
Masked Hypertension and Exaggerated Blood Pressure Response to Exercise: A Review and Meta-Analysis
 , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Methods
Statistical Analysis
3. Results
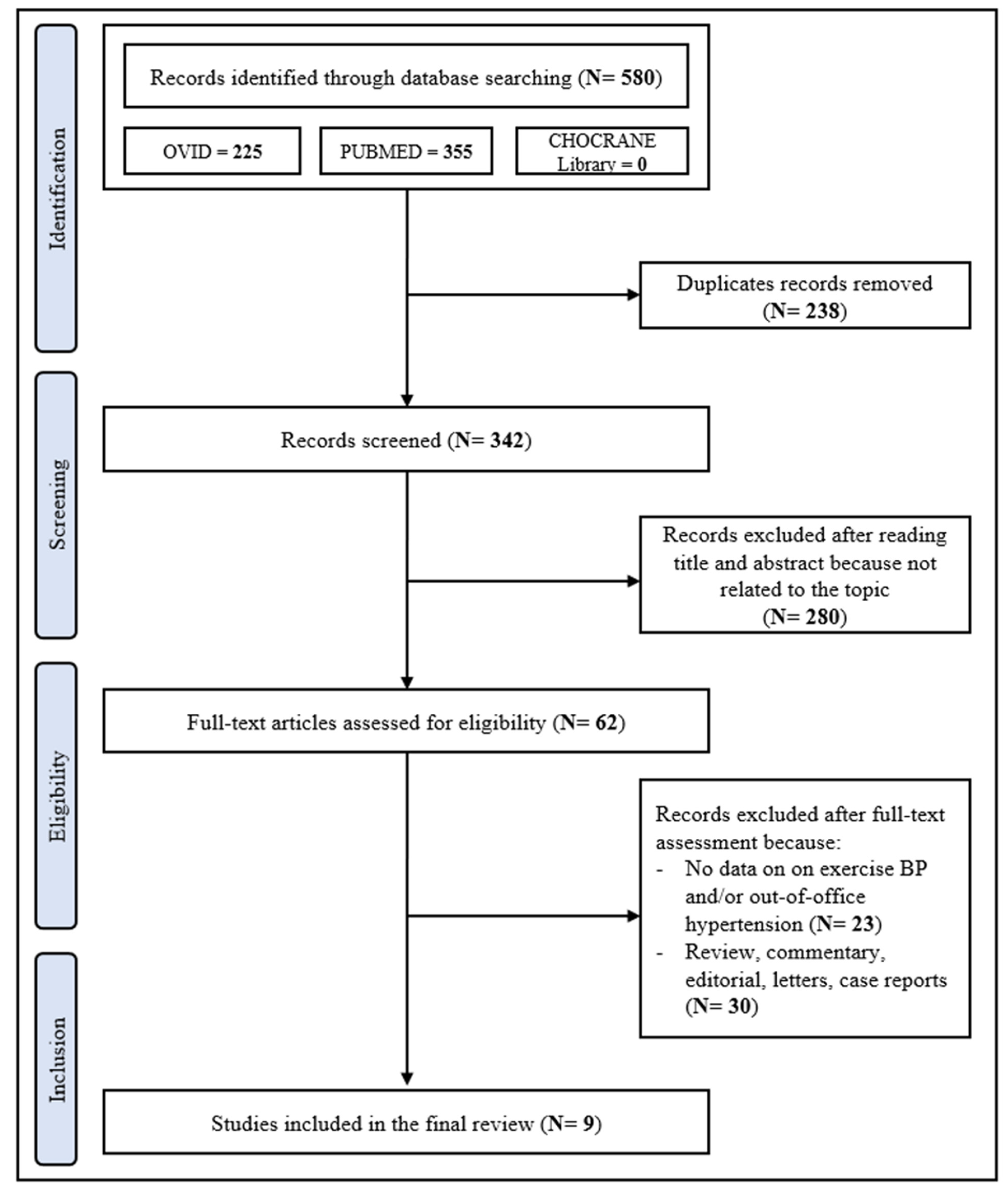
3.1. Search Results
3.2. Main Study Features
3.3. Demographic and Clinical Data in MH and Normotensive controls
3.4. Publication Bias
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension global hypertension practice guidelines. J. Hypertens. 2020, 38, 982–1004. [Google Scholar] [CrossRef]
- Sivén, S.S.; Niiranen, T.J.; Langén, V.L.; Puukka, P.J.; Kantola, I.M.; Jula, A.M. Home versus office blood pressure: Longitudinal relations with left ventricular hypertrophy: The Finn-Home study. J. Hypertens. 2017, 35, 266–271. [Google Scholar] [CrossRef]
- Botha, D.; Breet, Y.; Schutte, A.E. Comparing the associations of clinic vs. ambulatory blood pressure with subclinical organ damage in young healthy adults: The African-PREDICT study. Hypertens. Res. 2021, 44, 840–849. [Google Scholar] [CrossRef] [PubMed]
- Manousopoulos, K.; Koroboki, E.; Barlas, G.; Lykka, A.; Tsoutsoura, N.; Flessa, K.; Kanakakis, I.; Paraskevaidis, I.; Zakopoulos, N.; Manios, E. Association of home and ambulatory blood pressure variability with left ventricular mass index in chronic kidney disease patients. Hypertens. Res. 2021, 44, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Sega, R.; Facchetti, R.; Bombelli, M.; Cesana, G.; Corrao, G.; Grassi, G.; Mancia, G. Prognostic value of ambulatory and home blood pressures compared with office blood pressure in the general population: Follow-up results from the Pressioni Arteriose Monitorate e Loro Associazioni (PAMELA) study. Circulation 2005, 111, 1777–1778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J. Hypertens. 2018, 36, 2284–2309. [Google Scholar] [PubMed] [Green Version]
- Mancia, G.; Facchetti, R.; Bombelli, M.; Cuspidi, C.; Grassi, G. White-coat hypertension: Pathophysiological and clinical aspects: Excellence award for hypertension research. 2020. Hypertension 2021, 78, 1677–1688. [Google Scholar] [CrossRef]
- Coccina, F.; Borrelli, P.; Pierdomenico, A.M.; Pizzicannella, J.; Guagnano, M.T.; Cuccurullo, C.; Di Nicola, M.; Renda, G.; Trubiani, O.; Cipollone, F.; et al. Prediction of masked uncontrolled hypertension detected by ambulatory blood pressure monitoring. Diagnostics 2022, 12, 3156. [Google Scholar] [CrossRef]
