
Reproducibility and Predictive Value of White-Coat Hypertension in Young to Middle-Age Subjects
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
2.1. Procedures
2.2. Definition of Operational Threshold Level
2.3. Follow-Up
2.4. Patients’ Classification
2.5. Statistics
3. Results
3.1. Follow-Up BP Changes
3.2. WCH as Predictor of Hypertension Needing Antihypertensive Treatment
4. Discussion
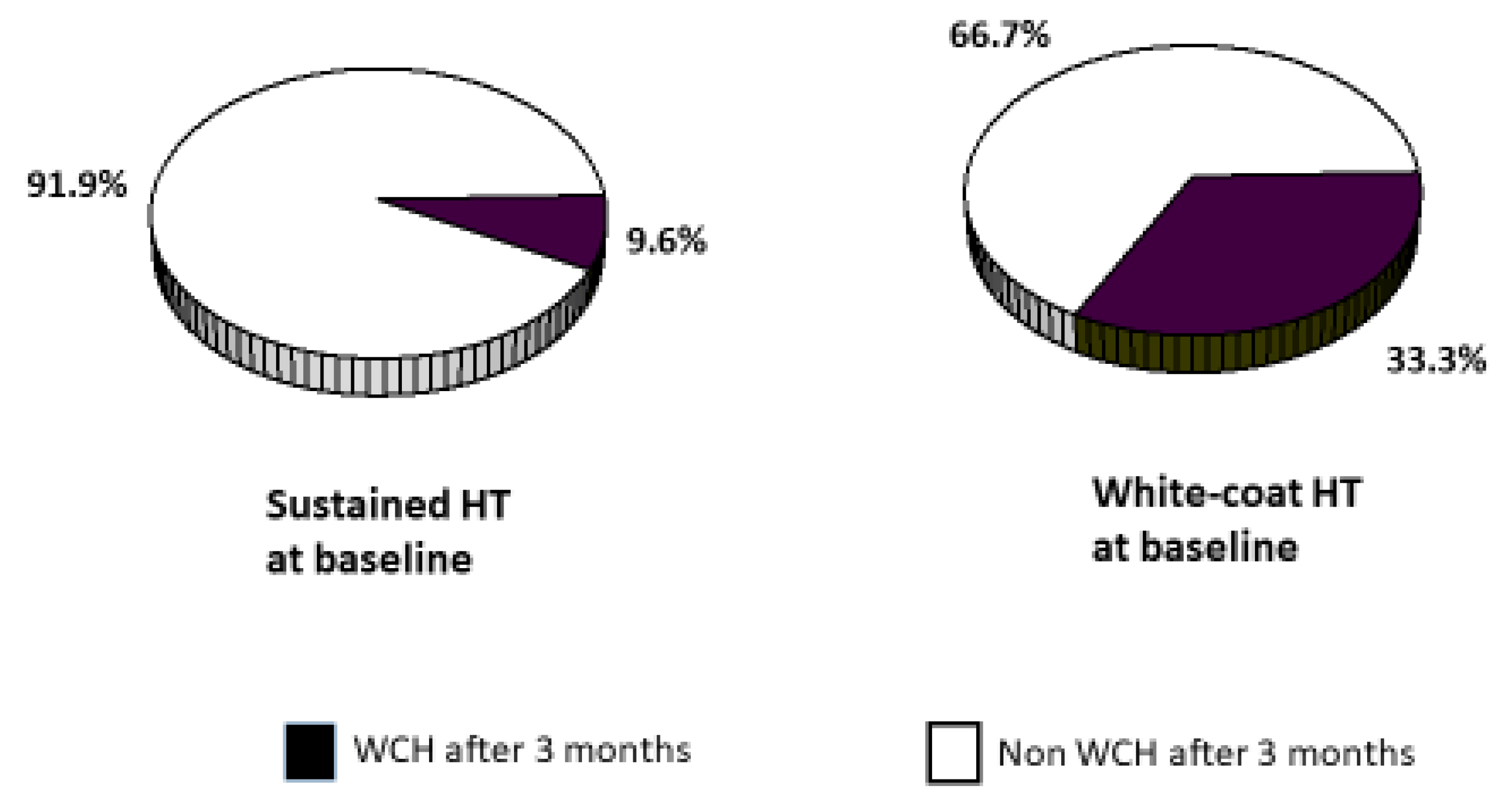
4.1. WCH Reproducibility
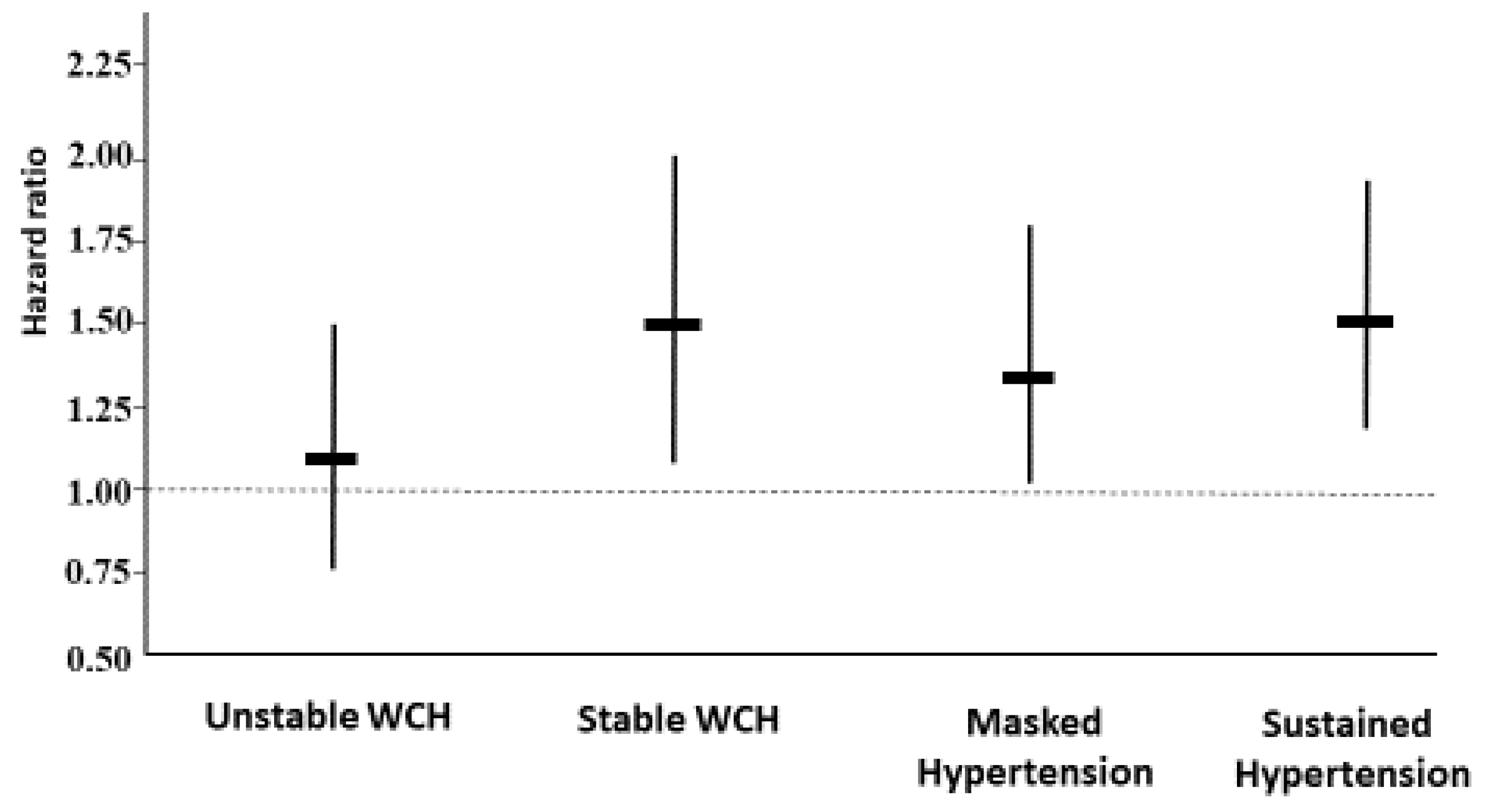
4.2. Predictive Value of WCH
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Disclosures
Ethical Approval
References
- Hanevold, C.D. White Coat Hypertension in Children and Adolescents. Hypertension 2019, 73, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Abolbashari, M. White Coat Hypertension and Cardiovascular Diseases: Innocent or Guilty. Curr. Cardiol. Rep. 2018, 20, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Pierdomenico, S.D.; Cuccurullo, F. Prognostic value of white-coat and masked hypertension diagnosed by ambulatory monitoring in initially untreated subjects: An updated meta analysis. Am. J. Hypertens. 2011, 24, 52–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancia, G.; Facchetti, R.; Bombelli, M.; Cuspidi, C.; Grassi, G. White-Coat Hypertension: Pathophysiological and Clinical Aspects: Excellence Award for Hypertension Research 2020. Hypertension 2021, 78, 1677–1688. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Huang, W.; Mai, W.; Cai, X.; An, D.; Liu, Z.; Huang, H.; Zeng, J.; Hu, Y.; Xu, D. White-coat hypertension is a risk factor for cardiovascular diseases and total mortality. J. Hypertens. 2017, 35, 677–688. [Google Scholar] [CrossRef] [Green Version]
- Puato, M.; Palatini, P.; Zanardo, M.; Dorigatti, F.; Tirrito, C.; Rattazzi, M.; Pauletto, P. Increase in carotid intima-media thickness in grade I hypertensive subjects: White-coat versus sustained hypertension. Hypertension 2008, 51, 1300–1305. [Google Scholar] [CrossRef] [Green Version]
- Franklin, S.S.; Thijs, L.; Asayama, K.; Li, Y.; Hansen, T.W.; Boggia, J.; Jacobs, L.; Zhang, Z.; Kikuya, M.; Björklund-Bodegård, K.; et al. The cardiovascular risk of white-coat hypertension. J. Am. Coll. Cardiol. 2016, 68, 2033–2043. [Google Scholar] [CrossRef]
