
The Accuracy of Pre-Endoscopic Scores for Mortality Prediction in Patients with Upper GI Bleeding and No Endoscopy Performed
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Aim of the Study
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Mean Scores
3.3. Accuracy of Prognostic Scores
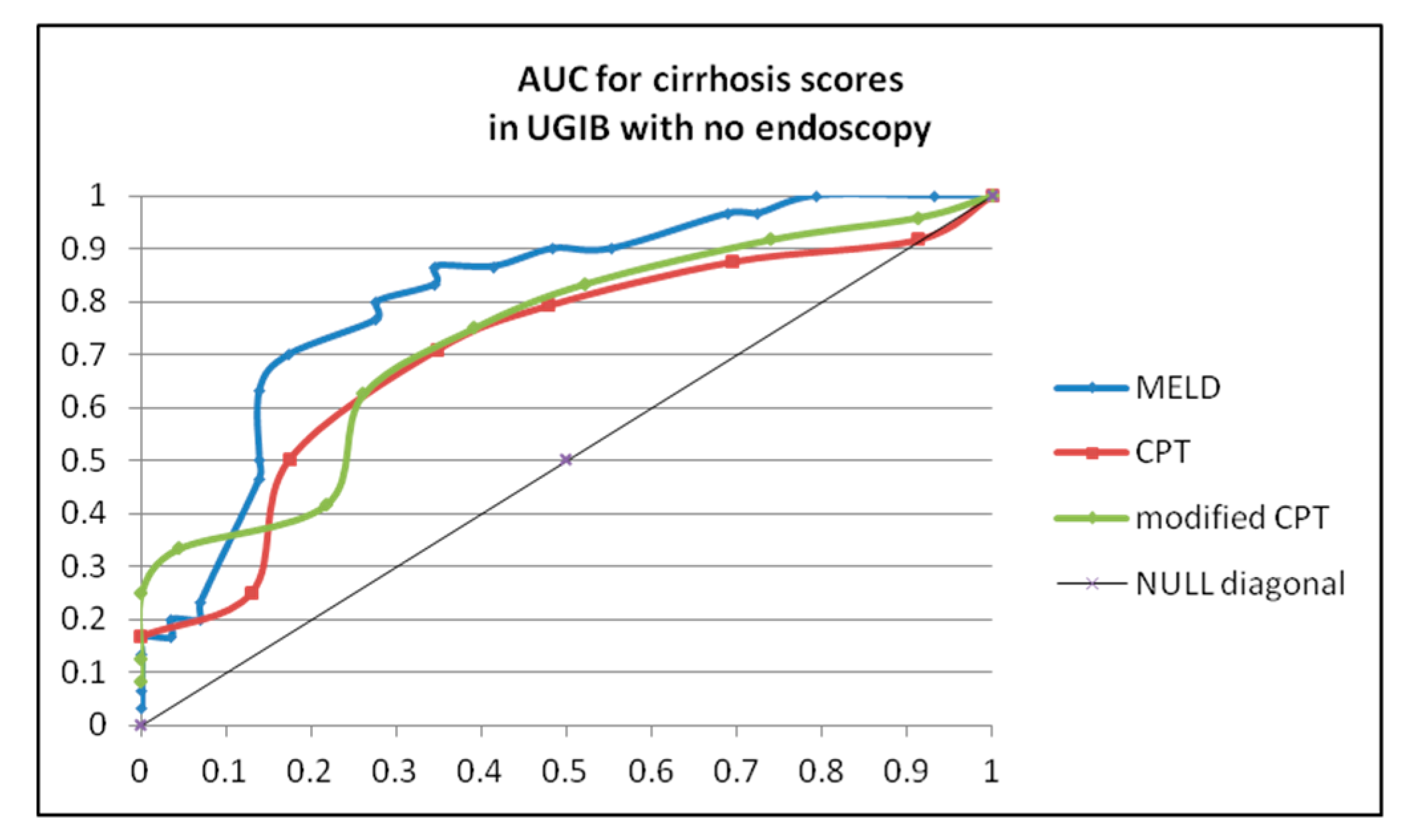
3.4. CPT and MELD Score in Cirrhosis Patients
3.5. Reasons for no Endoscopy Performed: Pathology Examination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BBS | Baylor bleeding score |
| CCI | Charlson comorbidity index |
| CPT | Child–Pugh Turcotte score |
| CSMCPI | Cedars–Sinai Medical Center Predictive Index |
| GBS | Glasgow-Blatchford score |
| ICU | intensive care unit |
| INBS | International Bleeding Score |
| mGBS | modified Glasgow-Blatchford score |
| m-N-score | modified N-score |
| NVUGIB | non-variceal upper gastrointestinal bleeding |
| PNED | Progetto Nazionale Emmoragia Digestive |
| RS | Rockall score |
| TSC | T-score |
| UGIB | upper gastrointestinal bleeding |
| VUGIB | variceal upper gastrointestinal bleeding |
References
- Tang, Y.; Shen, J.; Zhang, F.; Zhou, X.; Tang, Z.; You, T. Scoring systems used to predict mortality in patients with acute upper gastrointestinal bleeding in the ED. Am. J. Emerg. Med. 2018, 36, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Ko, I.G.; Kim, S.E.; Chang, B.S.; Kwak, M.S.; Yoon, J.Y.; Cha, J.M.; Shin, H.P.; Lee, J.I.; Kim, S.H.; Han, J.H.; et al. Evaluation of scoring systems without endoscopic findings for predicting outcomes in patients with upper gastrointestinal bleeding. BMC Gastroenterol. 2017, 17, 159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonçalves, T.C.; Barbosa, M.; Xavier, S.; Carvalho, P.B.; Machado, J.F.; Magalhães, J.; Marinho, C.; Cotter, J. Optimizing the Risk Assessment in Upper Gastrointestinal Bleeding: Comparison of 5 Scores Predicting 7 Outcomes. GE-Port. J. Gastroenterol. 2018, 25, 299–307. [Google Scholar] [CrossRef]
- Benedeto-Stojanov, D.; Bjelaković, M.; Stojanov, D.; Aleksovski, B. Prediction of in-hospital mortality after acute upper gastrointestinal bleeding: Cross-validation of several risk scoring systems. J. Int. Med. Res. 2022, 50, 3000605221086442. [Google Scholar] [CrossRef] [PubMed]
- Dhir, V.; Shah, R. Scoring systems for upper gastrointestinal bleeding: Which one scores better? Indian J. Gastroenterol. 2019, 38, 95–97. [Google Scholar] [CrossRef] [Green Version]
- Cheng, D.W.; Lu, Y.W.; Teller, T.; Sekhon, H.K.; Wu, B.U. A modified Glasgow Blatchford Score improves risk stratification in upper gastrointestinal bleed: A prospective comparison of scoring systems. Aliment. Pharmacol. Ther. 2012, 36, 782–789. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, Y.; Abe, T.; Kawamura, N.; Keitoku, T.; Shibata, I.; Ohno, S.; Ono, K.; Makishima, M. Prediction of the need for emergency endoscopic treatment for upper gastrointestinal bleeding and new score model: A retrospective study. BMC Gastroenterol. 2022, 22, 337. [Google Scholar] [CrossRef]
