
The Prognostic Significance of BRAF Gene Analysis in Children and Adolescents with Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Study Outcomes
2.3. Information Sources
2.4. Screening, Data Collection and Analysis
2.5. Quality Assessment of Included Studies
2.6. Measures of Effect
2.7. Data Synthesis
3. Results
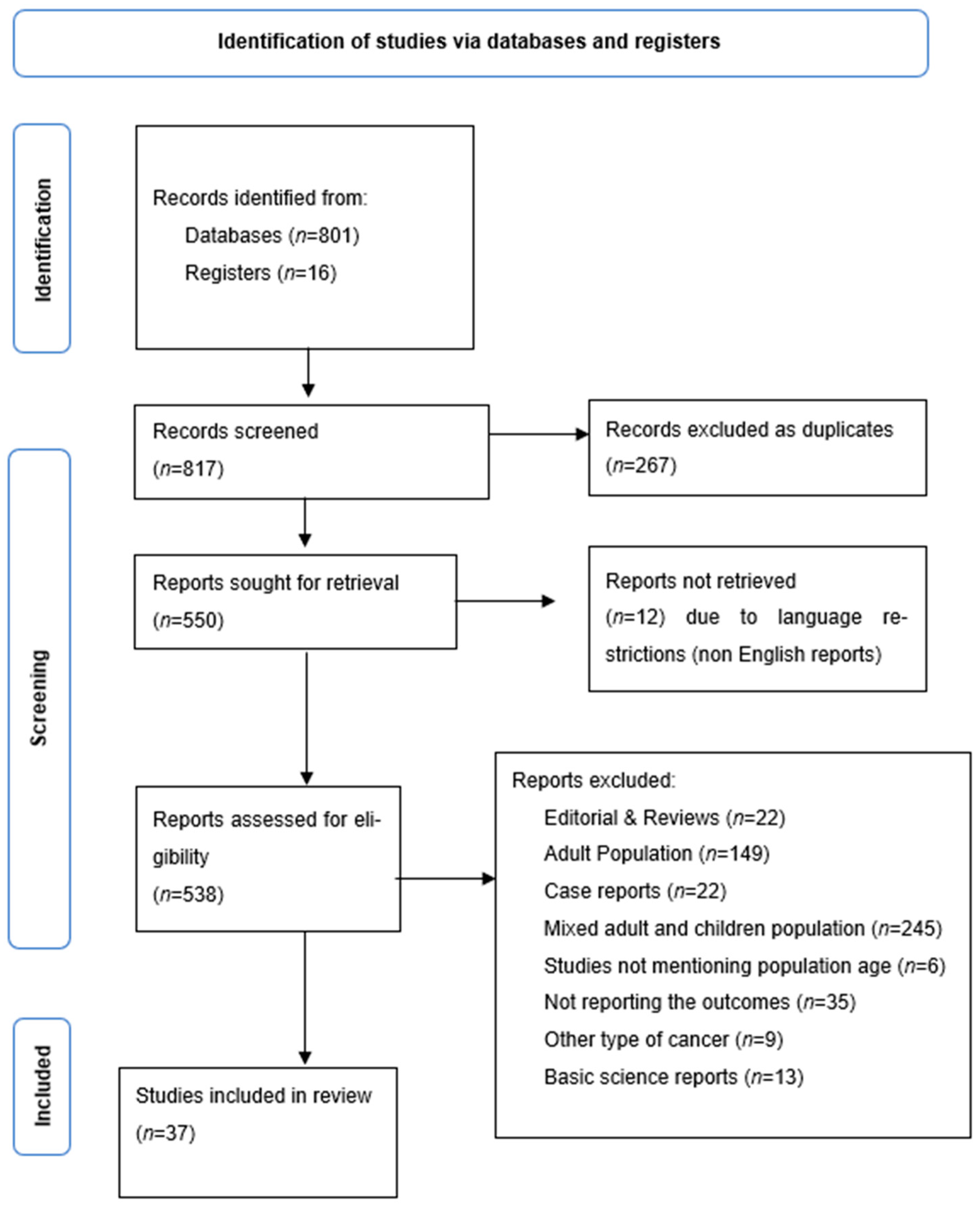
3.1. Study Selection and Characteristics
3.2. Prevalence of BRAF Mutation
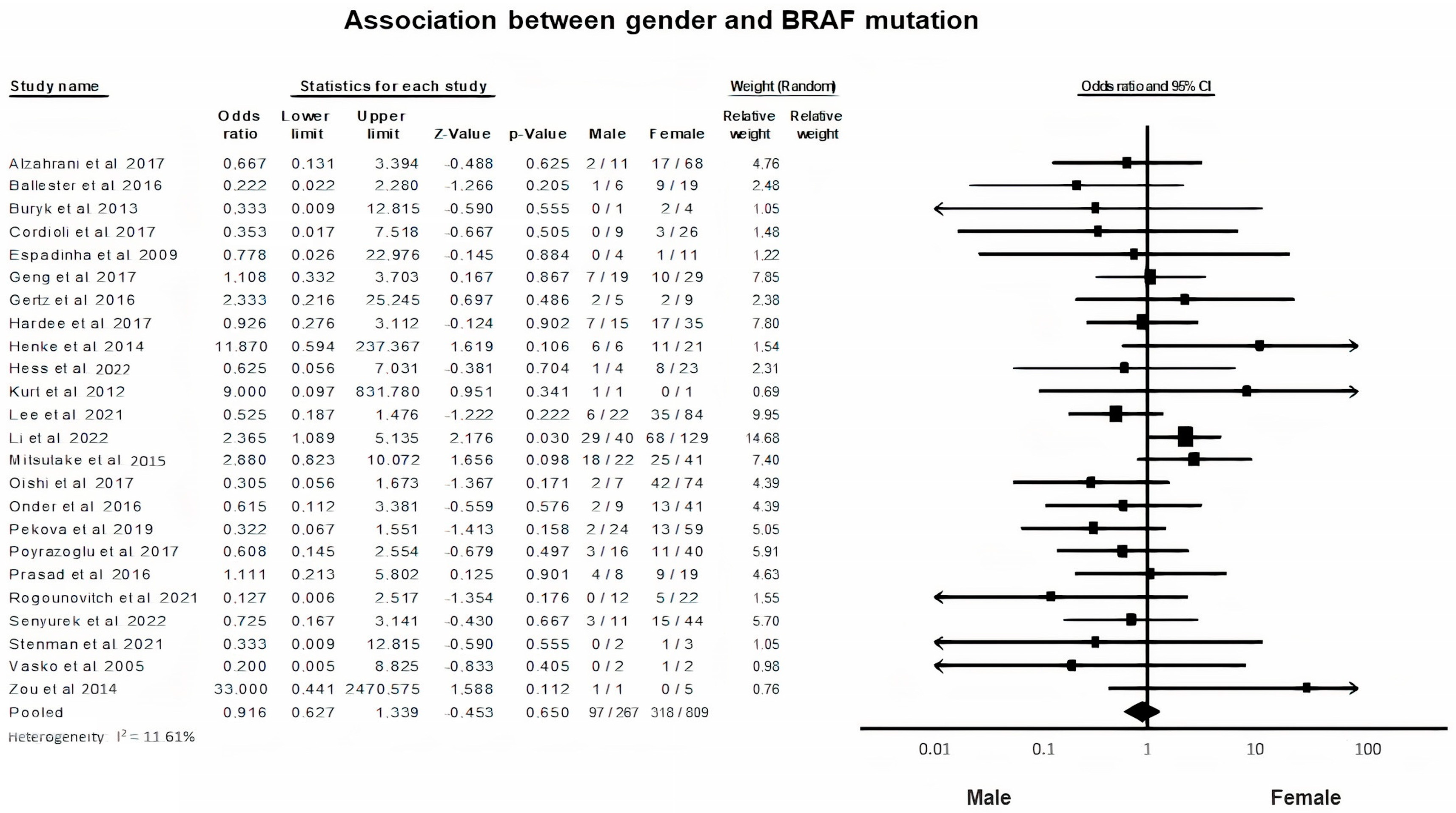
3.3. BRAF Mutation and Gender
3.4. BRAF Mutation and Tumor Size
3.5. BRAF Mutation and Multifocality
3.6. BRAF Mutation and Vascular Invasion
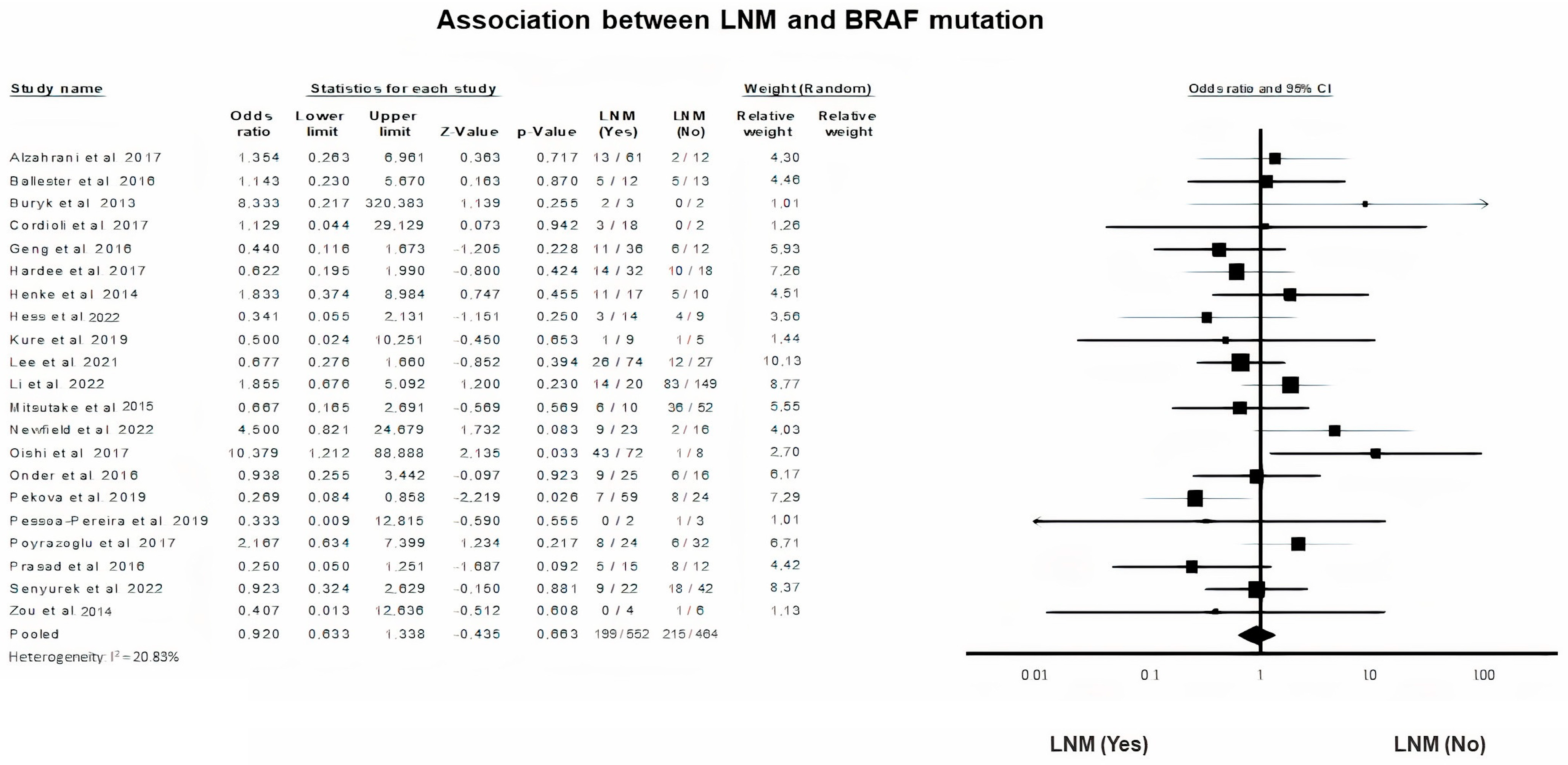
3.7. BRAF Mutation and Lymph Node Metastasis (LNM)
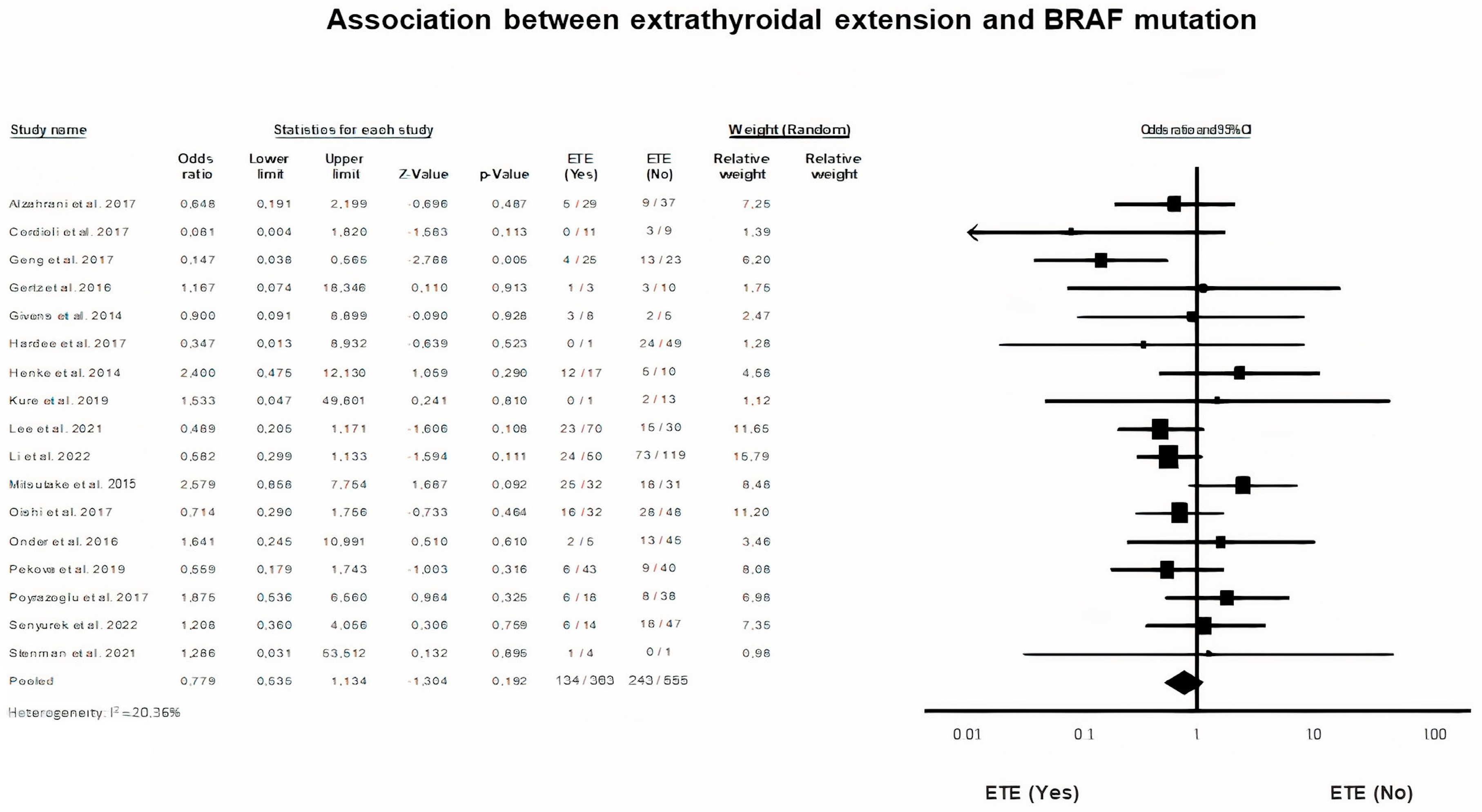
3.8. BRAF Mutation and Extrathyroidal Extension (ETE)
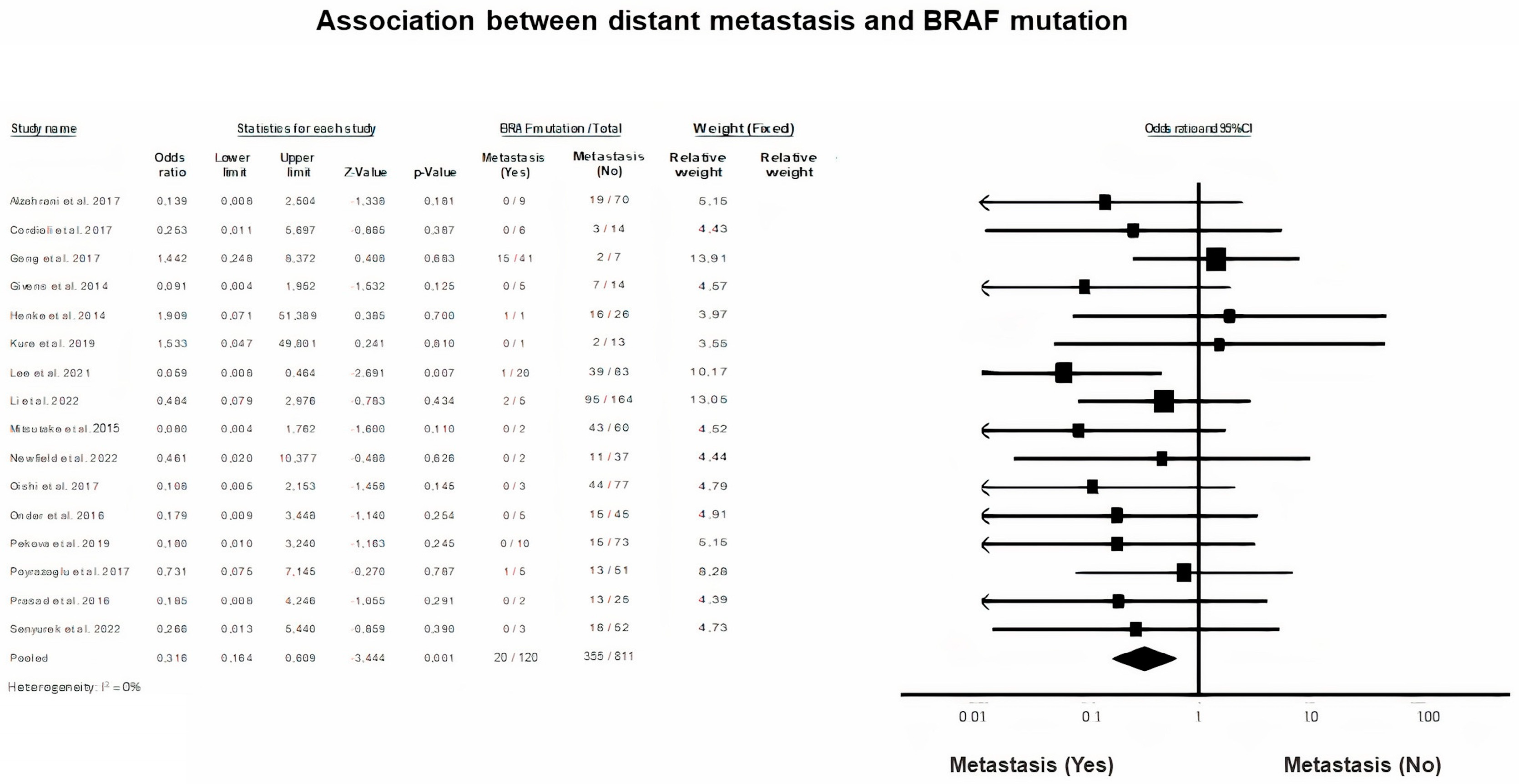
3.9. Distant Metastasis in BRAF Mutation
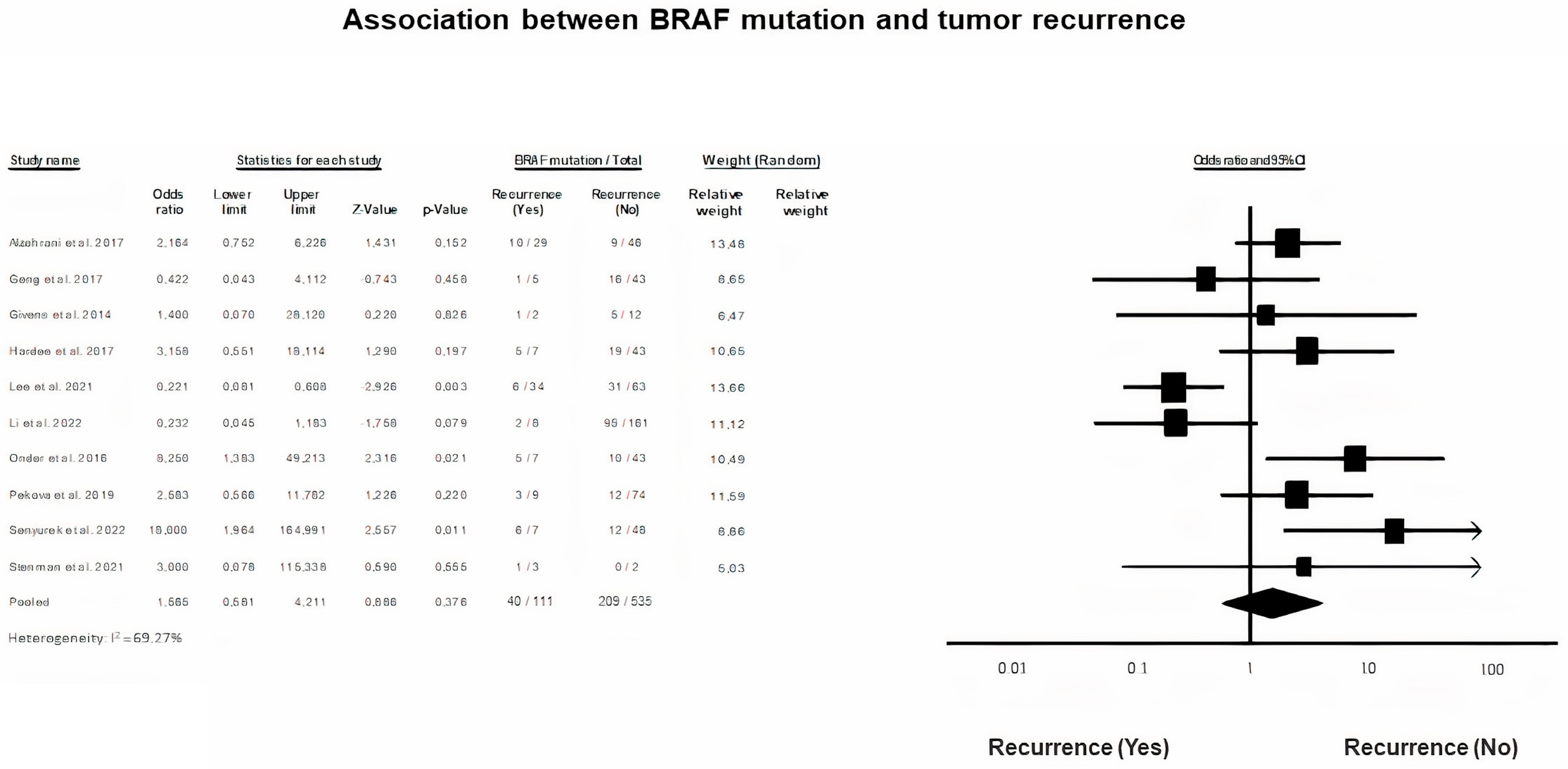
3.10. Tumor Recurrence and BRAF Mutation
3.11. BRAF Mutation and Survival Rate
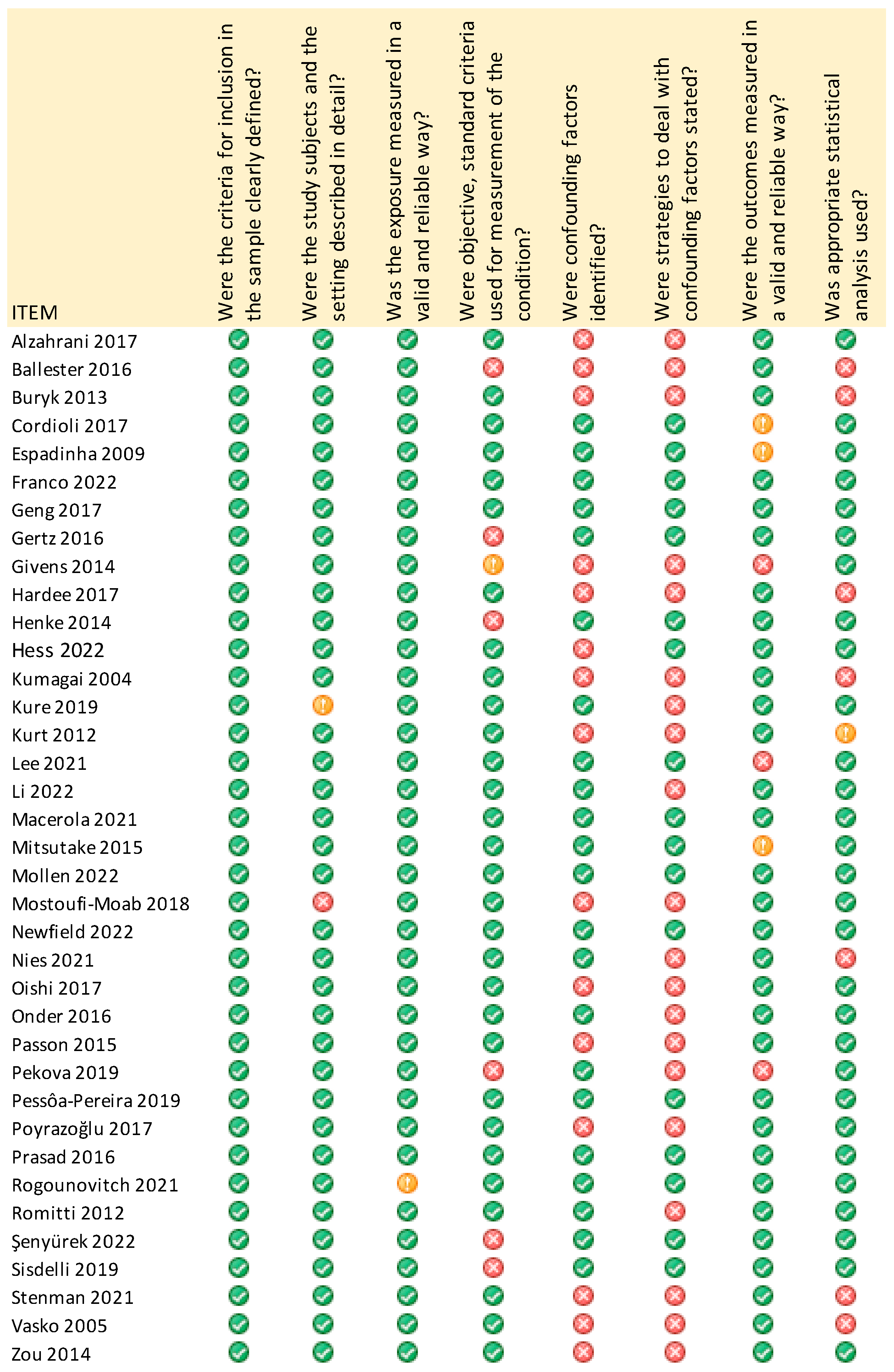
3.12. Assessment of Quality and Biases of the Included Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Francis, G.L.; Waguespack, S.G.; Bauer, A.J.; Angelos, P.; Benvenga, S.; Cerutti, J.M.; Dinauer, C.A.; Hamilton, J.; Hay, I.D.; Luster, M.; et al. Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2015, 25, 716–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaccarella, S.; Lortet-Tieulent, J.; Colombet, M.; Davies, L.; Stiller, C.A.; Schüz, J.; Togawa, K.; Bray, F.; Franceschi, S.; Dal Maso, L.; et al. Global Patterns and Trends in Incidence and Mortality of Thyroid Cancer in Children and Adolescents: A Population-Based Study. Lancet Diabetes Endocrinol. 2021, 9, 144–152. [Google Scholar] [CrossRef]
- Bernier, M.O.; Withrow, D.R.; Berrington de Gonzalez, A.; Lam, C.J.K.; Linet, M.S.; Kitahara, C.M.; Shiels, M.S. Trends in Pediatric Thyroid Cancer Incidence in the United States, 1998–2013. Cancer 2019, 125, 2497–2505. [Google Scholar] [CrossRef] [PubMed]
- Rangel-Pozzo, A.; Sisdelli, L.; Cordioli, M.I.V.; Vaisman, F.; Caria, P.; Mai, S.; Cerutti, J.M. Genetic Landscape of Papillary Thyroid Carcinoma and Nuclear Architecture: An Overview Comparing Pediatric and Adult Populations. Cancers 2020, 12, 3146. [Google Scholar] [CrossRef]
- Zhang, B.; Wu, W.; Shang, X.; Huang, D.; Liu, M.; Zong, L. Incidence and Prognosis of Thyroid Cancer in Children: Based on the SEER Database. Pediatr. Surg. Int. 2022, 38, 445–456. [Google Scholar] [CrossRef] [PubMed]
- Tufano, R.P.; Teixeira, G.V.; Bishop, J.; Carson, K.A.; Xing, M. BRAF Mutation in Papillary Thyroid Cancer and Its Value in Tailoring Initial Treatment: A Systematic Review and Meta-Analysis. Medicine 2012, 91, 274–286. [Google Scholar] [CrossRef]
- Li, C.; Lee, K.C.; Schneider, E.B.; Zeiger, M.A. BRAF V600E Mutation and Its Association with Clinicopathological Features of Papillary Thyroid Cancer: A Meta-Analysis. J. Clin. Endocrinol. Metab. 2012, 97, 4559–4570. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Chen, J.Q.; Liu, J.L.; Qin, X.G. Clinical Impact of BRAF Mutation on the Diagnosis and Prognosis of Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis. Eur. J. Clin. Investig. 2016, 46, 146–157. [Google Scholar] [CrossRef]