- Asayama, K.; Thijs, L.; Li, Y.; Gu, Y.M.; Hara, A.; Liu, Y.P.; Zhang, Z.; Wei, F.F.; Lujambio, I.; Mena, L.J.; et al. Setting thresholds to varying blood pressure monitoring intervals differentially affects risk estimates associated with white-coat and masked hypertension in the population. Hypertension 2014, 64, 935–942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansson, M.A.K.; Östgren, C.J.; Engvall, J.; Swahn, E.; Wijkman, M.; Nystrom, F.H. Relationships between cardiovascular risk factors and white-coat hypertension diagnosed by home blood pressure recordings in a middle-aged population. J. Hypertens. 2021, 39, 2009–2014. [Google Scholar] [CrossRef]
- Rosenberg, K. White Coat Hypertension Increases Risk of Cardiovascular Events. Am. J. Nurs. 2019, 119, 55–62. [Google Scholar] [CrossRef]
- Mancia, G.; Facchetti, R.; Grassi, G.; Bombelli, M. Adverse prognostic value of persistent office blood pressure elevation in white coat hypertension. Hypertension 2015, 66, 437–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancia, G.; Facchetti, R.; Cuspidi, C.; Bombelli, M.; Corrao, G.; Grassi, G. Limited reproducibility of MUCH and WUCH: Evidence from the ELSA study. Eur. Heart J. 2020, 41, 1565–1571. [Google Scholar] [CrossRef] [PubMed]
- Muxfeldt, E.S.; Fiszman, R.; de Souza, F.; Viegas, B.; Oliveira, F.C.; Salles, G.F. Appropriate time interval to repeat ambulatory blood pressure monitoring in patients with white-coat resistant hypertension. Hypertension 2012, 59, 384–389. [Google Scholar] [CrossRef] [Green Version]
- Ben-Dov, I.Z.; Ben-Arie, L.; Mekler, J.; Bursztyn, M. Reproducibility of white-coat and masked hypertension in ambulatory BP monitoring. Int. J. Cardiol. 2007, 117, 355–359. [Google Scholar] [CrossRef]
- De la Sierra, A.; Vinyoles, E.; Banegas, J.R.; Segura, J.; Gorostidi, M.; Juan, J.; Ruilope, L.M. Short-term and long-term reproducibility of hypertension phenotypes obtained by office and ambulatory blood pressure measurements. J. Clin. Hypertens. 2016, 18, 927–933. [Google Scholar] [CrossRef] [Green Version]