- Ito, N.; Funasaka, K.; Furukawa, K.; Kakushima, N.; Hirose, T.; Muroi, K.; Suzuki, T.; Suzuki, T.; Hida, E.; Ishikawa, T.; et al. A novel scoring system to predict therapeutic intervention for non-variceal upper gastrointestinal bleeding. Intern. Emerg. Med. 2021, 17, 423–430. [Google Scholar] [CrossRef]
- Horibe, M.; Iwasaki, E.; Bazerbachi, F.; Kaneko, T.; Matsuzaki, J.; Minami, K.; Masaoka, T.; Hosoe, N.; Ogura, Y.; Namiki, S.; et al. Horibe GI bleeding prediction score: A simple score for triage decision-making in patients with suspected upper GI bleeding. Gastrointest. Endosc. 2020, 92, 578–588.e4. [Google Scholar] [CrossRef]
- Li, Y.; Lu, Q.; Song, M.; Wu, K.; Ou, X. Comparisons of six endoscopy independent scoring systems for the prediction of clinical outcomes for elderly and younger patients with upper gastrointestinal bleeding. BMC Gastroenterol. 2022, 22, 187. [Google Scholar] [CrossRef]
- Redondo-Cerezo, E.; Vadillo-Calles, F.; Stanley, A.J.; Laursen, S.; Laine, L.; Dalton, H.R.; Ngu, J.H.; Schultz, M.; Jiménez-Rosales, R. MAP(ASH): A new scoring system for the prediction of intervention and mortality in upper gastrointestinal bleeding. J. Gastroenterol. Hepatol. 2019, 35, 82–89. [Google Scholar] [CrossRef]
- Marmo, R.; Koch, M.; Cipolletta, L.; Capurso, L.; Grossi, E.; Cestari, R.; Bianco, M.A.; Pandolfo, N.; Dezi, A.; Casetti, T.; et al. Predicting Mortality in Non-Variceal Upper Gastrointestinal Bleeders: Validation of the Italian PNED Score and Prospective Comparison with the Rockall Score. Am. J. Gastroenterol. 2010, 105, 1284–1291. [Google Scholar] [CrossRef] [PubMed]
- Horibe, M.; Iwasaki, E.; Matsuzaki, J.; Bazerbachi, F.; Kaneko, T.; Minami, K.; Fukuhara, S.; Masaoka, T.; Hosoe, N.; Ogura, Y.; et al. Superiority of urgent vs early endoscopic hemostasis in patients with upper gastrointestinal bleeding with high-risk stigmata. Gastroenterol. Rep. 2021, 9, 543–551. [Google Scholar] [CrossRef]
- Iino, C.; Mikami, T.; Igarashi, T.; Aihara, T.; Ishii, K.; Sakamoto, J.; Tono, H.; Fukuda, S. Evaluation of scoring models for identifying the need for therapeutic intervention of upper gastrointestinal bleeding: A new prediction score model for Japanese patients. Dig. Endosc. 2016, 28, 714–721. [Google Scholar] [CrossRef]
