

Association of Body Mass Index (BMI) with Lip Morphology Characteristics: A Cross-Sectional Study Based on Chinese Population
 , ,
, ,
Abstract
:1. Introduction
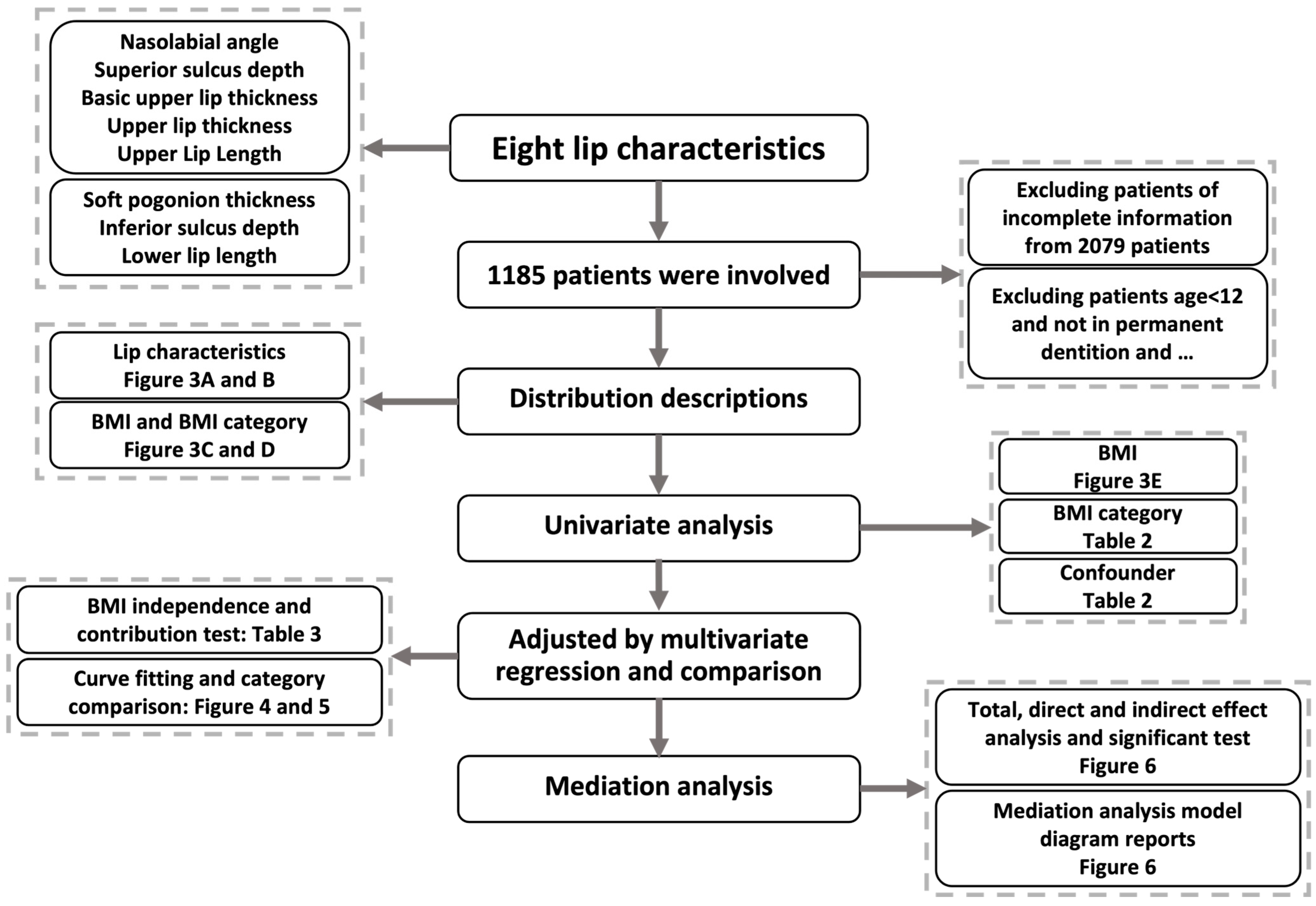
2. Materials and Methods