- Song, J.Y.; Sun, S.R.; Dong, F.; Huang, T.; Wu, B.; Zhou, J. Predictive Value of BRAFV600E Mutation for Lymph Node Metastasis in Papillary Thyroid Cancer: A Meta-Analysis. Curr. Med. Sci. 2018, 38, 785–797. [Google Scholar] [CrossRef]
- Wei, X.; Wang, X.; Xiong, J.; Li, C.; Liao, Y.; Zhu, Y.; Mao, J. Risk and Prognostic Factors for BRAFV600E Mutations in Papillary Thyroid Carcinoma. Biomed. Res. Int. 2022, 2022, 9959649. [Google Scholar] [CrossRef]
- Kumagai, A.; Namba, H.; Saenko, V.A.; Ashizawa, K.; Ohtsuru, A.; Ito, M.; Ishikawa, N.; Sugino, K.; Ito, K.; Jeremiah, S.; et al. Low Frequency of BRAFT1796A Mutations in Childhood Thyroid Carcinomas. J. Clin. Endocrinol. Metab. 2004, 89, 4280–4284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henke, L.E.; Perkins, S.M.; Pfeifer, J.D.; Ma, C.; Chen, Y.; Dewees, T.; Grigsby, P.W. BRAF V600E Mutational Status in Pediatric Thyroid Cancer. Pediatr. Blood Cancer 2014, 61, 1168–1172. [Google Scholar] [CrossRef] [PubMed]
- Givens, D.J.; Buchmann, L.O.; Agarwal, A.M.; Grimmer, J.F.; Hunt, J.P. BRAF V600E Does Not Predict Aggressive Features of Pediatric Papillary Thyroid Carcinoma. Laryngoscope 2014, 124, E389–E393. [Google Scholar] [CrossRef] [PubMed]
- Prasad, M.L.; Vyas, M.; Horne, M.J.; Virk, R.K.; Morotti, R.; Liu, Z.; Tallini, G.; Nikiforova, M.N.; Christison-Lagay, E.R.; Udelsman, R.; et al. NTRK Fusion Oncogenes in Pediatric Papillary Thyroid Carcinoma in Northeast United States. Cancer 2016, 122, 1097–1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gertz, R.J.; Nikiforov, Y.; Rehrauer, W.; McDaniel, L.; Lloyd, R.V. Mutation in BRAF and Other Members of the MAPK Pathway in Papillary Thyroid Carcinoma in the Pediatric Population. Arch. Pathol. Lab Med. 2016, 140, 134–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cordioli, M.I.C.V.; Moraes, L.; Bastos, A.U.; Besson, P.; de Alves, M.T.S.; Delcelo, R.; Monte, O.; Longui, C.; Cury, A.N.; Cerutti, J.M. Fusion Oncogenes Are the Main Genetic Events Found in Sporadic Papillary Thyroid Carcinomas from Children. Thyroid 2017, 27, 182–188. [Google Scholar] [CrossRef]
- Alzahrani, A.S.; Murugan, A.K.; Qasem, E.; Alswailem, M.; Al-Hindi, H.; Shi, Y. Single Point Mutations in Pediatric Differentiated Thyroid Cancer. Thyroid 2017, 27, 189–196. [Google Scholar] [CrossRef]
- Geng, J.; Wang, H.; Liu, Y.; Tai, J.; Jin, Y.; Zhang, J.; He, L.; Fu, L.; Qin, H.; Song, Y.; et al. Correlation between BRAF V600E Mutation and Clinicopathological Features in Pediatric Papillary Thyroid Carcinoma. Sci. China Life Sci. 2017, 60, 729–738. [Google Scholar] [CrossRef]
- Mostoufi-Moab, S.; Labourier, E.; Sullivan, L.; Livolsi, V.; Li, Y.; Xiao, R.; Beaudenon-Huibregtse, S.; Kazahaya, K.; Scott Adzick, N.; Baloch, Z.; et al. Molecular Testing for Oncogenic Gene Alterations in Pediatric Thyroid Lesions. Thyroid 2018, 28, 60–67. [Google Scholar] [CrossRef]
- Hardee, S.; Prasad, M.L.; Hui, P.; Dinauer, C.A.; Morotti, R.A. Pathologic Characteristics, Natural History, and Prognostic Implications of BRAFV600E Mutation in Pediatric Papillary Thyroid Carcinoma. Pediatr. Dev. Pathol. 2017, 20, 206–212. [Google Scholar] [CrossRef]
- Lebbink, C.A.; Links, T.P.; Czarniecka, A.; Dias, R.P.; Elisei, R.; Izatt, L.; Krude, H.; Lorenz, K.; Luster, M.; Newbold, K.; et al. 2022 European Thyroid Association Guidelines for the Management of Pediatric Thyroid Nodules and Differentiated Thyroid Carcinoma. Eur. Thyroid J. 2022, 11, e220146. [Google Scholar] [CrossRef] [PubMed]
