
The Prevalence and Risk Factors of Chronic Heart Failure in the Mongolian Population
 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
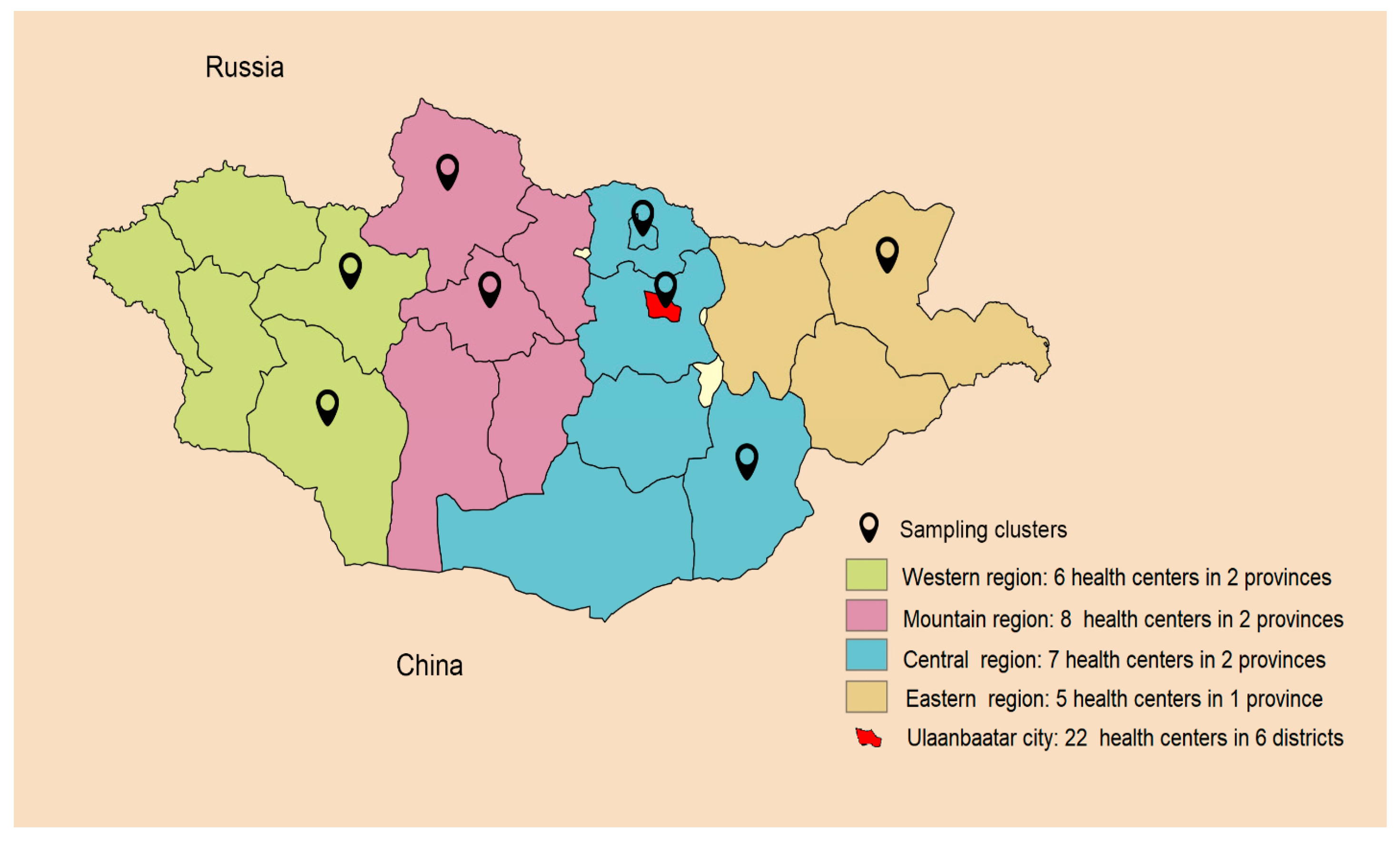
2.1. Data Source and Sampling
2.1.1. Study Sample Size
2.1.2. Sample Selection
2.2. Data Collection
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
- This is the first investigation in Mongolia that describes the prevalence of HF among the general population. The prevalence of HF appears high (4.94%) in the Mongolian population compared with other studies.
