
Prognostic Impact of 24-Hour Pulse Pressure Components in Treated Hypertensive Patients Older Than 65 Years
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Clinic BP Measurement
2.3. Ambulatory BP Monitoring
2.4. Echocardiography
2.5. Follow-Up
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dart, A.M.; Kingwell, B.A. Pulse pressure—A review of mechanisms and clinical relevance. J. Am. Coll. Cardiol. 2001, 37, 975–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Safar, M.E.; Levy, B.I.; Struijker-Boudier, H. Current perspectives on arterial stiffness and pulse pressure in hypertension and cardiovascular diseases. Circulation 2003, 107, 2864–2869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franklin, S.S.; Gustin, W., 4th; Wong, N.D.; Larson, M.G.; Weber, M.A.; Kannel, W.B.; Levy, D. Hemodynamic patterns of age-related changes in blood pressure. The Framingham Heart Study. Circulation 1997, 96, 308–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franklin, S.S.; Khan, S.A.; Wong, N.D.; Larson, M.G.; Levy, D. Is pulse pressure useful in predicting risk for coronary heart Disease? The Framingham heart study. Circulation 1999, 100, 354–360. [Google Scholar] [CrossRef] [Green Version]
- Benetos, A.; Rudnichi, A.; Safar, M.; Guize, L. Pulse pressure and cardiovascular mortality in normotensive and hypertensive subjects. Hypertension 1998, 32, 560–564. [Google Scholar] [CrossRef] [Green Version]
- Blacher, J.; Staessen, J.A.; Girerd, X.; Gasowski, J.; Thijs, L.; Liu, L.; Wang, J.G.; Fagard, R.H.; Safar, M.E. Pulse pressure not mean pressure determines cardiovascular risk in older hypertensive patients. Arch. Intern. Med. 2000, 160, 1085–1089. [Google Scholar] [CrossRef]
- Domanski, M.; Norman, J.; Wolz, M.; Mitchell, G.; Pfeffer, M. Cardiovascular risk assessment using pulse pressure in the first national health and nutrition examination survey (NHANES I). Hypertension 2001, 38, 793–797. [Google Scholar] [CrossRef] [Green Version]
