
Considering Diastolic Dyssynchrony as a Predictor of Favorable Response in LV-Only Fusion Pacing Cardiac Resynchronization Therapy
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria and Study Protocol
2.2. Implantation Strategy
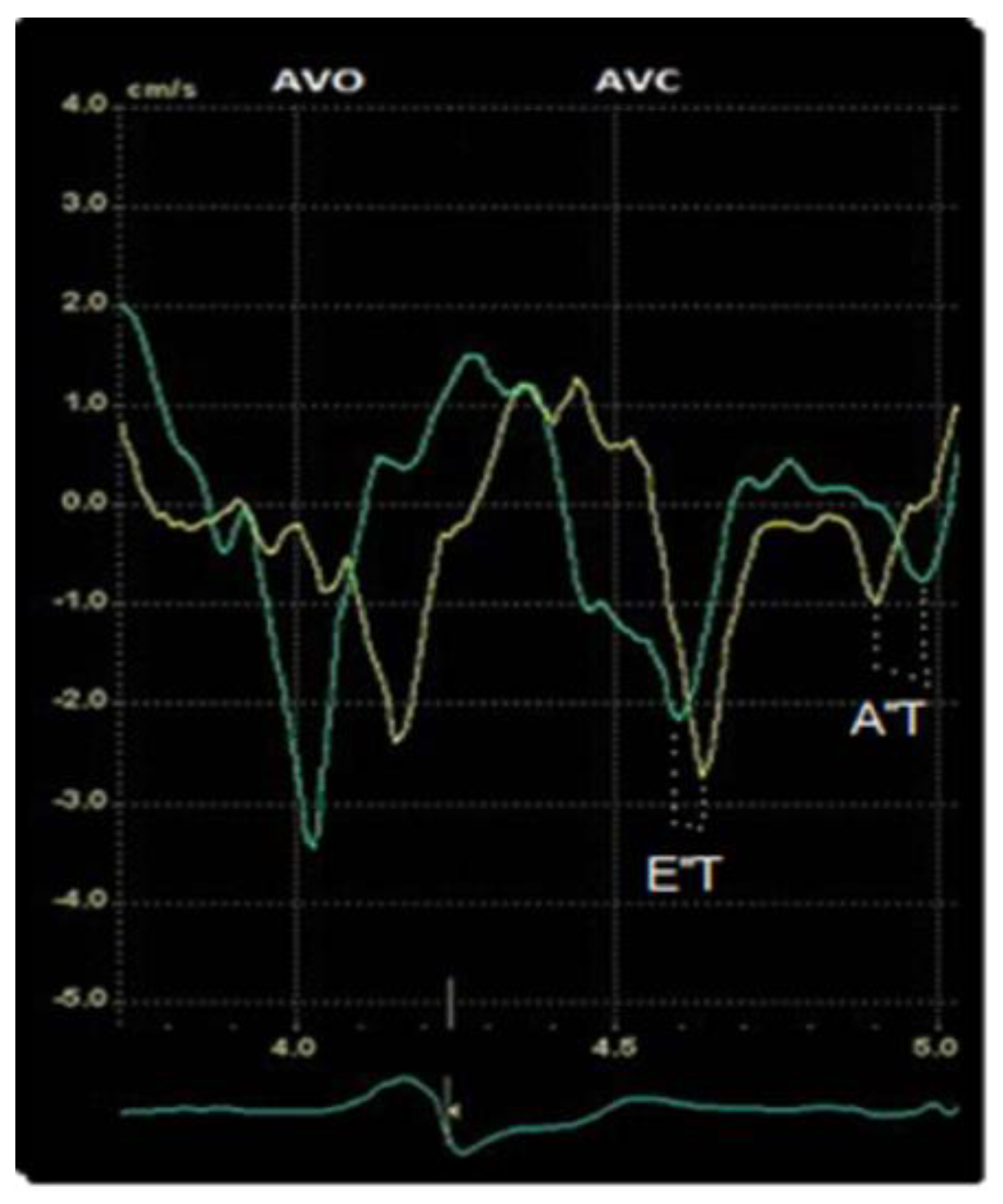
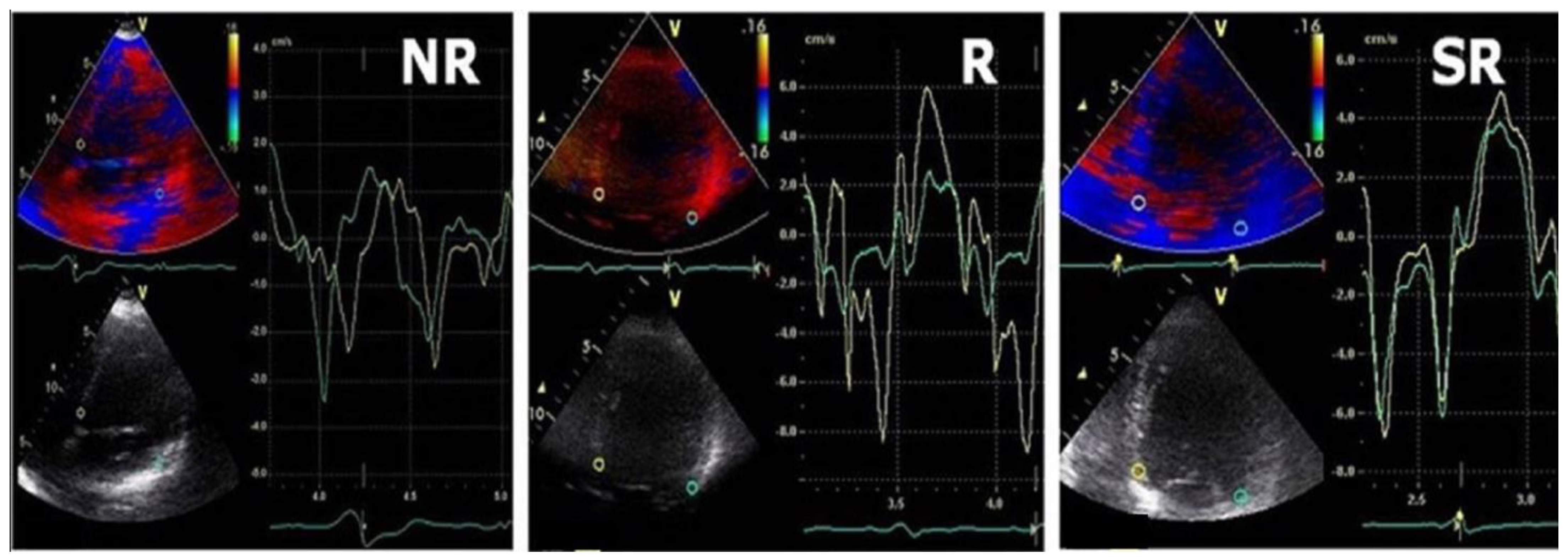
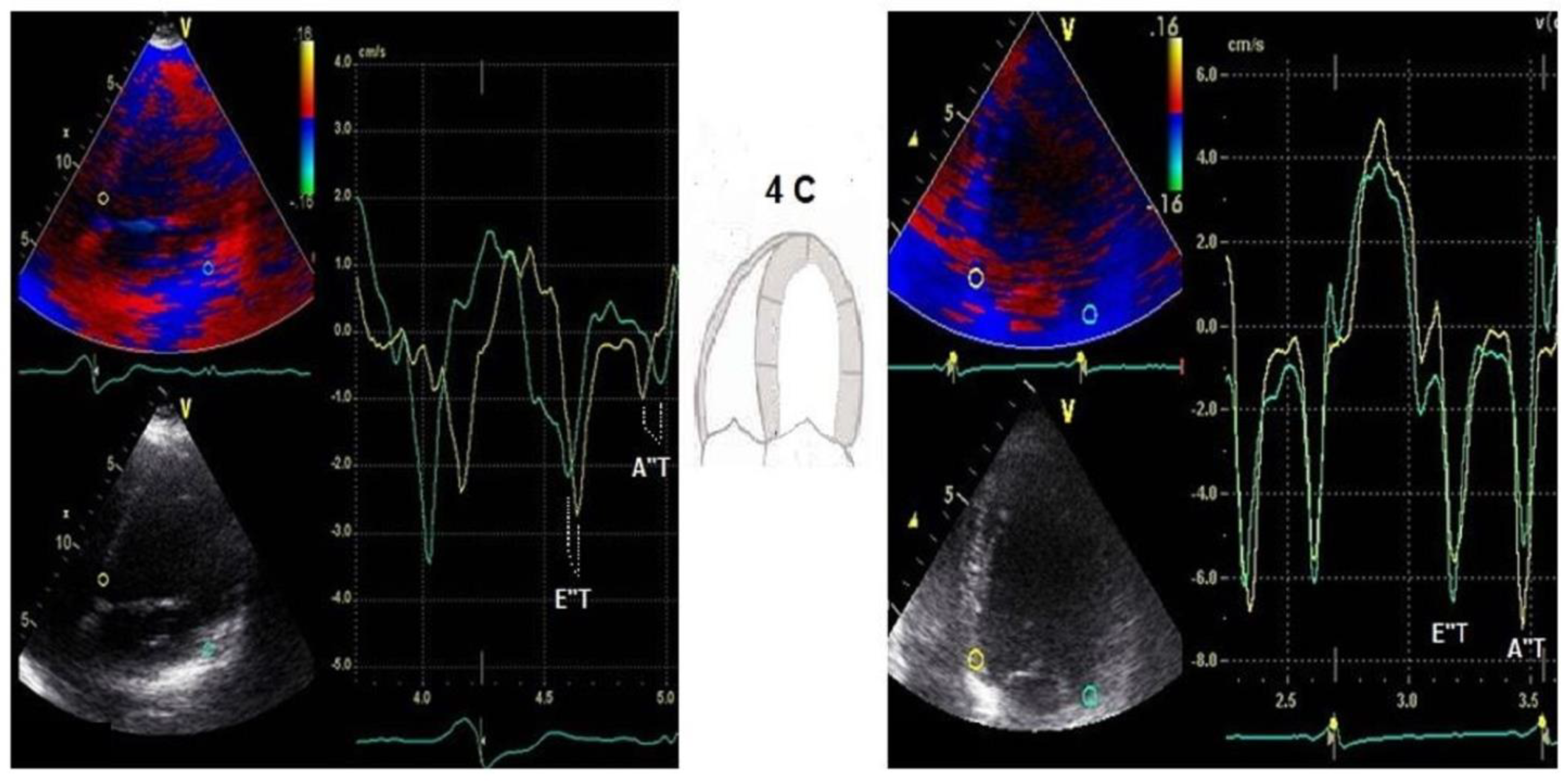
2.3. Transthoracic Echocardiography
2.4. CRT Response
2.5. Statistical Analysis
3. Results
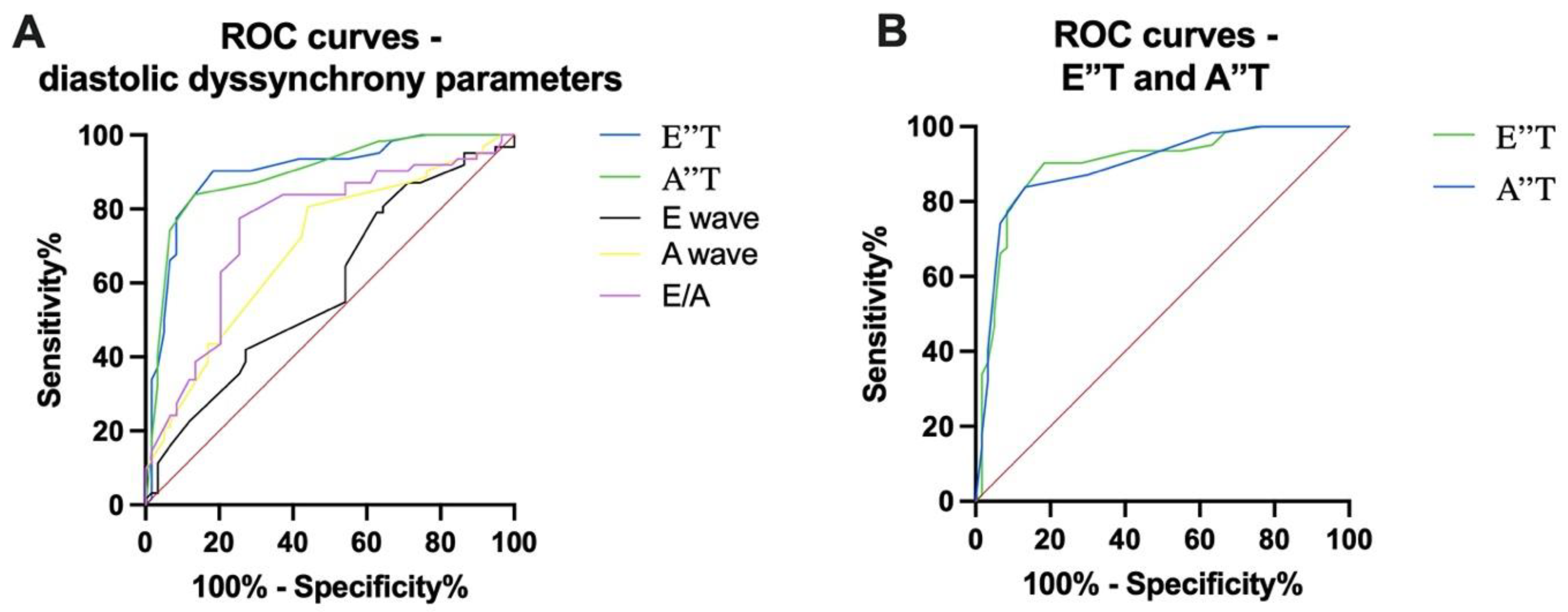
Prediction of Response
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thomas, G.; Kim, J.; Lerman, B.B. Improving Cardiac Resynchronisation Therapy. Arrhythmia Electrophysiol. Rev. 2019, 8, 220–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebrille, E.; DeSimone, C.V.; Vaidya, V.R.; Chahal, A.A.; Nkomo, V.T.; Asirvatham, S.J. Ventricular pacing—Electromechanical consequences and valvular function. Indian Pacing Electrophysiol. J. 2016, 16, 19–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Søgaard, P.; Egeblad, H.; Kim, W.; Jensen, H.K.; Pedersen, A.K.; Kristensen, B.; Mortensen, P.T. Tissue Doppler imaging predicts improved systolic performance and reversed left ventricular remodeling during long-term cardiac resynchronization therapy. J. Am. Coll. Cardiol. 2002, 40, 723–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cazeau, S.; Bordachar, P.; Jauvert, G.; Lazarus, A.; Alonso, C.; Vandrell, M.; Mugica, J.; Ritter, P. Echocardiographic Modeling of Cardiac Dyssynchrony Before and During Multisite Stimulation: A Prospective Study. Pacing Clin. Electrophysiol. 2003, 26, 137–143. [Google Scholar] [CrossRef]