- Our study revealed that coronary heart disease, hypertension, and valvular heart disease are the three foremost risk factors in the development chronic heart failure.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Savarese, G.; Lund, L.H. Global Public Health Burden of Heart Failure. Card. Fail. Rev. 2017, 3, 7–11. [Google Scholar] [CrossRef]
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789. [Google Scholar] [CrossRef] [Green Version]
- Cho, D.H.; Yoo, B.S. Current Prevalence, Incidence, and Outcomes of Heart Failure with Preserved Ejection Fraction. Heart Fail. Clin. 2021, 17, 315–326. [Google Scholar] [CrossRef] [PubMed]
- Ziaeian, B.; Fonarow, G.C. Epidemiology and aetiology of heart failure. Nat. Rev. Cardiol. 2016, 13, 68–378. [Google Scholar] [CrossRef] [Green Version]
- Savarese, G.; Becher, P.M.; Lund, L.H.; Seferovic, P.; Giuseppe Rosano, M.C.; Andrew Coats, J.S. Global burden of heart failure: A comprehensive and updated review of epidemiology. Cardiovasc. Cardiovasc. Res. 2022, 118, 3272–3287. [Google Scholar] [CrossRef] [PubMed]
- Ceia, F.; Fonseca, C.; Mota, T.; Morais, H.; Matias, F.; Sousa, A.; António Oliveira, A. Prevalence of chronic heart failure in Southwestern Europe: The EPICA study. Eur. J. Heart Fail. 2002, 4, 531–539. [Google Scholar] [CrossRef] [PubMed]
- Mosterd, A.; Hoes, A.W.; de Bruyne, M.C.; Deckers, J.M.; Linker, D.T.; Hofman, A.; Grobbee, D.E. Prevalence of heart failure and left ventricular dysfunction in the general population; The Rotterdam Study 1999. Eur. Heart J. 2000, 20, 447–455. [Google Scholar] [CrossRef]
- Redfield, M.M.; Jacobsen, S.J.; Burnett, J.C., Jr.; Mahoney, D.W.; Bailey, K.R.; Rodeheffer, R.J. Burden of systolic and diastolic ventricular dysfunction in the community: Appreciating the scope of the heart failure epidemic. J. Amer. Med. Assoc. 2003, 289, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, M.N.; Køber, L.; Weeke, P.; Vasan, R.S.; Jeppesen, J.L.; Smith, J.G.; Gislason, G.H.; Torp-Pedersen, C.; Andersson, C. Age-Specific Trends in Incidence, Mortality, and Comorbidities of Heart Failure in Denmark, 1995 to 2012. Circulation 2017, 135, 1214–1223. [Google Scholar] [CrossRef] [PubMed]