2.1. Study Population and Data Collection
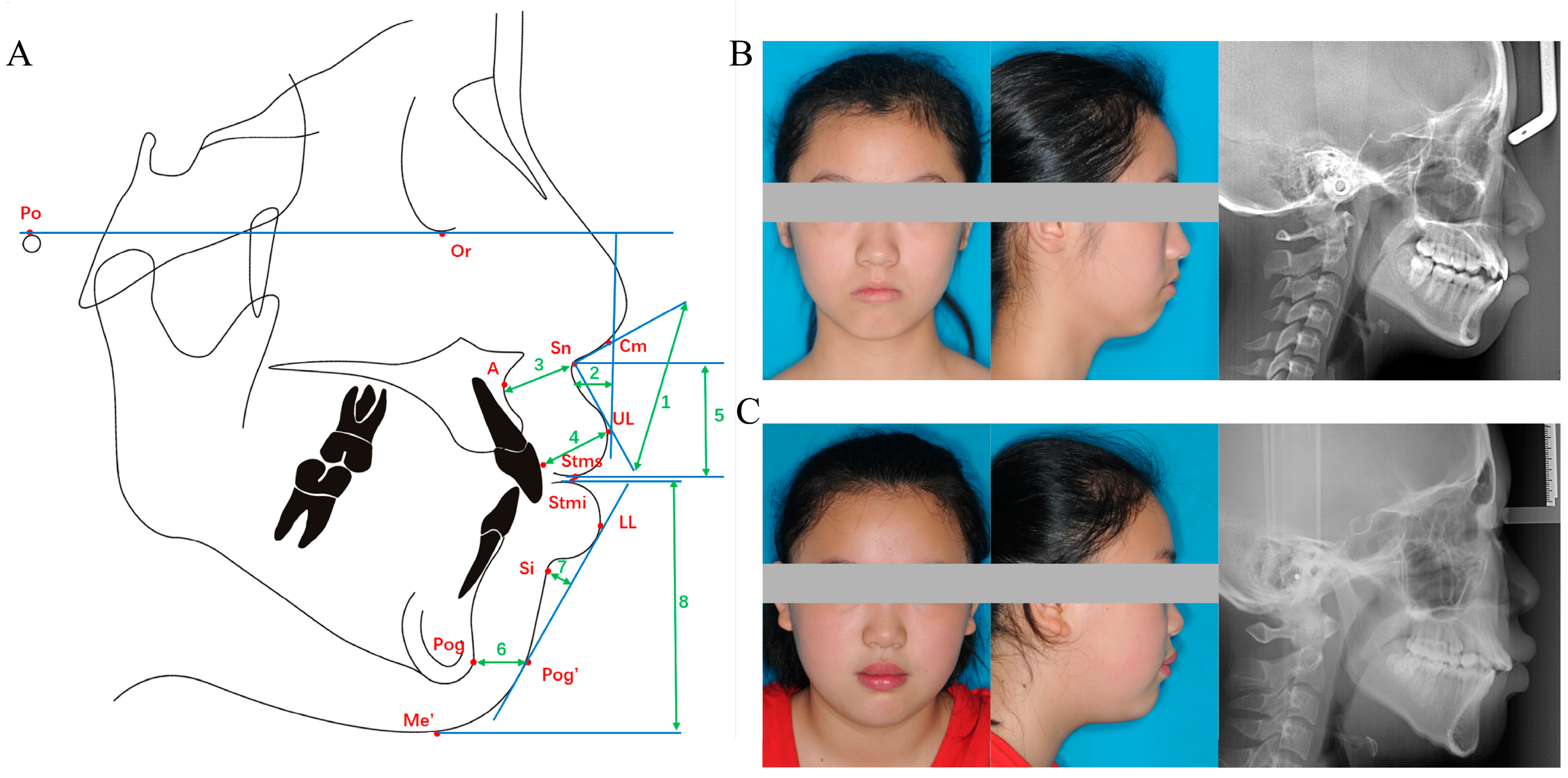
2.2. Lip Characteristics and BMI
2.3. Covariates
2.4. Statistical Analysis
3. Results
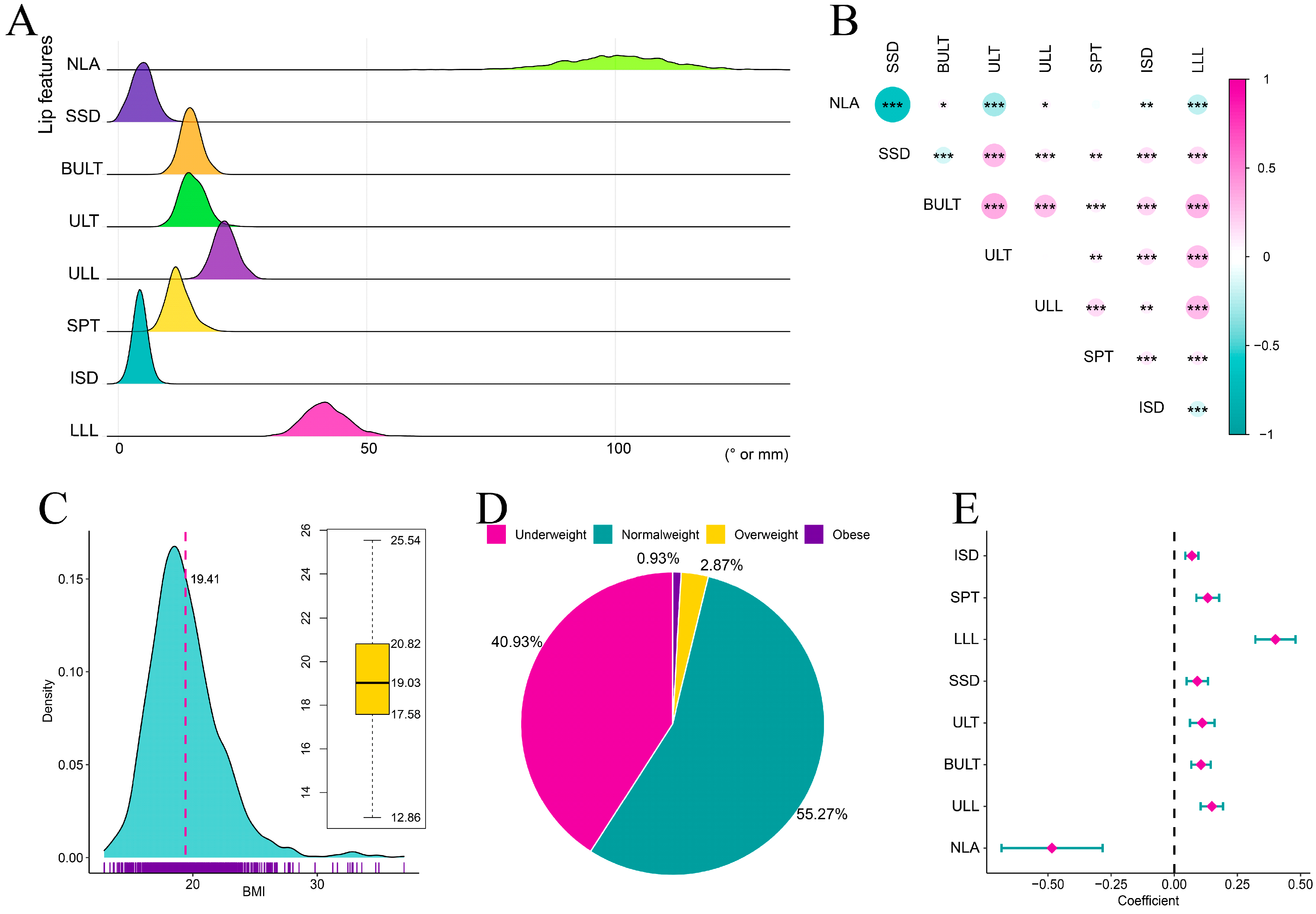
3.1. Study Participant Characteristics
