
Clinical Characteristics and Current Status of Treatment for Recurrent Bladder Cancer after Surgeries on Upper Tract Urothelial Carcinoma


Abstract
:1. Clonogenic Correlation and Tumor Implantation Theory
2. Comparison of the Characteristics of Recurrent and Primary BC
3. Risk Factors Affecting Recurrent BC
3.1. Patient-Specific Factors
3.1.1. Damaged eGFR
3.1.2. Venerable Age
3.1.3. Gender Difference
3.1.4. Smoking
3.1.5. Diabetes Mellitus with Poor Glycemic Control
3.1.6. Monocyte-to-Lymphocyte Ratio (MLR)
3.1.7. Neutrophil-to-Lymphocyte Ratio (NLR)
3.2. Tumor-Specific Factors
3.2.1. Multifocality of Upper Urinary Tract Tumors
3.2.2. Size of UTUC
3.2.3. Distal Ureteral Position
3.2.4. Lymph Node Involvement
3.2.5. Invasive pT Staging
3.2.6. Papillary Structure of Tumors
3.2.7. Extensive Tumor Necrosis
3.2.8. Concomitant Carcinoma In Situ (CIS)
3.3. Treatment-Specific Factors
3.3.1. Incomplete Excision
3.3.2. Immature Laparoscopic Technique
3.3.3. Surgery Time
3.3.4. Early Ureteral Ligation
3.3.5. Ureteroscopy
3.4. Molecular-Specific Factors
3.4.1. E-Calmodulin
3.4.2. Forkhead Box O3A
3.4.3. HER2
4. Current Treatment Measures for UTUC-BC
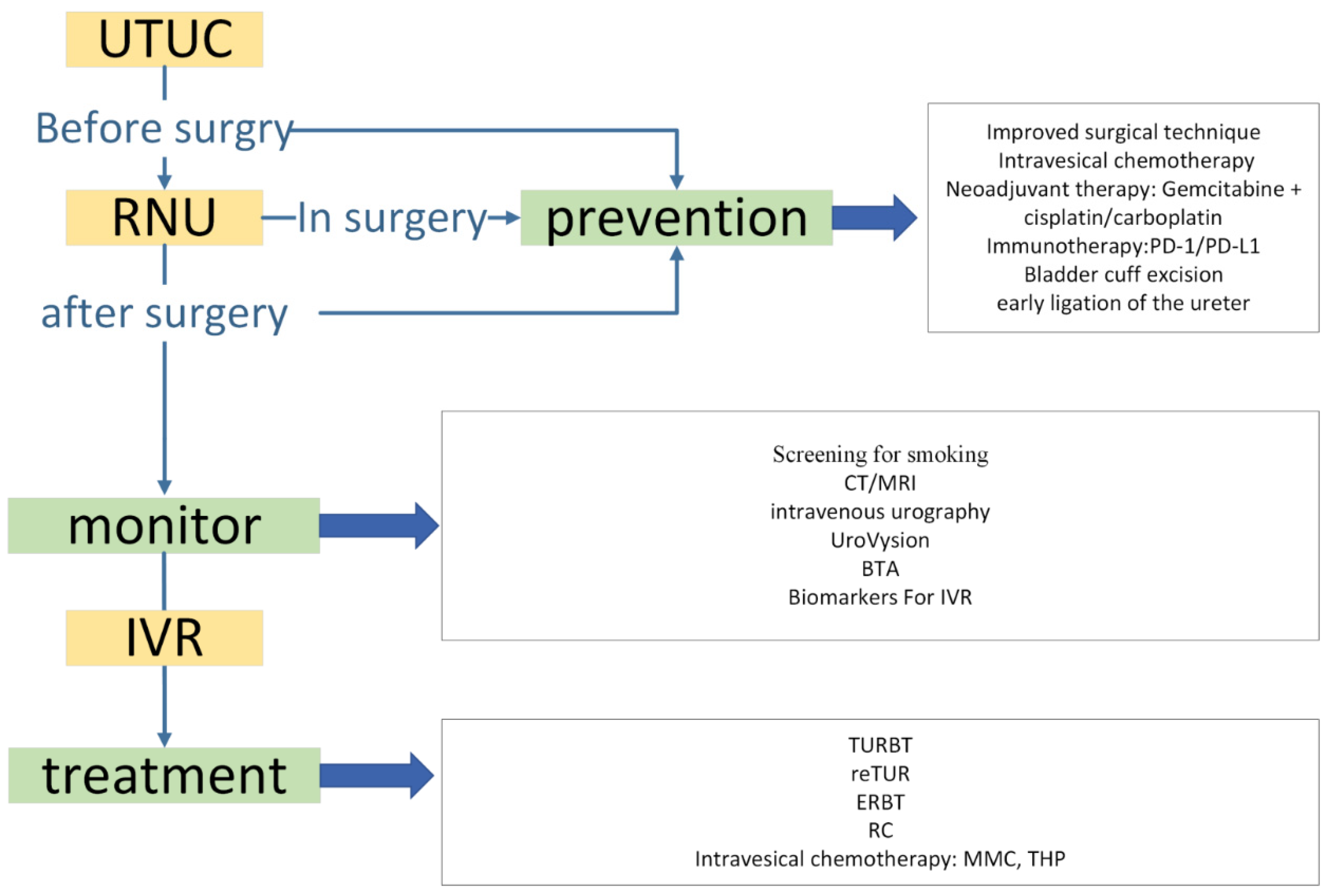
4.1. Prevention
4.1.1. Surgical Techniques
4.1.2. Intravesical Treatment
4.2. Monitoring during the Follow-Up
- Screening for smoking: Smoking is one of the risk factors for recurrence, as mentioned earlier. Crivelli JJ et al. analyzed six studies, estimating the effect of smoking for patients with UTUC after receiving RNU. Most of the studies were found a statistically significant relationship between smoking and IVR. The studies also found that smoking is associated with cancer-specific mortality for patients with UTUC-BC [31], so screening for smoking is also essential.
- Imaging: Computed tomography (CT) and intravenous urography of the bladder and ureter should be performed at least once a year. If necessary, MRI should also be added into the monitoring plan.
- Endoscopy: patients with UTUC must undergo endoscopic surveillance after RNU, and the surveillance program lasts for at least 5 years, with flexible cystoscopy recommended for the surveillance of male patients [14].
- Molecular biomarkers: Various molecular biomarkers can be used to help detect recurrent bladder cancer: e.g., tumor factors, UroVysion, and BTA tests. Using Kaplan–Meier analysis, Guan B et al. showed that UTUC patients with positive UroVysion results were more likely to develop IVR during the follow-up (p = 0.077). These data suggest that the urinary UroVysion test may be a powerful tool for predicting the risk of IVR in patients with UTUC [105]. Walsh et al. performed a study to evaluate the effectiveness of the BTA test in patients with UTUC and found that the sensitivity of the BTA was 82% and the specificity was 89%, which were significantly better than those of the urinalysis in the same group of patients (11% and 54%, respectively) [106]. However, the study conducted by Białek Ł et al. found moderate diagnostic accuracy when they were detecting bladder cancer for patients with UTUC by BTA [107]. Therefore, more evidence is needed for BTA to detect the occurrence of IVR in patients with UTUC. Tumor factors such as E-calmodulin and FGFR3 in molecular-specific factors have been shown to correlate with IVR, so these indicators can also be evaluated during the follow-up period.