- Barasa, A.; Schaufelberger, M.; Lappas, G.; Swedberg, K.; Dellborg, M.; Rosengren, A. Heart failure in young adults: 20-year trends in hospitalization, aetiology, and case fatality in Sweden. Eur. Heart J. 2014, 35, 25–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jencks, S.F.; Williams, M.V.; Coleman, E.A. Rehospitalizations among patients in the Medicare fee-for-service program. N. Engl. J. Med. 2009, 360, 418–428. [Google Scholar] [CrossRef]
- Komanduria, S.; Jadhaoa, Y.; Gudurua, S.S.; Cheriyatha, P.; Wertb, Y. Prevalence and risk factors of heart failure in the USA: NHANES 2013–2014. Epidemiological follow-up study. J. Community Hosp. Intern. Med. Perspect. 2017, 7, 15–20. [Google Scholar] [CrossRef] [Green Version]
- Pfeffer, M.A.; Shah, A.M.; Borlaug, B.A. Heart failure with preserved ejection fraction in perspective. Circ. Res. 2019, 24, 1598–1617. [Google Scholar] [CrossRef] [PubMed]
- Pillai, H.S.; Ganapathi, S. Heart failure in South Asia. Curr. Cardiol. Rev. 2013, 9, 102–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamo, C.E.; Kwak, L.; Wang, D.; Florido, R.; Echouffo-Tcheugui, J.B.; Blumenthal, R.S.; Loehr, L.; Matsushita, K.; Nambi, V.; Ballantyne, C.M.; et al. Heart failure risk associated with severity of modifiable heart failure risk factors: The ARIC Study. J. Am. Heart Assoc. 2022, 11, e021583. [Google Scholar] [CrossRef]
- Center for Health Development. Health Indicators; Center for Health Development: Ulaanbaatar, Mongolia, 2021. [Google Scholar]
- Schocken, D.D.; Benjamin, E.J.; Fonarow, G.C.; Krumholz, H.M.; Levy, D.; Mensah, G.A.; Narula, J.; Shor, E.S.; Young, J.B.; Hong, Y. Prevention of heart failure: A scientific statement from the American Heart Association Councils on Epidemiology and Prevention, Clinical Cardiology, Cardiovascular Nursing, and High Blood Pressure Research; Quality of Care and Outcomes Research Interdisciplinary Working Group; and Functional Genomics and Translational Biology Interdisciplinary Working GroupPrevention of Heart Failure. Circulation 2008, 117, 2544–2565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swedberg, K.; Cleland, J.; Dargie, H.; Drexler, H.; Follath, F.; Komajda, M.; Tavazzi, L.; Smiseth, O.A.; Gavazzi, A.; Haverich, A.; et al. Guidelines for the diagnosis and treatment of chronic heart failure: Executive summary (update 2005): The task force for the diagnosis and treatment of chronic heart failure of the European Society of Cardiology. Eur. Heart J. 2005, 26, 1115–1140. [Google Scholar] [CrossRef] [Green Version]