- Oakland, K.; Kahan, B.C.; Guizzetti, L.; Martel, M.; Bryant, R.V.; Brahmania, M.; Singh, S.; Nguyen, N.Q.; Sey, M.S.L.; Barkun, A.; et al. Development, Validation, and Comparative Assessment of an International Scoring System to Determine Risk of Upper Gastrointestinal Bleeding. Clin. Gastroenterol. Hepatol. 2019, 17, 1121–1129.e2. [Google Scholar] [CrossRef] [PubMed]
- Laursen, S.B.; Oakland, K.; Laine, L.; Bieber, V.; Marmo, R.; Redondo-Cerezo, E.; Dalton, H.R.; Ngu, J.; Schultz, M.; Soncini, M.; et al. ABC score: A new risk score that accurately predicts mortality in acute upper and lower gastrointestinal bleeding: An international multicentre study. Gut 2020, 70, 707–716. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Moon, H.S.; Kwon, I.S.; Park, J.H.; Kim, J.S.; Kang, S.H.; Sung, J.K.; Lee, E.S.; Kim, S.H.; Lee, B.S.; et al. Validation of a new risk score system for non-variceal upper gastrointestinal bleeding. BMC Gastroenterol. 2020, 20, 193. [Google Scholar] [CrossRef] [PubMed]
- Rout, G.; Sharma, S.; Gunjan, D.; Kedia, S.; Nayak, B. Shalimar Comparison of various prognostic scores in variceal and non-variceal upper gastrointestinal bleeding: A prospective cohort study. Indian J. Gastroenterol. 2019, 38, 158–166. [Google Scholar] [CrossRef]
- Thanapirom, K.; Ridtitid, W.; Rerknimitr, R.; Thungsuk, R.; Noophun, P.; Wongjitrat, C.; Luangjaru, S.; Vedkijkul, P.; Lertkupinit, C.; Poonsab, S.; et al. Prospective comparison of three risk scoring systems in non-variceal and variceal upper gastrointestinal bleeding. J. Gastroenterol. Hepatol. 2016, 31, 761–767. [Google Scholar] [CrossRef]
- Reed, E.A.; Dalton, H.; Blatchford, O.; Ashley, D.; Mowat, C.; Gaya, D.R.; Cahill, A.; Warshow, U.; Hare, N.; Groome, M.; et al. Is the Glasgow Blatchford score useful in the risk assessment of patients presenting with variceal haemorrhage? Eur. J. Gastroenterol. Hepatol. 2014, 26, 432–437. [Google Scholar] [CrossRef]
- Yang, L.; Sun, R.; Wei, N.; Chen, H. Systematic review and meta-analysis of risk scores in prediction for the clinical outcomes in patients with acute variceal bleeding. Ann. Med. 2021, 53, 1806–1815. [Google Scholar] [CrossRef] [PubMed]
- Mandal, A.K.; Paudel, M.; Kc, S.; Chaudhary, S.; Paudel, B.N.; Poudyal, N.S.; Shrestha, B.; Karki, B.; Thapa, S.; Khadka, D.; et al. Factors Predicting Mortality of Acute Variceal Bleeding in Liver Cirrhosis. J. Nepal. Med. Assoc. 2018, 56, 493–496. [Google Scholar] [CrossRef] [Green Version]
- Hassanien, M.; El-Ghannam, M.; El-Talkawy, M.D.; Abdelrahman, Y.; El Attar, G.; Taleb, H.A. Risk Scoring Systems to Predict In-Hospital Mortality in Patients with Acute Variceal Bleeding due to Hepatitis C Virus induced Liver Cirrhosis. Gastroenterol. Insights 2018, 9, 7629. [Google Scholar] [CrossRef] [Green Version]
