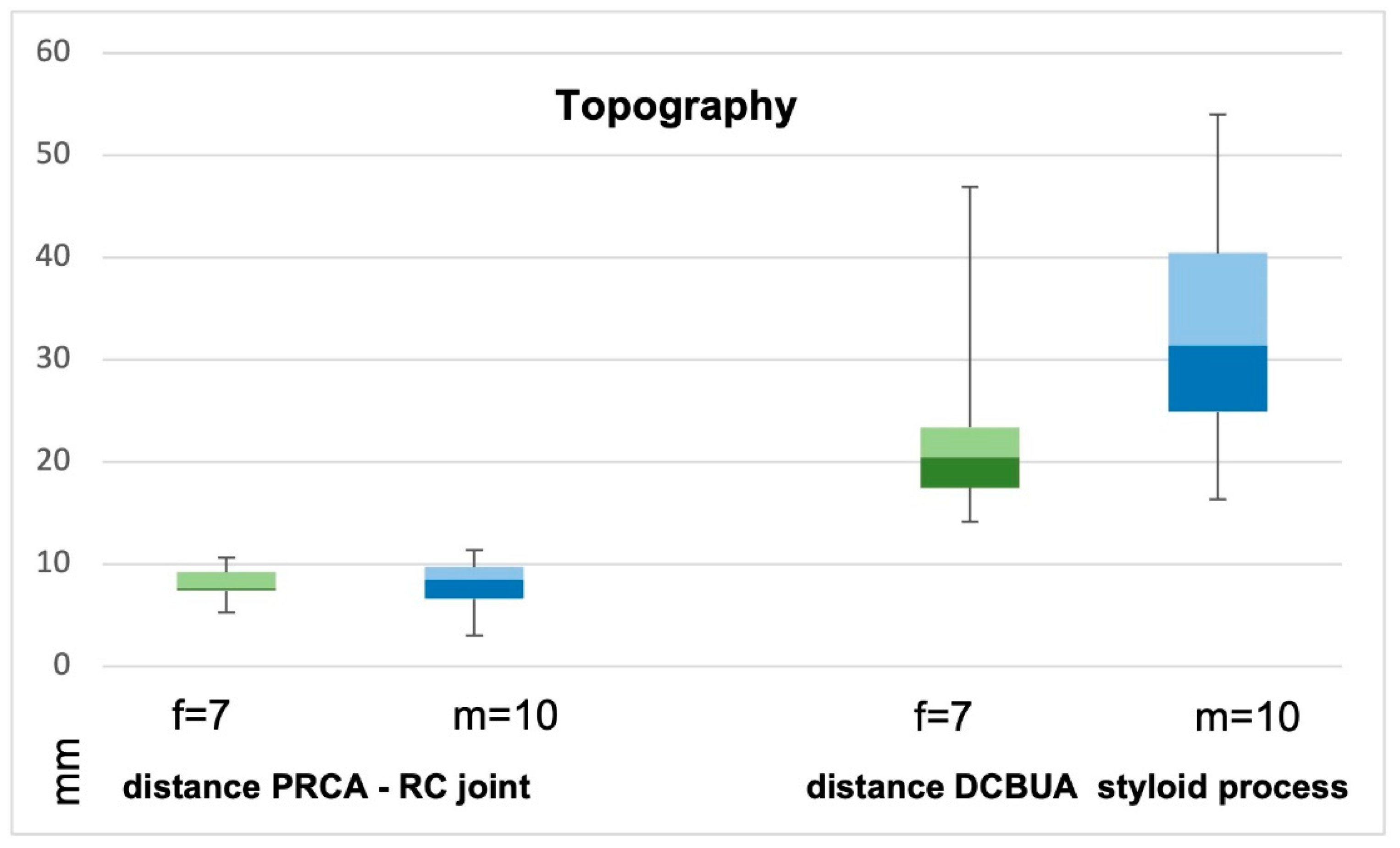
 distance from the DCBUA to the styloid process of the ulnar (DCBUA = dorsal carpal branch of the ulnar artery).
distance from the DCBUA to the styloid process of the ulnar (DCBUA = dorsal carpal branch of the ulnar artery).