4.3. Treatment
4.3.1. TUR-BT
4.3.2. En Bloc Resection of Bladder Tumor (ERBT)
4.3.3. Secondary Resection
4.3.4. Intravesical Chemotherapy
4.3.5. Photodynamic Diagnosis (PDD) and Radical Cystectomy (RC)
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fadl-Elmula, I.; Gorunova, L.; Mandahl, N.; Elfving, P.; Lundgren, R.; Mitelman, F.; Heim, S. Cytogenetic monoclonality in multifocal uroepithelial carcinomas: Evidence of intraluminal tumour seeding. Br. J. Cancer 1999, 81, 6–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, A.; Shintaku, I.; Satoh, M.; Ioritani, N.; Tochigi, T.; Numata, I.; Namima, T.; Kambe, K.; Kyan, A.; Ueno, S.; et al. Intravesical seeding of upper urinary tract urothelial carcinoma cells during nephroureterectomy: An exploratory analysis from the THPMG trial. Jpn. J. Clin. Oncol. 2013, 43, 1139–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habuchi, T. Origin of multifocal carcinomas of the bladder and upper urinary tract: Molecular analysis and clinical implications. Int. J. Urol. 2005, 12, 709–716. [Google Scholar] [CrossRef]
- van Doeveren, T.; van de Werken, H.J.G.; van Riet, J.; Aben, K.K.H.; van Leeuwen, P.J.; Zwarthoff, E.C.; Boormans, J.L. Synchronous and metachronous urothelial carcinoma of the upper urinary tract and the bladder: Are they clonally related? A systematic review. Urol. Oncol. 2020, 38, 590–598. [Google Scholar] [CrossRef] [PubMed]
- Audenet, F.; Isharwal, S.; Cha, E.K.; Donoghue, M.T.A.; Drill, E.N.; Ostrovnaya, I.; Pietzak, E.J.; Sfakianos, J.P.; Bagrodia, A.; Murugan, P.; et al. Clonal Relatedness and Mutational Differences between Upper Tract and Bladder Urothelial Carcinoma. Clin. Cancer Res. 2019, 25, 967–976. [Google Scholar] [CrossRef] [Green Version]
- Van Doeveren, T.; Nakauma-Gonzalez, J.A.; Mason, A.S.; van Leenders, G.J.L.H.; Zuiverloon, T.C.M.; Zwarthoff, E.C.; Meijssen, I.C.; van der Made, A.C.; van der Heijden, A.G.; Hendricksen, K.; et al. The clonal relation of primary upper urinary tract urothelial carcinoma and paired urothelial carcinoma of the bladder. Int. J. Cancer 2021, 148, 981–987. [Google Scholar] [CrossRef] [PubMed]
- Raman, J.D.; Sosa, R.E.; Vaughan, E.D., Jr.; Scherr, D.S. Pathologic features of bladder tumors after nephroureterectomy or segmental ureterectomy for upper urinary tract transitional cell carcinoma. Urology 2007, 69, 251–254. [Google Scholar] [CrossRef]
- Kang, C.H.; Yu, T.J.; Hsieh, H.H.; Yang, J.W.; Shu, K.; Huang, C.C.; Chiang, P.H.; Shiue, Y.L. The development of bladder tumors and contralateral upper urinary tract tumors after primary transitional cell carcinoma of the upper urinary tract. Cancer 2003, 98, 1620–1626. [Google Scholar] [CrossRef]
- Wu, J.; Xu, P.H.; Luo, W.J.; Dai, B.; Shen, Y.J.; Ye, D.W.; Wang, Y.C.; Zhu, Y.P. Intravesical Recurrence After Radical Nephroureterectomy of Upper Urinary Tract Urothelial Carcinoma: A Large Population-Based Investigation of Clinicopathologic Characteristics and Survival Outcomes. Front. Surg. 2021, 22, 590448. [Google Scholar] [CrossRef]
- Fang, D.; Zhang, L.; Li, X.; Yu, W.; Singla, N.; Zhao, G.; Xiong, G.; Song, Y.; He, Q.; He, Z. Presence of Concomitant Non-muscle-invasive Bladder Cancer in Chinese Patients with Upper Tract Urothelial Carcinoma: Risk Factors, Characteristics, and Predictive Value. Ann. Surg. Oncol. 2015, 22, 2789–2798. [Google Scholar] [CrossRef]
- Yates, D.R.; Catto, J.W. Distinct patterns and behaviour of urothelial carcinoma with respect to anatomical location: How molecular biomarkers can augment clinico-pathological predictors in upper urinary tract tumours. World J. Urol. 2013, 31, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Shigeta, K.; Matsumoto, K.; Ogihara, K.; Murakami, T.; Anno, T.; Umeda, K.; Izawa, M.; Baba, Y.; Sanjo, T.; Shojo, K.; et al. The clinicopathological characteristics of muscle-invasive bladder recurrence in upper tract urothelial carcinoma. Cancer Sci. 2021, 112, 1084–1094. [Google Scholar] [CrossRef] [PubMed]
- Miyake, M.; Tatsumi, Y.; Matsumoto, H.; Nagao, K.; Matsuyama, H.; Inamoto, T.; Azuma, H.; Yasumoto, H.; Shiina, H. Outcomes of subsequent non-muscle-invasive bladder cancer treated with intravesical Bacillus Calmette-Guerin after radical nephroureterectomy for upper urinary tract urothelial carcinoma. BJU Int. 2018, 121, 764–773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roupret, M.; Babjuk, M.; Compérat, E.; Zigeuner, R.; Sylvester, R.J.; Burger, M.; Cowan, N.C.; Gontero, P.; Van Rhijn, B.W.G.; Mostafid, A.H.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2017 Update. Eur. Urol. 2018, 73, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Xylinas, E.; Kluth, L.; Passoni, N.; Trinh, Q.D.; Rieken, M.; Lee, R.K.; Fajkovic, H.; Novara, G.; Margulis, V.; Raman, J.D.; et al. Prediction of intravesical recurrence after radical nephroureterectomy: Development of a clinical decision-making tool. Eur. Urol. 2014, 65, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, N.; Kikuchi, E.; Kanao, K.; Matsumoto, K.; Kobayashi, H.; Ide, H.; Miyazaki, Y.; Obata, J.; Hoshino, K.; Shirotake, S.; et al. Metastatic behavior of upper tract urothelial carcinoma after radical nephroureterectomy: Association with primary tumor location. Ann. Surg. Oncol. 2014, 21, 1038–1045. [Google Scholar] [CrossRef] [PubMed]
- Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Dominguez Escrig, J.L.; Gontero, P.; Liedberg, F.; Masson-Lecomte, A.; Mostafid, A.H.; et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (Ta, T1, and Carcinoma in Situ). Eur. Urol. 2022, 1, 75–94. [Google Scholar] [CrossRef]
- Freifeld, Y.; Krabbe, L.M.; Clinton, T.N.; Woldu, S.L.; Margulis, V. Therapeutic strategies for upper tract urothelial carcinoma. Expert Rev. Anticancer Ther. 2018, 8, 765–774. [Google Scholar] [CrossRef]