- Sakata, Y.; Shimokawa, H. Epidemiology of heart failure in Asia. Circ. J. 2013, 7, 2209–2217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, S.S.; Kong, L.Z.; Gao, R.L.; Zhu, M.L.; Wang, W.; Wang, Y.J.; Wu, Z.S.; Chen, W.W.; Liu, M.B. Outline of the report oncardiovascular disease in China, 2010. Biomed. Env. Sci. 2012, 25, 251–256. [Google Scholar] [CrossRef]
- Ponikowski, P.; Anker, S.D.; AlHabib, K.F.; Cowie, M.R.; Force, T.L.; Hu, S.; Jaarsma, T.; Krum, H.; Rastogi, V.; Rohde, L.E.; et al. Heart failure: Preventing disease and death worldwide. ESC Heart Fail. 2014, 1, 4–25. [Google Scholar] [CrossRef]
- Lam, C.S. Heart failure in Southeast Asia: Facts and numbers. ESC Heart Fail. 2015, 2, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, V.; Parakh, N.; Seth, S.; Bhargava, B.; Ramakrishnan, S.; Roy, A.; Saxena, A.; Gupta, N.; Misra, P.; Rai, S.K.; et al. Heart Failure in India: The INDUS (INDia Ukieri Study) Study. J. Pract. Cardiovasc. Sci. 2016, 2, 28–35. [Google Scholar] [CrossRef]
- Potter, E.L.; Hopper, I.; Sen, J.; Salim, A.; Marwick, T.H. Impact of socioeconomic status on incident heart failure and left ventricular dysfunction: Systematic review and meta-analysis. Eur. Heart J. Qual. Care Clin. Outcomes. 2019, 5, 169–179. [Google Scholar] [CrossRef]
- Wang, H.; Chai, K.; Du, M.; Wang, S. Prevalence and Incidence of Heart Failure Among Urban Patients China. Circ. Heart Fail. 2021, 14, e008406. [Google Scholar] [CrossRef]
- Tiller, D.; Russ, M.; Greiser, K.H.; Nuding, S.; Ebelt, H.; Kluttig, A.; Kors, J.A.; Thiery, J.; Bruegel, M.; Haerting, J.; et al. Prevalence of Symptomatic Heart Failure with Reduced and with Normal Ejection Fraction in an Elderly General Population–The CARLA Study. PLoS ONE. 2013, 8, e5922. [Google Scholar] [CrossRef] [Green Version]
- Cleland, J.G.; Erdmann, E.; Ferrari, R.; Hess, O.M.; Poole-Wilson, P.A.; Remme, W.J. Guidelines for the diagnosis of heart failure. Eur. Heart J. 1995, 16, 741–751. [Google Scholar]