- Porciani, M.C.; Lilli, A.; Macioce, R.; Cappelli, F.; Demarchi, G.; Pappone, A.; Ricciardi, G.; Padeletti, L. Utility of a new left ventricular asynchrony index as a predictor of reverse remodelling after cardiac resynchronization therapy. Eur. Heart J. 2006, 27, 1818–1823. [Google Scholar] [CrossRef]
- Cozma, D.; Vacarescu, C.; Petrescu, L.; Mornos, C.; Goanta, E.; Feier, H.; Luca, C.T.; Gusetu, G.; Vatasescu, R. CRT Pacing: Midterm Follow-Up in LV Only Pacing without RV Lead in Patients with Normal AV Conduction. J. Clin. Med. 2018, 7, 531. [Google Scholar] [CrossRef] [Green Version]
- Goanță, E.-V.; Luca, C.-T.; Vacarescu, C.; Crișan, S.; Petrescu, L.; Vatasescu, R.; Lazăr, M.-A.; Gurgu, A.; Turi, V.-R.; Cozma, D. Nonischemic Super-Responders in Fusion CRT Pacing with Normal Atrioventricular Conduction. Diagnostics 2022, 12, 2032. [Google Scholar] [CrossRef]
- Vacarescu, C.; Luca, C.-T.; Feier, H.; Gaiță, D.; Crișan, S.; Negru, A.-G.; Iurciuc, S.; Goanță, E.-V.; Mornos, C.; Lazăr, M.-A.; et al. Betablockers and Ivabradine Titration According to Exercise Test in LV Only Fusion CRT Pacing. Diagnostics 2022, 12, 1096. [Google Scholar] [CrossRef]
- Vacarescu, C.; Cozma, D.; Petrescu, L.; Dragan, S.; Mornos, C.; Crisan, S.; Feier, H.; Lazar, M.-A.; Cozlac, R.A.; Luca, C.T. Exercise test is essential in LV-only fusion CRT pacing without right ventricle lead. Clin. Interv. Aging 2019, 14, 969–975. [Google Scholar] [CrossRef] [Green Version]
- Abraham, W.T.; Fisher, W.G.; Smith, A.L.; Delurgio, D.B.; Leon, A.R.; Loh, E.; Kocovic, D.Z.; Packer, M.; MIRACLE Study Group; Multicenter InSync Randomized Clinical Evaluation; et al. Cardiac resynchronization in chronic heart failure. N. Engl. J. Med. 2002, 346, 1845–1853. [Google Scholar] [CrossRef] [Green Version]