- Rouprêt, M.; Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Cowan, N.C.; Dominguez-Escrig, J.L.; Gontero, P.; Mostafid., A.H.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2020 Update. Eur. Urol. 2021, 1, 62–79. [Google Scholar] [CrossRef]
- Kuroda, K.; Asakuma, J.; Horiguchi, A.; Kawaguchi, M.; Shinchi, M.; Masunaga, A.; Tasaki, S.; Sato, A.; Ito, K. Chronic kidney disease and positive surgical margins as prognosticators for upper urinary tract urothelial carcinoma patients undergoing radical nephroureterectomy. Mol. Clin. Oncol. 2019, 10, 547–554. [Google Scholar] [CrossRef] [Green Version]
- Xylinas, E.; Rink, M.; Margulis, V.; Clozel, T.; Lee, R.K.; Comploj, E.; Novara, G.; Raman, J.D.; Lotan, Y.; Weizer, A.; et al. Impact of renal function on eligibility for chemotherapy and survival in patients who have undergone radical nephro-ureterectomy. BJU Int. 2013, 112, 453–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasool, M.; Ashraf, M.A.; Malik, A.; Waquar, S.; Khan, S.A.; Qazi, M.H.; Ahmad, W.; Asif, M.; Khan, S.U.; Zaheer, A.; et al. Comparative study of extrapolative factors linked with oxidative injury and anti-inflammatory status in chronic kidney disease patients experiencing cardiovascular distress. PLoS ONE 2017, 12, e0171561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chowdhury, R.; Peel, N.M.; Krosch, M.; Hubbard, R.E. Frailty and chronic kidney disease: A systematic review. Arch. Gerontol. Geriatr. 2017, 68, 135–142. [Google Scholar] [CrossRef] [Green Version]
- Chromecki, T.F.; Ehdaie, B.; Novara, G.; Pummer, K.; Zigeuner, R.; Seitz, C.; Pycha, A.; Lee, R.K.; Cha, E.K.; Karakiewicz, P.I.; et al. Chronological age is not an independent predictor of clinical outcomes after radical nephroureterectomy. World J. Urol. 2011, 29, 473–480. [Google Scholar] [CrossRef]
- Shariat, S.F.; Godoy, G.; Lotan, Y.; Droller, M.; Karakiewicz, P.I.; Raman, J.D.; Isbarn, H.; Weizer, A.; Remzi, M.; Roscigno, M.; et al. Advanced patient age is associated with inferior cancer-specific survival after radical nephroureterectomy. BJU Int. 2010, 105, 1672–1677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chien, T.M.; Li, C.C.; Lu, Y.M.; Chang, H.W.; Chou, Y.H.; Wu, W.J. Prognostic value of renal function for upper tract urothelial carcinoma who underwent radical nephroureterectomy: Sex differences. J. Formos. Med. Assoc. 2022, 121, 2182–2190. [Google Scholar] [CrossRef]
- Chen, C.H.; Dickman, K.G.; Moriya, M.; Zavadil, J.; Sidorenko, V.S.; Edwards, K.L.; Gnatenko, D.V.; Wu, L.; Turesky, R.J.; Wu, X.R.; et al. Aristolochic acid-associated urothelial cancer in Taiwan. Proc. Natl. Acad. Sci. USA 2012, 109, 8241–8246. [Google Scholar] [CrossRef] [Green Version]
- Ploussard, G.; Xylinas, E.; Lotan, Y.; Novara, G.; Margulis, V.; Rouprêt, M.; Matsumoto, K.; Karakiewicz, P.I.; Montorsi, F.; Remzi, M.; et al. Conditional survival after radical nephroureterectomy for upper tract carcinoma. Eur. Urol. 2015, 67, 803–812. [Google Scholar] [CrossRef]
- Seisen, T.; Granger, B.; Colin, P.; Léon, P.; Utard, G.; Renard-Penna, R.; Compérat, E.; Mozer, P.; Cussenot, O.; Shariat, S.F.; et al. A Systematic Review and Meta-analysis of Clinicopathologic Factors Linked to Intravesical Recurrence After Radical Nephroureterectomy to Treat Upper Tract Urothelial Carcinoma. Eur. Urol. 2015, 67, 1122–1133. [Google Scholar] [CrossRef]
- Xylinas, E.; Kluth, L.A.; Rieken, M.; Lee, R.K.; Elghouayel, M.; Ficarra, V.; Margulis, V.; Lotan, Y.; Rouprêt, M.; Martinez-Salamanca, J.I.; et al. UTUC Collaboration. Impact of smoking status and cumulative exposure on intravesical recurrence of upper tract urothelial carcinoma after radical nephroureterectomy. BJU Int. 2014, 114, 56–61. [Google Scholar] [CrossRef]
- Crivelli, J.J.; Xylinas, E.; Kluth, L.A.; Rieken, M.; Rink, M.; Shariat, S.F. Effect of smoking on outcomes of urothelial carcinoma: A systematic review of the literature. Eur. Urol. 2014, 65, 742–754. [Google Scholar] [CrossRef] [PubMed]
- Ehdaie, B.; Furberg, H.; Zabor, E.C.; Ostroff, J.S.; Shariat, S.F.; Bochner, B.H.; Coleman, J.A.; Dalbagni, G. Impact of smoking status at diagnosis on disease recurrence and death in upper tract urothelial carcinoma. BJU Int. 2013, 111, 589–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tai, Y.S.; Chen, C.H.; Huang, C.Y.; Tai, H.C.; Wang, S.M.; Pu, Y.S. Diabetes mellitus with poor glycemic control increases bladder cancer recurrence risk in patients with upper urinary tract urothelial carcinoma. Diabetes Metab. Res. Rev. 2015, 31, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Zhou, L.; Ai, J.; Wang, W.; Di, X.; Peng, L.; Liao, B.; Jin, X.; Li, H.; Wang, K. The Impact of Diabetes on the Prognosis of Upper Tract Urothelial Carcinoma after Radical Nephroureterectomy: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 11, 741145. [Google Scholar] [CrossRef] [PubMed]
- Duan, W.; Shen, X.; Lei, J.; Xu, Q.; Yu, Y.; Li, R.; Wu, E.; Ma, Q. Hyperglycemia, a neglected factor during cancer progression. BioMed Res. Int. 2014, 2014, 461917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Wu, P.; Lai, S.; Song, X.; Fu, C.; Wang, X.; Liu, S.; Hou, H.; Liu, M.; Wang, J. Preoperative Monocyte-to-lymphocyte Ratio Predicts for Intravesical Recurrence in Patients with Urothelial Carcinoma of the Upper Urinary Tract after Radical Nephroureterectomy without a History of Bladder Cancer. Clin. Genitourin. Cancer 2021, 19, e156–e165. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.K.; Yang, P.; Zhang, Z.L.; Hu, W.M.; Cao, Y. Preoperative low lymphocyte-to-monocyte ratio predicts poor clinical outcomes for patients with urothelial carcinoma of the upper urinary tract. Urol. J. 2018, 15, 348–354. [Google Scholar] [PubMed]
- Mathieu, R.; Vartolomei, M.D.; Mbeutcha, A.; Karakiewicz, P.I.; Briganti, A.; Roupret, M.; Shariat, S.F. Urothelial cancer of the upper urinary tract: Emerging biomarkers and integrative models for risk stratification. Minerva Urol. Nefrol. 2016, 4, 381–395. [Google Scholar]