- McKee, P.A.; Castelli, W.P.; McNamara, P.M.; Kannel, W.B. The natural history of congestive heart failure: The Framingham study. N. Engl. J. Med. 1971, 26, 441–446. [Google Scholar] [CrossRef]
- Phillips, S.J.; Wishnant, J.P.; O’Fallon, W.M.; Frye, R.L. Prevalence of cardiovascular disease and diabettes mellitus in residents of Rochester, Minnesota. Mayo. Clin. Prod. 1990, 65, 344–359. [Google Scholar] [CrossRef]
- Banerjee, A.; Pasea, L.; Chung, S.; Direk, K.; Asselbergs, F.W.; Grobbee, D.E.; Kotecha, D.; Anker, S.A.; Dyszynski, T.; Tyl, B.; et al. A population-based study of 92 clinically recognized risk factors for heart failure: Co-occurrence, prognosis and preventive potential. Eur. J. Heart Fail. 2022, 24, 466–480. [Google Scholar] [CrossRef]
- Gottdiener, J.S.; Arnold, A.M.; Aurigemma, G.P.; Polak, J.F.; Tracy, R.P.; Kitzman, D.W.; Gardin, J.M.; Rutledge, J.E.; Boineau, R.C. Predictors of congestive heart failure in the elderly: The Cardiovascular Health Study. J. Am. Coll. Cardiol. 2000, 35, 1628–1637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawson, C.A.; Zaccardi, F.; Squire, I.; Okhai, H.; Davies, M.; Huang, W.; Mamas, M.; Lam, C.S.P.; Khunti, K.; Umesh, T.; et al. Risk Factors for Heart Failure. Circ. Heart Fail. 2020, 13, e006472. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Study Population (n = 3480) | Male (n = 1345) | Female (n = 2135) | p-Value |
|---|---|---|---|---|
| Age group | 0.484 | |||
| 20–29, n (%) | 807 (23.2) | 286 (21.3) | 521 (24.4) | |
| 30–39, n (%) | 863 (24.8) | 335 (24.9) | 528 (24.7) | |
| 40–49, n (%) | 682 (19.6) | 268 (19.9) | 414 (19.4) | |
| 50–59, n (%) | 595 (17.1) | 236 (17.6) | 359 (16.8) | |
| 60–69, n (%) | 381 (10.9) | 158 (11.8) | 223 (10.5) | |
| ≥70, n (%) | 152 (4.4) | 62 (4.6) | 90 (4.2) | |
| Education | <0.001 | |||
| Higher, n (%) | 1229 (35.3) | 418 (31.1) | 811 (38.0) | |
| Medium, n (%) | 1784 (51.3) | 696 (51.7) | 1088 (51.0) | |
| Lower, n (%) | 467(13.4) | 231 (17.2) | 236 (11.0) | |
| Occupation | <0.001 | |||
| Manual labor, n (%) | 830 (23.9) | 398 (29.6) | 432 (20.2) | |
| Intellectual labor, n (%) | 1238 (35.7) | 457 (34.0) | 781 (36.6) | |