- Assmann, G.; Cullen, P.; Evers, T.; Petzinna, D.; Schulte, H. Importance of arterial pulse pressure as a predictor of coronary heart disease risk in PROCAM. Eur. Heart J. 2005, 26, 2120–2126. [Google Scholar] [CrossRef] [Green Version]
- Benetos, A.; Thomas, F.; Joly, L.; Blacher, J.; Pannier, B.; Labat, C.; Salvi, P.; Smulyan, H.; Safar, M.E. Pulse pressure amplification a mechanical biomarker of cardiovascular risk. J. Am. Coll. Cardiol. 2010, 55, 1032–1037. [Google Scholar] [CrossRef] [Green Version]
- Verdecchia, P.; Schillaci, G.; Borgioni, C.; Ciucci, A.; Pede, S.; Porcellati, C. Ambulatory pulse pressure: A potent predictor of total cardiovascular risk in hypertension. Hypertension 1998, 32, 983–988. [Google Scholar] [CrossRef] [Green Version]
- Khattar, R.S.; Swales, J.D.; Banfield, A.; Dore, C.; Senior, R.; Lahiri, A. Prediction of coronary and cerebrovascular morbidity and mortality by direct continuous ambulatory blood pressure monitoring in essential hypertension. Circulation 1999, 100, 1071–1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khattar, R.S.; Swales, J.D.; Dore, C.; Senior, R.; Lahiri, A. Effect of aging on the prognostic significance of ambulatory systolic, diastolic, and pulse pressure in essential hypertension. Circulation 2001, 104, 783–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verdecchia, P.; Schillaci, G.; Reboldi, G.; Franklin, S.S.; Porcellati, C. Different prognostic impact of 24-hour mean blood pressure and pulse pressure on stroke and coronary artery disease in essential hypertension. Circulation 2001, 103, 2579–2584. [Google Scholar] [CrossRef] [Green Version]
- Staessen, J.A.; Thijs, L.; O’Brien, E.T.; Bulpitt, C.J.; de Leeuw, P.W.; Fagard, R.H.; Nachev, C.; Palatini, P.; Parati, G.; Tuomilehto, J.; et al. Ambulatory pulse pressure as predictor of outcome in older patients with systolic hypertension. Am. J. Hypertens. 2002, 15, 835–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inoue, R.; Ohkubo, T.; Kikuya, M.; Metoki, H.; Asayama, K.; Obara, T.; Hoshi, H.; Hashimoto, J.; Totsune, K.; Satoh, H.; et al. Predicting stroke using 4 ambulatory blood pressure monitoring-derived blood pressure indices: The Ohasama Study. Hypertension 2006, 48, 877–882. [Google Scholar] [CrossRef] [Green Version]