- De Larco, J.E.; Wuertz, B.R.; Furcht, L.T. The potential role of neutrophils in promoting the metastatic phenotype of tumors releasing interleukin-8. Clin. Cancer Res. 2004, 15, 4895–4900. [Google Scholar] [CrossRef] [Green Version]
- Vartolomei, M.D.; Kimura, S.; Ferro, M.; Vartolomei, L.; Foerster, B.; Abufaraj, M.; Shariat, S.F. Is neutrophil-to-lymphocytes ratio a clinical relevant preoperative biomarker in upper tract urothelial carcinoma? A meta-analysis of 4385 patients. World J. Urol. 2018, 7, 1019–1029. [Google Scholar] [CrossRef]
- Vartolomei, M.D.; Mathieu, R.; Margulis, V.; Karam, J.A.; Rouprêt, M.; Lucca, I.; Mbeutcha, A.; Seitz, C.; Karakiewicz, P.I.; Fajkovic, H.; et al. Promising role of preoperative neutrophil-to-lymphocyte ratio in patients treated with radical nephroureterectomy. World J. Urol. 2017, 1, 121–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milojevic, B.; Bumbasirevic, U.; Santric, V.; Kajmakovic, B.; Dragicevic, D.; Radisavcevic, D.; Sretenovic, M.; Grujicic, S.S. Prognostic significance of tumor multifocality on outcomes in patients with upper tract urothelial carcinoma after radical nephroureterectomy: A cohort study. Curr. Probl. Cancer 2021, 45, 100747. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.S.; Li, J.R.; Wang, S.S.; Yang, C.K.; Cheng, C.L.; Yang, C.R.; Ou, Y.C.; Ho, H.C.; Lin, C.Y.; Hung, S.C.; et al. Tumor Multifocality is a Significant Risk Factor of Urinary Bladder Recurrence after Nephroureterectomy in Patients with Upper Tract Urothelial Carcinoma: A Single-Institutional Study. Diagnostics 2020, 10, 201. [Google Scholar] [CrossRef] [Green Version]
- Sheu, Z.L.; Huang, C.P.; Chang, C.H.; Chen, C.H.; Hong, J.H.; Weng, H.Y.; Tai, T.Y.; Chung, S.D.; Lo, C.W.; Hsueh, T.Y.; et al. Tumor distribution affects bladder recurrence but not survival outcome of multifocal upper tract urothelial carcinoma treated with radical nephroureterectomy. Sci. Rep. 2021, 11, 19059. [Google Scholar] [CrossRef] [PubMed]
- Chromecki, T.F.; Cha, E.K.; Fajkovic, H.; Margulis, V.; Novara, G.; Scherr, D.S.; Lotan, Y.; Raman, J.D.; Kassouf, W.; Bensalah, K.; et al. The impact of tumor multifocality on outcomes in patients treated with radical nephroureterectomy. Eur. Urol. 2012, 61, 245–253. [Google Scholar] [CrossRef]
- Kauffman, E.C.; Raman, J.D. Bladder cancer following upper tract urothelial carcinoma. Expert Rev. Anticancer Ther. 2008, 8, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Shibing, Y.; Liangren, L.; Qiang, W.; Hong, L.; Turun, S.; Junhao, L.; Lu, Y.; Zhengyong, Y.; Yonghao, J.; Guangqing, F.; et al. Impact of tumour size on prognosis of upper urinary tract urothelial carcinoma after radical nephroureterectomy: A multi-institutional analysis of 795 cases. BJU Int. 2016, 118, 902–910. [Google Scholar] [CrossRef] [Green Version]
- Espiritu, P.N.; Sverrisson, E.F.; Sexton, W.J.; Pow-Sang, J.M.; Poch, M.A.; Dhillon, J.; Spiess, P.E. Effect of tumor size on recurrence-free survival of upper tract urothelial carcinoma following surgical resection. Urol. Oncol. 2014, 32, 619–624. [Google Scholar] [CrossRef]
- Su, X.; Fang, D.; Li, X.; Li, X.; Xiong, G.; Zhang, L.; Hao, H.; Gong, Y.; Zhang, Z.; Zhou, L. The Influence of Tumor Size on Oncologic Outcomes for Patients with Upper Tract Urothelial Carcinoma after Radical Nephroureterectomy. BioMed Res. Int. 2016, 2016, 4368943. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; Dong, Q.; Liu, L.; Han, P.; Wei, Q. The impact of tumor location and multifocality on prognosis for patients with upper tract urothelial carcinoma: A meta-analysis. Sci. Rep. 2014, 15, 6361. [Google Scholar] [CrossRef] [Green Version]
- Arancibia, M.F.; Bolenz, C.; Michel, M.S.; Keeley, F.X., Jr.; Alken, P. The modern management of upper tract urothelial cancer: Surgical treatment. BJU Int. 2007, 99, 978–981. [Google Scholar] [CrossRef] [PubMed]
- Roscigno, M.; Brausi, M.; Heidenreich, A.; Lotan, Y.; Margulis, V.; Shariat, S.F.; Van Poppel, H.; Zigeuner, R. Lymphadenectomy at the time of nephroureterectomy for upper tract urothelial cancer. Eur. Urol. 2011, 4, 776–783. [Google Scholar] [CrossRef]
- Novara, G.; De Marco, V.; Gottardo, F.; Dalpiaz, O.; Bouygues, V.; Galfano, A.; Martignoni, G.; Patard, J.J.; Artibani, W.; Ficarra, V. Independent predictors of cancer-specific survival in transitional cell carcinoma of the upper urinary tract: Multi-institutional dataset from 3 European centers. Cancer 2007, 8, 1715–1722. [Google Scholar] [CrossRef] [PubMed]
- Verhoest, G.; Shariat, S.F.; Chromecki, T.F.; Raman, J.D.; Margulis, V.; Novara, G.; Seitz, C.; Remzi, M.; Rouprêt, M.; Scherr, D.S.; et al. Predictive factors of recurrence and survival of upper tract urothelial carcinomas. World J. Urol. 2011, 29, 495–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peyrottes, A.; Califano, G.; Ouzaïd, I.; Lainé-Caroff, P.; Depaquit, T.L.; Hermieu, J.F.; Xylinas, E. Lymph Node Dissection During Radical Nephro-Ureterectomy for Upper Tract Urothelial Carcinoma: A Review. Front. Surg. 2022, 24, 852969. [Google Scholar] [CrossRef]
- Li, Y.R.; Yu, K.J.; Chang, Y.H.; Lin, P.H.; Shao, I.H.; Kan, H.C.; Chu, Y.C.; Chuang, C.K.; Pang, S.T.; Liu, C.Y. Predictors of Intravesical Recurrence After Radical Nephroureterectomy and Prognosis in Patients with Upper Tract Urothelial Carcinoma. Cancer Manag. Res. 2020, 12, 7439–7450. [Google Scholar] [CrossRef] [PubMed]
- Remzi, M.; Haitel, A.; Margulis, V.; Karakiewicz, P.; Montorsi, F.; Kikuchi, E.; Zigeuner, R.; Weizer, A.; Bolenz, C.; Bensalah, K.; et al. Tumour architecture is an independent predictor of outcomes after nephroureterectomy: A multi-institutional analysis of 1363 patients. BJU Int. 2009, 103, 307–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fritsche, H.M.; Novara, G.; Burger, M.; Gupta, A.; Matsumoto, K.; Kassouf, W.; Sircar, K.; Zattoni, F.; Walton, T.; Tritschler, S.; et al. Macroscopic sessile tumor architecture is a pathologic feature of biologically aggressive upper tract urothelial carcinoma. Urol. Oncol. 2012, 30, 666–672. [Google Scholar] [CrossRef]