| Unemployed, n (%) | 1412 (40.4) | 490 (36.4) | 922 (43.2) | |
| Marital status | 0.432 | |||
| Married, n (%) | 2661 (76.5) | 1032 (76.7) | 1629 (76.3) | |
| Divorced, n (%) | 132 (3.8) | 45 (3.3) | 87 (4.1) | |
| Unmarried, n (%) | 687 (19.7) | 268 (20.0) | 419 (19.6) | 0.459 |
| Administrative region | ||||
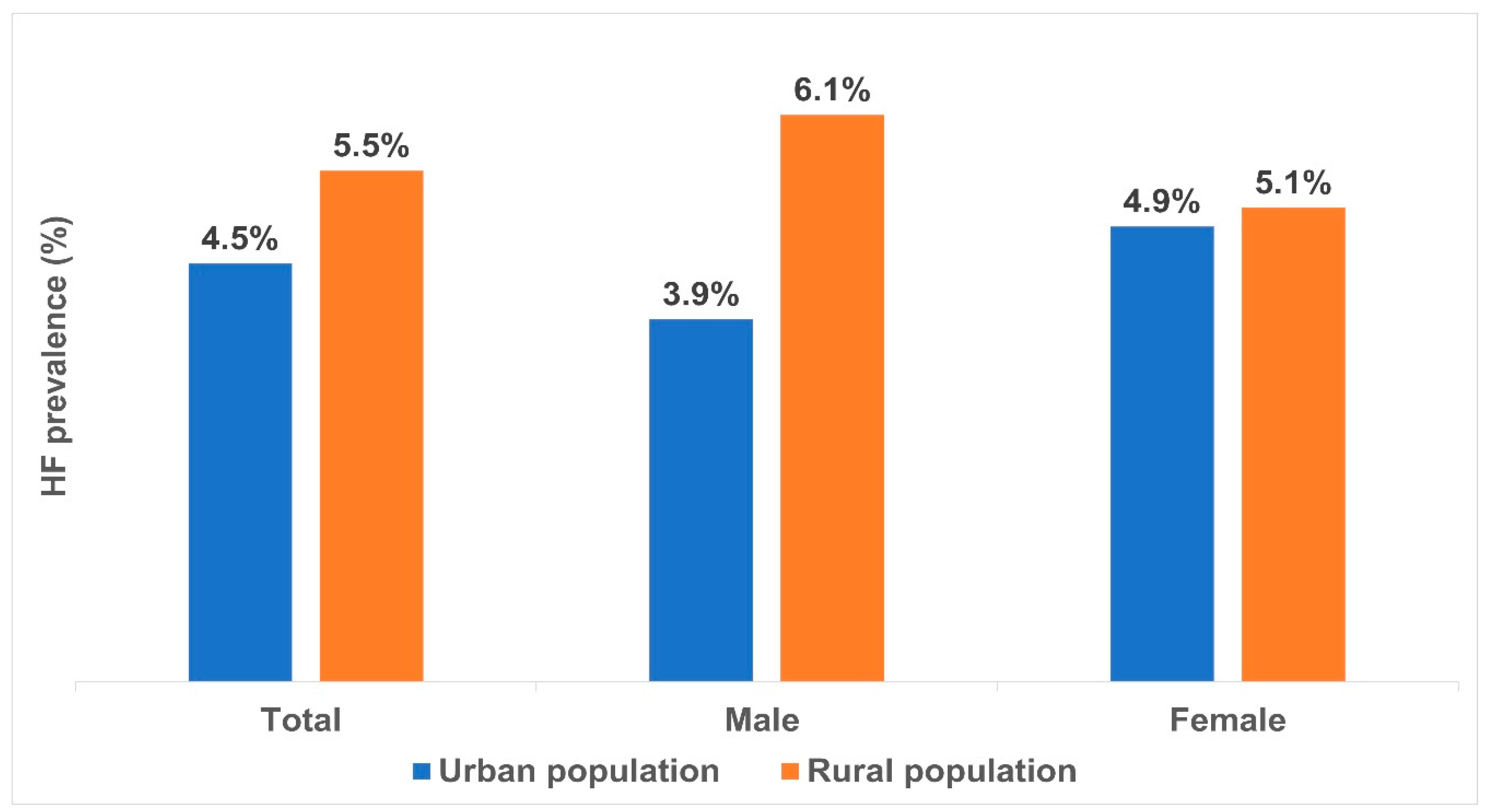
| Urban area, n (%) | 1686 (48) | 641 (47.6) | 1045 (49.9) | |
| Rural area, n (%) | 1794 (52) | 704 (52.3) | 1090 (51.1) |
| Variables | Total Subjects (n = 3480) | 20–29 Years (n = 807) | 30–39 Years (n = 863) | 40–49 Years (n = 682) | 50–59 Years (n = 595) | 60–69 Years (n = 381) | ≥70 Years (n = 152) | p-Value |
|---|---|---|---|---|---|---|---|---|
| CAD, n (%) | 90 (3) | 1 (0) | 6 (1) | 20 (3) | 26 (4) | 23 (6) | 14 (9) | <0.0001 |
| Hypertension, n (%) | 1358 (39) | 91 (11) | 210 (24) | 295 (43) | 392 (66) | 246 (65) | 124 (82) | <0.0001 |
| DM, n (%) | 198 (6) | 12 (2) | 33 (4) | 37 (5) | 59 (10) | 36 (9) | 21 (14) | <0.0001 |
| VHD, n (%) | 82 (2) | 8 (1) | 12 (1) | 17 (3) | 28 (5) | 16 (4) | 1 (1) | <0.0001 |
| Obesity, n (%) | 1358 (39) | 86 (11) | 175 (20) | 207 (30) | 173 (29) | 114 (30) | 35 (23) | <0.0001 |
| Smoking, n (%) | 712 (21) | 117 (15) | 191 (22) | 164 (24) | 135 (23) | 78 (21) | 27 (18) | <0.0001 |
| Abnormal alcohol consumption, n (%) | 300 (9) | 30 (4) | 82 (10) | 74 (11) | 76 (13) | 28 (7) | 10 (7) | <0.0001 |
| Variables | Total Participants n = 3480 | Population in Urban Area (n = 1686) | Population in Rural Area (n = 1794) | p-Value |
|---|---|---|---|---|
| Coronary heart disease, n (%) | 90 (3) | 46 (3) | 44 (3) | 0.609 |
| Hypertension, n (%) | 1358 (39) | 661 (39) | 697 (39) | 0.831 |
| Diabetes mellitus, n (%) | 198 (6) | 113 (7) | 85 (5) | 0.012 |
| Valvular heart disease | 82 (2) | 35 (3) | 47 (2) | 0.290 |
| Obesity, n (%) | 790 (23) | 350 (21) | 440 (25) | 0.008 |
| Smoking, n (%) | 712 (21) | 373 (22) | 339 (19) | 0.018 |
| Abnormal alcohol consumption, n (%) | 300 (9) | 118 (7) | 182 (10) | 0.001 |
| Characteristics | Total Study Population n = 3480 | Non-HF Group n = 3308 (95%) | HF Group n = 172 (5%) | p-Value |
|---|---|---|---|---|
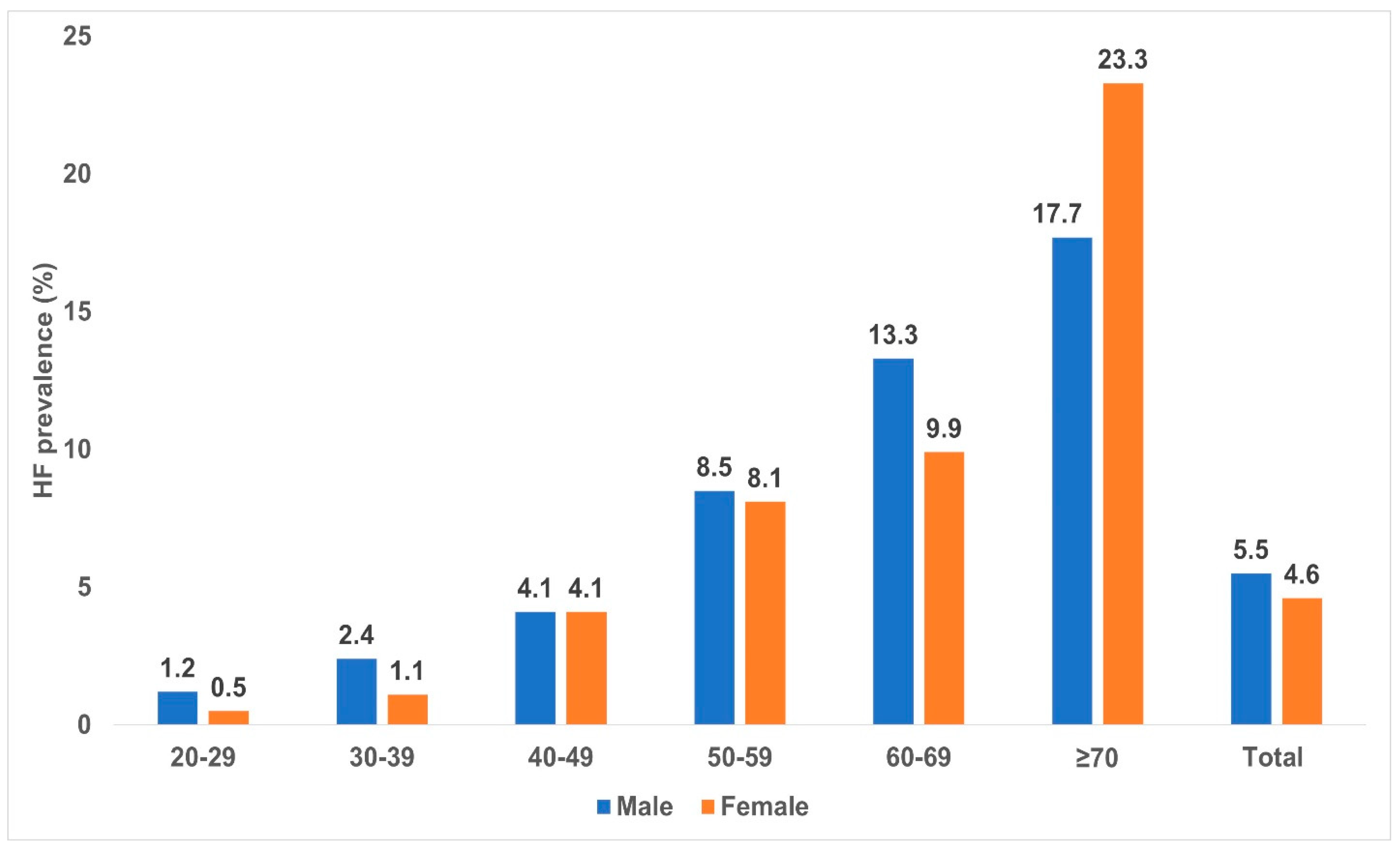
| Sex | 0.227 | |||
| Male | 1345 (39) | 1271 (94.5) | 74 (5.5) | |