- Palatini, P.; Graniero, G.R.; Mormino, P.; Nicolosi, L.; Mos, L.; Visentin, P.; Pessina, A.C. Relation between physical training and ambulatory blood pressure in stage I hypertensive subjects. Results of the HARVEST Trial. Hypertension and Ambulatory Recording Venetia Study. Circulation 1994, 90, 2870–2876. [Google Scholar] [CrossRef] [Green Version]
- Palatini, P.; Mormino, P.; Canali, C.; Santonastaso, M.; De Venuto, G.; Zanata, G.; Pessina, A.C. Factors affecting ambulatory blood pressure reproducibility. Results of the HARVEST trial. Hypertension 1994, 23, 211–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palatini, P.; Canali, C.; Graniero, G.R.; Rossi, G.; de Toni, R.; Santonastaso, M.; dal Follo, M.; Zanata, G.; Ferrarese, E.; Mormino, P.; et al. Relationship of plasma renin activity with caffeine intake and physical training in mild hypertensive men. HARVEST Study Group. Eur. J. Epidemiol. 1996, 12, 485–491. [Google Scholar] [CrossRef]
- Winnicki, M.; Somers, V.K.; Dorigatti, F.; Longo, D.; Santonastaso, M.; Mos, L.; Mattarei, M.; Pessina, A.C.; Palatini, P.; HARVEST Study Group. Lifestyle, family history and progression of hypertension. J. Hypertens. 2006, 24, 1479–1487. [Google Scholar] [CrossRef]
- Palatini, P.; Penzo, M.; Canali, C.; Pessina, A.C. Validation of the accuracy of the A & D TM-2420 model 7 for ambulatory blood pressure monitoring and effect of microphone replacement on its performance. J. Amb. Monit. 1991, 4, 281–288. [Google Scholar]
- O’Brien, E.; Mee, F.; Atkins, N.; O’Malley, K. Accuracy of the SpaceLabs 90207 determined by the British Hypertension Society protocol. J. Hypertens. 1991, 9, 573–575. [Google Scholar] [CrossRef] [PubMed]
- British Hypertension Society Working Part. Treating mild hypertension. Report of the British Hypertension Society working party. BMJ 1989, 298, 694–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chalmers, J.; MacMahon, S.; Mancia, G.; Whitworth, J.; Beilin, L.; Hansson, L.; Neal, B.; Rodgers, A.; Ni Mhurchu, C.; Clark, T. 1999 World Health Organization-International Society of Hypertension. Guidelines for the Management of Hypertension. Guidelines Sub-Committee. J. Hypertens. 1999, 21, 1009–1060. [Google Scholar]