- Ishioka, J.; Saito, K.; Kijima, T.; Nakanishi, Y.; Yoshida, S.; Yokoyama, M.; Matsuoka, Y.; Numao, N.; Koga, F.; Masuda, H.; et al. Risk stratification for bladder recurrence of upper urinary tract urothelial carcinoma after radical nephroureterectomy. BJU Int. 2015, 115, 705–712. [Google Scholar] [CrossRef]
- Zigeuner, R.; Shariat, S.F.; Margulis, V.; Karakiewicz, P.I.; Roscigno, M.; Weizer, A.; Kikuchi, E.; Remzi, M.; Raman, J.D.; Bolenz, C.; et al. Tumour necrosis is an indicator of aggressive biology in patients with urothelial carcinoma of the upper urinary tract. Eur. Urol. 2010, 57, 575–581. [Google Scholar] [CrossRef]
- Simone, G.; Papalia, R.; Loreto, A.; Leonardo, C.; Sentinelli, S.; Gallucci, M. Independent prognostic value of tumour diameter and tumour necrosis in upper urinary tract urothelial carcinoma. BJU Int. 2009, 103, 1052–1057. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Zha, Z.; Qu, W.; Zhao, H.; Yuan, J.; Feng, Y.; Wu, B. Tumor necrosis as a prognostic variable for the clinical outcome in patients with renal cell carcinoma: A systematic review and meta-analysis. BMC Cancer 2018, 18, 870. [Google Scholar] [CrossRef]
- Wheat, J.C.; Weizer, A.Z.; Wolf, J.S., Jr.; Lotan, Y.; Remzi, M.; Margulis, V.; Wood, C.G.; Montorsi, F.; Roscigno, M.; Kikuchi, E.; et al. Concomitant carcinoma in situ is a feature of aggressive disease in patients with organ confined urothelial carcinoma following radical nephroureterectomy. Urol. Oncol. 2012, 30, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Roscigno, M.; Shariat, S.F.; Margulis, V.; Karakiewicz, P.; Remzi, M.; Kikuchi, E.; Zigeuner, R.; Weizer, A.; Sagalowsky, A.; Bensalah, K.; et al. The extent of lymphadenectomy seems to be associated with better survival in patients with nonmetastatic upper-tract urothelial carcinoma: How many lymph nodes should be removed? Eur. Urol. 2009, 56, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Zhang, L.; Zhang, H.; Jiang, H.; Ding, Q. Comparison of post-operative intravesical recurrence and oncological outcomes after open versus laparoscopic nephroureterectomy for upper urinary tract urothelial carcinoma. World J. Urol. 2014, 32, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.H.; Song, W.; Kang, M.; Jeon, H.G.; Jeong, B.C.; Seo, S.I.; Jeon, S.S.; Lee, H.M.; Sung, H.H. Conditional Intravesical Recurrence-Free Survival Rate After Radical Nephroureterectomy With Bladder Cuff Excision for Upper Tract Urothelial Carcinoma. Front. Oncol. 2021, 7, 730114. [Google Scholar] [CrossRef] [PubMed]
- Favaretto, R.L.; Shariat, S.F.; Chade, D.C.; Godoy, G.; Kaag, M.; Cronin, A.M.; Bochner, B.H.; Coleman, J.; Dalbagni, G. Comparison between laparoscopic and open radical nephroureterectomy in a contemporary group of patients: Are recurrence and disease-specific survival associated with surgical technique? Eur. Urol. 2010, 58, 645–651. [Google Scholar] [CrossRef] [Green Version]
- Piszczek, R.; Nowak, Ł.; Krajewski, W.; Chorbińska, J.; Poletajew, S.; Moschini, M.; Kaliszewski, K.; Zdrojowy, R. Oncological outcomes of laparoscopic versus open nephroureterectomy for the treatment of upper tract urothelial carcinoma: An updated meta-analysis. World J. Surg. Oncol. 2021, 19, 129. [Google Scholar] [CrossRef]
- Shigeta, K.; Matsumoto, K.; Takeda, T.; Hattori, S.; Kaneko, G.; Matsushima, M.; Abe, T.; Tanaka, N.; Mizuno, R.; Asanuma, H.; et al. Evaluating the Oncological Outcomes of Pure Laparoscopic Radical Nephroureterectomy Performed for Upper-Tract Urothelial Carcinoma Patients: A Multicenter Cohort Study Adjusted by Propensity Score Matching. Ann. Surg. Oncol. 2021, 28, 465–473. [Google Scholar] [CrossRef]
- Shigeta, K.; Kikuchi, E.; Hagiwara, M.; Ando, T.; Mizuno, R.; Miyajima, A.; Nakagawa, K.; Oya, M. Prolonged pneumoperitoneum time is an independent risk factor for intravesical recurrence after laparoscopic radical nephroureterectomy in upper tract urothelial carcinoma. Surg. Oncol. 2017, 26, 73–79. [Google Scholar] [CrossRef]
- Yanagi, M.; Hamasaki, T.; Akatsuka, J.; Endo, Y.; Takeda, H.; Kondo, Y. Risk factor analysis of intravesical recurrence after retroperitoneoscopic nephroureterectomy for upper tract urothelial carcinoma. BMC Urol. 2021, 21, 167. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, S.; Ito, A.; Mitsuzuka, K.; Ioritani, N.; Ishidoya, S.; Ikeda, Y.; Numahata, K.; Orikasa, K.; Tochigi, T.; Soma, F.; et al. Efficacy of early ureteral ligation on prevention of intravesical recurrence after radical nephroureterectomy for upper urinary tract urothelial carcinoma: A prospective single-arm multicenter clinical trial. Jpn. J. Clin. Oncol. 2017, 47, 870–875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.K.; Ye, Y.L.; Zhou, F.J.; Liu, J.Y.; Lu, K.S.; Han, H.; Liu, Z.W.; Xu, Z.Z.; Qin, Z.K. Clipping the extremity of ureter prior to nephroureterectomy is effective in preventing subsequent bladder recurrence after upper urinary tract urothelial carcinoma. Chin. Med. J. 2012, 125, 3821–3826. [Google Scholar] [PubMed]
- Sung, H.H.; Jeon, H.G.; Han, D.H.; Jeong, B.C.; Seo, S.I.; Lee, H.M.; Choi, H.Y.; Jeon, S.S. Diagnostic Ureterorenoscopy Is Associated with Increased Intravesical Recurrence following Radical Nephroureterectomy in Upper Tract Urothelial Carcinoma. PLoS ONE 2015, 10, e0139976. [Google Scholar] [CrossRef]
- Yoo, S.; You, D.; Song, C.; Hong, B.; Hong, J.H.; Kim, C.S.; Ahn, H.; Jeong, I.G. Risk of Intravesical Recurrence After Ureteroscopic Biopsy for Upper Tract Urothelial Carcinoma: Does the Location Matter? J. Endourol. 2017, 31, 259–265. [Google Scholar] [CrossRef]