| Female | 2135 (61) | 2037 (95.4) | 98 (4.6) | |
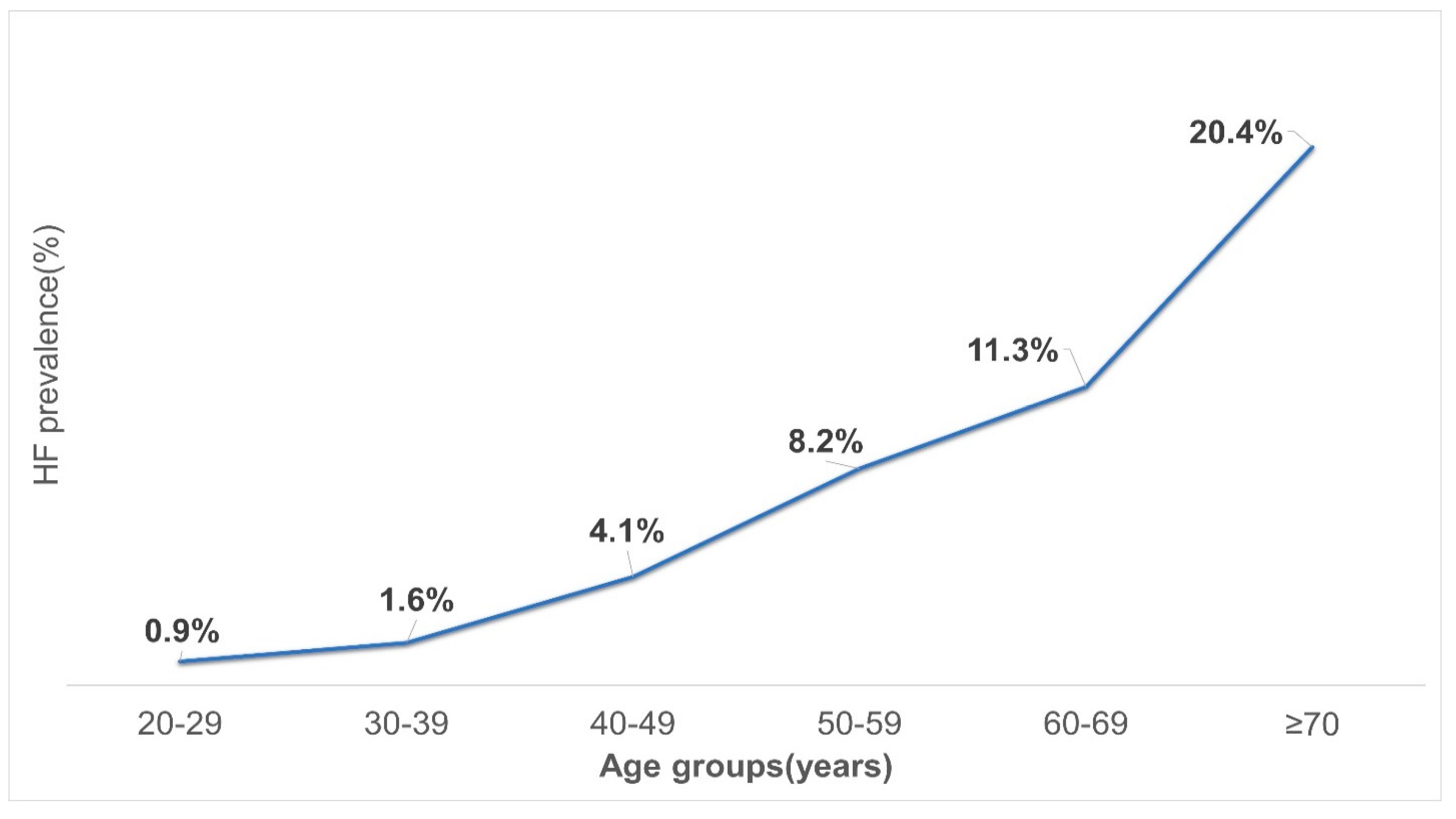
| Age group | <0.0001 | |||
| 20–29 | 807 (23) | 801(24) | 6 (4) | |
| 30–39 | 863 (25) | 849 (26) | 14 (8) | |
| 40–49 | 682 (20) | 654 (20) | 28 (16) | |
| 50–59 | 595 (17) | 546 (16) | 49 (28) | |
| 60–69 | 381 (11) | 338 (10) | 43 (25) | |
| ≥70 | 152 (4) | 120 (4) | 32 (19) | |
| Average age | 41.0 (30.0–54.0) | 40.0 (30.0–53.0) | 57.0 (49.0–65.8) | <0.0001 |
| Education | <0.0001 | |||
| Higher | 1229 (35) | 1198 (36) | 31 (18) | |
| Medium | 1784(51) | 1695 (51) | 89 (52) | |
| Lower | 467(14) | 415 (13) | 52 (30) | |
| Occupation | <0.0001 | |||
| Manual labor work | 830 (24) | 793 (24) | 37 (21) | |
| Intellectual labor work | 1238 (51) | 1202 (36) | 36 (21) | |
| Unemployed | 1412 (40) | 1313 (40) | 99 (58) | |
| Marital status | 0.479 | |||
| Married | 2661 (76) | 2523 (76) | 138 (80) | |
| Divorced | 132 (4) | 127 (4) | 5 (3) | |
| Unmarried | 687 (20) | 658 (20) | 29 (17) |
| Variable | OR | Min Value | Max Value | p-Value |
|---|---|---|---|---|
| Hypertension | 4.855 | 3.127 | 7.538 | <0.0001 |
| CAD | 5.117 | 3.040 | 8.614 | <0.0001 |
| Valvular heart disease | 3.872 | 2.112 | 7.099 | <0.0001 |
| Abnormal alcohol consumption | 1.861 | 1.155 | 2.998 | 0.011 |
| Smoking | 1.391 | 0.918 | 2.109 | 0.120 |
| Obesity | 2.136 | 1.542 | 2.959 | <0.0001 |
| Diabetes mellitus | 1.440 | 0.865 | 2.397 | 0.161 |
| Variables | Total Study Population (n = 3480) | Non-HF Group n = 3308 (95%) | HF Group n = 172 (5%) | p-Value |
|---|---|---|---|---|
| Risk factors | ||||
| Hypertension, n (%) | 1358 (39) | 1213 (37) | 145 (84) | <0.0001 |
| Valvular heart disease, n (%) | 82 (2) | 67 (2) | 15 (9) | <0.0001 |
| Abnormal alcohol consumption, n (%) | 300(9) | 275 (8) | 25 (15) | 0.005 |
| Smoking, n (%) | 712 (20) | 667 (20) | 45 (26) | 0.057 |
| Diabetes mellitus, n (%) | 198 (6) | 178 (5) | 20 (12) | 0.001 |
| Obesity, n (%) | 790 (23) | 719 (22) | 71 (41) | <0.0001 |
| Coronary artery disease, n (%) | 90 (3) | 63 (2) | 27 (16) | <0.0001 |
| Clinical charactheristics | ||||
| Body mass index, (kg/m2) | 26.4 ± 5.1 | 26.2 ± 5.0 | 28.8 ± 6.2 | <0.0001 |