- Poulikakos, P.I.; Sullivan, R.J.; Yaeger, R. Molecular Pathways and Mechanisms of BRAF in Cancer Therapy. Clin. Cancer Res. 2022, 28, 4618–4628. [Google Scholar] [CrossRef]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic Reviews of Etiology and Risk. In JBI Manual for Evidence Synthesis; JBI: North Adelaide, SA, Australia, 2020. [Google Scholar] [CrossRef]
- Ballester, L.Y.; Sarabia, S.F.; Sayeed, H.; Patel, N.; Baalwa, J.; Athanassaki, I.; Hernandez, J.A.; Fang, E.; Quintanilla, N.M.; Roy, A.; et al. Integrating Molecular Testing in the Diagnosis and Management of Children with Thyroid Lesions. Pediatr. Dev. Pathol. 2016, 19, 94–100. [Google Scholar] [CrossRef]
- Buryk, M.A.; Monaco, S.E.; Witchel, S.F.; Mehta, D.K.; Gurtunca, N.; Nikiforov, Y.E.; Simons, J.P. Preoperative Cytology with Molecular Analysis to Help Guide Surgery for Pediatric Thyroid Nodules. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 1697–1700. [Google Scholar] [CrossRef] [PubMed]
- Espadinha, C.; Santos, J.R.; Sobrinho, L.G.; Bugalho, M.J. Expression of Iodine Metabolism Genes in Human Thyroid Tissues: Evidence for Age and BRAFV600E Mutation Dependency. Clin. Endocrinol. 2009, 70, 629–635. [Google Scholar] [CrossRef]
- Franco, A.T.; Ricarte-Filho, J.C.; Isaza, A.; Jones, Z.; Jain, N.; Mostoufi-Moab, S.; Surrey, L.; Laetsch, T.W.; Li, M.M.; DeHart, J.C.; et al. Fusion Oncogenes Are Associated With Increased Metastatic Capacity and Persistent Disease in Pediatric Thyroid Cancers. J. Clin. Oncol. 2022, 40, 1081–1090. [Google Scholar] [CrossRef] [PubMed]
- Hess, J.R.; Newbern, D.K.; Beebe, K.L.; Walsh, A.M.; Schafernak, K.T. High Prevalence of Gene Fusions and Copy Number Alterations in Pediatric Radiation Therapy-Induced Papillary and Follicular Thyroid Carcinomas. Thyroid 2022, 32, 411–420. [Google Scholar] [CrossRef]
- Kure, S.; Ishino, K.; Kudo, M.; Wada, R.; Saito, M.; Nagaoka, R.; Sugitani, I.; Naito, Z. Incidence of BRAF V600E Mutation in Patients with Papillary Thyroid Carcinoma: A Single-Institution Experience. J. Int. Med. Res. 2019, 47, 5560–5572. [Google Scholar] [CrossRef] [Green Version]
- Kurt, B.; YalçIn, S.; Alagöz, E.; KarslIoǧlu, Y.; Yigit, N.; Günal, A.; Deveci, M.S. The Relationship of the BRAF(V600E) Mutation and the Established Prognostic Factors in Papillary Thyroid Carcinomas. Endocr. Pathol. 2012, 23, 135–140. [Google Scholar] [CrossRef]
- Lee, Y.A.; Lee, H.; Im, S.W.; Song, Y.S.; Oh, D.Y.; Kang, H.J.; Won, J.K.; Jung, K.C.; Kwon, D.; Chung, E.J.; et al. NTRK and RET Fusion-Directed Therapy in Pediatric Thyroid Cancer Yields a Tumor Response and Radioiodine Uptake. J. Clin. Investig. 2021, 131, e144847. [Google Scholar] [CrossRef]
- Macerola, E.; Proietti, A.; Poma, A.M.; Ugolini, C.; Torregrossa, L.; Vignali, P.; Basolo, A.; Materazzi, G.; Elisei, R.; Santini, F.; et al. Molecular Alterations in Relation to Histopathological Characteristics in a Large Series of Pediatric Papillary Thyroid Carcinoma from a Single Institution. Cancers 2021, 13, 3123. [Google Scholar] [CrossRef] [PubMed]