- Loizzo, D.; Pandolfo, S.D.; Del Giudice, F.; Cerrato, C.; Chung, B.I.; Wu, Z.; Imbimbo, C.; Ditonno, P.; Derweesh, I.; Autorino, R. Ureteroscopy and tailored treatment of upper tract urothelial cancer: Recent advances and unmet needs. BJU Int. 2022, 1, 35–37. [Google Scholar] [CrossRef]
- Ha, J.S.; Jeon, J.; Ko, J.C.; Lee, H.S.; Yang, J.; Kim, D.; Kim, J.S.; Ham, W.S.; Choi, Y.D.; Cho, K.S. Intravesical Recurrence after Radical Nephroureterectomy in Patients with Upper Tract Urothelial Carcinoma Is Associated with Flexible Diagnostic Ureteroscopy, but Not with Rigid Diagnostic Ureteroscopy. Cancers 2022, 14, 5629. [Google Scholar] [CrossRef]
- Inoue, K.; Kamada, M.; Slaton, J.W.; Fukata, S.; Yoshikawa, C.; Tamboli, P.; Dinney, C.P.; Shuin, T. The prognostic value of angiogenesis and metastasis-related genes for progression of transitional cell carcinoma of the renal pelvis and ureter. Clin. Cancer Res. 2002, 8, 1863–1870. [Google Scholar]
- Zhang, G.; Shi, W.; Jia, E.; Zhang, L.; Han, Y.; Rodriguez, R.; Ma, T. FOXO3A Expression in Upper Tract Urothelial Carcinoma. Front. Oncol. 2021, 11, 603681. [Google Scholar] [CrossRef]
- Li, J.; Yang, R.; Dong, Y.; Chen, M.; Wang, Y.; Wang, G. Knockdown of FOXO3a induces epithelial-mesenchymal transition and promotes metastasis of pancreatic ductal adenocarcinoma by activation of the β-catenin/TCF4 pathway through SPRY2. J. Exp. Clin. Cancer Res. 2019, 38, 38. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, Y.; Sasaki, T.; Kawai, T.; Morikawa, T.; Matsusaka, K.; Kunita, A.; Kume, H.; Aoki, I.; Homma, Y.; Fukayama, M. HER2 protein overexpression and gene amplification in upper urinary tract urothelial carcinoma-an analysis of 171 patients. Int. J. Clin. Exp. Pathol. 2014, 7, 699–708. [Google Scholar] [PubMed]
- Soria, F.; Moschini, M.; Haitel, A.; Wirth, G.J.; Karam, J.A.; Wood, C.G.; Rouprêt, M.; Margulis, V.; Karakiewicz, P.I.; Briganti, A.; et al. HER2 overexpression is associated with worse outcomes in patients with upper tract urothelial carcinoma (UTUC). World J. Urol. 2017, 35, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Otto, W.; Shariat, S.F.; Fritsche, H.M.; Gupta, A.; Matsumoto, K.; Kassouf, W.; Martignoni, G.; Walton, T.J.; Tritschler, S.; Baba, S.; et al. Concomitant carcinoma in situ as an independent prognostic parameter for recurrence and survival in upper tract urothelial carcinoma: A multicenter analysis of 772 patients. World J. Urol. 2011, 29, 487–494. [Google Scholar] [CrossRef]
- Hanna, N.; Sun, M.; Trinh, Q.D.; Hansen, J.; Bianchi, M.; Montorsi, F.; Shariat, S.F.; Graefen, M.; Perrotte, P.; Karakiewicz, P.I. Propensity-score-matched comparison of perioperative outcomes between open and laparoscopic nephroureterectomy: A national series. Eur. Urol. 2012, 61, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Peyronnet, B.; Seisen, T.; Dominguez-Escrig, J.L.; Bruins, H.M.; Yuan, C.Y.; Lam, T.; Maclennan, S.; N’dow, J.; Babjuk, M.; Comperat, E.; et al. Oncological Outcomes of Laparoscopic Nephroureterectomy Versus Open Radical Nephroureterectomy for Upper Tract Urothelial Carcinoma: An European Association of Urology Guidelines Systematic Review. Eur. Urol. Focus. 2019, 5, 205–223. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.Y.; Li, W.M.; Huang, C.N.; Lee, H.L.; Niu, S.W.; Chen, L.T.; Wu, W.J.; Hwang, S.J. Dialysis Increases the Risk of Bladder Recurrence in Patients with Upper Tract Urothelial Cancer: A Population-Based Study. Ann. Surg. Oncol. 2018, 25, 1086–1093. [Google Scholar] [CrossRef] [PubMed]
- Leow, J.J.; Liu, Z.; Tan, T.W.; Lee, Y.M.; Yeo, E.K.; Chong, Y.L. Optimal Management of Upper Tract Urothelial Carcinoma: Current Perspectives. OncoTargets Ther. 2020, 13, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Van Doeveren, T.; Van Leeuwen, P.J.; Aben, K.K.H.; van der Aa, M.; Barendrecht, M.; Boevé, E.R.; Cornel, E.B.; van der Heijden, A.G.; Hendricksen, K.; Hirdes, W.; et al. Reduce bladder cancer recurrence in patients treated for upper urinary tract urothelial carcinoma: The REBACARE-trial. Contemp. Clin. Trials Commun. 2018, 9, 121–129. [Google Scholar] [CrossRef]
- Nadler, N.; Oedorf, K.; Jensen, J.B.; Azawi, N. Intraoperative Mitomycin C Bladder Instillation During Radical Nephroureterectomy Is Feasible and Safe. Eur. Urol. Open Sci. 2021, 34, 41–46. [Google Scholar] [CrossRef]
- Fang, D.; Li, X.S.; Xiong., G.Y.; Yao, L.; He, Z.S.; Zhou, L.Q. Prophylactic intravesical chemotherapy to prevent bladder tumors after nephroureterectomy for primary upper urinary tract urothelial carcinomas: A systematic review and meta-analysis. Urol. Int. 2013, 91, 291–296. [Google Scholar] [CrossRef]
- Hwang, E.C.; Sathianathen, N.J.; Jung, J.H.; Kim, M.H.; Dahm, P.; Risk, M.C. Single-dose intravesical chemotherapy after nephroureterectomy for upper tract urothelial carcinoma. Cochrane Database Syst. Rev. 2019, 5, CD013160. [Google Scholar] [CrossRef]
- Ito, A.; Shintaku, I.; Satoh, M.; Ioritani, N.; Aizawa, M.; Tochigi, T.; Kawamura, S.; Aoki, H.; Numata, I.; Takeda, A.; et al. Prospective randomized phase II trial of a single early intravesical instillation of pirarubicin (THP) in the prevention of bladder recurrence after nephroureterectomy for upper urinary tract urothelial carcinoma: The THP Monotherapy Study Group Trial. J. Clin. Oncol. 2013, 31, 1422–1427. [Google Scholar] [CrossRef] [PubMed]
- Noennig, B.; Bozorgmehri, S.; Terry, R.; Otto, B.; Su, L.M.; Crispen, P.L. Evaluation of intraoperative versus postoperative adjuvant mitomycin c with nephroureterectomy for urothelial carcinoma of the upper urinary tract. Bladder Cancer 2018, 4, 389–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, P.; Zhu, G.; Wei, D.; Liu, S.; Walsh, K.; Li, D.; Harron, U.; Wang, X.; Ma, H.; Wan, B.; et al. Prophylactic intravesical chemotherapy decreases bladder tumor recurrence after nephroureterectomy for primary upper tract urothelial carcinoma: A systematic review and meta-analysis. J BUON 2015, 20, 1229–1238. [Google Scholar] [PubMed]