- Lu, X.; Zhang, X.; Chen, H. Comparison of the AIMS65 score with the Glasgow-Blatchford and Rockall scoring systems for the prediction of the risk of in-hospital death among patients with upper gastrointestinal bleeding. Rev. Esp. Enferm. Dig. 2020, 112, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.; Sun, G.; Huang, H.; Zhang, X.; Xu, Y.; Chen, S.; Song, Y.; Li, X.; Lv, B.; Ren, J.; et al. Comparison of the Glasgow-Blatchford and Rockall Scores for prediction of nonvariceal upper gastrointestinal bleeding outcomes in Chinese patients. Medicine 2019, 98, e15716. [Google Scholar] [CrossRef]
- Custovic, N.; Selimovic, A.; Srsen, N.; Prohic, D. Comparison of Glasgow-Blatchford Score and Rockall Score in Patients with Upper Gastrointestinal Bleeding. Med. Arch. 2020, 74, 270–274. [Google Scholar] [CrossRef]
- Shahrami, A.; Ahmadi, S.; Safari, S. Full and Modified Glasgow-Blatchford Bleeding Score in Predicting the Outcome of Patients with Acute Upper Gastrointestinal Bleeding; a Diagnostic Accuracy Study. Emergency 2018, 6, e31. [Google Scholar] [CrossRef]
- Ebrahimi Bakhtavar, H.; Morteza Bagi, H.R.; Rahmani, F.; Shahsavari Nia, K.; Ettehadi, A. Clinical Scoring Systems in Predicting the Outcome of Acute Upper Gastrointestinal Bleeding; a Narrative Review. Emergency 2017, 5, e36. [Google Scholar] [PubMed]
- Das, S.K.; Roy, D.K.; Chowdhury, A.A.; Roy, A.S.; Ahammed, S.U.; Asadujjaman, M.; Rabbani, M.G.; Islam, M.S.; Barman, G.C.; Chanda, K.; et al. Correlation of eGFR By MDRD and CKD-EPI Formula with Cre-atinine Clearance Estimation in CKD Patients and Healthy Subjects. Mymensingh Med. J. 2021, 30, 35–42. [Google Scholar]
- Ramaekers, R.; Mukarram, M.; Smith, C.A.M.; Thiruganasambandamoorthy, V. The Predictive Value of Preendoscopic Risk Scores to Predict Adverse Outcomes in Emergency Department Patients with Upper Gastrointestinal Bleeding: A Systematic Review. Acad. Emerg. Med. 2016, 23, 1218–1227. [Google Scholar] [CrossRef] [Green Version]
- Laursen, S.B.; Dalton, H.R.; Murray, I.A.; Michell, N.; Johnston, M.R.; Schultz, M.; Hansen, J.M.; de Muckadell, O.B.S.; Blatchford, O.; Stanley, A.J.; et al. Performance of New Thresholds of the Glasgow Blatchford Score in Managing Patients with Upper Gastrointestinal Bleeding. Clin. Gastroenterol. Hepatol. 2015, 13, 115–121.e2. [Google Scholar] [CrossRef] [PubMed]
- Ak, R.; Hökenek, N.M. Comparison of AIMS65 and Glasgow Blatchford scores in predicting mortality in patients with upper gastrointestinal bleeding. Rev. Assoc. Med. Bras. 2021, 67, 766–770. [Google Scholar] [CrossRef] [PubMed]
- Franco, M.C.; Jang, S.; Martins, B.D.C.; Stevens, T.; Jairath, V.; Lopez, R.; Vargo, J.J.; Barkun, A.; Maluf-Filho, F. Risk Stratification in Cancer Patients with Acute Upper Gastrointestinal Bleeding: Comparison of Glasgow-Blatchford, Rockall and AIMS65, and Development of a New Scoring System. Clin. Endosc. 2022, 55, 240–247. [Google Scholar] [CrossRef]