distance from the DCBUA to the styloid process of the ulnar (DCBUA = dorsal carpal branch of the ulnar artery).
distance from the DCBUA to the styloid process of the ulnar (DCBUA = dorsal carpal branch of the ulnar artery).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Gender | Disease Stage on MRI | Δ PRCA to Midface Radiocarpal j. (mm) | PRCA Max. Diameter (mm) | Relation RA to PRCA | Δ DCBUA to Styloid Proc. (mm) | DCBUA Max. Diameter (mm) | Relation UA to DCBUA | AIA Max. Diameter (mm) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 2 | 4.1 | 0.4 | 0.25 | 18.5 | 0.6 | 0.22 | 0.5 |
| 2 | M | 3a | 9.3 | 1.0 | 0.32 | 54.0 | 0.9 | 0.32 | 1.7 |
| 3 | M | 3a | 6.6 | 0.5 | 0.14 | 25.2 | 1.5 | 0.38 | 1.3 |
| 4 | M | 3a | 3.0 | 0.5 | 0.2 | 31.6 | 1.2 | 0.56 | 1.3 |
| 5 | M | 3a | 11.4 | 0.8 | 0.33 | 41.4 | 1.2 | 0.33 | 1.6 |
| 6 | M | 3a | 10.6 | 0.6 | 0.19 | 49.3 | 1.6 | 0.45 | 1.0 |
| 7 | M | 3b | 6.5 | 0.5 | 0.2 | 16.3 | 1.2 | 0.65 | 1.0 |
| 8 | M | 3b | 9.6 | 0.8 | 0.29 | 31.2 | 1.4 | 0.43 | 1.4 |
| 9 | M | 3b | 7.6 | 0.3 | 0.15 | 24.8 | 1.7 | 0.64 | 1.1 |
| 10 | M | 4 | 9.7 | 0.8 | 0.3 | 37.4 | 1.2 | 0.37 | 1.2 |
| 11 | F | 2 | 7.5 | 0.6 | 0.22 | 14.1 | 0.8 | 0.54 | 1.1 |
| 12 | F | 3a | 5.3 | 0.3 | 0.16 | 16.9 | 0.6 | 0.28 | 0.8 |
| 13 | F | 3a | 7.3 | 0.5 | 0.23 | 20.4 | 0.5 | 0.28 | 0.9 |
| 14 | F | 3a | 10.0 | 0.6 | 0.24 | 18.0 | 1.5 | 0.45 | 1.8 |
| 15 | F | 3b | 7.7 | 0.5 | 0.26 | 24.2 | 0.8 | 0.5 | 1.1 |
| 16 | F | 3b | 8.4 | 0.7 | 0.3 | 22.6 | 1.3 | 0.43 | 1.1 |
| 17 | F | 3b | 10.1 | 0.3 | 0.21 | 56.9 | 1.5 | 0.45 | 1.0 |
| p-value | F vs. M | 0.96 | 0.36 | 0.96 | 0.11 | 0.27 | 1.0 | 0.32 | |
| p-value | 2/3a vs. 3b/4 | 0.88 | 0.27 | 0.84 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goelz, L.; Kim, S.; Eisenschenk, A.; Mutze, S.; Asmus, A. Superselective Catheter Angiographies of the Wrist (SCAW): Approaches for Vascularized Bone Grafts. Diagnostics 2023, 13, 1198. https://doi.org/10.3390/diagnostics13061198
Goelz L, Kim S, Eisenschenk A, Mutze S, Asmus A. Superselective Catheter Angiographies of the Wrist (SCAW): Approaches for Vascularized Bone Grafts. Diagnostics. 2023; 13(6):1198. https://doi.org/10.3390/diagnostics13061198
Chicago/Turabian StyleGoelz, Leonie, Simon Kim, Andreas Eisenschenk, Sven Mutze, and Ariane Asmus. 2023. "Superselective Catheter Angiographies of the Wrist (SCAW): Approaches for Vascularized Bone Grafts" Diagnostics 13, no. 6: 1198. https://doi.org/10.3390/diagnostics13061198