- Guidelines Committee. 2003 European Society of Hypertension-European Society of Cardiology guidelines for the management of arterial hypertension. J. Hypertens. 2003, 21, 1011–1053. [Google Scholar]
- Cohen, J. Weighted kappa: Nominal scale agreement with provision for scaled disagreement or partial credit. Psychol. Bull. 1968, 70, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Fleiss, J.L.; Levin, B.; Paik, M.C.; Myunghee, C.P. Statistical Methods for Rates and Proportions, 3rd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2003. [Google Scholar]
- Altman, D.G. Practical Statistics for Medical Research; Chapman and Hall: London, UK, 1991. [Google Scholar]
- Mancia, G.; Bombelli, M.; Facchetti, R.; Madotto, F.; Quarti-Trevano, F.; Friz, H.P.; Grassi, G.; Sega, R. Long term risk of sustained hypertension in white-coat or masked hypertension. Hypertension 2009, 54, 226–232. [Google Scholar] [CrossRef] [Green Version]
- Ugajin, T.; Hozawa, A.; Ohkubo, T.; Asayama, K.; Kikuya, M.; Obara, T.; Metoki, H.; Hoshi, H.; Hashimoto, J.; Totsune, K.; et al. White-coat hypertension as a risk factor for the development of home hypertension: The Ohasama study. Arch. Intern. Med. 2005, 165, 1541–1546. [Google Scholar] [CrossRef] [Green Version]
- Miyashita, Y.; Hanevold, C.; Faino, A.; Scher, J.; Lande, M.; Yamaguchi, I.; Hernandez, J.; Acosta, A.; Weaver, D.J., Jr.; Thomas, J.; et al. White Coat Hypertension Persistence in Children and Adolescents: The Pediatric Nephrology Research Consortium Study. J. Pediatr. 2022, 246, 154–160. [Google Scholar] [CrossRef]
- Palatini, P.; Fania, C.; Mos, L.; Garavelli, G.; Mazzer, A.; Cozzio, S.; Saladini, F.; Casiglia, E. Coffee consumption and risk of cardiovascular events in hypertensive patients. Results from the HARVEST. Int. J. Cardiol. 2016, 212, 131–137. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Normotensive (n = 132) | Masked HT (n = 195) | Sustained HT (n = 610) | Stable WCH (n = 76) | Unstable WCH (n = 83) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | p-value |