- Stanley, A.J.; Laine, L.; Dalton, H.; Ngu, J.H.; Schultz, M.; Abazi, R.; Zakko, L.; Thornton, S.; Wilkinson, K.; Khor, C.J.L.; et al. Comparison of risk scoring systems for patients presenting with upper gastrointestinal bleeding: International multicentre prospective study. BMJ 2017, 356, i6432. [Google Scholar] [CrossRef] [Green Version]
- Bardakçı, O.; Sıddıkoğlu, D.; Akdur, G.; Şimşek, G.; Atalay, Ü.; Das, M.; Akdur, O.; Beyazit, Y. Prediction of Adverse Outcomes using Non-Endoscopic Scoring Systems in Patients over 80 Years of Age Who Present with Upper Gastrointestinal Bleeding in the Emergency Department. Turk. J. Trauma Emerg. Surg. 2022, 28, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Ch’Ng, C.L.; Kingham, J.G.C. Scoring systems and risk assessment for upper gastrointestinal bleeding. Eur. J. Gastroenterol. Hepatol. 2001, 13, 1137–1139. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| 0 | 1 | 2 | 3 | |
|---|---|---|---|---|
| Age | <60 | 60–79 | ≥80 | - |
| Shock | p < 100 sBP ≥ 100 | p ≥ 100 ≥100 | sBP < 100 | - |
| Comorbidities | NO major | - | Cardiac failure, coronary ischemia | Renal/liver failure Disseminated malignancy |
| Diagnosis | MW No lesion No stigmata | Other exc. malignancy | Malignancy | |
| Bleeding stigmata | No/ dark spot | - | Blood, adherent clot Visible/spurting vessel | - |
| Urea (mg/dL) | 39–47 | 2 |
| 48–60 | 3 | |
| 60–149 | 4 | |
| ≥150 | 6 | |
| Hb (g/dL) | Men 12–12.99 | 1 |
| Men ≥ 10 | 3 | |
| Woman ≥ 10 | 1 | |
| Both sexes < 10 | 6 | |
| sBP (mm Hg) | 100–109 | 1 |
| 90–99 | 2 | |
| <90 | 3 | |
| Pulse (>100/min) | 1 | |
| Melena | 1 | |
| Syncope | 2 | |
| Liver disease | 2 | |
| Cardiac failure | 2 |
| 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|
| Age | 30–49 | 50–59 | 60–69 | ≥70 | |
| Number of diseases | 1–2 | 3–4 | ≥5 | ||
| Severity of diseases | Chronic | Acute | |||
| Endoscopy score | |||||
| Site of bleeding | Posterior DU | ||||
| Bleeding stigmata | IIb | IIa | I |
| 1 | 2 | 3 | |
|---|---|---|---|
| Pulse | >110 | 90–110 | <90 |
| Systolic blood pressure | <90 | 90–110 | >110 |
| Hemoglobin | ≤8 g% | 9–10 | >10 |
| General condition | Poor | Intermediate | Good |
| Score | |
|---|---|
| Age > 65 year | 1 |
| Systolic blood pressure < 90 | 1 |
| Altered mental status | 1 |
| Alb < 3 g% | 1 |
| INR > 1.5 | 1 |
| N-Score | m-N-Score | |
|---|---|---|
| Syncope | 3 | 3 |
| Hematemesis | 2 | |
| Red blood hematemesis | 2 | |
| Coffee-ground hematemesis | 1 | |
| BUN ≥ 22.4 | 1 | 1 |
| BUN/creatinine ≥ 30 | 1 | 1 |
| Points | |
|---|---|
| Hematemesis | 1 |
| Heart rate (times/minute) ≥ 100 | 1 |
| Blood pressure (systolic) ≤ 100 mm Hg | 1 |
| Hb ≤ 10 g/dL | 1 |