- Cleland, J.G.; Daubert, J.C.; Erdmann, E.; Freemantle, N.; Gras, D.; Kappenberger, L.; Tavazzi, L. Longer-term effects of cardiac resynchronization therapy on mortality in heart failure [the Cardiac Resynchronization-Heart Failure (CARE-HF) trial extension phase]. Eur. Heart J. 2006, 27, 1928–1932. [Google Scholar] [CrossRef] [Green Version]
- Tomassoni, G. How to Define Cardiac Resynchronization Therapy Response. J. Innov. Card. Rhythm. Manag. 2016, 7, S1–S7. [Google Scholar] [CrossRef]
- Prinzen, F.W.; Vernooy, K.; DeBoeck, B.W.; Delhaas, T. Mechano-energetics of the asynchronous and resynchronized heart. Heart Fail Rev. 2011, 16, 215–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teske, A.J.; De Boeck, B.W.; Melman, P.G.; Sieswerda, G.T.; Doevendans, P.A.; Cramer, M.J. Echocardiographic quantification of myocardial function using tissue deformation imaging, a guide to image acquisition and analysis using tissue Doppler and speckle tracking. Cardiovasc. Ultrasound 2007, 30, 5–27. [Google Scholar] [CrossRef] [Green Version]
- Friedberg, M.K.; Silverman, N.H.; Dubin, A.M.; Rosenthal, D.N. Mechanical dyssynchrony in children with systolic dysfunction secundary to cardiomyopathy: A Doppler tissue vector velocity imaging study. J. Am. Soc. Echocardiogr. 2007, 20, 756–763. [Google Scholar] [CrossRef]
- Becker, M.; Franke, A.; Breithardt, O.A.; Ocklenburg, C.; Kaminski, T.; Kramann, R.; Knackstedt, C.; Stellbrink, C.; Hanrath, P.; Schauerte, P.; et al. Impact of left ventricular lead position on the efficacy of cardiac resynchronization therapy: A two-dimensional strainechocardiography study. Heart 2007, 93, 1197–1203. [Google Scholar] [CrossRef] [PubMed]