- Ben-Dov, I.Z.; Kark, J.D.; Ben-Ishay, D.; Mekler, J.; Ben-Arie, L.; Bursztyn, M. Predictors of all-cause mortality in clinical ambulatory monitoring: Unique aspects of blood pressure during sleep. Hypertension 2007, 49, 1235–1241. [Google Scholar] [CrossRef]
- Kao, Y.T.; Huang, C.C.; Leu, H.B.; Wu, T.C.; Huang, P.H.; Lin, S.J.; Chen, J.W. Ambulatory pulse pressure as a novel predictor for long-term prognosis in essential hypertensive patient. J. Hum. Hypertens. 2011, 25, 444–450. [Google Scholar] [CrossRef] [Green Version]
- Gu, Y.M.; Thijs, L.; Li, Y.; Asayama, K.; Boggia, J.; Hansen, T.W.; Liu, Y.P.; Ohkubo, T.; Björklund-Bodegård, K.; Jeppesen, J.; et al. Outcome-driven thresholds for ambulatory pulse pressure in 9938 participants recruited from 11 populations. Hypertension 2014, 63, 229–237. [Google Scholar] [CrossRef] [Green Version]
- Schillaci, G.; Pucci, G.; Gavish, B. Ambulatory pulse pressure: Does it improve cardiovascular risk stratification? Hypertension 2014, 63, 217–219. [Google Scholar] [CrossRef] [Green Version]
- Tadic, M.; Quarti-Trevano, F.; Bombelli, M.; Facchetti, R.; Cuspidi, C.; Mancia, G.; Grassi, G. The importance of pulse pressure on cardiovascular risk and total mortality in the general population: Is sex relevant? J. Clin. Hypertens. 2018, 20, 1001–1007. [Google Scholar] [CrossRef] [Green Version]
- Melgarejo, J.D.; Thijs, L.; Wei, D.M.; Bursztyn, M.; Yang, W.Y.; Li, Y.; Asayama, K.; Hansen, T.W.; Kikuya, M.; Ohkubo, T.; et al. Relative and Absolute Risk to Guide the Management of Pulse Pressure, an Age-Related Cardiovascular Risk Factor. Am. J. Hypertens. 2021, 34, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Hozawa, A.; Ohkubo, T.; Nagai, K.; Kikuya, M.; Matsubara, M.; Tsuji, I.; Ito, S.; Satoh, H.; Hisamichi, S.; Imai, Y. Prognosis of isolated systolic and isolated diastolic hypertension as assessed by self-measurement of blood pressure at home: The Ohasama study. Arch. Intern. Med. 2000, 160, 3301–3306. [Google Scholar] [CrossRef] [Green Version]