| BUN ≥ 22.4 | 2 |
| Points | |
|---|---|
| Disturbance of consciousness | 1 |
| ASA score > 2 | 1 |
| Heart rate (times/minute) > 100 | 1 |
| Blood pressure (systolic) < 90 mm Hg | 2 |
| Hb < 10 g/dL | 2 |
| Albumin < 2.5 g/dL | 2 |
| Points | |
|---|---|
| Blood pressure (systolic) < 100 mm Hg | 2 |
| Syncope | 2 |
| Hematemesis | 3 |
| Hb < 10 g/dL | 1 |
| BUN ≥ 22.4 | 2 |
| eGFR (ml/min/1.73 mm) ≥ 60 | −2 |
| Oral antiplatelet drug | −2 |
| Points | |
|---|---|
| Age | |
| 60–74 years | 1 |
| ≥75 years | 2 |
| Comorbidity | |
| Altered mental status | 2 |
| Liver cirrhosis | 2 |
| Disseminated malignancy | 2 |
| ASA score | |
| 3 | 1 |
| ≥4 | 3 |
| Blood tests | 1 |
| Urea > 10 mmol/L | 1 |
| Albumin < 30 g/L | 2 |
| Creatinine | |
| 100–150 μmol/L | 1 |
| >150 μmol/L | 2 |
| Variceal (N = 520) | Non-Variceal (N = 1628) | Unknown (N = 198) | |
|---|---|---|---|
| Age (years, min–max) | 58.7 (21–85) | 63.9 (17–95) | 65 (26–99) |
| <60 | 47.3 | 35.1 | 33.8 |
| 60–79 | 51.2 | 51.1 | 53.0 |
| >80 | 1.5 | 13.8 | 13.1 |
| M (%) | 342 (65.8) | 1101 (67.6) | 119 (60.1) |
| Comorbidities | |||
| Cirrhosis (%) | 503 (96.7) | 179 (11) | 71 (35.9) |
| Renal disease (%) | 8 (1.5) | 125 (7.7) | 14 (7.1) |
| Cardiac disease (%) | 17 (3.3) | 242 (14.9) | 25 (12.6) |
| Metastatic malignancy (%) | 3 (0.6) | 6 (0.4) | 9 (4.6) |
| Medication | |||
| Antiplatelet agents (%) | 3 (0.6) | 106 (6.5) | 6 (3) |
| Anticoagulants (%) | 9 (1.7) | 217 (13.3) | 8 (4) |
| NSAID (%) | 16 (3.1) | 250 (15.4) | 8 (4) |
| Alcohol abuse | 365 (70.2) | 519 (31.9) | 72 (36.4) |
| Mean onset-adm. time (h) | 24.4 | 46.7 | 37.1 |
| Hematemesis (%) | 78.7 | 45.8 | 50 |
| Melena (%) | 89.6 | 86.9 | 81.3 |
| Hematochezia (%) | 5 | 2.6 | 10.1 |
| Laboratory analysis | |||
| Hb | 8.28 | 8.77 | 8.39 |
| Urea | 65.1 | 82.6 | 90.7 |
| Creatinine | 0.96 | 1.24 | 1.56 |
| INR | 1.74 | 1.58 | 1.77 |
| Albumin | 2.70 | 3.27 | 2.82 |
| Mean adm. to endo time (h) | 18.5 | 18.4 | NA |
| Admission to endoscopy (%) | |||
| <12 h | 65.5 | 58 | NA |
| 12–24 h | 20 | 25.9 | NA |
| >24 h | 14.5 | 16.1 | NA |
| Blood transfusions% | 55.2 | 45.9 | 34.8 |
| Rebleeding rate (%) | 38 (7.3) | 68 (4.2) | 1 (0.5) |
| Mean hospital stay (days) | 7.95 | 7.39 | 5.47 |
| In-hospital mortality | 114 (21.9) | 121 (7.4) | 75 (37.9) |
| Death during first 24 h adm. | 17 (14.9) | 13 (10.7) | 17 (22.7) |
| No Endoscopy | VUGIB | p-Value | NVUGIB | p-Value | |
|---|---|---|---|---|---|
| Scores (Mean ± SD) | |||||
| Classic scores | |||||
| Glasgow Blatchford | 10.60 ± 4.11 | 10.71 ± 3.42 | 0.7574 | 9.28 ± 3.69 | <0.0001 |
| Glasgow Blatchford modified | 8.44 ± 3.72 | 7.66 ± 3.25 | 0.0119 | 7.62 ± 3.34 | 0.0038 |
| Rockall pre-endoscopy | 3.62 ± 1.51 | 4.16 ± 0.96 | <0.0001 | 2.71 ± 1.69 | <0.0001 |