- Knebel, F.; Schattke, S.; Bondke, H.; Walde, T.; Eddicks, S.; Reibis, R.; Baumann, G.; Borges, A.C. Evaluation of longitudinal and radial two-dimensional strain imaging versus Doppler tissue echocardiography in predicting long-term response to cardiac resynchronization therapy. J. Am. Soc. Echocardiogr. 2007, 20, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Becker, M.; Kramann, R.; Franke, A.; Breithard, O.-A.; Heussen, N.; Knackstedt, C.; Stellbrink, C.; Schauerte, P.; Kelm, M.; Hoffmann, R. Impact of left ventricular lead position in cardiac resynchronization therapy on left ventricular remodeling. A circumferential strain analysis based on 2D echocardiography. Eur. Heart J. 2007, 28, 1211–1220. [Google Scholar] [CrossRef] [Green Version]
- Gorcsan, J., 3rd; Tanabe, M.; Bleeker, G.B.; Suffoletto, M.S.; Thomas, N.C.; Saba, S.; Tops, L.F.; Schalij, M.J.; Bax, J.J. Combined longitudinal and radial dyssynchrony predicts ventricular response after resynchronization therapy. J. Am. Coll. Cardiol. 2007, 50, 1476–1483. [Google Scholar] [CrossRef] [Green Version]
- Yu, C.M.; Fung, W.H.; Lin, H.; Zhang, Q.; Sanderson, J.E.; Lau, C.P. Predictors of left ventricular reverse remodeling after cardiac resynchronization therapy for heart failure secondary to idiopathic dilated or ischaemic cardiomyopathy. Am. J. Cardiol. 2003, 91, 684–688. [Google Scholar] [CrossRef]
- Bax, J.J.; Bleeker, G.B.; Marwick, T.H.; Molhoek, S.G.; Boersma, E.; Steendijk, P.; van der Wall, E.E.; Schalij, M.J. Left ventricular dyssynchrony predicts response and prognosis after cardiac resynchronization therapy. J. Am. Coll. Cardiol. 2004, 44, 1834–1840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penicka, M.; Bartunek, J.; De Bruyne, B.; Vanderheyden, M.; Goethals, M.; De Zutter, M.; Brugada, P.; Geelen, P. Improvement of left ventricular function after cardiac resynchronization therapy is predicted by tissue Doppler imaging echocardiography. Circulation 