- Mitsutake, N.; Fukushima, T.; Matsuse, M.; Rogounovitch, T.; Saenko, V.; Uchino, S.; Ito, M.; Suzuki, K.; Suzuki, S.; Yamashita, S. BRAFV600E Mutation Is Highly Prevalent in Thyroid Carcinomas in the Young Population in Fukushima: A Different Oncogenic Profile from Chernobyl. Sci. Rep. 2015, 5, 16976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mollen, K.P.; Shaffer, A.D.; Yip, L.; Monaco, S.E.; Huyett, P.; Viswanathan, P.; Witchel, S.F.; Duvvuri, U.; Simons, J.P. Unique Molecular Signatures Are Associated with Aggressive Histology in Pediatric Differentiated Thyroid Cancer. Thyroid 2022, 32, 236–244. [Google Scholar] [CrossRef]
- Newfield, R.S.; Jiang, W.; Sugganth, D.X.; Hantash, F.M.; Lee, E.; Newbury, R.O. Mutational Analysis Using next Generation Sequencing in Pediatric Thyroid Cancer Reveals BRAF and Fusion Oncogenes Are Common. Int. J. Pediatr. Otorhinolaryngol. 2022, 157, 111121. [Google Scholar] [CrossRef] [PubMed]
- Nies, M.; Vassilopoulou-Sellin, R.; Bassett, R.L.; Yedururi, S.; Zafereo, M.E.; Cabanillas, M.E.; Sherman, S.I.; Links, T.P.; Waguespack, S.G. Distant Metastases From Childhood Differentiated Thyroid Carcinoma: Clinical Course and Mutational Landscape. J. Clin. Endocrinol. Metab. 2021, 106, E1683–E1697. [Google Scholar] [CrossRef]
- Oishi, N.; Kondo, T.; Nakazawa, T.; Mochizuki, K.; Inoue, T.; Kasai, K.; Tahara, I.; Yabuta, T.; Hirokawa, M.; Miyauchi, A.; et al. Frequent BRAF V600E and Absence of TERT Promoter Mutations Characterize Sporadic Pediatric Papillary Thyroid Carcinomas in Japan. Endocr. Pathol. 2017, 28, 103–111. [Google Scholar] [CrossRef]
- Onder, S.; Ozturk Sari, S.; Yegen, G.; Sormaz, I.C.; Yilmaz, I.; Poyrazoglu, S.; Sanlı, Y.; Giles Senyurek, Y.; Kapran, Y.; Mete, O. Classic Architecture with Multicentricity and Local Recurrence, and Absence of TERT Promoter Mutations Are Correlates of BRAF (V600E) Harboring Pediatric Papillary Thyroid Carcinomas. Endocr. Pathol. 2016, 27, 153–161. [Google Scholar] [CrossRef]
- Passon, N.; Bregant, E.; Sponziello, M.; Dima, M.; Rosignolo, F.; Durante, C.; Celano, M.; Russo, D.; Filetti, S.; Damante, G. Somatic Amplifications and Deletions in Genome of Papillary Thyroid Carcinomas. Endocrine 2015, 50, 453–464. [Google Scholar] [CrossRef]
- Pekova, B.; Dvorakova, S.; Sykorova, V.; Vacinova, G.; Vaclavikova, E.; Moravcova, J.; Katra, R.; Vlcek, P.; Sykorova, P.; Kodetova, D.; et al. Somatic Genetic Alterations in a Large Cohort of Pediatric Thyroid Nodules. Endocr. Connect 2019, 8, 796. [Google Scholar] [CrossRef] [Green Version]
- Pessôa-Pereira, D.; da Medeiros, M.F.S.; Lima, V.M.S.; da Silva, J.C.; de Cerqueira, T.L.O.; da Silva, I.C.; Fonseca, L.E.; Sampaio, L.J.L.; de Lima, C.R.A.; Ramos, H.E. Association between BRAF (V600E) Mutation and Clinicopathological Features of Papillary Thyroid Carcinoma: A Brazilian Single-Centre Case Series. Arch. Endocrinol. Metab. 2019, 63, 97–106. [Google Scholar] [CrossRef]
- Poyrazoğlu, Ş.; Bundak, R.; Baş, F.; Yeğen, G.; Şanlı, Y.; Darendeliler, F. Clinicopathological Characteristics of Papillary Thyroid Cancer in Children with Emphasis on Pubertal Status and Association with BRAFV600E Mutation. J. Clin. Res. Pediatr. Endocrinol. 2017, 9, 185–193. [Google Scholar] [CrossRef] [Green Version]
- Rogounovitch, T.I.; Mankovskaya, S.V.; Fridman, M.V.; Leonova, T.A.; Kondratovitch, V.A.; Konoplya, N.E.; Yamashita, S.; Mitsutake, N.; Saenko, V.A. Major Oncogenic Drivers and Their Clinicopathological Correlations in Sporadic Childhood Papillary Thyroid Carcinoma in Belarus. Cancers 2021, 13, 3374. [Google Scholar] [CrossRef]