3.2. Associations between BMI and Lip Characteristics
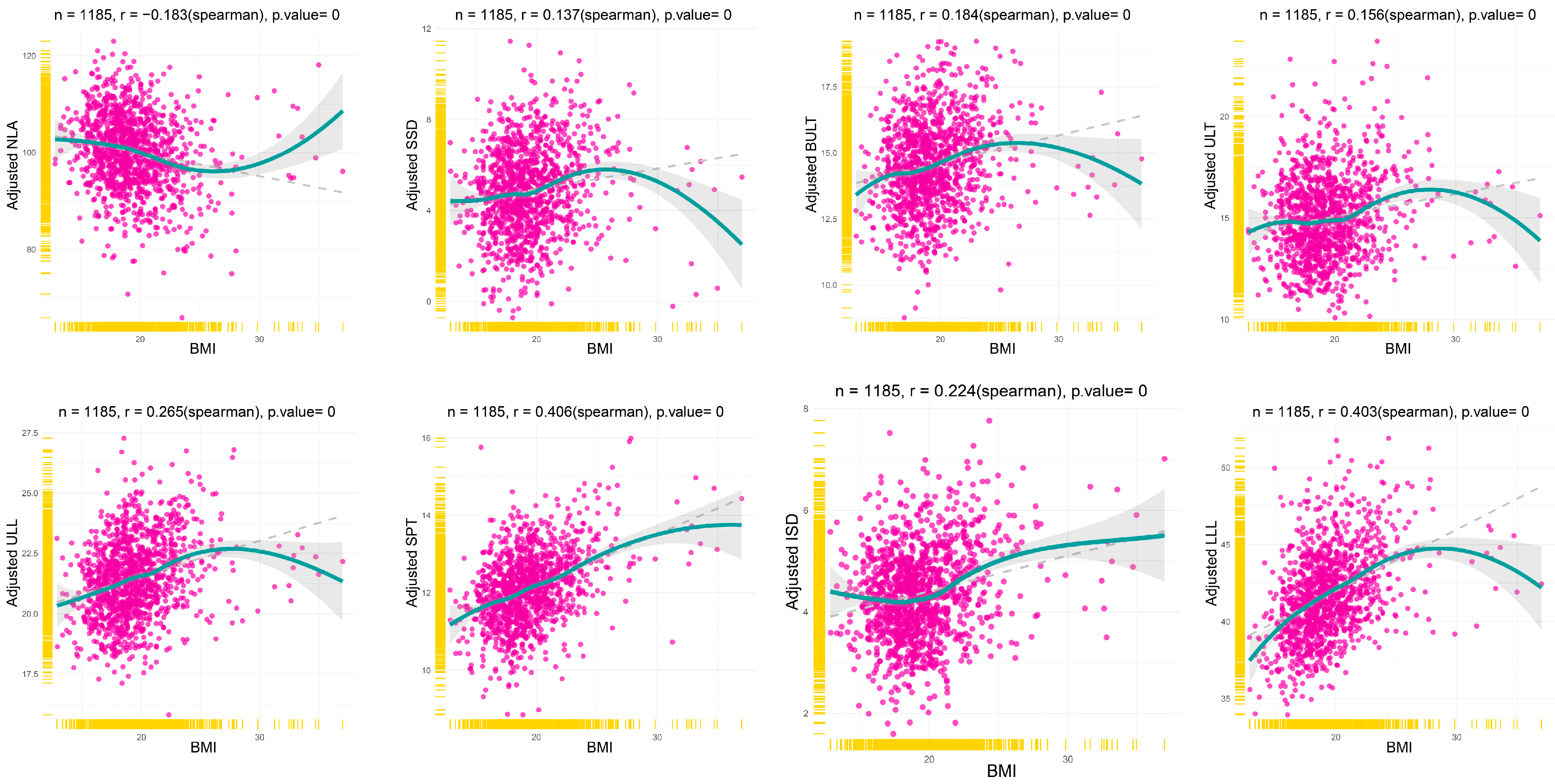
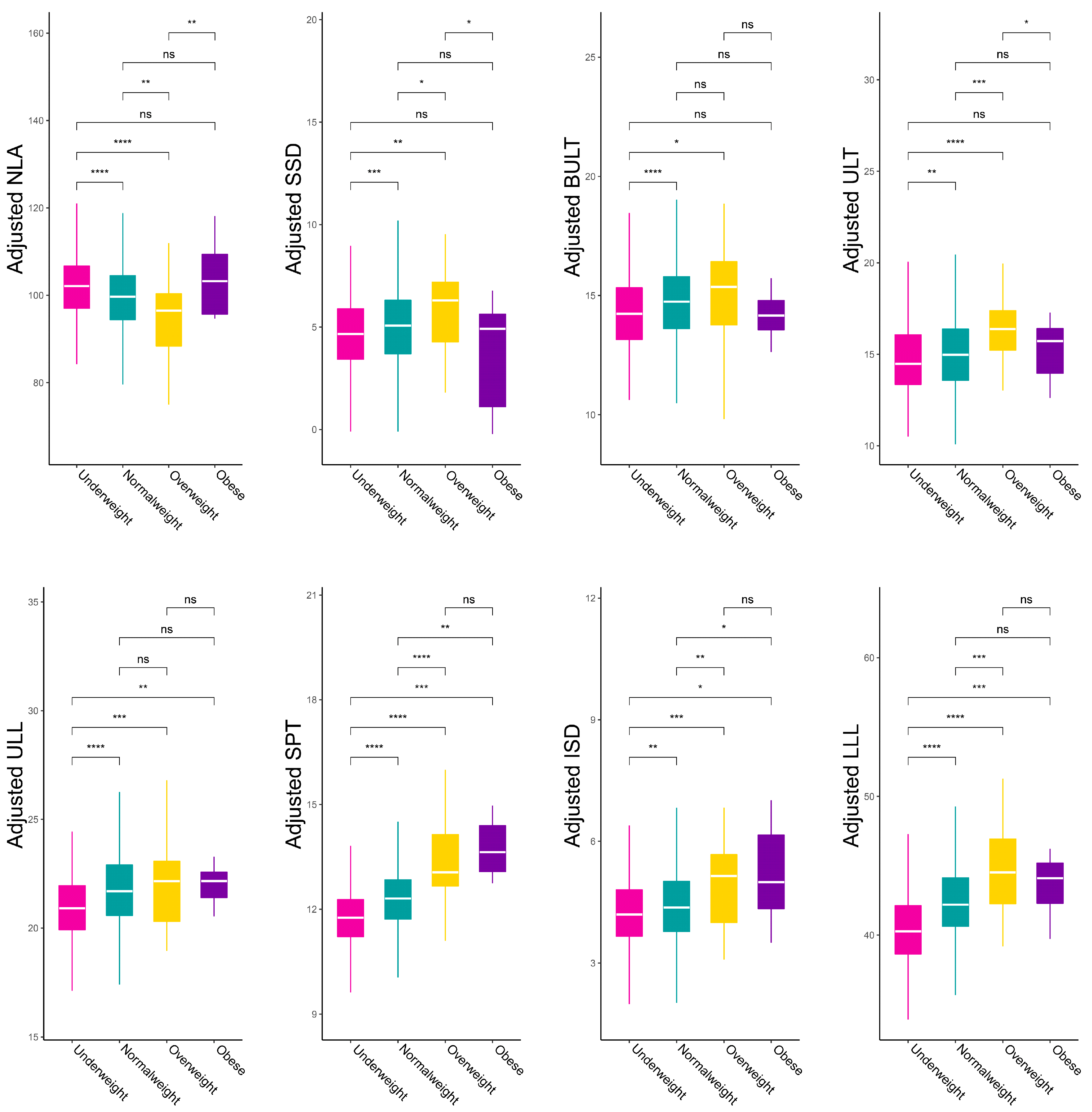
3.3. Tendency of Lip Characteristics with BMI Variation
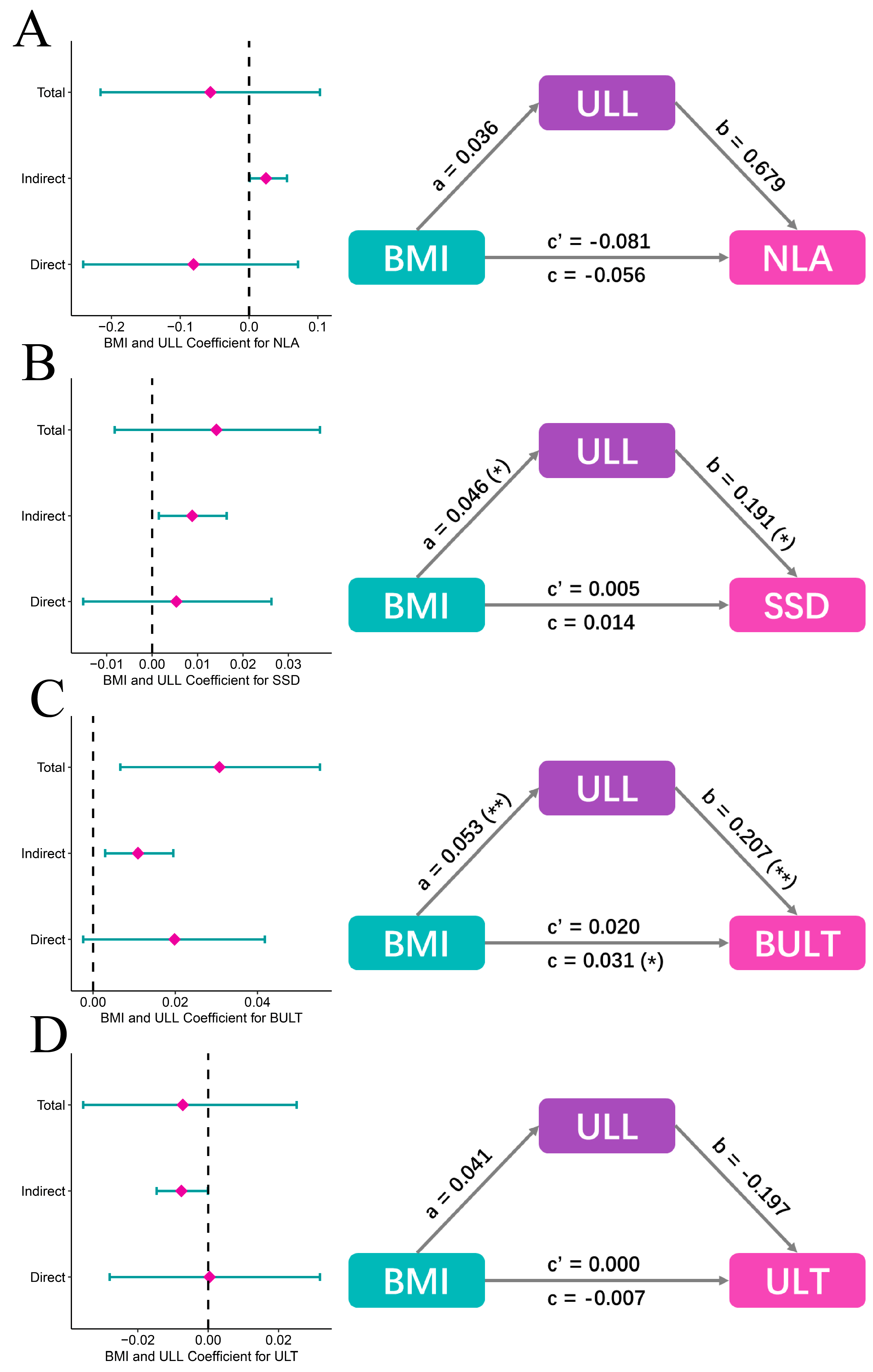
3.4. Mediation Analysis
4. Discussion
5. Conclusions
- The study provided the reference values of lip morphology characteristics and BMI in a Chinese population, which can provide a reference for Chinese doctors and researchers.