2004, 109, 978–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Notabartolo, D.; Merlino, J.D.; Smith, A.L.; De Lurgio, D.B.; Vera, F.V.; Easily, K.A.; Martin, R.P.; Leon, A.R. Usefulness of the peak velocity difference by tissue Doppler imaging technique as an effective predictor of response to cardiac resinchronization therapy. Am. J. Cardiol. 2004, 94, 817–820. [Google Scholar] [CrossRef] [PubMed]
- Mullens, W.; Grimm, R.A.; Verga, T.; Dresing, T.; Starling, R.C.; Wilkoff, B.L.; Tang, W.H. Insights from a cardiac resynchronization optimization clinic as part of a heart failure disease management program. J. Am. Coll. Cardiol. 2009, 53, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Cao, Y.; Liang, L. Effect of dynamic atrioventricular and interventricular delay optimization for cardiac resynchronization therapy on cardiac function and neuroendocrine factors in patients with congestive heart failure. Arch. Med. Sci. 2021, 17, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Gasparini, M.; Biffi, M.; Landolina, M.; Cattafi, G.; Rordorf, R.; Botto, G.L.; Battista Forleo, G.; Morani, G.; Santini, L.; Dello Russo, A.; et al. The Interplay of PR Interval and AV Pacing Delays Used for Cardiac Resynchronization Therapy in Heart Failure Patients: Association with Clinical Response in a Retrospective Analysis of a Large Observational Study. J. Pers. Med. 2022, 12, 1512. [Google Scholar] [CrossRef]
- Brignole, M.; Auricchio, A.; Baron-Esquivias, G.; Bordachar, P.; Boriani, G.; Breithardt, O.A.; Cleland, J.; Deharo, J.; Delgado, V. 2013 ESC guidelines on cardiac pacing and cardiac resynchronization therapy: The task force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Europace 2013, 15, 1070–1118. [Google Scholar]