- Romitti, M.; Wajner, S.M.; Zennig, N.; Goemann, I.M.; Bueno, A.L.; Meyer, E.L.S.; Maia, A.L. Increased Type 3 Deiodinase Expression in Papillary Thyroid Carcinoma. Thyroid 2012, 22, 897–904. [Google Scholar] [CrossRef] [PubMed]
- Şenyürek, Y.G.; İşcan, Y.; Sormaz, İ.C.; Poyrazoğlu, Ş.; Tunca, F. The Role of American Thyroid Association Pediatric Thyroid Cancer Risk Stratification and BRAFV600E Mutation in Predicting the Response to Treatment in Papillary Thyroid Cancer Patients ≤18 Years Old. J. Clin. Res. Pediatr. Endocrinol. 2022, 14, 196. [Google Scholar] [CrossRef] [PubMed]
- Sisdelli, L.; Cordioli, M.I.C.V.; Vaisman, F.; Moraes, L.; Colozza-Gama, G.A.; Alves, P.A.G.; Araújo, M.L.; Alves, M.T.S.; Monte, O.; Longui, C.A.; et al. AGK-BRAF Is Associated with Distant Metastasis and Younger Age in Pediatric Papillary Thyroid Carcinoma. Pediatr. Blood Cancer 2019, 66, e27707. [Google Scholar] [CrossRef]
- Stenman, A.; Backman, S.; Johansson, K.; Paulsson, J.O.; Stålberg, P.; Zedenius, J.; Christofer Juhlin, C. Pan-Genomic Characterization of High-Risk Pediatric Papillary Thyroid Carcinoma. Endocr. Relat. Cancer 2021, 28, 337. [Google Scholar] [CrossRef] [PubMed]
- Vasko, V.; Hu, S.; Wu, G.; Xing, J.C.; Larin, A.; Savchenko, V.; Trink, B.; Xing, M. High Prevalence and Possible de Novo Formation of BRAF Mutation in Metastasized Papillary Thyroid Cancer in Lymph Nodes. J. Clin. Endocrinol. Metab. 2005, 90, 5265–5269. [Google Scholar] [CrossRef] [Green Version]
- Zou, M.; Baitei, E.Y.; Alzahrani, A.S.; Binhumaid, F.S.; Alkhafaji, D.; Al-Rijjal, R.A.; Meyer, B.F.; Shi, Y. Concomitant RAS, RET/PTC, or BRAF Mutations in Advanced Stage of Papillary Thyroid Carcinoma. Thyroid 2014, 24, 1256–1266. [Google Scholar] [CrossRef] [Green Version]
- Celik, M.; Bulbul, B.Y.; Ayturk, S.; Durmus, Y.; Gurkan, H.; Can, N.; Tastekin, E.; Ustun, F.; Sezer, A.; Guldiken, S. The Relation between BRAFV600E Mutation and Clinicopathological Characteristics of Papillary Thyroid Cancer. Med. Glas (Zenica) 2020, 17, 30–34. [Google Scholar] [CrossRef]
- Jung, Y.Y.; Yoo, J.H.; Park, E.S.; Kim, M.K.; Lee, T.J.; Cho, B.Y.; Chung, Y.J.; Kang, K.H.; Ahn, H.Y.; Kim, H.S. Clinicopathologic Correlations of the BRAFV600E Mutation, BRAF V600E Immunohistochemistry, and BRAF RNA in Situ Hybridization in Papillary Thyroid Carcinoma. Pathol. Res. Pract. 2015, 211, 162–170. [Google Scholar] [CrossRef]
- Iwadate, M.; Mitsutake, N.; Matsuse, M.; Fukushima, T.; Suzuki, S.; Matsumoto, Y.; Ookouchi, C.; Mizunuma, H.; Nakamura, I.; Nakano, K.; et al. The Clinicopathological Results of Thyroid Cancer With BRAFV600E Mutation in the Young Population of Fukushima. J. Clin. Endocrinol. Metab. 2020, 105, dgaa573. [Google Scholar] [CrossRef] [PubMed]
- Hogan, A.R.; Zhuge, Y.; Perez, E.A.; Koniaris, L.G.; Lew, J.I.; Sola, J.E. Pediatric Thyroid Carcinoma: Incidence and Outcomes in 1753 Patients. J. Surg. Res. 2009, 156, 167–172. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No | Authors, Year | Study Type | Recruitment (Country, Time) | Sample Size (n) | Sample Origin | Age (Years) | Gender (Boys/Girls) | BRAF Mutations Prevalence (%) | |
|---|---|---|---|---|---|---|---|---|---|
| BRAF V600E | Other | ||||||||
| 1 | Alzahrani [17], 2017 | RC | Middle East, 1998–2015 | 79 | registry | 8–18 | 11/68 | 24 | |
| 2 | Ballester [24], 2016 | RCrS | USA, 2009–2014 | 25 | clinical | 10–19 | 6/19 | 40 | |