- Omboni, S.; Aristizabal, D.; De la Sierra, A.; Dolan, E.; Head, G.; Kahan, T.; Kantola, I.; Kario, K.; Kawecka-Jaszcz, K.; Malan, L.; et al. ARTEMIS (International Ambulatory blood pressure Registry: TEleMonitoring of hypertension and cardiovascular rISk project) Investigators. Hypertension types defined by clinic and ambulatory blood pressure in 14–143 patients referred to hypertension clinics worldwide. Data from the ARTEMIS study. J. Hypertens. 2016, 34, 2187–2198. [Google Scholar]
- Xia, J.H.; Zhang, D.Y.; Kang, Y.Y.; Guo, Q.H.; Cheng, Y.B.; Huang, J.F.; Huang, Q.F.; Zhang, W.; Zhang, L.J.; Dou, Y.; et al. The prevalence of masked hypertension and masked uncontrolled hypertension in relation to overweight and obesity in a nationwide registry in China. Hypertens. Res. 2022, 45, 1690–1700. [Google Scholar] [CrossRef]
- Cuspidi, C.; Sala, C.; Grassi, G.; Mancia, G. White coat hypertension: To treat or not to treat? Curr. Hypertens. Rep. 2016, 18, 80. [Google Scholar] [CrossRef] [PubMed]
- Mancia, G.; Bombelli, M.; Facchetti, R.; Madotto, F.; Quarti-Trevano, F.; Polo Friz, H.; Grassi, G.; Sega, R. Long-term risk of sustained hypertension in white-coat or masked hypertension. Hypertension 2009, 54, 226–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pierdomenico, S.D.; Cuccurullo, F. Prognostic value of white-coat and masked hypertension diagnosed by ambulatory monitoring in initially untreated subjects: An updated meta analysis. Am. J. Hypertens. 2011, 24, 52–58. [Google Scholar] [CrossRef] [Green Version]
- Holanger, M.; Kjeldsen, S.E.; Jamerson, K.; Julius, S. HOT Study investigators. Smoking and overweight associated with masked uncontrolled hypertension:a Hypertension Optimal Treatment (HOT) Sub-Study. Blood Press. 2021, 30, 51–59. [Google Scholar] [CrossRef]
- Pickering, T.G. The natural history of hypertension: Pre-hypertension or masked hypertension? J. Clin. Hypertens. 2007, 9, 807–810. [Google Scholar] [CrossRef] [Green Version]
- Shimbo, D.; Newman, J.D.; Schwartz, J.E. Masked hypertension and pre-hypertension: Diagnostic overlap and interrelationships with left ventricular mass: The Masked Hypertension Study. Am. J. Hypertens. 2012, 25, 664–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shultz, M.G.; Sharman, J.E. Exercise hypertension. Pulse 2013, 1, 161–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manolio, T.A.; Burke, G.L.; Savage, P.J.; Sidney, S.; Gardin, J.M.; Oberman, A. Exercise blood pressure response and 5-year risk of elevated blood pressure in a cohort of young adults: The CARDIA study. Am. J. Hypertens. 1994, 7, 234–241. [Google Scholar] [CrossRef]