- Gavish, B.; Izzo, J.L., Jr. Arterial stiffness: Going a step beyond. Am. J. Hypertens. 2016, 29, 1223–1233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gavish, B.; Bursztyn, M. Ambulatory pulse pressure components: Concepts, determination and clinical relevance. J. Hypertens. 2019, 37, 765–774. [Google Scholar] [CrossRef] [PubMed]
- Bursztyn, M.; Kikuya, M.; Asayama, K.; Satoh, M.; Gavish, B.; Ohkubo, T. Do estimated 24-h pulse pressure components affect outcome? The Ohasama study. J. Hypertens. 2020, 38, 1286–1292. [Google Scholar] [CrossRef]
- Gavish, B.; Bursztyn, M.; Thijs, L.; Wei, D.M.; Melgarejo, J.D.; Zhang, Z.Y.; Boggia, J.; Hansen, T.W.; Asayama, K.; Ohkubo, T.; et al. Predictive power of 24-h ambulatory pulse pressure and its components for mortality and cardiovascular outcomes in 11 848 participants recruited from 13 populations. J. Hypertens. 2022, 40, 2245–2255. [Google Scholar] [CrossRef]
- Pierdomenico, S.D.; Lapenna, D.; Guglielmi, M.D.; Antidormi, T.; Schiavone, C.; Cuccurullo, F.; Mezzetti, A. Target organ status and serum lipids in patients with white coat hypertension. Hypertension 1995, 26, 801–807. [Google Scholar] [CrossRef]
- O’Brien, E.; Parati, G.; Stergiou, G.; Asmar, R.; Beilin, L.; Bilo, G.; Clement, D.; de la Sierra, A.; de Leeuw, P.; Dolan, E.; et al. European Society of Hypertension position paper on ambulatory blood pressure monitoring. J. Hypertens. 2013, 31, 1731–1768. [Google Scholar] [CrossRef] [Green Version]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for chamber quantification: A report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar]
- de Simone, G.; Devereux, R.B.; Daniels, S.R.; Koren, M.J.; Meyer, R.A.; Laragh, J.H. Effect of growth on variability of left ventricular mass: Assessment of allometric signals in adults and children and their capacity to predict cardiovascular risk. J. Am. Coll. Cardiol. 1995, 25, 1056–1062. [Google Scholar] [CrossRef]