| Baylor pre-endoscopy | 9.07 ± 3.37 | 9.12 ± 2.25 | 0.8193 | 8.09 ± 4.16 | 0.0014 |
| AIM65 | 1.76 ± 1.19 | 1.68 ± 0.99 | 0.4464 | 1.12 ± 0.99 | <0.0001 |
| T-score | 9.62 ± 1.59 | 9.98 ± 1.43 | 0.0070 | 9.95 ± 1.51 | 0.0082 |
| New scores | |||||
| N-score | 3.01 ± 1.86 | 3.15 ± 1.66 | 0.3761 | 2.90 ± 1.85 | 0.4400 |
| Adjusted N-score | 2.64 ± 1.88 | 2.82 ± 1.72 | 0.3046 | 2.54 ± 1.78 | 0.5361 |
| H3B2 | 3.25 ± 1.61 | 3.43 ± 1.47 | 0.2009 | 3.12 ± 1.49 | 0.2752 |
| Iino score | 3.22 ± 2.96 | 3.22 ± 2.31 | 0.9930 | 2.50 ± 2.53 | 0.0009 |
| MAP (ASH) score | 3.34 ± 2.01 | 3.54 ± 1.65 | 0.2565 | 2.38 ± 1.60 | <0.0001 |
| INBS score | |||||
| Charlson comorbidity index (CCI) | 4.28 ± 2.01 | 4.76 ± 1.45 | 0.0004 | 3.37 ± 2.24 | <0.0001 |
| AUC | 95% CI | Significance | |
|---|---|---|---|
| Glasgow Blatchford | 0.783 | 0.712–0.854 | 0.000 |
| Glasgow Blatchford (adjusted) | 0.730 | 0.653–0.807 | 0.000 |
| Rockall pre-endoscopy | 0.686 | 0.606–0.766 | 0.000 |
| Baylor pre-endoscopy | 0.632 | 0.554–0.710 | 0.002 |
| AIM65 | 0.745 | 0.660–0.829 | 0.000 |
| T-score | 0.563 | 0.471–0.656 | 0.168 |
| N-score | 0.701 | 0.622–0.780 | 0.000 |
| mN-score | 0.745 | 0.659–0.831 | 0.000 |
| H3B2 | 0.701 | 0.621–0.780 | 0.000 |
| Iino score | 0.766 | 0.690–0.842 | 0.000 |
| MAP (ASH) score | 0.780 | 0.696–0.865 | 0.000 |
| INBS | 0.844 | 0.781–0.906 | 0.000 |
| CCI | 0.609 | 0.529–0.688 | 0.000 |
| CPT score | 0.706 | 0.557–0.857 | 0.016 |
| Modified CPT | 0.732 | 0.587–0.877 | 0.003 |
| MELD score | 0.811 | 0.699–0.923 | 0.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cazacu, S.M.; Alexandru, D.O.; Statie, R.-C.; Iordache, S.; Ungureanu, B.S.; Iovănescu, V.F.; Popa, P.; Sacerdoțianu, V.M.; Neagoe, C.D.; Florescu, M.M. The Accuracy of Pre-Endoscopic Scores for Mortality Prediction in Patients with Upper GI Bleeding and No Endoscopy Performed. Diagnostics 2023, 13, 1188. https://doi.org/10.3390/diagnostics13061188
Cazacu SM, Alexandru DO, Statie R-C, Iordache S, Ungureanu BS, Iovănescu VF, Popa P, Sacerdoțianu VM, Neagoe CD, Florescu MM. The Accuracy of Pre-Endoscopic Scores for Mortality Prediction in Patients with Upper GI Bleeding and No Endoscopy Performed. Diagnostics. 2023; 13(6):1188. https://doi.org/10.3390/diagnostics13061188
Chicago/Turabian StyleCazacu, Sergiu Marian, Dragoș Ovidiu Alexandru, Răzvan-Cristian Statie, Sevastița Iordache, Bogdan Silviu Ungureanu, Vlad Florin Iovănescu, Petrică Popa, Victor Mihai Sacerdoțianu, Carmen Daniela Neagoe, and Mirela Marinela Florescu. 2023. "The Accuracy of Pre-Endoscopic Scores for Mortality Prediction in Patients with Upper GI Bleeding and No Endoscopy Performed" Diagnostics 13, no. 6: 1188. https://doi.org/10.3390/diagnostics13061188