- After adjusting for confounders, lip morphology characteristics were found to be significantly different among various BMI categories, suggesting that orthodontists should develop more personalized treatment options for patients with different BMI.
- BMI is associated with all LMCs, but only independently associated with upper lip length, soft pogonion thickness, inferior sulcus depth and lower lip length.
- The relationship between BMI and LMCs in obese patients was different from that in other BMI categories.
- BMI was associated with superior sulcus depth (SSD) and basic upper lip thickness (BULT) through upper lip length (ULL).
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ghorbanyjavadpour, F.; Rakhshan, V. Factors associated with the beauty of soft-tissue profile. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 832–843. [Google Scholar] [CrossRef] [PubMed]
- Varatharaju, V.; Caflisch, M.; Soroken, C.; Kiliaridis, S.; Antonarakis, G.S. Does age influence self-perception of the soft-tissue profile in children? Am. J. Orthod. Dentofac. Orthop. 2021, 159, e207–e215. [Google Scholar] [CrossRef] [PubMed]
- Patil, H.S.; Golwalkar, S.; Chougule, K.; Kulkarni, N.R. Comparative Evaluation of Soft Tissue Chin Thickness in Adult Patients with Skeletal Class II Malocclusion with Various Vertical Growth Patterns: A Cephalometric Study. Folia Med. 2021, 63, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.Q.; Pan, B.L.; An, Y.; An, J.X.; Chen, L.J.; Li, D. Lip Morphology and Aesthetics: Study Review and Prospects in Plastic Surgery. Aesthetic Plast. Surg. 2019, 43, 637–643. [Google Scholar] [CrossRef]
- Alshahrani, I.; Kamran, M.A.; Asiry, M.A.; Alshahrani, A.; Almoammar, S.; Alhaizaey, A. Evaluation of cephalometric lip morphology in a Saudi sub population: A cross sectional study. J. Pak. Med. Assoc. 2020, 70, 151–153. [Google Scholar] [CrossRef]
- El Asmar, R.; Akl, R.; Ghoubril, J.; El Khoury, E. Evaluation of the ideal position of the maxillary incisor relative to upper lip thickness. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Zhang, X.; Chen, Y.; Long, H.; Lai, W. Association of Upper Lip Morphology Characteristics with Sagittal and Vertical Skeletal Patterns: A Cross Sectional Study. Diagnostics 2021, 11, 1713. [Google Scholar] [CrossRef]
- Daniels, S.R. The use of BMI in the clinical setting. Pediatrics 2009, 124 (Suppl. S1), S35–S41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Consultation WHOE. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, C.C.C.; Silva, M.; Nunes, A.M.M.; Thomaz, E.; Carmo, C.D.S.; Ribeiro, M.R.C.; da Silva, A.A.M. Overweight, obese, underweight, and frequency of sugar consumption as risk indicators for early childhood caries in Brazilian preschool children. Int. J. Paediatr. Dent. 2017, 27, 532–539. [Google Scholar] [CrossRef]
- Aluckal, E.; Anzil, K.; Baby, M.; George, E.K.; Lakshmanan, S.; Chikkanna, S. Association between Body Mass Index and Dental Caries among Anganwadi Children of Belgaum City, India. J. Contemp. Dent. Pract. 2016, 17, 844–848. [Google Scholar]
- Sfasciotti, G.L.; Marini, R.; Pacifici, A.; Ierardo, G.; Pacifici, L.; Polimeni, A. Childhood overweight-obesity and periodontal diseases: Is there a real correlation? Ann. Stomatol. 2016, 7, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Simsek, H.; Korkmaz, Y.N.; Buyuk, S.K. Relationship between obesity and prevalence of dental anomalies: Does body mass index play a role? Eur. J. Paediatr. Dent. 2019, 20, 95–99. [Google Scholar] [PubMed]
- Michelogiannakis, D.; Rossouw, P.E.; Khan, J.; Akram, Z.; Menenakos, E.; Javed, F. Influence of increased body mass index on orthodontic tooth movement and related parameters in children and adolescents: A systematic review of longitudinal controlled clinical studies. J. Orthod. 2019, 46, 323–334. [Google Scholar] [CrossRef]
- López-Gómez, J.J.; Pérez Castrillón, J.L.; de Luis Román, D.A. Impact of obesity on bone metabolism. Endocrinol. Nutr. 2016, 63, 551–559. [Google Scholar] [CrossRef]
- Al-Jewair, T.; Marwah, S.; Preston, C.B.; Wu, Y.; Yu, G. Correlation between craniofacial structures, anthropometric measurements, and nasopharyngeal dimensions in black adolescents. Int. Orthod. 2021, 19, 96–106. [Google Scholar] [CrossRef]
- Giuca, M.R.; Giannotti, L.; Saggese, R.; Vanni, A.; Pasini, M. Evaluation of cephalometric, hormonal and enzymatic parameters in young obese subjects. Eur. J. Paediatr. Dent. 2013, 14, 175–180. [Google Scholar] [PubMed]