- Caselli, S.; Serdoz, A.; Mango, F.; Lemme, E.; Vaquer Seguì, A.; Milan, A.; Attenhofer Jost, C.; Schmied, C.; Spataro, A.; Pelliccia, A. High blood pressure response to exercise predicts future development of hypertension in young athletes. Eur. Heart J. 2019, 40, 62–68. [Google Scholar] [CrossRef] [Green Version]
- Perçuku, L.; Bajraktari, G.; Jashari, H.; Bytyçi, I.; Ibrahimi, P.; Henein, M.Y. Exaggerated systolic hypertensive response to exercise predicts cardiovascular events: A systematic review and meta-analysis. Pol. Arch. Intern Med. 2019, 129, 855–863. [Google Scholar] [CrossRef]
- Kramer, C.K.; Leitão, C.B.; Canani, L.H.; Ricardo, E.D.; Pinto, L.C.; Gross, J.L. Blood pressure responses to exercise in type II diabetes mellitus patients with masked hypertension. J. Hum. Hypertens. 2009, 23, 620–622. [Google Scholar] [CrossRef]
- Kayrak, M.; Bacaksiz, A.; Vatankulu, M.A.; Ayhan, S.S.; Kaya, Z.; Ari, H.; Sonmez, O.; Gok, H. Exaggerated blood pressure response to exercise, a new portent of masked hypertension. Clin. Exp. Hypertens. 2010, 32, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Sharman, J.E.; Hare, J.L.; Thomas, S.; Davies, J.E.; Leano, R.; Jenkins, C.; Marwick, T.H. Association of masked hypertension and left ventricular remodelling with the hypertensive response to exercise. Am. J. Hypertens. 2011, 24, 898–903. [Google Scholar] [CrossRef] [Green Version]
- Akilli, H.; Kayrak, M.; Arıbas, A.; Tekinalp, M.; Ayhan, S.S.; Gündüz, M.; Alibasic, H.; Altunbas, G.; Yazıcı, M. The relationship between exercise capacity and masked hypertension in sedentary patients with diabetes mellitus. Clin. Exp. Hypertens. 2014, 36, 9–16. [Google Scholar] [CrossRef]
- Grossman, A.; Cohen, N.; Shemesh, J.; Koren-Morag, N.; Leibowitz, A.; Grossman, E.J. Exaggerated blood pressure response to exercise is not associated with masked hypertension in patients with high normal blood pressure levels. J. Clin. Hypertens. 2014, 16, 277–282. [Google Scholar] [CrossRef]
- Aung, S.M.; Güler, A.; Güler, Y.; Karabay, C.Y.; Akdemir, I. Two-dimensional speckle-tracking echocardiography-based left atrial strain parameters predict masked hypertension in patients with hypertensive response to exercise. Blood Press. Monit. 2017, 22, 27–33. [Google Scholar] [CrossRef]
- Koletsos, N.; Dipla, K.; Triantafyllou, A.; Gkaliagkousi, E.; Sachpekidis, V.; Zafeiridis, A.; Douma, S. A brief submaximal isometric exercise test ‘unmasks’ systolic and diastolic masked hypertension. J. Hypertens. 2019, 37, 710–719. [Google Scholar] [CrossRef]
- Małek, Ł.A.; Jankowska, A.; Greszata, L. Mild left ventricular hypertrophy in middle-age male athletes as a sign of masked arterial hypertension. Int. J. Environ. Res. Public Health 2022, 19, 10038. [Google Scholar] [CrossRef] [PubMed]