| 3 | Buryk [25], 2013 | RCaS | USA, 2009–2012 | 5 | clinical | 12–15 | 1/4 | 40 | |
| 4 | Cordioli [16], 2017 | RC | Brazil, NR | 35 | clinical | 4–18 | 9/26 | 8.6 | |
| 5 | Espadinha [26], 2009 | C | Portugal, 2000–2007 | 15 | clinical | 5–21 | 4/11 | 7 | |
| 6 | Franko [27], 2022 | RC | USA, 1989–2019 | 122 | clinical | <18 | NR | 21.3 | 0.75 (T599del) |
| 7 | Geng [18], 2017 | RC | China, 1994–2014 | 48 | clinical | 3–14 | 19/29 | 35.4 | |
| 8 | Gertz [15], 2016 | RCrS | USA, 2008–2012 | 14 | registry | 8–18 | 5/9 | 31 | 7 (c.1799_1801delTGA) |
| 9 | Givens [13], 2014 | RCrS | USA, 1999–2012 | 19 | registry | 3–18 | NR | 36.8 | |
| 10 | Hardee [20], 2017 | RCrS | USA, 2003–2015 | 50 | registry | <21 | 15/35 | 48 | |
| 11 | Henke [12], 2014 | RCrs | USA, 1973–2005 | 27 | registry | 6–21 | 6/21 | 63 | |
| 12 | Hess [28], 2022 | RCrS | USA, 2010–2019 | 27 | clinical | 9.1–18.7 | 4/23 | 33.3 | |
| 13 | Kumagai [11], 2004 | C | Japan/Ukraine, 1962–1995 | 44 | registry | <17 | NR | 6.81 (T1796A) | |
| 14 | Kure [29], 2019 | RC | Japan, 2009–2017 | 14 | registry | 13–21 | 0/14 | 14.3 | |
| 15 | Kurt [30], 2012 | C | Turkey, 1995–2010 | 2 | registry | 14–20 | 1/1 | 50 | |
| 16 | Lee [31], 2021 | RCrS | Korea, 1983–2020 | 106 | clinical/registry | 4.3–19.8 | 22/ 84 | 38.7 | |
| 17 | Li [7], 2022 | RC | China, 2018–2021 | 169 | clinical | 6–18 | 40/129 | 57.4 | |
| 18 | Macerola [32], 2021 | RC | Italy, 2014–2020 | 163 | registry | 8–18 | 47/116 | 36.2 | 0.6 (K599I) |
| 19 | Mitsutake [33], 2015 | RC | Japan, 2013–2014 | 67 | clinical | 9–22 | NR | 64.2 | |
| 20 | Mollen [34], 2022 | RCrS | USA, 2001–2017 | 62 | clinical | 4.2–18.9 | 47/15 | 30.6 | |
| 21 | Mostufi-Moab [19], 2018 | RCrS | USA, 1989–2012 | 62 | registry | 2–18 | NR | 19.4 | |
| 22 | Newfield [35], 2022 | RC | USA, 2001–2015 | 39 | registry | <18 | NR | 28.2 | 2.6 (K601E) |
| 23 | Nies [36], 2021 | RC | USA, 1946–2019 | 94 | registry | 10–16 | NR | 8.5 | |
| 24 | Oishi [37], 2017 | CC | Japan, 1991–2013 | 81 | registry | 6–20 | 7/74 | 54 | |
| 25 | Onder [38], 2016 | RC | Turkey, 1995–2015 | 50 | registry | 6–18 | 9/41 | 30 | |
| 26 | Passon [39], 2015 | RC | Italy, NR | 2 | clinical | 17–19 | 0/2 | 0 | |
| 27 | Pekova [40], 2019 | RC | Czech Rep, 2003–2017 | 83 | clinical | 14.2 ± 3.4 | 24/59 | 18.1 | |
| 28 | Pessôa-Pereira [41], 2019 | RC | Brazil, 2006–2012 | 5 | registry | 12–20 | 0/5 | 20 | |
| 29 | Poyrazoglu [42], 2017 | RC | Turkey, 1983–2015 | 75 | clinical | 1.3–17.8 | 24/51 | 25 | |
| 30 | Prasad ML [14], 2016 | RCrS | USA, 2009–2015 | 28 | clinical | 6–18 | 8/20 | 48 | |
| 31 | Rogounovitch [43], 2021 | RC | Belarus, 2001–2007 | 34 | registry | 4–14 | 12/22 | 14.7 | 0 (K601E) |
| 32 | Romittii [44], 2012 | RCrS | Brazil, NR | 3 | registry | 10–18 | 0/3 | 0 | |
| 33 | Şenyürek [45], 2022 | RC | Turkey, 1995–2020 | 55 | registry | 5–18 | 15/55 | 33 | |
| 34 | Sisdeli L [46], 2019 | RC | Brazil, 1993–2017 | 80 | registry | <18 | NR | 15 | |
| 35 | Stenman [47], 2021 | RC | Sweden, 1992–2021 | 5 | registry | 9–15 | 2/3 | 20 | |
| 36 | Vasko V [48], 2005 | RCrS | Ukraine, 1999–2004 | 4 | clinical | 14–20 | 2/2 | 25 | |
| 37 | Zou M [49], 2014 | RC | Saudi Arabia, 1987–2006 | 6 | clinical | 12–21 | 1/5 | 16.7 | |