- Chu, G.; Han, M.-Q.; Ji, L.-L.; Li, M.-J.; Zhou, H.; Chen, T.; Guo, Y.-C. Will different sagittal and vertical skeletal types relate the soft tissue thickness: A study in Chinese female adults. Leg Med. 2020, 42, 101633. [Google Scholar] [CrossRef]
- Buyuk, S.K.; Genc, E.; Simsek, H.; Karaman, A. Analysis of facial soft tissue values and cranial skeletal widths in different body mass index percentile adolescent subjects. Cranio 2019, 37, 223–230. [Google Scholar] [CrossRef]
- Joshi, M.; Wu, L.P.; Maharjan, S.; Regmi, M.R. Sagittal lip positions in different skeletal malocclusions: A cephalometric analysis. Prog. Orthod. 2015, 16, 8. [Google Scholar] [CrossRef] [Green Version]
- Al Taki, A.; Yaqoub, S.; Hassan, M. Legan-burstone soft tissue profile values in a Circassian adult sample. J. Orthod. Sci. 2018, 7, 18. [Google Scholar] [CrossRef] [PubMed]
- Ayoub, F.; Saadeh, M.; Fayyad-Kazan, H.; Haddad, R. Stereophotogrammetric analysis of labial morphology in a young adult Middle Eastern population. J. Craniomaxillofac. Surg. 2019, 47, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, C.; Wang, D.; Chen, J.; Li, K.; Yang, M.; Chen, Z.; Zhu, Z.; Yin, C.; Chen, P.; Cao, D.; et al. Facial soft tissue thickness in Yangtze River delta Han population: Accurate assessment and comparative analysis utilizing Cone-Beam CT. Leg Med. 2020, 44, 101693. [Google Scholar] [CrossRef] [PubMed]
- Ricketts, R.M. The value of cephalometrics and computerized technology. Angle Orthod. 1972, 42, 179–199. [Google Scholar]
- Bishara, S.E.; Hession, T.J.; Peterson, L.C. Longitudinal soft-tissue profile changes: A study of three analyses. Am. J. Orthod. 1985, 88, 209–223. [Google Scholar] [CrossRef]
- Huang, L.; Gao, X. The interaction of obesity and craniofacial deformity in obstructive sleep apnea. Dentomaxillofac. Radiol. 2021, 50, 20200425. [Google Scholar] [CrossRef]
- Lee, Y.J.; Park, J.T.; Cha, J.Y. Perioral soft tissue evaluation of skeletal Class II Division 1: A lateral cephalometric study. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Arora, A.; Valiathan, A. Age changes of jaws and soft tissue profile. Sci. World J. 2014, 2014, 301501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johari, M.; Esmaeili, F.; Hamidi, H. Facial Soft Tissue Thickness of Midline in an Iranian Sample: MRI Study. Open Dent. J. 2017, 11, 375–383. [Google Scholar] [CrossRef] [Green Version]
- Nikolis, A.; Frank, K.; Guryanov, R.; Gombolevskiy, V.; Morozov, S.; Makhmud, K.; Chernina, V.; Gotkin, R.H.; Green, J.B.; Cotofana, S. Differences in Temporal Volume between Males and Females and the Influence of Age and BMI: A Cross-Sectional CT-Imaging Study. Facial Plast. Surg. 2021, 37, 632–638. [Google Scholar] [CrossRef]
- De Greef, S.; Claes, P.; Vandermeulen, D.; Mollemans, W.; Suetens, P.; Willems, G. Large-scale in-vivo Caucasian facial soft tissue thickness database for craniofacial reconstruction. Forensic Sci. Int. 2006, 159 (Suppl. S1), S126–S146. [Google Scholar] [CrossRef]
- Dong, Y.; Huang, L.; Feng, Z.; Bai, S.; Wu, G.; Zhao, Y. Influence of sex and body mass index on facial soft tissue thickness measurements of the northern Chinese adult population. Forensic Sci. Int. 2012, 222, 396.e1–396.e7. [Google Scholar] [CrossRef]
- Hwang, H.S.; Park, M.K.; Lee, W.J.; Cho, J.H.; Kim, B.K.; Wilkinson, C.M. Facial soft tissue thickness database for craniofacial reconstruction in Korean adults. J. Forensic Sci. 2012, 57, 1442–1447. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhao, X.; Mi, C.; Raza, I. The study on facial soft tissue thickness using Han population in Xinjiang. Forensic Sci. Int. 2016, 266, 585.e1–585.e5. [Google Scholar] [CrossRef] [PubMed]
- Briers, N.; Briers, T.M.; Becker, P.J.; Steyn, M. Soft tissue thickness values for black and coloured South African children aged 6–13 years. Forensic Sci. Int. 2015, 252, 188.e1–188.e10. [Google Scholar] [CrossRef] [Green Version]
- Negruţiu, B.M.; Vaida, L.L.; Todor, B.I.; Judea, A.S.; Lile, I.E.; Moca, A.E.; Judea-Pusta, C.T. An important morphological feature of the face: Upper lip length. Rom. J. Morphol. Embryol. 2019, 60, 537–541. [Google Scholar] [PubMed]
- McNamara, L.; McNamara, J.A.; Jr Ackerman, M.B.; Baccetti, T. Hard- and soft-tissue contributions to the esthetics of the posed smile in growing patients seeking orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 491–499. [Google Scholar] [CrossRef]