| Heart rate, per minute | 80.0 ± 11.1 | 79.6 ± 10.8 | 84.9 ± 15.7 | <0.0001 |
| Respiratory rate, per minute | 18.2 ± 5.1 | 18.2 ± 5.2 | 19.2 ± 3.1 | 0.012 |
| Oxygen saturation, % | 96.2 ± 3.7 | 96.2 ±3.8 | 95.0 ± 3.1 | <0.0001 |
| Systolic blood pressure, mmHg | 122.0 ± 19.4 | 121.2 ± 18.9 | 137.7 ± 22.4 | <0.0001 |
| Diastolic blood pressure, mmHg | 78.7 ± 12.6 | 78.3 ± 12.4 | 86.2 ± 15.2 | <0.0001 |
| Medications | Non-HF Group (n = 3308) | HF Group (n = 172) | p-Value |
|---|---|---|---|
| Diuretics, n (%) | 181 (5.4) | 88 (51.2) | <0.0001 |
| RAAS inhibitors, n (%) | 210 (6.3) | 86 (50.0) | <0.0001 |
| Beta blockers, n (%) | 190 (5.7) | 75 (43.6) | <0.0001 |
| Sacubitril/valsartan, n (%) | 42 (1.3) | 44 (25.6) | <0.0001 |
| Digoxin, n (%) | 26 (0.8) | 26 (15.1) | <0.0001 |
| Ivabradine, n (%) | 27 (0.8) | 22 (12.8) | <0.0001 |
| Age Group | Present Study (Mongolia) | CARLA Study (Germany) | Rotterdam Study (The Netherlands) | Olmsted County Study (USA) |
|---|---|---|---|---|
| 45–54 years | 4.3% | 3.0% | 0.7% | - |
| 55–64 years | 9.4% | 6.0% | 0.7% | 1.3% |
| 65–74 years | 13.1% | 10.4% | 2.7% | 1.5% |
| 75–84 years | 25.7% | 22.0% | 13% | 8.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sukhbaatar, P.; Bayartsogt, B.; Ulziisaikhan, G.; Byambatsogt, B.; Khorloo, C.; Badrakh, B.; Tserendavaa, S.; Sodovsuren, N.; Dagva, M.; Khurelbaatar, M.-U.; et al. The Prevalence and Risk Factors of Chronic Heart Failure in the Mongolian Population. Diagnostics 2023, 13, 999. https://doi.org/10.3390/diagnostics13050999
Sukhbaatar P, Bayartsogt B, Ulziisaikhan G, Byambatsogt B, Khorloo C, Badrakh B, Tserendavaa S, Sodovsuren N, Dagva M, Khurelbaatar M-U, et al. The Prevalence and Risk Factors of Chronic Heart Failure in the Mongolian Population. Diagnostics. 2023; 13(5):999. https://doi.org/10.3390/diagnostics13050999
Chicago/Turabian StyleSukhbaatar, Pagmadulam, Batzorig Bayartsogt, Ganchimeg Ulziisaikhan, Bolortuul Byambatsogt, Chingerel Khorloo, Burmaa Badrakh, Sumiya Tserendavaa, Naranchimeg Sodovsuren, Mungunchimeg Dagva, Mungun-Ulzii Khurelbaatar, and et al. 2023. "The Prevalence and Risk Factors of Chronic Heart Failure in the Mongolian Population" Diagnostics 13, no. 5: 999. https://doi.org/10.3390/diagnostics13050999