| No | Author, Year | Total Study Sample (n) | BRAF Mutation Status (+/−) | Sample per BRAF Group (n) | Tumor Size (cm) or (f*) | Multifocality (%) | Vascular Invasion (%) | LNM (%) | ETE (%) | DM (%) | Tumor Recurrence (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Alzahrani [17], 2017 | 79 | + | 19 | 2.8 ± 1.4 | 50 | 40 | 86.7 | 35.7 | 0 | 52.6 |
| − | 60 | 3.3 ± 1.6 | 53.8 | 51.4 | 82.8 | 46.2 | 15 | 33.9 | |||
| 2 | Ballester [24], 2016 | 25 | + | 10 | NR | NR | NR | 50 | NR | NR | NR |
| − | 15 | NR | NR | NR | 46.7 | NR | NR | NR | |||
| 3 | Buryk [25], 2013 | 5 | + | 2 | 2.7 ± 0.56 | NR | NR | 100 | NR | NR | NR |
| − | 3 | 1.7 ± 0.17 | NR | NR | 33.3 | NR | NR | NR | |||
| 4 | Cordioli [16], 2017 | 35 | + | 3 | 4.6 ± 1.25 | NR | NR | 100 | 0 | 0 | NR |
| − | 16 | 2.9 ± 1.48 | NR | NR | 88.2 | 64.7 | 35.2 | NR | |||
| 5 | Espadinha [26], 2009 | 15 | + | 1 | NR | NR | NR | 0 | NR | NR | NR |
| − | 14 | NR | NR | NR | NR | NR | NR | NR | |||
| 6 | Franko [27], 2022 | 122 | + | 26 | * <2 cm = 11, 2–4 cm = 5, >4 cm = 10 | NR | 30.7 | 72 | 46.1 | 0 | NR |
| − | 96 | NR | NR | NR | NR | NR | NR | NR | |||
| 7 | Geng [18], 2017 | 48 | + | 17 | * <2 cm = 2, 2–4 cm = 11, >4 cm = 4 | 20 | NR | 64.7 | 16.0 | 36.6 | 20 |
| − | 31 | * 2–4 cm = 17, >4 cm = 14 | 80 | NR | 80.6 | 84.0 | 63.4 | 80 | |||
| 8 | Gertz [15], 2016 | 14 | + | 4 | 1.7 ± 1.2 | NR | 33.3 | NR | 25 | 0 | NR |
| − | 9 | 2.7 ± 2.4 | NR | 33.3 | NR | 22.2 | 0 | NR | |||
| 9 | Givens [13], 2014 | 19 | + | 7 | 2.08 ± 1.21 | NR | NR | NR | 60 | 0 | 16.7 |
| − | 12 | 2.22 ± 1.78 | NR | NR | NR | 62.5 | 41.7 | 12.5 | |||
| 10 | Hardee [20], 2017 | 50 | + | 24 | * <2cm = 18, 2–4 cm = 2, >4 cm = 4 | NR | NR | 58 | 0 | NR | 21 |
| − | 26 | * <2cm = 13, 2–4 cm = 5, >4 cm = 7 | NR | NR | 69% | 4 | NR | 8 | |||
| 11 | Henke [12], 2014 | 27 | + | 17 | NR | NR | NR | 64.7 | 70.6 | 5.9 | NR |
| − | 10 | NR | NR | NR | 60 | 50 | 0 | NR | |||
| 12 | Hess [28], 2022 | 27 | + | 9 | 1.37 ± 1.09 | NR | NR | 42.8 | NR | NR | NR |
| − | 18 | 3.22 ± 2.04 | NR | NR | 68.75 | NR | NR | NR | |||
| 13 | Kumagai [11], 2004 | 44 | + | 3 | 1.56 ± 0.87 | NR | NR | 33.3 | NR | 0 | NR |
| − | NR | NR | NR | NR | NR | NR | NR | NR | |||
| 14 | Kure [29], 2019 | 14 | + | 2 | 1.25 ± 0.77 | NR | 50 | 33.3 | 0 | 0 | NR |
| − | 12 | 2.34 ± 1.79 | NR | 50 | 66.6 | 8.3 | 8.33 | NR | |||
| 15 | Kurt [30], 2012 | 2 | + | 1 | NR | NR | NR | 100 | 100 | 0 | NR |
| − | 1 | NR | 32.5 | NR | 0 | 0 | 0 | NR | |||
| 16 | Lee [31], 2021 | 106 | + | 41 | 1.40 ± 1.00 | 41.5 | NR | 68.4 | 60.5 | 2.5 | 16.2 |
| − | 65 | 2.10 ± 1.30 | 23.7 | NR | 76.2 | 75.8 | 43.18 | 46.6 | |||
| 17 | Li [7], 2022 | 169 | + | 97 | 1.55 ± 1.03 | 50 | NR | 14.4 | 24.7 | 2.1 | 2 |
| − | 72 | 2.49 ± 1.18 | NR | NR | 8.3 | 36.1 | 4.1 | 8.3 | |||
| 18 | Macerola [32], 2021 | 163 | + | 59 | NR | NR | NR | NR | NR | NR | NR |
| − | 104 | NR | NR | NR | NR | NR | NR | NR | |||
| 19 | Mitsutake [33], 2015 | 67 | + | 43 | 1.22 ± 0.68 | NR | NR | 14.2 | 58.1 | 0 | NR |
| − | 20 | 1.83 ± 0.95 | NR | NR | 20 | 35 | 10.5 | NR | |||
| 20 | Mollen [34], 2022 | 62 | + | 19 | NR | NR | NR | NR | NR | NR | NR |
| − | 43 | NR | NR | NR | NR | NR | NR | NR | |||
| 21 | Mostufi-Moab [19], 2018 | 62 | + | 12 | 1.10–4.00 | NR | NR | 63.6 | NR | 0 | NR |
| − | 50 | NR | NR | NR | NR | NR | NR | NR | |||
| 22 | Newfield [35], 2022 | 39 | + | 11 | 2.67 ± 1.98 | NR | 54.5 | 81.8 | NR | 0 | NR |
| − | 18 | 2.70 ± 1.44 | NR | 50 | 50 | NR | 7.14 | NR | |||