- Baillie, L.J.; Mirijali, S.A.; Niven, B.E.; Blyth, P.; Dias, G.J. Ancestry and BMI Influences on Facial Soft Tissue Depths for A Cohort of Chinese and Caucasoid Women in Dunedin, New Zealand. J. Forensic Sci. 2015, 60, 1146–1154. [Google Scholar] [CrossRef] [PubMed]
- Toneva, D.; Nikolova, S.; Georgiev, I.; Harizanov, S.; Zlatareva, D.; Hadjidekov, V.; Lazarov, N. Facial soft tissue thicknesses in Bulgarian adults: Relation to sex, body mass index and bilateral asymmetry. Folia Morphol. 2018, 77, 570–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saloom, H.F.; Boustan, R.; Seehra, J.; Papageorgiou, S.N.; Carpenter, G.H.; Cobourne, M.T. The impact of obesity on orthodontic treatment outcome in adolescents: A prospective clinical cohort study. Eur. J. Orthod. 2021, 43, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Leonard, M.B.; Shults, J.; Wilson, B.A.; Tershakovec, A.M.; Zemel, B.S. Obesity during childhood and adolescence augments bone mass and bone dimensions. Am. J. Clin. Nutr. 2004, 80, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Danze, A.; Jacox, L.A.; Bocklage, C.; Whitley, J.; Moss, K.; Hardigan, P.; Garcia-Godoy, C.; Jackson, T.H. Influence of BMI percentile on craniofacial morphology and development in children and adolescents. Eur. J. Orthod. 2021, 43, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Yasa, Y.; Buyuk, S.K.; Genc, E. Comparison of mandibular cortical bone among obese, overweight, and normal weight adolescents using panoramic mandibular index and mental index. Clin. Oral Investig. 2020, 24, 2919–2924. [Google Scholar] [CrossRef]
- Yin, G.; Liao, S.; Gong, D.; Qiu, H. Association of acrylamide and glycidamide haemoglobin adduct levels with diabetes mellitus in the general population. Environ. Pollut. 2021, 277, 116816. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Zheng, D.; Li, Z.; Wu, Z.; Feng, W.; Cao, X.; Wang, J.; Gao, Q.; Li, X.; Wang, W.; et al. Association of Depressive Symptoms With Incident Cardiovascular Diseases in Middle-Aged and Older Chinese Adults. JAMA Netw. Open 2019, 2, e1916591. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Landmarks | Definition |
|---|---|
| Porion (Po) | The most superior point of the anatomical image of the external auditory canal. |
| Orbitale (Or) | The lowest point of the inferior orbital margin. |
| Sub-spinale (point A) | The most concave point of the bone between anterior nasal spine and upper alveolar margin. |
| Pogonion (Pog) | The most protruding point of the chin. |
| Columella (Cm) | The most prominent point below the nasal contour at the junction with the nasal tip. |
| Sub-nasale (Sn) | The junction of the nasal columella with the upper lip. |
| Labrale superius (UL) | The most prominent point on the upper lip. |
| Stomion superius (Stms) | The lowest point of the upper lip vermilion margin. |
| Stomion inferius (Stmi) | The highest point of the lower lip vermilion margin. |
| Labrale inferius (LL) | The most prominent point on the lower lip. |
| Mento-labial sulcus (Si) | The most concave point between the chin and lower lip. |
| Pogonion of soft tissue (Pog’) | The most anterior point of soft tissue of the chin. |
| Menton of soft tissue (Me’) | The lowest point of soft tissue of the chin. |
| Level | Overall | Underweight | Normal Weight | Overweight | Obese | p-Value |
|---|---|---|---|---|---|---|
| N | 1185 | 485 | 655 | 34 | 11 | |
| Demographic characteristics | ||||||
| BMI (median (IQR)) | 19.03 (17.58, 20.82) | 17.19 (16.23, 17.88) | 20.29 (19.25, 21.72) | 26.26 (25.59, 27.61) | 32.87 (32.55, 34.14) | <0.001 |
| Age (median (IQR)) | 19 (14, 24) | 15 (13. 21) | 20 (16, 25) | 18 (12, 22) | 15 (13, 21) | <0.001 |
| Gender (%) | ||||||
| Male | 396 (33.4) | 136 (28.0) | 234 (35.7) | 21 (61.8) | 5 (45.5) | <0.001 |
| Female | 789 (66.6) | 349 (72.0) | 421 (64.3) | 13 (38.2) | 6 (54.5) | |
| Dental characteristics | ||||||
| Molar Relationship (%) | ||||||
| I | 416 (35.1) | 174 (35.9) | 226 (34.5) | 12 (35.3) | 4 (36.4) | 0.034 |
| II-1 | 381 (32.2) | 175 (36.1) | 196 (29.9) | 7 (20.6) | 3 (27.3) | |
| II-2 | 111 (9.4) | 49 (10.1) | 59 (9.0) | 2 (5.9) | 1 (9.1) | |
| III | 277 (23.4) | 87 (17.9) | 174 (26.6) | 13 (38.2) | 3 (27.3) | |
| Upper crowding (%) | ||||||
| I | 685 (57.8) | 263 (54.2) | 393 (60.0) | 22 (64.7) | 7 (63.6) | 0.24 |
| II | 319 (26.9) | 141 (29.1) | 171 (26.1) | 6 (17.6) | 1 (9.1) | |
| III | 181 (15.3) | 81 (16.7) | 91 (13.9) | 6 (17.6) | 3 (27.3) | |
| Lower crowding (%) | ||||||
| I | 740 (62.4) | 291 (60.0) | 415 (63.4) | 26 (76.5) | 8 (72.7) | 0.309 |
| II | 336 (28.4) | 149 (30.7) | 180 (27.5) | 6 (17.6) | 1 (9.1) | |