- Daubert, J.C.; Saxon, L.; Adamson, P.B.; Auricchio, A.; Berger, R.D.; Beshai, J.F.; Breithard, O.; Brignole, M.; Cleland, J.; Delurgio, D.B.; et al. 2012 EHRA/HRS expert consensus statement on cardiac resynchronization therapy in heart failure: Implant and follow-up recommendations and management. Europace 2012, 14, 1236–1286. [Google Scholar] [CrossRef]
- Chung, E.S.; Leon, A.R.; Tavazzi, L.; Sun, J.P.; Nihoyannopoulos, P.; Merlino, J.; Abraham, W.T.; Ghio, S.; Leclercq, C.; Bax, J.J.; et al. Results of the Predictors of Response to CRT (PROSPECT) trial. Circulation 2008, 117, 2608–2616. [Google Scholar] [CrossRef] [Green Version]
- Auricchio, A.; Abraham, W.T. Cardiac resynchronization therapy: Current state of the art, cost versus benefit. Circulation 2004, 109, 300–307. [Google Scholar] [CrossRef]
- Citro, R.; Galderisi, M. Myocardial postsystolic motion in ischaemic and not ischaemic myocardium: The clinical value of tissue Doppler. Echocardiography 2005, 22, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Weidemann, F.; Broschett, J.A.; Bijnens, B.; Claus, P.; Sutherland, G.R.; Voelker, W.; Ertl, G.; Strotmann, J. How to distinguish between ischaemic and nonischaemic postsystolic thickening: A strain rate imaging study. Ultrasound Med. Biol. 2006, 32, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Voigt, J.U.; Lindenmeier, G.; Exner, B.; Regenfus, M.; Werner, D.; Reulbach, U.; Nixdorff, U.; Flachskmpf, F.A.; Daniel, W.G. Incidence and characteristics of segmental postsystolic longitudinal shortening in normal, acutely ischaemic, and scarred myocardium. J. Am. Soc. Echocardiogr. 2003, 16, 415–423. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 62) | SR (n = 21) | R(n = 38) | NR (n = 3) | ||
|---|---|---|---|---|---|