| Age, years | 32.1 | 8.3 | 32.9 | 8.3 | 33.5 | 8.8 | 31.7 | 7.7 | 32.3 | 8.2 | 0.21 |
| BMI, kg/m2 | 24.4 | 2.9 | 24.8 | 3.2 | 25.8 | 3.4 | 25.4 | 4.6 | 25.3 | 3.4 | 0.002 |
| Office SBP, mmHg | 128.0 | 7.6 | 129.6 | 7.6 | 145.8 | 9.9 | 143.9 | 11.8 | 144.2 | 9.8 | <0.001 |
| Office DBP, mmHg | 81.5 | 6.7 | 83.6 | 6.0 | 94.0 | 7.0 | 93.8 | 7.9 | 92.3 | 6.7 | <0.001 |
| 24 h-SBP, mmHg | 118.9 | 7.2 | 132.9 | 8.6 | 135.0 | 9.7 | 118.7 | 6.6 | 122.1 | 5.8 | <0.001 |
| 24 h-DBP, mmHg | 73.3 | 5.5 | 81.7 | 7.7 | 84.0 | 7.6 | 74.2 | 5.4 | 74.3 | 6.0 | <0.001 |
| 24 h-HR, bpm | 70.9 | 7.4 | 72.5 | 7.1 | 72.6 | 7.7 | 72.8 | 8.1 | 71.0 | 9.2 | 0.009 |
| FU length, years * | 18.2 | 12.0–23.3 | 16.0 | 7.8–23.6 | 17.4 | 9.1–22.3 | 15.7 | 8.1–20.4 | 19.0 | 11.9–25.1 | 0.047 |
| Sex, men | 62.9% | -- | 71.8% | -- | 75.9% | -- | 63.2% | -- | 75.9% | -- | 0.009 |
| Smoking, yes | 16.7% | -- | 21.0% | -- | 22.8% | -- | 20.6% | -- | 15.7% | -- | 0.20 |
| Alcohol use, yes | 37.9% | -- | 46.7% | -- | 50.2% | -- | 39.5% | -- | 48.2% | -- | 0.07 |
| Coffee use, yes | 70.5% | -- | 66.7% | -- | 76.2% | -- | 71.1% | -- | 75.9% | -- | 0.09 |
| Physical activity, yes | 40.9% | -- | 41.0% | -- | 36.1% | -- | 38.2% | -- | 47.0% | -- | 0.30 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palatini, P.; Mos, L.; Saladini, F.; Vriz, O.; Fania, C.; Ermolao, A.; Battista, F.; Rattazzi, M. Reproducibility and Predictive Value of White-Coat Hypertension in Young to Middle-Age Subjects. Diagnostics 2023, 13, 434. https://doi.org/10.3390/diagnostics13030434
Palatini P, Mos L, Saladini F, Vriz O, Fania C, Ermolao A, Battista F, Rattazzi M. Reproducibility and Predictive Value of White-Coat Hypertension in Young to Middle-Age Subjects. Diagnostics. 2023; 13(3):434. https://doi.org/10.3390/diagnostics13030434
Chicago/Turabian StylePalatini, Paolo, Lucio Mos, Francesca Saladini, Olga Vriz, Claudio Fania, Andrea Ermolao, Francesca Battista, and Marcello Rattazzi. 2023. "Reproducibility and Predictive Value of White-Coat Hypertension in Young to Middle-Age Subjects" Diagnostics 13, no. 3: 434. https://doi.org/10.3390/diagnostics13030434