- Pierdomenico, S.D.; Pierdomenico, A.M.; Cuccurullo, F. Morning blood pressure surge, dipping, and risk of ischemic stroke in elderly patients treated for hypertension. Am. J. Hypertens. 2014, 27, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Pierdomenico, S.D.; Pierdomenico, A.M.; Di Tommaso, R.; Coccina, F.; Di Carlo, S.; Porreca, E.; Cuccurullo, F. Morning blood pressure surge, dipping, and risk of coronary events in elderly treated hypertensive patients. Am. J. Hypertens. 2016, 29, 39–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pierdomenico, S.D.; Pierdomenico, A.M.; Coccina, F.; Lapenna, D.; Porreca, E. Ambulatory blood pressure parameters and heart failure with reduced or preserved ejection fraction in elderly treated hypertensive patients. Am. J. Hypertens. 2016, 29, 1001–1007. [Google Scholar] [CrossRef] [PubMed]
- Pierdomenico, S.D.; Pierdomenico, A.M.; Coccina, F.; Lapenna, D.; Porreca, E. Circadian blood pressure changes and cardiovascular risk in elderlytreated hypertensive patients. Hypertens. Res. 2016, 39, 805–811. [Google Scholar] [CrossRef]
- Coccina, F.; Pierdomenico, A.M.; Pizzicannella, J.; Ianni, U.; Bufano, G.; Madonna, R.; Trubiani, O.; Cipollone, F.; Pierdomenico, S.D. Prognostic value of daytime and nighttime blood pressure in treated hypertensive patients according to age and sex. J. Clin. Hypertens. 2020, 22, 2014–2021. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| n. | 745 |
| Age, years | 71 (68–76) |
| Men, n (%) | 304 (41) |
| Body mass index, kg/m2 | 27.5 ± 4.0 |
| Smokers, n (%) | 73 (10) |
| Diabetes, n (%) | 114 (15) |
| Previous events, n (%) | 75 (10) |
| eGFR, mL/min | 62 ± 14 |
| LDL cholesterol, mg/dL | 127 ± 29 |
| LV hypertrophy, n (%) | 245 (33) |
| LA enlargement, n (%) | 168 (23) |
| ALVSD, n (%) | 36 (5) |
| n. | 745 |
| Clinic systolic BP, mmHg | 152 ± 18 |
| Clinic diastolic BP, mmHg | 86 ± 10 |
| Clinic PP, mmHg | 66.0 ± 15.5 |
| 24-hour systolic BP, mmHg | 133 ± 14 |
| 24-hour diastolic BP, mmHg | 74 ± 8 |
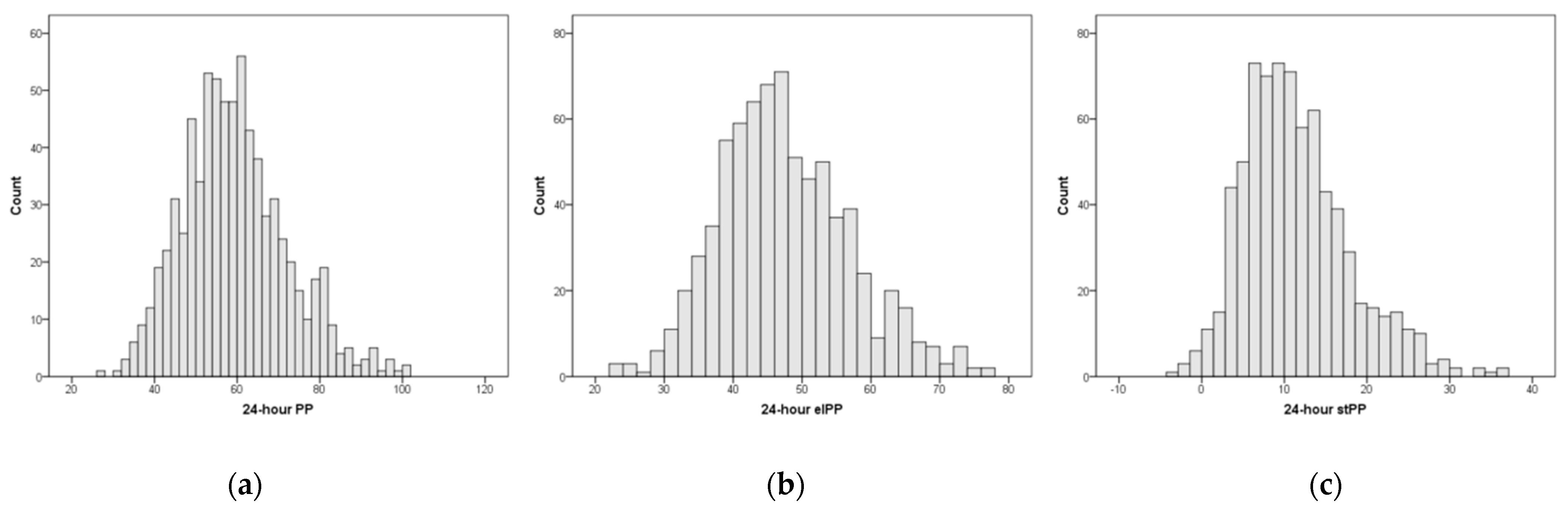
| 24-hour PP, mmHg | 59.0 ± 12.5 |
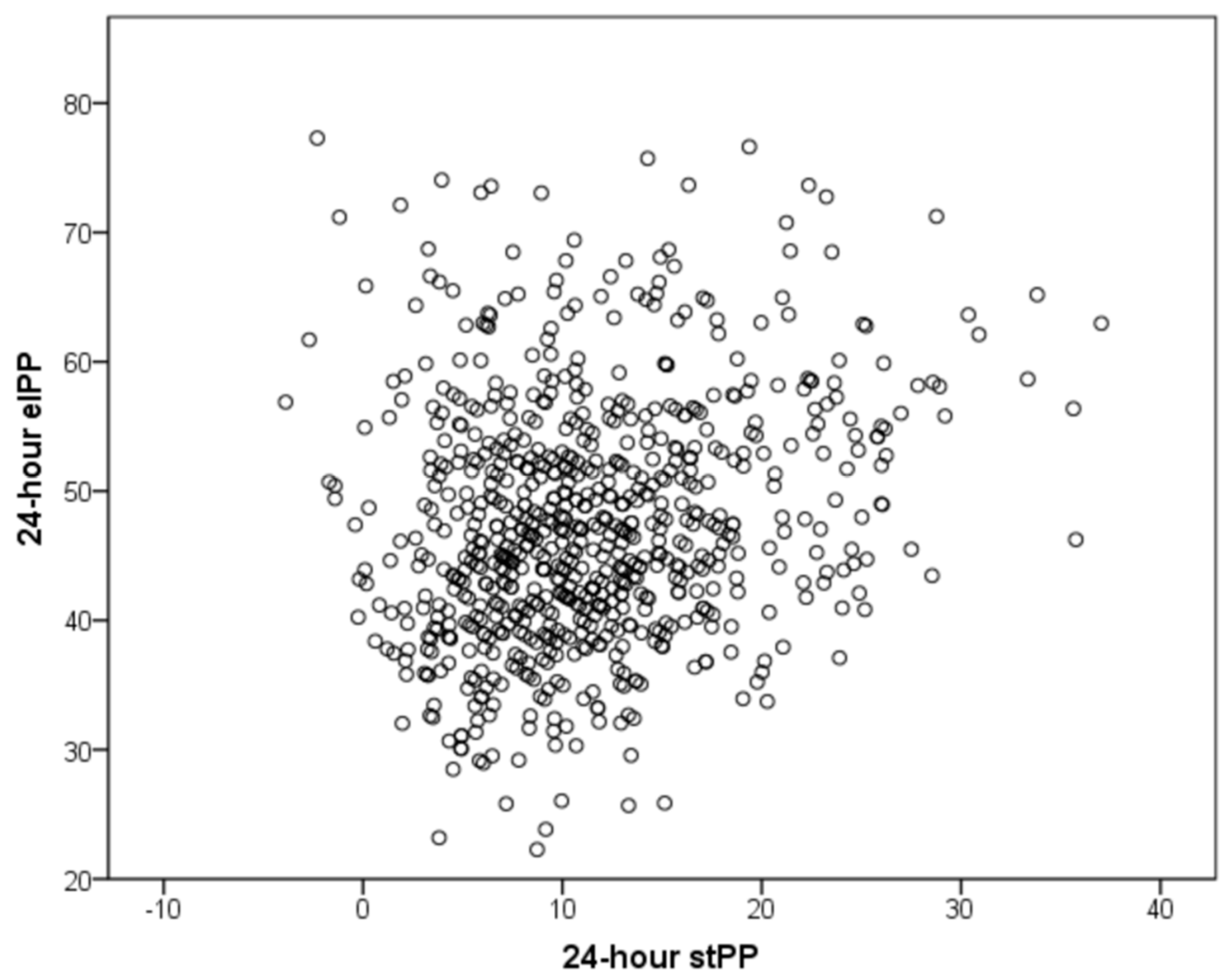
| 24-hour elastic PP, mmHg | 47.5 ± 9.5 |