| Age, years (mean ± SD) | 62 ± 11 | 61 ± 9 | 69 ± 10 | 73 ± 11 | |
| Male, n (%) | 38 (61%) | 11 (52%) | 25 (65%) | 2 (66%) | |
| NYHA functional class, n (%) | II | 6 (10%) | 2 (10%) | 4 (11%) | 0 |
| III | 47 (76%) | 18 (86%) | 27(71%) | 2 (67%) | |
| IV | 9 (1%) | 1 (5%) | 7 (18%) | 1 (33%) | |
| NT-proBNP pg/mL, n (%) | 400–1000 pg/mL | 11 (17%) | 3 (14%) | 8 (21%) | 0 |
| 1000–2000 pg/mL | 36 (58%) | 15 (71%) | 20 (52%) | 1 (33%) | |
| >2000 pg/mL | 16 (26%) | 4 (19%) | 10 (26%) | 2 (66%) | |
| Hypertension, n (%) | 35 (56%) | 11 (52%) | 21(55%) | 3 (100%) * | |
| Diabetes mellitus, n (%) | 25 (40%) | 9 (43%) | 14 (37%) | 2 (67%) | |
| Dyslipidemia, n (%) | 48 (77%) | 19 (90%) | 26 (68%) | 3 (100%) * | |
| Obesity, n (%) | 26(42%) | 10 (47%) | 14 (36%) | 2 (67%) | |
| Chronic kidney disease, n (%) ** | 25 (40%) | 5 (23%) | 17 (44%) | 3 (100%) * | |
| Medication | Beta blockers, n (%) | 46 (74%) | 18 (85%) | 26 (68%) | 2 (67%) |
| Ivabradine, n (%) | 26 (42%) | 9 (43%) | 15 (39%) | 2 (67%) | |
| ACEI/ARB, n (%) | 54 (87%) | 19 (90%) | 33 (86%) | 2 (67%) | |
| Diuretics, n (%) | 56 (90%) | 18 (85%) | 35 (92%) | 3 (100%) | |
| Mineralocorticoid receptor blockers, n (%) | 47 (76 %) | 14 (66%) | 31 (81%) | 2 (67%) | |
| Sacubitril/valsartan, n (%) | 8 (12%) | 2 (9%) | 5 (13%) | 1 (33%) | |
| Super-Responders | p | Responders (n = 38) | p | Non-Responders | p Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| (n = 21) | (n = 3) | ||||||||
| Baseline | FU | Baseline | FU | Baseline | FU | ||||
| EF (%) | 31 ± 4 | 45 ± 4 | <0.0001 | 26 ± 5 | 34 ± 6 | <0.0001 | 24 ± 4 | 26 ± 5 | 0.61 |
| LV EDV (mL) | 243 ± 82 | 193 ± 81 | 0.0028 | 272 ± 72 | 217 ± 64 | 0.0007 | 308 ± 105 | 278 ± 93 | 0.72 |
| LV ESV (mL) | 126 ± 44 | 75 ± 21 | <0.0001 | 206 ± 62 | 148 ± 51 | <0.0001 | 224 ± 73 | 174 ± 29 | 0.33 |