- Inanc, I.H.; Sabanoglu, C. The relationship of masked hypertension with autonomic dysfunction and cardiometabolic parameters: A case-control study. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 6265–6272. [Google Scholar]
- Fletcher, G.F.; Ades, P.A.; Kligfield, P.; Arena, R.; Balady, G.J.; Bittner, V.A.; Coke, L.A.; Fleg, J.L.; Forman, D.E.; Gerber, T.C.; et al. Exercise standards for testing and training: A scientific statement from the American Heart Association. Circulation 2013, 128, 873–934. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, A.; Sharma, S.; Gati, S.; Back, M.; Borjesson, M.; Caselli, S.; Collet, J.P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur. Heart J. 2021, 42, 17–96. [Google Scholar] [CrossRef] [PubMed]
- Currie, K.D.; Floras, J.S.; La Gerche, A.; Goodman, J.M. Exercise blood pressure guidelines: Time to re-evaluate what is normal and exaggerated? Sports Med. 2018, 48, 1763–1771. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Ha, J.W. Hypertensive response to exercise: Mechanisms and clinical implication. Clin. Hypertens. 2016, 22, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, K.J.; Sung, J.; Silber, H.A.; Fleg, J.L.; Kelemen, M.D.; Turner, K.L.; Bacher, A.C.; Dobrosielski, D.A.; De Regis, J.R.; Shapiro, E.P.; et al. Exaggerated exercise blood pressure is related to impaired endothelial vasodilator function. Am. J. Hypertens. 2004, 17, 314–320. [Google Scholar] [CrossRef] [Green Version]
- Miyai, N.; Shiozaki, M.; Terada, K.; Takeshita, T.; Utsumi, M.; Miyashita, K.; Arita, M. Exaggerated blood pressure response to exercise is associated with subclinical vascular impairment in healthy normotensive individuals. Clin. Exp. Hypertens. 2021, 43, 56–62. [Google Scholar] [CrossRef]
- Bond, V.; Curry, B.H.; Adams, R.G.; Obisesan, T.; Pemminati, S.; Gorantla, V.R.; Kadur, K.; Millis, R.M. Cardiovascular responses to an isometric handgrip exercise in females with prehypertension. N. Am. J. Med. Sci. 2016, 8, 243–249. [Google Scholar]
- Sénéchal-Dumais, I.; Auclair, A.; Leclerc, J.; Poirier, P. Effect of bariatric surgery on blood pressure response to exercise in a severely obese population. Blood Press. Monit. 2021, 26, 357–363. [Google Scholar] [CrossRef]
- Cuspidi, C.; Sala, C.; Tadic, M.; Grassi, G. When office blood pressure is not enough: The case of masked hypertension. Am. J. Hypertens. 2019, 32, 225–233. [Google Scholar] [CrossRef] [Green Version]