| 24-hour stiffening PP, mmHg | 11.5 ± 6.5 |
| 24-hour MAP, mmHg | 93 ± 9 |
| 24-hour systolic SD, mmHg | 13.5 ± 3.0 |
| 24-hour diastolic SD, mmHg | 9 ± 2 |
| 24-hour HR, beats/min | 68 ± 9 |
| n. | 745 |
| Diuretic, n (%) | 431 (58) |
| Beta blocker, n (%) | 210 (28) |
| Calcium antagonist, n (%) | 260 (35) |
| ACE-inhibitor, n (%) | 396 (53) |
| ARB, n (%) | 188 (25) |
| Alpha blocker, n (%) | 104 (14) |
| Single therapy, n (%) | 180 (24) |
| Double therapy, n (%) | 344 (46) |
| Triple therapy, n (%) | 176 (24) |
| Quadruple or more therapy, n (%) | 45 (6) |
| Parameter | HR (95% CI) |
| Age (10 years) | 2.69 (2.17–3.44) |
| Diabetes (yes vs. no) | 1.82 (1.31–2.52) |
| Previous events (yes vs. no) | 1.51 (1.00–2.30) |
| eGFR (10 mL/min) | 0.86 (0.80–0.93) |
| LV hypertrophy (yes vs. no) | 1.95 (1.55–2.47) |
| LA enlargement (yes vs. no) | 1.46 (1.14–1.88) |
| ALVSD (yes vs. no) | 2.65 (1.73–4.04) |
| Clinic PP (1 SD) | 1.28 (1.13–1.45) |
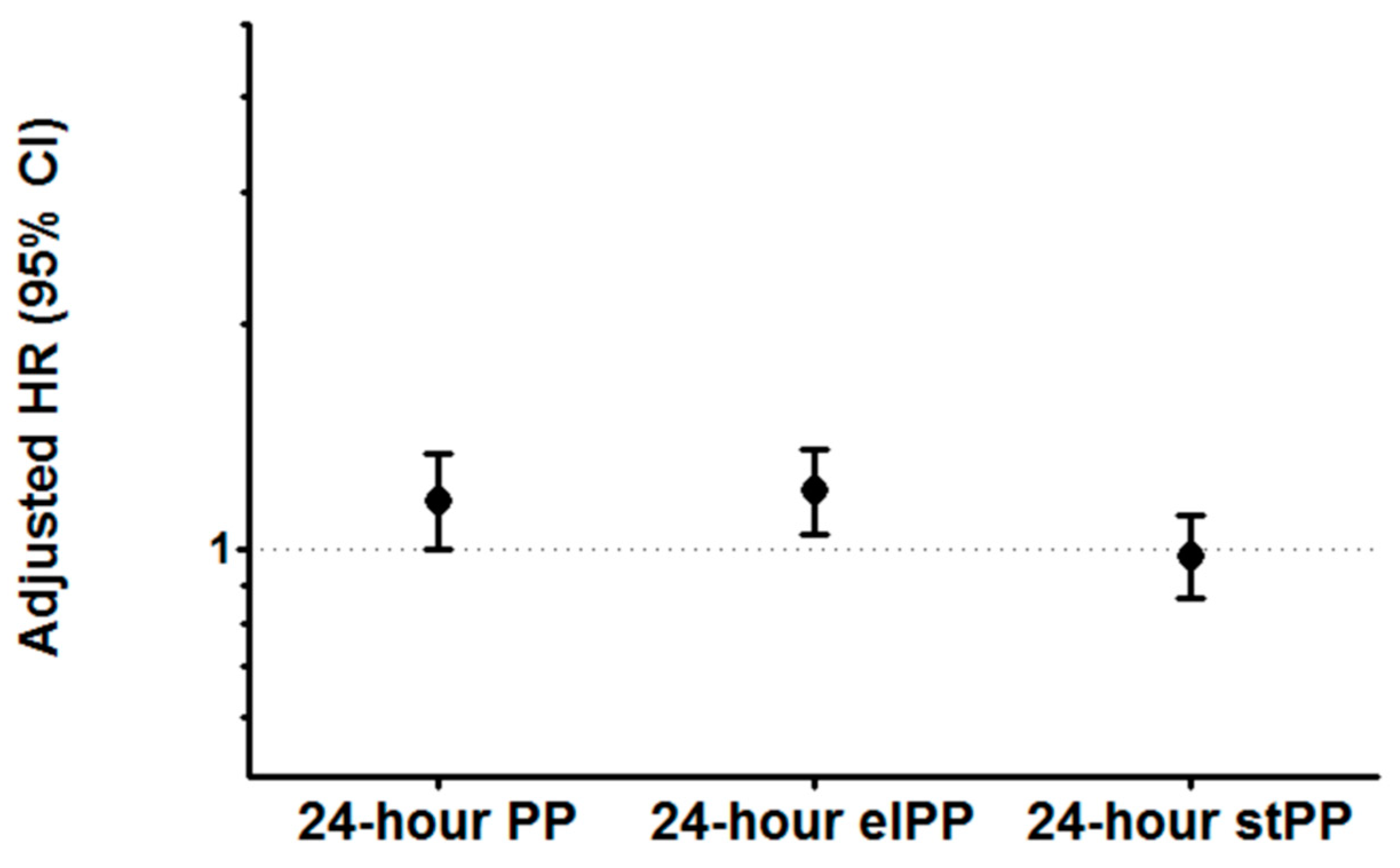
| 24-hour PP (1 SD) | 1.51 (1.37–1.67) |
| 24-hour elPP (1 SD) | 1.46 (1.33–1.60) |
| 24-hour stPP (1 SD) | 1.23 (1.10–1.38) |
| 24-hour MAP (1 SD) | 1.31 (1.18–1.46) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coccina, F.; Pierdomenico, A.M.; Cuccurullo, C.; Pizzicannella, J.; Trubiani, O.; Pierdomenico, S.D. Prognostic Impact of 24-Hour Pulse Pressure Components in Treated Hypertensive Patients Older Than 65 Years. Diagnostics 2023, 13, 845. https://doi.org/10.3390/diagnostics13050845
Coccina F, Pierdomenico AM, Cuccurullo C, Pizzicannella J, Trubiani O, Pierdomenico SD. Prognostic Impact of 24-Hour Pulse Pressure Components in Treated Hypertensive Patients Older Than 65 Years. Diagnostics. 2023; 13(5):845. https://doi.org/10.3390/diagnostics13050845
Chicago/Turabian StyleCoccina, Francesca, Anna M. Pierdomenico, Chiara Cuccurullo, Jacopo Pizzicannella, Oriana Trubiani, and Sante D. Pierdomenico. 2023. "Prognostic Impact of 24-Hour Pulse Pressure Components in Treated Hypertensive Patients Older Than 65 Years" Diagnostics 13, no. 5: 845. https://doi.org/10.3390/diagnostics13050845