- Huang, Y.; Cen, J.; Liu, Z.; Wei, J.; Chen, Z.; Feng, Z.; Lu, J.; Fang, Y.; Zhou, F.; Luo, J.; et al. A Comparison of Different Prophylactic Intravesical Chemotherapy Regimens for Bladder Cancer Recurrence After Nephroureterectomy for Primary Upper Tract Urothelial Carcinomas: A Retrospective 2-center Study. Technol. Cancer Res. Treat. 2019, 18, 1533033819844483. [Google Scholar] [CrossRef] [PubMed]
- Farrow, J.M.; Kern, S.Q.; Gryzinski, G.M.; Sundaram, C.P. Nephron-sparing management of upper tract urothelial carcinoma. Investig. Clin. Urol. 2021, 62, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Rastinehad, A.R.; Ost, M.C.; Vanderbrink, B.A.; Greenberg, K.L.; El-Hakim, A.; Marcovich, R.; Badlani, G.H.; Smith, A.D. A 20-year experience with percutaneous resection of upper tract transitional carcinoma: Is there an oncologic benefit with adjuvant bacillus Calmette Guérin therapy? Urology 2009, 73, 27–31. [Google Scholar] [CrossRef]
- Carmignani, L.; Bianchi, R.; Cozzi, G.; Grasso, A.; Macchione, N.; Marenghi, C.; Melegari, S.; Rosso, M.; Tondelli, E.; Maggioni, A.; et al. Intracavitary immunotherapy and chemotherapy for upper urinary tract cancer: Current evidence. Rev. Urol. 2013, 15, 145–153. [Google Scholar]
- Wu, Z.; Li, M.; Wang, L.; Paul, A.; Raman, J.D.; Necchi, A.; Psutka, S.P.; Buonerba, C.; Zargar, H.; Black, P.C.; et al. Neoadjuvant systemic therapy in patients undergoing nephroureterectomy for urothelial cancer: A multidisciplinary systematic review and critical analysis. Minerva Urol. Nephrol. 2022, 5, 518–527. [Google Scholar] [CrossRef]
- Zennami, K.; Sumitomo, M.; Takahara, K.; Nukaya, T.; Takenaka, M.; Fukaya, K.; Ichino, M.; Fukami, N.; Sasaki, H.; Kusaka, M.; et al. Two cycles of neoadjuvant chemotherapy improves survival in patients with high-risk upper tract urothelial carcinoma. BJU Int. 2021, 127, 332–339. [Google Scholar] [CrossRef]
- Shigeta, K.; Matsumoto, K.; Ogihara, K.; Murakami, T.; Anno, T.; Umeda, K.; Izawa, M.; Baba, Y.; Sanjo, T.; Shojo, K.; et al. Does neoadjuvant chemotherapy have therapeutic benefit for node-positive upper tract urothelial carcinoma? Results of a multi-center cohort study. Urol. Oncol. 2022, 40, 105.e19–105.e26. [Google Scholar] [CrossRef] [PubMed]
- Leow, J.J.; Chong, Y.L.; Chang, S.L.; Valderrama, B.P.; Powles, T.; Bellmunt, J. Neoadjuvant and Adjuvant Chemotherapy for Upper Tract Urothelial Carcinoma: A 2020 Systematic Review and Meta-analysis, and Future Perspectives on Systemic Therapy. Eur. Urol. 2021, 79, 635–654. [Google Scholar] [CrossRef] [PubMed]
- Leow, J.J.; Martin-Doyle, W.; Fay, A.P.; Choueiri, T.K.; Chang, S.L.; Bellmunt, J. A systematic review and meta-analysis of adjuvant and neoadjuvant chemotherapy for upper tract urothelial carcinoma. Eur. Urol. 2014, 66, 529–541. [Google Scholar] [CrossRef] [PubMed]
- Fradet, Y.; Bellmunt, J.; Vaughn, D.J.; Lee, J.L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; Necchi, A.; et al. Randomized phase III KEYNOTE-045 trial of pembrolizumab versus paclitaxel, docetaxel, or vinflunine in recurrent advanced urothelial cancer: Results of >2 years of follow-up. Ann. Oncol. 2019, 30, 970–976. [Google Scholar] [CrossRef]
- Guan, B.; Du, Y.; Su, X.; Cao, Z.; Li, Y.; Zhan, Y.; Peng, D.; Xiong, G.; Fang, D.; Ding, Y.; et al. Positive urinary fluorescence in situ hybridization indicates poor prognosis in patients with upper tract urothelial carcinoma. Oncotarget 2018, 9, 14652–14660. [Google Scholar] [CrossRef] [Green Version]
- Walsh, I.K.; Keane, P.F.; Ishak, L.M.; Flessland, K.A. The BTA stat test: A tumor marker for the detection of upper tract transitional cell carcinoma. Urology 2001, 58, 532–535. [Google Scholar] [CrossRef]
- Białek, Ł.; Bilski, K.; Dobruch, J.; Krajewski, W.; Szydełko, T.; Kryst, P.; Poletajew, S. Non-Invasive Biomarkers in the Diagnosis of Upper Urinary Tract Urothelial Carcinoma-A Systematic Review. Cancers 2022, 14, 1520. [Google Scholar] [CrossRef]
- Lonergan, P.E.; Porten, S.P. Bladder tumor recurrence after urothelial carcinoma of the upper urinary tract. Transl. Androl. Urol. 2020, 9, 1891–1896. [Google Scholar] [CrossRef]
- Mariappan, P.; Zachou, A.; Grigor, K.M. Detrusor muscle in the first, apparently complete transurethral resection of bladder tumour specimen is a surrogate marker of resection quality, predicts risk of early recurrence, and is dependent on operator experience. Eur. Urol. 2010, 57, 843–849. [Google Scholar] [CrossRef]
- Abe, T.; Shinohara, N.; Harabayashi, T.; Sazawa, A.; Akino, T.; Ishikawa, S.; Kubota, K.; Matsuno, Y.; Osawa, T.; Shibata, T.; et al. Pathological characteristics and clinical course of bladder tumour developing after nephroureterectomy. BJU Int. 2010, 105, 1102–1106. [Google Scholar] [CrossRef]
- Tanaka, N.; Kikuchi, E.; Kanao, K.; Matsumoto, K.; Shirotake, S.; Kobayashi, H.; Miyazaki, Y.; Ide, H.; Obata, J.; Hoshino, K.; et al. Independent predictors for bladder outcomes after treatment of intravesical recurrence following radical nephroureterectomy in patients with primary upper tract urothelial carcinoma. Ann. Surg. Oncol. 2014, 21, 3151–3158. [Google Scholar] [CrossRef] [PubMed]
- Naito, S.; Algaba, F.; Babjuk, M.; Bryan, R.T.; Sun, Y.H.; Valiquette, L.; de la Rosette, J. The Clinical Research Office of the Endourological Society (CROES) Multicentre Randomised Trial of Narrow Band Imaging-Assisted Transurethral Resection of Bladder Tumour (TURBT) Versus Conventional White Light Imaging-Assisted TURBT in Primary Non-Muscle-invasive Bladder Cancer Patients: Trial Protocol and 1-year Results. Eur. Urol. 2016, 70, 506–515. [Google Scholar] [PubMed]