- Cuspidi, C.; Facchetti, R.; Quarti-Trevano, F.; Sala, C.; Tadic, M.; Grassi, G.; Mancia, G. Incident left ventricular hypertrophy in masked hypertension. Hypertension 2019, 74, 56–62. [Google Scholar] [CrossRef]
- Mallion, J.M.; Clerson, P.; Bobrie, G.; Genes, N.; Vaisse, B.; Chatellier, G. Predictive factors for masked hypertension within a population of controlled hypertensives. J. Hypertens. 2006, 24, 2365–2370. [Google Scholar] [CrossRef]
- Obara, T.; Ohkubo, T.; Funahashi, J.; Kikuya, M.; Asayama, K.; Metoki, H.; Oikawa, T.; Hashimoto, J.; Totsune, K.; Imai, Y. Isolated uncontrolled hypertension at home and in the office among treated hypertensive patients from the J-HOME study. J. Hypertens. 2005, 23, 1653–1660. [Google Scholar] [CrossRef] [PubMed]
- Cacciolati, C.; Hanon, O.; Alpérovitch, A.; Dufouil, C.; Tzourio, C. Masked hypertension in the elderly: Cross-sectional analysis of a population-based sample. Am. J. Hypertens. 2011, 24, 674–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barroso, W.K.S.; Feitosa, A.D.M.; Barbosa, E.C.D.; Miranda, R.D.; Brandão, A.A.; Vitorino, P.V.O.; Ribeiro, L.P.S.; Gomes, M.M. Prevalence of masked and white-coat hypertension in pre-hypertensive and stage 1 hypertensive patients with the use of TeleMRPA. Arq. Bras. Cardiol. 2019, 113, 970–975. [Google Scholar] [CrossRef] [PubMed]
- Omboni, S.; Ballatore, T.; Rizzi, F.; Tomassini, F.; Campolo, L.; Panzeri, E. Age-related patterns of ambulatory blood pressure in a large cohort of individuals referred to Italian community pharmacies: Results from the TEMPLAR project. J. Hypertens. 2023, 41, 336–343. [Google Scholar] [CrossRef]
- Moore, M.N.; Climie, R.E.; Otahal, P.; Sharman, J.E.; Schultz, M.G. Exercise blood pressure and cardiac structure: A systematic review and meta-analysis of cross-sectional studies. J. Sci. Med. Sport. 2021, 24, 925–930. [Google Scholar] [CrossRef]
- Levy, R.L.; White, P.D.; Stroud, W.D.; Hillman, C.C. Transient tachycardia: Prognostic significance alone and in association with transient hypertension. JAMA 1945, 129, 585–588. [Google Scholar] [CrossRef]
- Grassi, G.; Seravalle, G.; Quarti-Trevano, F.; Dell’Oro, R.; Bombelli, M.; Cuspidi, C.; Facchetti, R.; Bolla, G.; Mancia, G. Adrenergic, metabolic, and reflex abnormalities in reverse and extreme dipper hypertensives. Hypertension 2008, 52, 925–931. [Google Scholar] [CrossRef] [Green Version]
- Grassi, G.; Seravalle, G.; Trevano, F.Q.; Dell’Oro, R.; Bolla, G.; Cuspidi, C.; Arenare, F.; Mancia, G. Neurogenic abnormalities in masked hypertension. Hypertension 2007, 50, 537–542. [Google Scholar] [CrossRef] [Green Version]