| LA Volume (mL) | 92 ± 30 | 89 ± 30 | 0.74 | 116 ± 40 | 101 ± 33 | 0.07 | 148 ± 33 | 141 ± 0.5 | 0.73 |
| LA Surface (cm2) | 24 ± 4 | 22 ± 5 | 0.16 | 30 ± 7 | 27 ± 7 | 0.06 | 32 ± 2 | 33 ± 3 | 0.70 |
| PASP (mmHg) | 37 ± 12 | 31 ±8 | 0.06 | 42 ± 13 | 34 ± 10 | 0.0036 | 58 ± 6 | 38 ± 6 | 0.0151 |
| E/E′ | 13 ± 4 | 11 ± 4 | 0.0295 | 21 ± 9 | 14 ± 4 | <0.0001 | 29 ± 4 | 23 ± 7 | 0.26 |
| E/A | 2 ± 0 | 1 ± 0 | − | 1.4 ± 5 | 0.8 ± 3.9 | 0.44 | 2 ± 0 | 2 ± 0 | − |
| E′ Time (ms) | 90 ± 20 | 25 ± 10 | <0.0001 | 76 ± 13 | 51 ± 11 | <0.0001 | 118 ± 10 | 102 ± 14 | 0.18 |
| A′ Time (ms) | 16 ± 7 | 8 ± 5 | =0.0001 | 26 ± 8 | 17 ± 5 | <0.0001 | 67 ± 9 | 57 ± 5 | 0.16 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gurgu, A.; Luca, C.-T.; Vacarescu, C.; Petrescu, L.; Goanta, E.-V.; Lazar, M.-A.; Arnăutu, D.-A.; Cozma, D. Considering Diastolic Dyssynchrony as a Predictor of Favorable Response in LV-Only Fusion Pacing Cardiac Resynchronization Therapy. Diagnostics 2023, 13, 1186. https://doi.org/10.3390/diagnostics13061186
Gurgu A, Luca C-T, Vacarescu C, Petrescu L, Goanta E-V, Lazar M-A, Arnăutu D-A, Cozma D. Considering Diastolic Dyssynchrony as a Predictor of Favorable Response in LV-Only Fusion Pacing Cardiac Resynchronization Therapy. Diagnostics. 2023; 13(6):1186. https://doi.org/10.3390/diagnostics13061186
Chicago/Turabian StyleGurgu, Andra, Constantin-Tudor Luca, Cristina Vacarescu, Lucian Petrescu, Emilia-Violeta Goanta, Mihai-Andrei Lazar, Diana-Aurora Arnăutu, and Dragos Cozma. 2023. "Considering Diastolic Dyssynchrony as a Predictor of Favorable Response in LV-Only Fusion Pacing Cardiac Resynchronization Therapy" Diagnostics 13, no. 6: 1186. https://doi.org/10.3390/diagnostics13061186