| III | 109 (9.2) | 45 (9.3) | 60 (9.2) | 2 (5.9) | 2 (18.2) | |
| Overbite (mm) (median (IQR)) | 2.50 (1.00, 4.10) | 2.80 (1.10, 4.10) | 2.40 (0.90, 4.10) | 2.10 (0.35, 4.25) | 4.00 (2.20, 5.25) | 0.065 |
| Overjet (mm) (median (IQR)) | 4.0 (2.5, 5.7) | 4.3 (2.7, 5.8) | 3.7 (2.4, 5.7) | 3.0 (−0.8, 5.3) | 5.2 (2.9, 6.5) | 0.037 |
| Skeletal characteristics | ||||||
| SNA (mean (SD)) | 80.82 (3.69) | 80.58 (3.42) | 80.90 (3.86) | 82.08 (3.72) | 82.74 (3.44) | 0.025 |
| SNB (mean (SD)) | 77.42 (4.51) | 76.85 (4.07) | 77.72 (4.73) | 79.36 (5.44) | 78.40 (3.31) | 0.001 |
| ANB (median (IQR)) | 3.9 (1.6, 5.6) | 4.1 (2.0, 5.8) | 3.6 (1.3, 5.5) | 4.0 (−0.2, 5.8) | 4.1 (2.4, 6.3) | 0.070 |
| SN-MP (mean (SD)) | 34.50 (7.04) | 35.12 (6.59) | 34.22 (7.22) | 32.00 (8.94) | 31.85 (6.59) | 0.014 |
| FH-MP (mean (SD)) | 24.60 (6.56) | 25.15 (6.44) | 24.26 (6.55) | 23.54 (8.20) | 23.85 (6.82) | 0.104 |
| U1-NA (mm) (mean (SD)) | 5.56 (2.84) | 5.36 (2.82) | 5.74 (2.83) | 5.86 (3.20) | 3.56 (2.37) | 0.013 |
| U1-SN (median (IQR)) | 109 (103, 115) | 109 (103, 115) | 110 (102, 115) | 110 (106, 120) | 107 (100, 112) | 0.20 |
| L1-NB (mm) (mean (SD)) | 6.43 (3.00) | 6.25 (2.80) | 6.58 (3.13) | 6.59 (3.41) | 5.06 (2.47) | 0.13 |
| L1-MP (mean (SD)) | 96.42 (9.38) | 96.16 (8.97) | 96.58 (9.68) | 98.04 (8.37) | 94.04 (11.79) | 0.517 |
| Lip morphology characteristics | ||||||
| Nasolabial angle (NLA) (mean (SD)) | 100.25 (10.41) | 101.74 (10.44) | 99.34 (10.09) | 95.45 (11.79) | 103.33 (13.91) | <0.001 |
| Superior sulcus depth (SSD) (mm) (mean (SD)) | 4.88 (2.18) | 4.62 (2.02) | 5.01 (2.25) | 6.16 (2.40) | 3.80 (2.52) | <0.001 |
| Basic upper lip thickness (BULT) (mm) (mean (SD)) | 14.55 (2.00) | 14.24 (1.86) | 14.75 (2.05) | 15.24 (2.60) | 14.46 (1.51) | <0.001 |
| Upper lip thickness (ULT) (mm) (mean (SD)) | 15.01 (2.52) | 14.76 (2.45) | 15.12 (2.56) | 16.40 (2.56) | 14.56 (1.86) | 0.001 |
| Upper lip length (ULL) (mm) (mean (SD)) | 21.46 (2.33) | 21.00 (2.09) | 21.77 (2.41) | 22.09 (2.91) | 21.42 (1.77) | <0.001 |
| Soft pogonion thickness (SPT) (mm) (mean (SD)) | 12.12 (2.36) | 11.66 (2.24) | 12.42 (2.34) | 13.44 (2.56) | 10.42 (2.99) | <0.001 |
| Inferior sulcus depth (ISD) (mm) (mean (SD)) | 4.36 (1.35) | 4.19 (1.29) | 4.46 (1.37) | 4.78 (1.59) | 4.68 (1.43) | 0.001 |
| Lower lip length (LLL) (mm) (mean (SD)) | 41.75 (4.26) | 40.29 (4.04) | 42.69 (4.05) | 44.60 (5.16) | 41.02 (3.17) | <0.001 |
| β (95% CI) | ||||
|---|---|---|---|---|
| Model 1 a | Model 2 b | Model 3 c | Model 4 d | |
| Nasolabial angle (NLA) | −0.260 * (−0.465, −0.056) | −0.342 *** (−0.529, −0.154) | −0.177 * (−0.337, −0.017) | −0.081 (−0.235, 0.074) |
| Superior sulcus depth (SSD) (mm) | 0.059 ** (0.016, 0.102) | 0.044 * (0.007, 0.080) | −0.002 (−0.035, 0.030) | 0.005 (−0.017, 0.027) |
| Basic upper lip thickness (BULT) (mm) | 0.070 *** (0.033, 0.107) | 0.092 *** (0.055, 0.129) | 0.013 (−0.021, 0.048) | 0.020 (−0.004, 0.044) |
| Upper lip thickness (ULT) (mm) | 0.098 *** (0.053, 0.142) | 0.090 *** (0.045, 0.135) | −0.002 (−0.047, 0.043) | 0.0004 (−0.031, 0.032) |
| Upper lip length (ULL) (mm) | 0.084 *** (0.042, 0.126) | 0.147 *** (0.108, 0.186) | 0.060 ** (0.018, 0.103) | 0.039 * (0.002, 0.075) |
| Soft pogonion thickness (SPT) (mm) | 0.147 *** (0.100, 0.194) | 0.155 *** (0.111, 0.200) | 0.091 *** (0.043, 0.139) | 0.120 *** (0.073, 0.168) |
| Inferior sulcus depth (ISD) (mm) | 0.076 *** (0.053, 0.099) | 0.074 *** (0.051, 0.097) | 0.070 *** (0.045, 0.096) | 0.040 *** (0.018, 0.063) |
| Lower lip length (LLL) (mm) | 0.269 *** (0.193, 0.344) | 0.352 *** (0.283, 0.422) | 0.278 *** (0.206, 0.351) | 0.208 *** (0.139, 0.276) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.; Yang, H.; Zheng, Z.; Zhang, X.; Yan, X.; Long, H.; Lai, W. Association of Body Mass Index (BMI) with Lip Morphology Characteristics: A Cross-Sectional Study Based on Chinese Population. Diagnostics 2023, 13, 997. https://doi.org/10.3390/diagnostics13050997
Chen Y, Yang H, Zheng Z, Zhang X, Yan X, Long H, Lai W. Association of Body Mass Index (BMI) with Lip Morphology Characteristics: A Cross-Sectional Study Based on Chinese Population. Diagnostics. 2023; 13(5):997. https://doi.org/10.3390/diagnostics13050997
Chicago/Turabian StyleChen, Yiyin, Hongmei Yang, Zhijin Zheng, Xiaoqi Zhang, Xinyu Yan, Hu Long, and Wenli Lai. 2023. "Association of Body Mass Index (BMI) with Lip Morphology Characteristics: A Cross-Sectional Study Based on Chinese Population" Diagnostics 13, no. 5: 997. https://doi.org/10.3390/diagnostics13050997