- Călin, P.; Viorel, M.; Luchiana, P.; Mihaela, C.; Lavinia, P. Masked nocturnal hypertension as a result of high prevalence of non-dippers among apparently well-controlled hypertensive patients with type 2 diabetes mellitus: Data from a prospective study. Diabetol. Metab. Syndr. 2022, 14, 130. [Google Scholar] [CrossRef]
- Kario, K.; Hoshide, S.; Nagai, M.; Okawara, Y.; Kanegae, H. Sleep and cardiovascular outcomes in relation to nocturnal hypertension: The J-HOP Nocturnal Blood Pressure Study. Hypertens. Res. 2021, 44, 1589–1596. [Google Scholar] [CrossRef]
- Cuspidi, C.; Facchetti, R.; Quarti-Trevano, F.; Dell’Oro, R.; Tadic, M.; Grassi, G.; Mancia, G. Left ventricular hypertrophy in isolated and dual masked hypertension. J. Clin. Hypertens. 2020, 22, 673–677. [Google Scholar] [CrossRef] [PubMed]
- Mancia, G.; Facchetti, R.; Cuspidi, C.; Bombelli, M.; Corrao, G.; Grassi, G. Limited reproducibility of MUCH and WUCH: Evidence from the ELSA study. Eur. Heart J. 2020, 41, 1565–1571. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author [Reference] Year Publication | Type of Study | Sample Size (n) | Men (%) | Age (years) | BMI (kg/m2) | Setting | Exercise Testing | EBPR Definition | EBPR (%) | MH (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| Kramer [21] 2009 | Observational cross-sectional case-control study | 61 | 49 | 53 ± 9 | 28.2 ± 4.2 | DM | Treadmill | SBP > 180 mmHg | 41 | 39 |
| Kairak [22] 2010 | Observational cross-sectional study | 61 | 79 | 47 ± 10 | 28.5 ± 4.5 | Healthy subjects with EBPR | Treadmill | SBP ≥ 210 (M), ≥190 mmHg (F) | 100 | 41 |
| Sharman [23] 2011 | Observational cross-sectional study | 72 | 60 | 54 ± 9 | 28.6 ± 3.9 | Healthy subjects with EBPR | Treadmill | BP ≥ 210/105 (M), ≥190/105 mmHg (F) | 100 | 58 |
| Akilli [24] 2014 | Observational cross-sectional study | 85 | 62 | 51 ± 8 | 30.1 ± 5.1 | DM | Treadmill | BP > 200/100 mmHg | 13 | 28 |
| Grossman [25] 2014 | Retrospective observational cross-sectional study | 69 | 87 | 54 ± 9 | 27.2 ± 3.1 | Healthy subjects with high-normal BP | Treadmill | SBP ≥ 200 mmHg | 62 | 72 |
| Aung [26] 2017 | Observational cross-sectional study | 98 | 62 | 41 ± 6 | 27.3 ± 1.9 | Healthy subjects with EBPR | Treadmill | SBP > 200 (M), >190 mmHg (F) | 100 | 40 |
| Koletsos [27] 2019 | Observational cross-sectional study | 86 | 56 | 46 ± 10 | 27.0 ± 4.2 | Hypertensive and normotensive subjects | Handgrip | n. a. | n.a. | 31 |
| Malek [28] 2022 | Observational cross-sectional study | 71 | 100 | 41 ± 6 | 24.5 ± 3.0 | Athletes | Treadmill | SBP > 210 mmHg | 30 | 37 |