| 23 | Nies [36], 2021 | 94 | + | 8 | 2.90 (2.3–3.2) | NR | NR | 100 | NR | 100 | NR |
| − | 86 | 3.50 (2.3–5.5) | NR | NR | NR | NR | 100 | NR | |||
| 24 | Oishi [37], 2017 | 81 | + | 44 | 3.20 ± 1.8 | NR | NR | 98 | 36 | 0 | NR |
| − | 37 | 2.80 ± 1.3 | NR | NR | 81 | 44 | 8 | NR | |||
| 25 | Onder [38], 2016 | 50 | + | 15 | 2.12 ± NR | 93.3 | NR | 60 | 13.3 | 0 | 33.3 |
| − | 35 | 2.26 ± NR | 57.14 | NR | 61.5 | 8.57 | 14.2 | 5.7 | |||
| 26 | Passon [39], 2015 | 2 | + | 0 | NR | NR | NR | 0 | NR | 0 | NR |
| − | 2 | NR | NR | NR | 0 | NR | 0 | NR | |||
| 27 | Pekova [40], 2019 | 83 | + | 15 | 2.00 ± 1.06 | 53.3 | 20 | 46.6 | 40 | 0 | 20 |
| − | 68 | 2.22 ± 1.36 | 55.8 | 24.3 | 76.47 | 54.4 | 14.7 | 8.8 | |||
| 28 | Pessôa-Pereira [41], 2019 | 5 | + | 1 | 1 ± 0 | 0 | 0 | 0 | 0 | 0 | NR |
| − | 4 | 2.32 ± 1.39 | 75 | 25 | 50 | 0 | 0 | NR | |||
| 29 | Poyrazoglu [42], 2017 | 75 | + | 14 | * ≤1 cm = 3 >1 cm = 11 | 85.7 | 50 | 57.1 | 42.8 | 7.1 | NR |
| − | 42 | * ≤1 cm = 16 >1 cm = 26 | 42.8 | 40.5 | 38 | 28.6 | 9.5 | NR | |||
| 30 | Prasad ML [14], 2016 | 28 | + | 13 | 1.44 ± 1.04 | 23.1 | 23.1 | 38.4 | 7.7 | 0 | NR |
| − | 14 | 2.21 ± 1.13 | 50 | NR | 71.4 | NR | 14.3% | NR | |||
| 31 | Rogounovitch [43], 2021 | 34 | + | 5 | 1.44 ± 0.34 | 0 | 100 | 100 | 0 | 0 | NR |
| − | 29 | 1.6 ± 0.9 | NR | NR | NR | NR | NR | NR | |||
| 32 | Romittii [44], 2012 | 3 | + | - | - | - | - | - | - | - | - |
| − | 1 | 10.5 ± 0 | NR | NR | NR | 0 | NR | ||||
| 33 | Şenyürek [45], 2022 | 55 | + | 18 | 1.50 (0.6–5) | 83.3 | 55.5 | 33.3 | 25 | 0 | 33.3 |
| − | 37 | 1.40 (0.4–5) | 56.7 | 32.4 | 35.1 | 21.6 | 8.1 | 2.7 | |||
| 34 | Sisdeli L [46], 2019 | 80 | + | 12 | 3.35 ± 1.38 | NR | NR | 75 | NR | 25 | NR |
| − | 68 | 2.64 ± 1.58 | NR | NR | NR | NR | NR | NR | |||
| 35 | Stenman [47], 2021 | 5 | + | 1 | 4.20 ± 0 | 0 | NR | 100 | 100 | NR | 100 |
| − | 4 | 4.57 ± 2.12 | 50 | NR | 100 | 75 | 25 | 50 | |||
| 36 | Vasko V [48], 2005 | 4 | + | 3 | 2.36 ± 0.55 | 0 | NR | NR | NR | NR | NR |
| − | 1 | 1.50 ± 0 | 0 | NR | NR | NR | NR | NR | |||
| 37 | Zou M [49], 2014 | 6 | + | 1 | NR | NR | NR | 0 | NR | 0 | NR |
| − | 3 | NR | NR | NR | 44.4 | NR | 0 | NR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kotanidou, E.P.; Giza, S.; Tsinopoulou, V.R.; Margaritis, K.; Papadopoulou, A.; Sakellari, E.; Kolanis, S.; Litou, E.; Serbis, A.; Galli-Tsinopoulou, A. The Prognostic Significance of BRAF Gene Analysis in Children and Adolescents with Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis. Diagnostics 2023, 13, 1187. https://doi.org/10.3390/diagnostics13061187
Kotanidou EP, Giza S, Tsinopoulou VR, Margaritis K, Papadopoulou A, Sakellari E, Kolanis S, Litou E, Serbis A, Galli-Tsinopoulou A. The Prognostic Significance of BRAF Gene Analysis in Children and Adolescents with Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis. Diagnostics. 2023; 13(6):1187. https://doi.org/10.3390/diagnostics13061187
Chicago/Turabian StyleKotanidou, Eleni P, Styliani Giza, Vasiliki Rengina Tsinopoulou, Kosmas Margaritis, Anastasia Papadopoulou, Eleni Sakellari, Savvas Kolanis, Eleni Litou, Anastasios Serbis, and Assimina Galli-Tsinopoulou. 2023. "The Prognostic Significance of BRAF Gene Analysis in Children and Adolescents with Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis" Diagnostics 13, no. 6: 1187. https://doi.org/10.3390/diagnostics13061187