- Symeonidis, E.N.; Lo, K.L.; Chui, K.L.; Vakalopoulos, I.; Sountoulides, P. En bloc resection of bladder tumors: Challenges and unmet needs in 2022. Future Oncol. 2022, 18, 2545–2558. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Zhou, Z.; Cui, Y.; Zhang, Y. Systematic review and meta-analysis of randomized controlled trials of perioperative outcomes and prognosis of transurethral en-bloc resection vs. conventional transurethral resection for non-muscle-invasive bladder cancer. Int. J. Surg. 2022; in press. [Google Scholar]
- Babjuk, M.; Burger, M.; Compérat, E.M.; Gontero, P.; Mostafid, A.H.; Palou, J.; van Rhijn, B.W.G.; Rouprêt, M.; Shariat, S.F.; Sylvester, R.; et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and Carcinoma In Situ)—2019 Update. Eur. Urol. 2019, 76, 639–657. [Google Scholar] [CrossRef]
- Flaig, T.W.; Spiess, P.; Abern, M.; Agarwal, N.; Bangs, R.; Boorjian, S.A.; Buyyounouski, M.K.; Chan, K.; Chang, S.; Friedlander, T.; et al. NCCN Guidelines® Insights: Bladder Cancer, Version 2.2022. J. Natl. Compr. Canc. Netw. 2022, 20, 866–878. [Google Scholar] [CrossRef]
- Sylvester, R.J.; Oosterlinck, W.; Holmang, S.; Sydes, M.R.; Birtle, A.; Gudjonsson, S.; De Nunzio, C.; Okamura, K.; Kaasinen, E.; Solsona, E.; et al. Systematic Review and Individual Patient Data Meta-analysis of Randomized Trials Comparing a Single Immediate Instillation of Chemotherapy After Transurethral Resection with Transurethral Resection Alone in Patients with Stage pTa-pT1 Urothelial Carcinoma of the Bladder: Which Patients Benefit from the Instillation? Eur. Urol. 2016, 69, 231–244. [Google Scholar]
- Messing, E.M.; Tangen, C.M.; Lerner, S.P.; Sahasrabudhe, D.M.; Koppie, T.M.; Wood, D.P., Jr.; Mack, P.C.; Svatek, R.S.; Evans, C.P.; Hafez, K.S.; et al. Effect of Intravesical Instillation of Gemcitabine vs Saline Immediately Following Resection of Suspected Low-Grade Non-Muscle-Invasive Bladder Cancer on Tumor Recurrence: SWOG S0337 Randomized Clinical Trial. JAMA 2018, 319, 1880–1888. [Google Scholar] [CrossRef]
- Rink, M.; Babjuk, M.; Catto, J.W.; Jichlinski, P.; Shariat, S.F.; Stenzl, A.; Stepp, H.; Zaak, D.; Witjes, J.A. Hexyl aminolevulinate-guided fluorescence cystoscopy in the diagnosis and follow-up of patients with non-muscle-invasive bladder cancer: A critical review of the current literature. Eur. Urol. 2013, 64, 624–638. [Google Scholar] [CrossRef]
- Shen, P.; Yang, J.; Wei, W.; Li, Y.; Li, D.; Zeng, H.; Wang, J. Effects of fluorescent light-guided transurethral resection on non-muscle-invasive bladder cancer: A systematic review and meta-analysis. BJU Int. 2012, 110, E209–E215. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Categories | Risk Factors | Reference |
|---|---|---|
| Patient specific factors | Damaged eGFR | Kuroda K et al. [20] Xylinas E et al. [21] Rasool M et al. [22] Chowdhury R et al. [23] |
| Venerable age | Xylinas E et al. [15] Chromecki TF et al. [24] Shariat SF et al. [25] | |
| Gender difference | Chien TM et al. [26] Chen CH et al. [27] Xylinas E et al. [15] Ploussard G et al. [28] Seisen T et al. [29] | |
| Smoking | Xylinas E et al. [15] Xylinas E et al. [30] Crivelli JJ et al. [31] Ehdaie B et al. [32] | |
| Diabetes mellitus with poor glycemic control | Tai YS et al. [33] Gao X et al. [34] Duan W et al. [35] | |
| Monocyte-to-lymphocyte ratio (MLR) | Liu J et al. [36] Zhang XK et al. [37] | |
| Neutrophil-to-lymphocyte ratio (NLR) | Mathieu R et al. [38] De Larco JE et al. [39] Vartolomei MD et al. [40] Vartolomei MD et al. [41] | |
| Tumor specific factors | Multifocality of upper urinary tract tumors | Milojevic B et al. [42] Chen CS et al. [43] Sheu ZL et al. [44] Chromecki TF et al. [45] |
| Size of upper urinary tract tumor | Kauffman EC et al. [46] Shibing Y et al. [47] Espiritu PN et al. [48] Su X et al. [49] | |
| Distal ureteral position | Tanaka N et al. [16] Xylinas E et al. [15] Seisen T et al. [29] Wu Y et al. [50] | |
| Lymph node involvement | Arancibia MF et al. [51] Xylinas E et al. [15] Roscigno M et al. [52] Novara G et al. [53] Verhoest G et al. [54] Peyrottes A et al. [55] | |
| Invasive pT staging | Seisen T et al. [29] Verhoest G et al. [54] Li YR et al. [56] | |
| papillary structure of tumors | Remzi M et al. [57] Fritsche HM et al. [58] Ishioka J et al. [59] | |
| Extensive tumor necrosis | Seisen T et al. [29] Zigeuner R et al. [60] Simone G et al. [61] Zhang L et al. [62] | |
| Concomitant carcinoma in situ (CIS) | Wheat JC et al. [63] Roscigno M et al. [64] Otto W et al. [5] | |
| Treatment specific factors | Incomplete excision | Kauffman EC et al. [46] Zou L et al. [65] Chung JH et al. [66] Seisen T et al. [29] |
| Immature laparoscopic technique | Favaretto RL et al. [67] Piszczek R et al. [68] Seisen T et al. [29] Shigeta K et al. [69] | |
| Surgery time | Yanagi M et al. [70] Shigeta K et al. [71] | |
| Early ureteral ligation | Yamashita S et al. [72] Chen MK et al. [73] | |
| Ureteroscopy | Sung HH et al. [74] Li YR et al. [56] Yoo S et al. [75] Loizzo D et al. [76] Ha JS et al. [77] | |
| Molecular specific factors | E-calmodulin | E- Inoue K et al. [78] |
| FOXO3A | Zhang G et al. [79] Li J et al. [80] | |
| HER2 | Sasaki Y et al. [81] Soria F et al. [82] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, X.; Xue, Y.; Zhu, G. Clinical Characteristics and Current Status of Treatment for Recurrent Bladder Cancer after Surgeries on Upper Tract Urothelial Carcinoma. Diagnostics 2023, 13, 1004. https://doi.org/10.3390/diagnostics13051004
Hu X, Xue Y, Zhu G. Clinical Characteristics and Current Status of Treatment for Recurrent Bladder Cancer after Surgeries on Upper Tract Urothelial Carcinoma. Diagnostics. 2023; 13(5):1004. https://doi.org/10.3390/diagnostics13051004
Chicago/Turabian StyleHu, Xinfeng, Yufan Xue, and Guodong Zhu. 2023. "Clinical Characteristics and Current Status of Treatment for Recurrent Bladder Cancer after Surgeries on Upper Tract Urothelial Carcinoma" Diagnostics 13, no. 5: 1004. https://doi.org/10.3390/diagnostics13051004