| Inanc [29] 2022 | Observational cross-sectional study | 190 | 45 | 59 ± 10 | 22.3 ± 1.2 | Masked hypertensive and normotensive subject | Treadmill | SBP ≥ 210 (M), ≥190 mmHg (F) | 22 | 68 |
| OFFICE BP at Rest (mmHg) | DAY-TIME BP (mmHg) | NIGHT-TIME BP (mmHg) | EXERCISE BP (mmHg) | EBPR (%) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Author [Reference] Publication Year | NTN | MH | NTN | MH | NTN | MH | NTN | MH | NTN | MH |
| Kramer [21] 2009 | 122 ± 9/74 ± 6 | 126 ± 6/79 ± 7 | n.a. | n.a. | n.a. | n.a. | 167 ± 16 | 185 ± 22 | 21 | 71 |
| Kairak [22] 2010 | 126 ± 13/84 ± 10 | 129 ± 12/ ± 89 ± 10 | 123 ± 7/77 ± 5 | 142 ± 7/87 ± 6 | 111 ± 8/66 ± 7 | 133 ± 10/81 ± 8 | 209 ± 19/91 ± 9 | 214 ± 9/98 ± 13 | 100 | 100 |
| Sharman [23] 2011 | 121 ± 9/72 ± 6 | 126 ± 10/74 ± 7 | 127 ± 6/78 ± 5 | 142 ± 8/86 ± 6 | 112 ± 5/67 ± 5 | 119 ± 6/71 ± 5 | 212 ± 14/90 ± 10 | 222 ± 17/96 ± 12 | 100 | 100 |
| Akilli [24] 2014 | 121 ± 8/77 ± 6 | 125 ± 8/80 ± 7 | 122 ± 4/78 ± 5 | 140 ± 5/84 ± 4 | 115 ± 10/65 ± 6 | 131 ± 13/74 ± 6 | 155/83 | 168/87 | 8 | 25 |
| Grossman [25] 2014 | 129 ± 7/81 ± 6 | 132 ± 8/82 ± 5 | n. a. | n. a. | n.a. | n.a. | n. a. | n. a. | 73 | 58 |
| Aung [26] 2017 | 130 ± 9/73 ± 5 | 126 ± 11/73 ± 5 | n. a. | n.a. | n.a. | n.a. | n. a. | n. a. | 100 | 100 |
| Koletsos [27] 2019 | 123 ± 9/79 ± 7 | 128 ± 8/81 ± 8 | 121 ± 8/76 ± 6 | 137 ± 7/86 ± 6 | 106 ± 9/63 ± 6 | 116 ± 10/70 ± 7 | 160 ± 16/91 ± 9 | 175 ± 13/98 ± 7 | n. a. | n. a. |
| Malek [28] 2022 | n. a. | n. a. | n. a. | 132 ± 7/80 ± 5 | n.a. | n.a. | n. a. | n. a. | 13 | 51 |
| Inanc [29] 2022 | 120 ± 15/72 ± 11 | 120 ± 15/72 ± 11 | 111 ± 9/73 ± 4 | 164 ± 22/106 ± 15 | 97 ± 9/62 ± 4 | 147 ± 16/89 ± 13 | 140 ± 8/98 ± 11 | 177 ± 18/103 ± 11 | 2 | 31 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cuspidi, C.; Gherbesi, E.; Faggiano, A.; Sala, C.; Carugo, S.; Grassi, G.; Tadic, M. Masked Hypertension and Exaggerated Blood Pressure Response to Exercise: A Review and Meta-Analysis. Diagnostics 2023, 13, 1005. https://doi.org/10.3390/diagnostics13061005
Cuspidi C, Gherbesi E, Faggiano A, Sala C, Carugo S, Grassi G, Tadic M. Masked Hypertension and Exaggerated Blood Pressure Response to Exercise: A Review and Meta-Analysis. Diagnostics. 2023; 13(6):1005. https://doi.org/10.3390/diagnostics13061005
Chicago/Turabian StyleCuspidi, Cesare, Elisa Gherbesi, Andrea Faggiano, Carla Sala, Stefano Carugo, Guido Grassi, and Marijana Tadic. 2023. "Masked Hypertension and Exaggerated Blood Pressure Response to Exercise: A Review and Meta-Analysis" Diagnostics 13, no. 6: 1005. https://doi.org/10.3390/diagnostics13061005